
Abstract
Background:
Childhood maltreatment is a known risk factor for the development of mental disorders, such as psychotic symptoms. An extensive body of literature about childhood maltreatment and mental health has been developed in wealthy countries, but information about this connection is lacking in developing countries.
Aims:
To explore a possible relationship between childhood maltreatment and ultra-high risk of psychosis in a non-help-seeking population in a low- and middle-income country.
Methods:
A household survey was conducted in Sao Paulo, Brazil, involving over 2,500 individuals aged 18–30 years who were randomly selected from the general population. The participants underwent screening with the Prodromal Questionnaire. Ultra-high risk status was assessed using the Structured Interview for Prodromal Syndromes, and childhood maltreatment was assessed using the Childhood Trauma Questionnaire. The final sample comprised 87 ultra-high risk individuals and 115 controls.
Results:
Childhood maltreatment was significantly more present among ultra-high risk individuals. In ultra-high risk individuals, physical and emotional neglect were inversely related to grandiosity symptoms, physical abuse was related to perceptual abnormalities and physical neglect was related to disorganized speech and thought.
Conclusion:
This is the first study to investigate the relationship between childhood maltreatment and ultra-high risk status and psychopathological features in a large Latin American sample. Further studies in this field are necessary to better understand the specific influence of various early life adversities on psychosis risk.
Keywords
Introduction
Childhood maltreatment (CM) is defined as any act or series of acts of commission or omission by a parent or other caregiver that result in harm, potential for harm or threat of harm to a child (Leeb et al., 2008). The World Health Organization’s (WHO) global status report on violence prevention highlighted alarming numbers concerning CM worldwide; 25% of all adults reported being physically abused as children, and one in five women reported being sexually abused as children (Butchart et al., 2015). This burden has already been estimated in high-income countries, where 4%–16% of children are physically abused and 10% are neglected or psychologically abused each year (Gilbert et al., 2009).
The high number of individuals who suffer CM is a serious public health problem, as this exposure is a relevant risk factor for a range of psychiatric disorders, such as substance misuse, depressive disorder, post-traumatic stress disorder, panic disorder and social phobia (Gilbert et al., 2009; Kraan et al., 2018). Most importantly, CM has also been associated with the development of psychotic symptoms (Fusar-Poli et al., 2017; Read et al., 2005; Varese et al., 2012). In a meta-analysis that included case–control, cross-sectional and prospective cohort studies, patients with psychosis were 2.72 times more likely to have been exposed to childhood adversity compared to members of the control group (Varese et al., 2012). Other studies suggested a dose–response effect of childhood adversities that increased the risk of psychosis (Trauelsen et al., 2015) and a strong correlation of CM with hallucination severity and delusions within psychotic disorders (Bailey et al., 2018), and some evidence points to smaller cortical brain volume in those exposed to deprivation as children (LoPilato et al., 2019). The association of CM with psychosis is in line with the most recent advances regarding the etiopathogenesis of psychosis, which integrate genetic predisposition with environmental factors, such as early life adversities, urbanity, violence and drug use (Kaufman & Torbey, 2019; LoPilato et al., 2019; van Os et al., 2010).
For individuals in a prodromal phase or in subclinical states, defined as ultra-high risk (UHR) for psychosis (Fusar-Poli et al., 2013), CM was revealed to be more prevalent (Kraan et al., 2015; Peh et al., 2019) and more severe (Peh et al., 2019) in UHR individuals as compared to members of the control group. In a meta-analysis that examined childhood trauma and recent life events, the former was highly prevalent among UHR subjects, and childhood trauma was correlated with UHR status (Kraan et al., 2018). A representative 30-year prospective cohort study found a correlation between childhood adversity (i.e., broken homes, family problems, conflicts between parents, conflicts with parents, sexual abuse, severe punishment, dislike, rejection and repeated fights) and subclinical psychotic symptoms, and subjects who were affected by such adversities reported higher total distress over the entire 30-year period (Rössler et al., 2014). A recent meta-analysis suggested differential effects of CM subtypes on UHR individuals and pointed to distinct prevalences of CM subtypes, among which emotional abuse was more prevalent in UHR individuals compared to controls (odds ratio (OR) = 5.06) (Peh et al., 2019). Similarly, Velthorst et al. (2013) argued that different types of trauma are related to different attenuated psychosis symptoms for those at UHR. In particular, physical abuse suffered during childhood was associated with higher perceptual abnormalities, especially visual abnormalities. Although this finding was not confirmed in other studies, sexual abuse has been associated with transition to psychosis in a large UHR cohort (Thompson et al., 2014). These results show that different CM subtypes might have different effects on the clinical symptomatology and development of psychosis. This possibility reinforces the importance of studying CM subtypes and their specific effects on UHR individuals.
Socioeconomic status (SES) and sex have been presented in the literature as risk factors associated with both CM and UHR status. In a multilevel meta-analysis, Viola et al. (2016) estimated that high-income countries presented lower physical neglect rates, and countries’ per-capita gross domestic products were negatively associated with childhood physical neglect estimates. Conversely, Stoltenborgh et al. (2015) compared a series of meta-analyses of the prevalence of CM and concluded that CM is widespread worldwide, but there are insufficient studies for meta-analytical calculations in more deprived areas outside of North America and Europe. SES has also been accepted as a possible risk factor for the UHR condition (Fusar-Poli et al., 2017), as lower SES levels might be associated with subclinical psychotic symptoms (Loch et al., 2017). Regarding sex, the majority of studies on CM conducted in wealthy countries pointed to differences between sex and maltreatment type and indicated higher sexual abuse rates among girls and higher physical abuse rates among boys (Moody et al., 2018; Witt et al., 2017). However, research in regions outside the Western world indicates mixed trends. A Chinese meta-analysis found no association between sex and CM subtype prevalence (Fu et al., 2018), and an extensive study conducted in Balkan countries found more sexual exposure and sexual violence among boys than among girls (Nikolaidis et al., 2018). Furthermore, male sex has been associated with higher risk for developing psychosis (Kirkbride et al., 2012). Sex differences for those with UHR status have been addressed less frequently, but some evidence suggests that males tend to exhibit more negative symptoms and poorer social functioning (Rietschel et al., 2017; Salokangas et al., 2013), whereas female sex is a predictor for affective psychosis (Barajas et al., 2015).
Despite elevated CM prevalence rates and the serious and profound effects they entail, some aspects of CM must be better understood. There is a lack of cross-cultural research that addresses CM and its possible effects on the UHR condition in low- and middle-income countries (LMIC) (Brietzke et al., 2011; Gaspar et al., 2019; Viola et al., 2016). In addition, few studies assess CM subtypes other than sexual or physical abuse (Stoltenborgh et al., 2015). To address this issue, we examined the relationship between CM and UHR status in a populational sample from Sao Paulo, Brazil. We hypothesized that (1) UHR individuals would present higher CM levels compared to controls, (2) SES and sex could be modulating factors for CM and/or the UHR condition and (3) CM subtypes could be specifically correlated with various prodromal symptoms.
Methods
Sample and procedures
This study is part of the Subclinical Symptoms and Prodromal Psychosis (SSAPP) project, a cohort study situated in Sao Paulo City, Brazil, and aimed at following up with a cohort of individuals at UHR for psychosis (Loch et al., 2017). Over 2,500 individuals aged between 18 and 30 years were asked to participate in the research through a household survey conducted by a renowned international research company (IPSOS).
The Prodromal Questionnaire (PQ) (Loewy et al., 2005) was used as screening instrument. The PQ is a self-report questionnaire with 92 true/false items related to prodromal symptoms of psychosis. Most items are similar to the Structured Interview for Prodromal Syndromes (SIPS) and the Schizotypal Personality Questionnaire (SPQ). Items are grouped into four distinct dimensions: positive symptoms (N = 45), negative symptoms (N = 19), disorganized symptoms (N = 13) and general symptoms (N = 15). Sociodemographic data comprised age, sex, years of education and SES. The latter was classified according to the IBGE (Instituto Brasileiro de Geografia e Estatística; www.ibge.gov.br). According to the Brazilian Association of Research Enterprises (www.abep.org), reported income may differ from actual income in community surveys. As such, we used a proxy scoring system that accounts for house and neighborhood infrastructure (paved streets, piped water, number of bathrooms in the household, presence of housekeepers, etc.), as well as the family’s patrimony (number of cars, televisions, refrigerators, etc.) to rank individuals into IBGE’s socioeconomic classes (A is the highest class, and D is the lowest class). Further information about the study is detailed elsewhere (Loch et al., 2017).
Participants with scores higher than 18 on the PQ’s positive subscale were invited to participate in the study’s second phase, which was conducted at the Institute of Psychiatry, University of Sao Paulo. Although the suggested threshold for an SIPS diagnosis ranges from 8 to 14 on the positive subscale (Loewy et al., 2005), other studies suggested a score as high as 18 on that subscale for UHR detection (Rietdijk et al., 2014). Two hundred thirty-six individuals agreed to participate; a group of psychiatrists experienced in the field of psychosis assessed participants’ UHR status using the SIPS.
Briefly, the SIPS and the Scale of Prodromal Symptoms (SOPS) (McGlashan et al., 2001) are structured diagnostic interview instruments used to diagnose three prodromal syndromes for psychosis: brief intermittent psychotic symptoms syndrome (BIPS, experience of frankly psychotic symptoms that do not meet sufficient criteria for a full psychotic episode), genetic risk and deterioration syndrome (GRD, the presence of a first-degree relative with any psychotic disorder or personally meeting the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria for schizotypal personality disorder and experiencing a drop in global functioning) and attenuated positive symptom syndrome (APS, attenuated psychotic symptoms that have not yet reached a psychotic level) (Miller et al., 2003). The SOPS contains four subscales for positive, negative, disorganization and general symptoms. For the positive subscale, items are separated into P1 (unusual thought content/delusional ideas), P2 (suspiciousness/persecutory ideas), P3 (grandiosity), P4 (perceptual abnormalities/hallucinations) and P5 (conceptual disorganization). The SIPS also includes the Schizotypal Personality Disorder Checklist (American Psychiatric Association, 1994), a family history questionnaire (Andreasen et al., 1977) and the Global Assessment of Functioning scale (Hall, 1995).
After the assessment, 98 individuals were classified as UHR individuals, 134 as controls and four as having a psychotic disorder. The final sample consisted of individuals with complete information on the Childhood Trauma Questionnaire (CTQ): 87 UHR individuals and 115 controls.
Childhood trauma evaluation
We used the short version of the 28-item self-report CTQ (Bernstein et al., 2003), which was translated into Portuguese (Grassi-Oliveira et al., 2006). The CTQ showed good consistency in assessing the five trauma dimensions: emotional abuse, physical abuse, sexual abuse, emotional neglect and physical neglect. According to the CTQ (Bernstein et al., 2003), sexual abuse is defined as ‘sexual contact or conduct between a child younger than 18 years of age and an adult or older person’. Physical abuse is defined as ‘bodily assaults on a child by an adult or older person that posed a risk of or resulted in injury’. Emotional abuse is defined as ‘verbal assaults on a child’s sense of worth or well-being or any humiliating or demeaning behavior directed toward a child by an adult or older person’. Physical neglect is defined as ‘the failure of caretakers to provide for a child’s basic physical needs, including food, shelter, clothing, safety, and health care’. Poor parental supervision is also included in this definition if it places children’s safety in jeopardy. Emotional neglect is defined as ‘the failure of caretakers to meet children’s basic emotional and psychological needs, including love, belonging, nurturance, and support’. Each trauma dimension presents traumatic situations that might have occurred during childhood, and subjects must rate their frequency using a 5-point-Likert-type scale (1 = never true, 2 = rarely true, 3 = sometimes true, 4 = often true, 5 = very often true).
Statistical analysis
Mean scores were calculated for each of the CTQ’s five subscales for each individual, and the scores of UHR individuals and controls were compared. We used the Kolmogorov–Smirnov and Shapiro–Wilk tests to evaluate the distribution of childhood trauma scores as nonnormal, so the nonparametric test and independent-samples Mann–Whitney U test were employed to determine whether childhood trauma scores differed between UHR individuals and controls. Because SES and sex may affect both CM and the UHR state, and CM may affect the UHR state, we used path analysis to assess direct and indirect effects of sex and SES on prodromal psychosis psychopathology. To better assess psychopathology, scores on the five positive items of the SOPS were included in the model, along with CTQ subscale scores, sex, and SES. Path coefficients were indicated with standardized regression coefficients (β) and standard errors (SEs). SPSS 23.0 and Mplus 1.5 for Mac were used.
Results
Sample characteristics are depicted in Table 1. Three CM dimensions showed significantly higher scores in UHR individuals than in controls: physical abuse (MEAN RANK: controls = 93.81, UHR = 111.67; p = .027), sexual abuse (mean rank: controls = 94.67, UHR = 110.52; p = .007) and emotional abuse (mean rank: controls = 85.93, UHR = 122.09; p < .001). No differences were found for physical and emotional neglect. Mean age, years of education, sex and social class did not differ between UHR individuals and controls.
Sociodemographic and clinical data.

SD: standard deviation; UHR: ultra-high risk for psychosis; SIPS: Structured Interview for Prodromal Syndromes.
Bold values indicate significant differences.
The path analysis conducted with the controls showed no significant results and is not illustrated. The path analysis model conducted with the UHR sample is depicted in Figure 1. Sex and SES did not have a significant direct effect on SIPS positive symptoms (Ps) and significantly worsened the model. As such, their direct effects were retracted from the final model, which then showed good fit indices (Figure 1; χ2 test p = .515, comparative fit index (CFI) = 1.000, root mean square error of approximation (RMSEA) = .000 and standardized root mean square residual (SRMR) = .031).
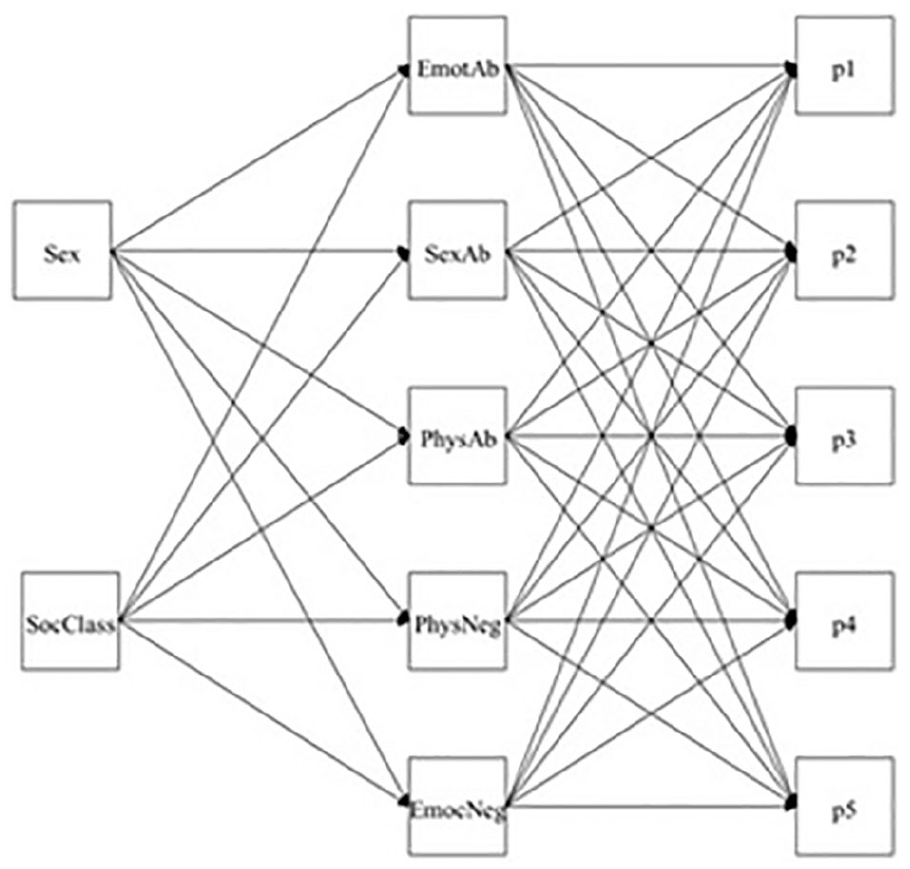
Path analysis model.
Regarding statistically significant correlations in the path analysis model, physical and emotional neglect negatively correlated with grandiosity symptoms (P3) (β = −0.423, SE = 0.15, p = .005 and β = −0.309, SE = 0.13, p = .017, respectively), physical abuse correlated with perceptual abnormalities/hallucinations (P4) (β = 5.918, SE = 1.77, p = .001) and physical neglect correlated with conceptual disorganization (P5) (β = 0.117, SE = 0.05, p = .026) (Figure 2).
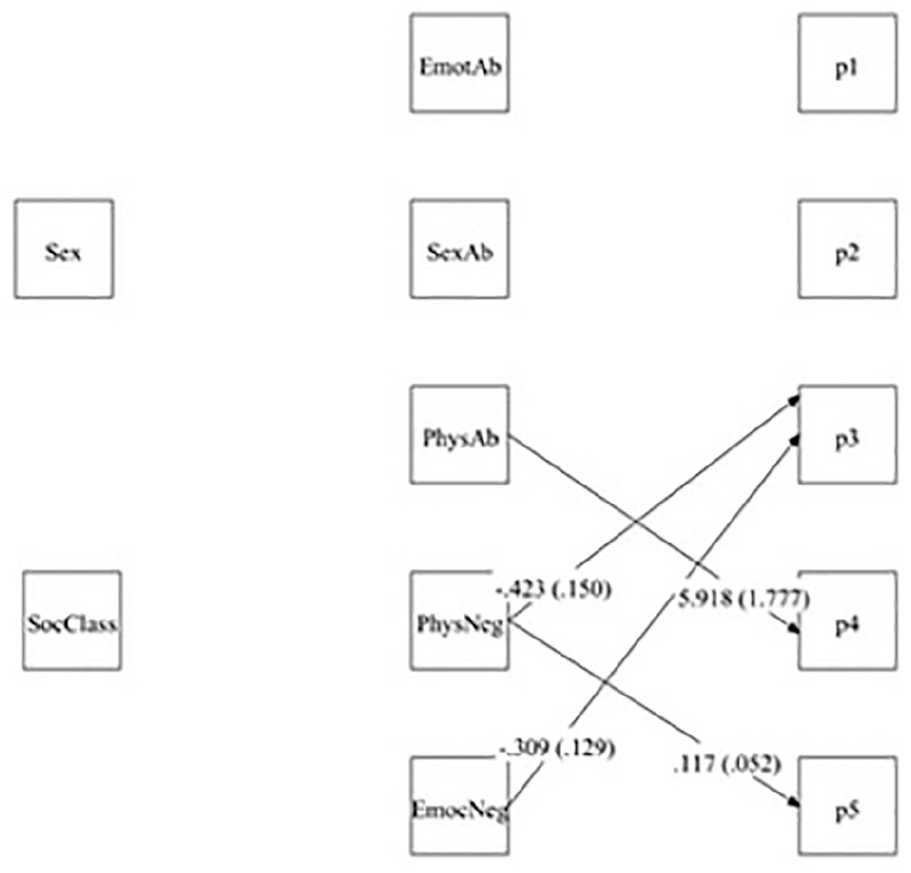
Path analysis (only significant correlations shown, p < .05).
Discussion
Our findings are in accordance with previous literature and correlate CM – emotional abuse, physical abuse and sexual abuse, physical neglect and emotional neglect – with UHR status. Furthermore, in UHR individuals, physical abuse correlated with perceptual abnormalities, and physical neglect correlated with disorganized speech/thought, whereas physical and emotional neglect negatively correlated with grandiosity symptoms. Contrary to our initial hypotheses, we found no correlation between SES status and sex with CM or UHR symptoms.
Our study contributes to the growing body of evidence in the literature that relates CM to the risk of developing a psychotic disorder. Varese et al. (2012) estimated that exposure to childhood adversity and trauma increased the risk of psychosis by 2.8 times and that approximately one-third of psychosis cases could be reduced if these adversities were eliminated. Similarly, UHR individuals presented elevated rates of CM similar to those found in schizophrenia patients (Kraan et al., 2015). The traumagenic neurodevelopmental model of psychosis proposed in 2001 provides a possible mechanism through which CM provokes psychosis onset. Early exposure to CM could enhance stress reactivity and lead to a deregulation in the hypothalamic–pituitary–adrenal axis and the dopaminergic system. After years of deregulation, nonhostile signals from the environment could be received as potential threats and provoke suspicion of others and paranoia, for example (Read et al., 2001, 2014).
In our study, emotional, sexual and physical abuse were significantly correlated with UHR status. Previous findings support these specific CM subtypes’ relationship with UHR, and emotional and physical abuse are the most prevalent among UHR individuals (Peh et al., 2019). Furthermore, emotional abuse (Kraan et al., 2018) and sexual abuse (Thompson et al., 2014) were proposed as predictors for transition to psychosis.
The positive correlation between physical abuse and perceptual abnormalities is in line with a study that analyzed CM subtypes and found an association between physical abuse during childhood and higher intensity of perceptual abnormalities (Velthorst et al., 2013). A recent meta-analysis also supported the correlation between CM and hallucinations severity (Bailey et al., 2018). As such, a relationship between traumatic experiences and hallucinations has been proposed in which dissociative symptoms are a halfway experience that connects both (Bailey et al., 2018; Pilton et al., 2015). Some studies that evaluated nonclinical samples, as in the present study, also found a correlation between traumatic experiences in childhood and proneness to hallucination and hearing voices (Bellido-Zanin et al., 2018; Berry et al., 2018). A comprehensive theory that integrates biological mechanisms – impairments to the hypothalamic–pituitary–adrenal axis and stress regulation – and psychological mechanisms – negative beliefs about the self and others (Garety et al., 2001; Morrison, 2001) and the belief that paranoia is a helpful survival strategy (Morrison et al., 2005) – is needed to better explain how CM leads to later psychotic symptoms. Nevertheless, for now, the traumagenic neurodevelopmental model of schizophrenia hypothetically integrates the complexities of biological predisposition, psychological aspects and environmental expositions with CM (Read et al., 2001, 2014).
Compared to physical and sexual child abuse, much less is known about the effects of emotional and physical neglect (Taillieu et al., 2016). Unfortunately, neglect is even less studied in LMIC countries (Stoltenborgh et al., 2013). Nevertheless, compelling evidence indicates worse mental health outcomes for children exposed to nonsupportive environments (Mansueto et al., 2019; Sonuga-Barke et al., 2017; Taillieu et al., 2016), and animal studies support these findings (Mela et al., 2015). Recent studies described neglect as a risk factor and modulative agent for phenotype presentation and course of disease in bipolar disorder (Aas et al., 2016; Levandowski & Grassi-Oliveira, 2018). As such, various forms of childhood neglect could lead to chronic feelings of worthlessness and low self-esteem, which could partly explain the negative correlation we found between physical and emotional neglect to grandiosity symptoms.
Some evidence of an association between trauma and depressive symptomatology was found in a large longitudinal study of patients with psychosis, their siblings and control subjects (Van Dam et al., 2015). In another study that evaluated major depression, physical and emotional neglect predicted a less favorable course for depressive symptoms; the former was associated with a slower rate of depression remission and the second predicted a higher rate of recurrence (Paterniti et al., 2017). Despite the existence of such data associating neglect suffered during childhood with depressive symptomatology, further studies are needed to specifically elucidate the link we found in the present sample.
We found no association between sociodemographic variables and CM subtype or UHR status. Regarding sex, some evidence from developing, non-Western countries indicated no sex-related effect on CTQ estimates (Fu et al., 2018; Viola et al., 2016). A well-established association between female sex and sexual abuse in Europe and the United States was not present in Balkan countries (Nikolaidis et al., 2018), South Africa (Meinck et al., 2017) and Saudi Arabia (Al-Eissa et al., 2015; Ghaffar et al., 2018). Lower SES could theoretically lead to parental stress, increasing the risk of CM (Anderson, 2008; Deater-Deckard et al., 1996; Dodge et al., 1994; Guterman et al., 2009; Stith et al., 2009), but these associations were not observed in our sample. However, some caution is necessary when generalizing results obtained from developed countries to LMIC countries (Stoltenborgh et al., 2015). Besides the paucity of data in these scenarios, subtypes of CM, such as physical abuse, could be underestimated in LMIC because some cultures use physical punishment as a normative way to discipline children (Gracia & Herrero, 2008; Richter et al., 2017).
We found no correlation between SES and UHR status, an association suggested for high-income countries (Fusar-Poli et al., 2017). However, there is evidence against this association, such as a study of a birth cohort in which deprivation and inequality at birth were not associated with a higher risk of psychosis (Solmi et al., 2020). Furthermore, SES can be seen as a confounding factor for ethnicity and the risk of developing psychosis, as SES is a possible marker of some important adversities for the development of psychotic conditions (Kirkbride et al., 2008). In addition, having a lower SES in an LMIC may not change protective factors, such as family and social cohesion (Avasthi, 2010).
As a strength of this study, conducting an assessment on CM and the possible implications in UHR in São Paulo City is of remarkable importance given the cultural and geographical peculiarities of Sao Paulo, the largest South American city. Epidemiological data assessing psychosis in São Paulo City have already disclosed high prevalent rates of psychotic symptoms (Andrade et al., 2002; Loch et al., 2011), and the relationship to a lower income (Loch et al., 2017). But there is still a great gap in the literature about the relationship between CM and mental disorders in Latin American environments (Barbosa et al., 2014; Scomparini et al., 2013). Furthermore, though CM was reported to be high in Brazil, when compared to other countries, there is still the concern of underreporting of CM (Zanoti-Jeronymo et al., 2009). As such, our study points to the importance of addressing CM.
This study had some limitations. First, we evaluated individuals presenting higher scores on the PQ, a screening questionnaire applied by lay interviewers. Consequently, the risk of false-positive or false-negative results was higher. However, the proportion of false positives was relatively low after the clinical evaluation, proving the adequacy of using the PQ applied by lay interviewers as a screening instrument. Second, CM was quantified using the self-completion CTQ, which incurs a potential recall bias. Assessing an a priori nonclinical sample not characterized by help-seeking behavior might reduce this bias. Third, this is a transversal evaluation, so follow-up assessments are needed to better understand the mechanisms and potential causal roles revealed herein. Fourth, childhood traumatic experiences comprise a wide range of adversities, not all of which are discussed in this study. Additional adversities include collective violence, accidents/injuries, parental mental health, parental divorce and peer victimization and bullying, which are already associated with an increased risk of psychotic experiences (Baudin et al., 2017; McGrath et al., 2017; Sweeney et al., 2015).
In conclusion, this is the first Brazilian study to focus on non-help-seeking individuals at high risk of psychosis and childhood trauma. Our findings highlight the importance of evaluating early life experiences, especially CM. More importantly, we seek to address the profound lack of Latin American studies on CM and psychosis, and, in accordance with the extensive literature on the subject, our study corroborates a possible association between CM and the development of psychotic symptoms. This information, along with other clinical and epidemiological criteria, could help public health agencies and practitioners develop adequate treatment and management techniques to prevent the conversion of UHR individuals to a fully psychotic state. Further studies in this field should address the impact of detection and prevention of early life adversities across the life span and their possible impact on psychosis incidence, prevalence, severity and burden in LMICs.
Footnotes
Acknowledgements
We would like to thank IPSOS Brasil for the field work in conducting the interviews. The Laboratory of Neuroscience LIM27 receives financial support from the Associacao Beneficente Alzira Denise Hertzog da Silva.
Conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Collegium Helveticum, Zurich (Grant #: INTL 15 0360-v3), Switzerland, and by Fundaçao de Amparo a Pesquisa do Estado de Sao Paulo (FAPESP) (Grant #: 2016/09069-1), Brazil. The sponsors had no influence on the design of the study; on the collection, analysis and interpretation of data; on the writing of the manuscript; or on the decision to submit the manuscript for publication.