
Abstract
Aim:
To study the sleep and mental health of chronic insomnia patients in China during coronavirus disease in 2019 (COVID-19) epidemic.
Methods:
A total of 764 patients with chronic insomnia were included in this study. From 17 January 2020 to 24 January 2020, insomnia, anxiety and physical symptoms were evaluated online, and they were followed up for 4 and 8 weeks. Main outcomes and indicators were assessed using the Pittsburgh Sleep Quality Index (PSQI) and each factor score, the General Anxiety Disorder-7 (GAD-7) and the Patient Health Questionnaire-15 (PHQ-15), respectively. In addition, insomnia, anxiety and physical symptoms were assessed at baseline and at the end of fourth and eighth weeks. Wilcoxon signed rank test was used to compare the changes in patients’ scale scores at different time points.
Results:
Among the 764 participants, there were 755 and 738 evaluators who completed the fourth and eighth weeks, respectively, and the questionnaire completion rates were 98.82% and 96.60%, respectively. Among them, there are 459 (60.0%) aged 41–60 years old, 546 (71.5%) women, 218 (28.5%) men and 313 (41%) college degrees. After 8 weeks of follow-up, the differences in sleep status, anxiety symptoms and physical symptoms were statistically significant. Among the factors of PSQI, there were differences in subjective sleep quality, sleep latency, sleep duration, sleep disturbance (disorder), sleep efficiency and daytime function. At 4 weeks of follow-up, there was a statistically significant difference in the use of hypnotic drugs; at 8 weeks of follow-up, there was no statistically significant difference in the use of hypnotic drugs.
Conclusion:
Under the influence of the COVID-19, the sleep status and anxiety of patients with chronic insomnia are affected by the epidemic.
Introduction
Since the end of December 2019, a case of pneumonia caused by a new coronavirus disease in 2019 (COVID-19) has been reported in Wuhan, China (N. Chen et al., 2020), which is spreading at home and abroad. New pneumonia is similar to Severe Acute Respiratory Syndrome (SARS). Although the actual transmission route is still unclear, it can be transmitted to humans through intermediate hosts such as bats. As more and more patients who have not been exposed to the animal market were still ill, and even infections have appeared in medical staff (Huang et al., 2020), indicating that there is human-to-human transmission.
According to the Announcement No. 1 issued by the National Health Commission, New Coronary Pneumonia was included in the Class B infectious diseases as stipulated in the Law of the People’s Republic of China on the Prevention and Control of Infectious Diseases, and prevention and control of Class A infectious diseases were adopted (Disease Prevention and Control Bureau, National Health Commission of the People’s Republic of China, 2020). The World Health Organization (WHO) also announced that the COVID-19 epidemic was regarded as a public health emergency of international concern (Mahase, 2020). Many provinces and cities across the country have initiated major public health emergencies with a Class I response and have entered a state of prevention and control of new coronary pneumonia. The Chinese government has taken active and effective measures to control the epidemic, set up designated hospitals nationwide to fully treat patients with new coronary pneumonia and ordered the blockade of Wuhan on 23 January 2020, which is an unprecedented measure (C. Y. Wang et al., 2020). Restrictions on the movement of people, segregation of homes for all residents, work stoppages and school suspensions nationwide and all entertainment venues are closed. As of 24:00 on 31 March 2020, China had a total of 81,554 confirmed cases and a total of 3,312 deaths (National Health Commission of the People’s Republic of China). Many countries around the world have also outbreaks, which spread all over the world. Most people in the country receive information at home from the Internet, including untrue reports and alarmist rumors, causing widespread panic and anxiety. Related studies have shown that survivors of acute infectious diseases (such as SARS) can cause anxiety, depression, stress and post-traumatic stress disorder (Hawryluck et al., 2004; Wu et al., 2005a, 2005b). In addition, the current transmission route and treatment of new coronary pneumonia are still unclear. In the case of an uncontrolled epidemic, previous studies have shown that emotions such as anxiety, stress and self-efficacy affect sleep quality (X. F. Chen et al., 2019; Dahlgren et al., 2005). On 2 February 2020, the State Council of China announced that it would open a nationwide psychological assistance hotline to provide help during the outbreak, but there were few specific psychological measures for people with chronic diseases.
About one-quarter of current adults are dissatisfied with their sleep time or sleep quality, and the diagnostic criteria for insomnia are about 6%–10% (Ohayon & Reynolds, 2009). At present, the main treatment for chronic insomnia is drug therapy. Due to the epidemic situation, it is difficult to come to the hospital in time for standardized treatment. Related studies have shown that the longer the insomniac in chronic insomniacs, the greater the possibility of the use of hypnotic drugs (Yang et al., 2019). This study mainly observed the sleep and emotional status of chronic insomniac patients at home during the epidemic to provide experience for home management of chronic diseases under public health events.
Materials and methods
Ethical recognition
This research was conducted according to the ‘Helsinki Declaration’. All participants verbally agreed and signed electronic consent forms. This study was approved by the Ethics Committee of Hangzhou Seventh People’s Hospital, Mental Health Center, School of Medicine, Zhejiang University. The ethics reference number was 2019009. All participants were informed that this study was a voluntary project that could be terminated at any time.
Research subjects
The case report rate starting on 17 January 2020 was considered to be 21 times higher than in the first half of January 2020 (Zhao et al., 2020), so this study was included from 17 January 2020 to 24 January 2020. For the patients evaluated on the ‘Good Sleep 365’ platform, 764 chronic insomniacs were randomly selected by the system. All the enrollees were patients who had visited our outpatient clinic and diagnosed chronic insomnia by two psychiatrists. Inclusion criteria were as follows: (1) meets the diagnostic criteria for chronic insomnia in Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5; American Psychiatric Association, 2013); (2) education level: junior high school and above, age 18–65 years; (3) skilled use of ‘Good Sleep 365’ computer application (application, APP). Good Sleep 365 is an application software for sleep assessment, intelligent intervention and rehabilitation training. Exclusion criteria include (1) secondary insomnia or comorbid insomnia caused by various mental diseases, especially insomnia caused by depression or anxiety or comorbid insomnia; (2) patients taking regular antipsychotic drugs; (3) insomnia caused by taking psychoactive drugs or physical diseases; (4) patients with the recent history of business trips and traveling in the epidemic area, or any suspected or diagnosed patient contact history, and recent symptoms of colds and fever.
Research methods
The patients included in the study were all chronic insomnia patients who followed up with good sleep 365APP network. The patients with informed consent and willingness to cooperate were taken an online assessment questionnaire. Patients understood the contents of the questionnaire, filled in general situation questionnaires such as age, gender and education level accurately and completed Pittsburgh Sleep Quality Index (PSQI) Questionnaire, General Anxiety Disorder-7 (GAD-7) and Patient Health Questionnaire-15 (PHQ-15) assessment.
General questionnaire
The research staffs it by themselves. The main contents include name, gender, age, occupation, residence, contact information, education level and other general conditions.
PSQI Questionnaire
It is mainly used to assess the sleep quality of patients in the past month and has been proven to have good reliability and validity (Liu et al., 1996), in which 18 items constitute seven factors (Buysse et al., 1991). Each factor is scored on a scale of 0–3, with a total score of 21 points. The higher the score, the worse the sleep quality. Through this table, you can understand the patient’s sleep quality, time to fall asleep, sleep duration, sleep efficiency, sleep disorders, hypnotic drugs and daytime function; 5–9 points are mild, 10–14 points are moderate and 15–21 points are severe.
GAD-7
It is mainly used for the screening of general anxiety and the evaluation of symptom severity (Spitzer et al., 2006). It has been proved to have good reliability and validity (He et al., 2010) and consists of seven items. Each item has a score of 0–3 points and a total score of 21 points; 0–4 points are no anxiety, 5–9 points are mild anxiety, 10–14 points are moderate anxiety and ⩾15 points are severe anxiety.
PHQ-15
It mainly evaluates the degree of troubles caused by various common physical symptoms or symptom groups in the past 4 weeks (Kroenke et al., 2002). It is an independent self-rating scale for somatic symptom groups. It consists of 15 items, with a score of 0–2 points for each item, and 30 points total. The higher the score, the more severe the physical symptoms. 0–4 are classified as no physical symptoms, 5–9 are classified as mild physical symptoms, 10–14 are classified as moderate physical symptoms and 15–30 are classified as severe physical symptoms.
Statistical analysis
SPSS 25.0 software was used for analysis, and the rank sum test was used to compare the changes in PSQI, GAD-7 and PHQ-15 at 0, 4 and 8 weeks and to compare changes in sleep and anxiety at different time points during the epidemic. Because the scale data are not normally distributed, Wilcoxon signed rank test was used to compare the differences in scale scores of patients at different time points. We used a fixed order (all compared with week 0) for multiple comparisons between groups. To reduce type I errors, we used the α value of 0.025 for comparison.
Results
Basic situation
A total of 800 persons were questionnaire surveyed, 32 unqualified questionnaires were excluded, 768 people were enrolled and the response rate was 96%. Among them, 20 people failed to complete the questionnaire and 12 people had incomplete basic information. There were 755 and 738 people who completed 4 and 8 weeks, respectively, and the questionnaire response rate was 98.82% and 96.60%, respectively. Among them, there were 546 females (71.50%) and 218 males (28.5%); they aged 18–65 years the average age of females was (46.70 ± 11.32) years and the average age of males was (44.66 ± 13.59) years; the difference was statistically significant (F = 10.30, p < .01).
General information of patients with chronic insomnia
There are 764 patients with chronic insomnia, including 313 (41%) with university education and 459 (60.0%) aged 41–60 years old (Table 1).
General information of patients with chronic insomnia.

Comparison of severity of insomnia and anxiety in patients with chronic insomnia
After 8 weeks of follow-up, the difference in the degree of insomnia in patients with chronic insomnia was statistically significant (p < .05); the anxiety degree in patients with chronic insomnia was statistically significant (p < .05) (Table 2).
Severity of insomnia and anxiety in chronic insomnia patients at different times.

IQR: interquartile range; PSQI: Pittsburgh Sleep Quality Index; NA: not applicable; GAD-7: General Anxiety Disorder-7; PHQ-15: Patient Health Questionnaire-15.
Category p value refers to each category versus the baseline.
Comparison of the scores of the factors in the PSQI questionnaire among chronic insomniacs
After 8 weeks of follow-up, there were statistically significant differences in subjective sleep quality, sleep latency, sleep duration, sleep disturbance (disorder), sleep efficiency and daytime function in PSQI of chronic insomniacs (p < .05). At 4 weeks of follow-up, there was a statistically significant difference in the use of hypnotic drugs; at 8 weeks of follow-up, there was no statistically significant difference in the use of hypnotic drugs. (Table 3).
PSQI factors of chronic insomnia patients at different time points.
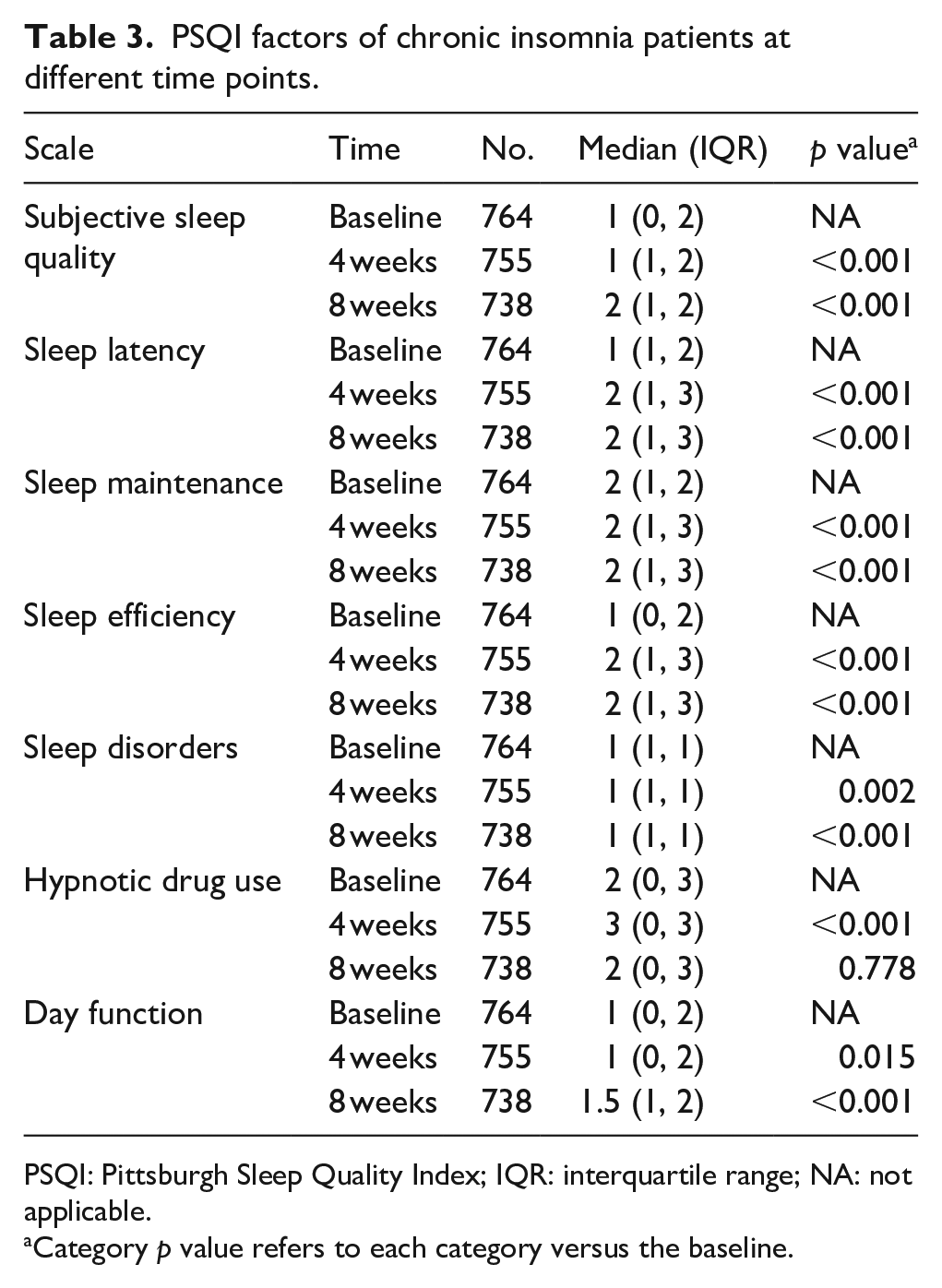
PSQI: Pittsburgh Sleep Quality Index; IQR: interquartile range; NA: not applicable.
Category p value refers to each category versus the baseline.
Discussion
The purpose of this study was to investigate the sleep status and anxiety of Chinese chronic insomniacs during home isolation in the COVID-19 epidemic from 17 January 2020 to 24 March 2020. The PSQI was used to assess sleep quality, and the GAD-7 and PHQ-15 were used to assess anxiety and physical symptoms. Using rank sum test analysis to evaluate differences at different time points. The 764 participants in this study were mostly female (71.50%), with an average age of 46.12 ± 12.04 years.
In this study, during the isolation period of chronic insomnia patients, the average scores of PSQI, GAD-7 and PHQ-15 were 11.28, 3.26 and 4.99 during the 8-week follow-up period, which was much higher than the baseline score, indicating worse sleep quality, higher anxiety scores and increased severity of somatic symptoms. All these suggest that during the epidemic, we need to pay attention to not only the physical health, but also the mental health of patients with chronic diseases (Dong & Bouey, 2020). The viral transmission route, the uncertainty of the incubation period and the possible existence of asymptomatic transmission have caused people’s fear and anxiety about unknown diseases. This unprecedented measures of lockdown of Wuhan and home isolation across the country, coupled with the increasing number of patients, the shortage of medical supplies and even reports of successive infections by medical and health workers, has exacerbated the anxiety and pressure of the people. Studies have shown widespread fear and over reactivity triggered by SARS in 2003 and Ebola virus disease outbreaks in 2014, and it prevented effective infection control (Person et al., 2004; Shultz et al., 2016). The influence of anxiety on sleep quality has been clearly confirmed, which make it difficult to fall asleep and interrupt the continuity of sleep, and wake up frequently from sleep (Alvaro et al., 2013; Johnson et al., 2006). Stress is also closely related to sleep quality (Reeth et al., 2000), and an increase in stress can lead to a decrease in sleep quality (Jarrin et al., 2014).
Good sleep quality not only helps patients adjust their mentality during home isolation, but also enhances immunity against viruses (Lange et al., 2010). This study showed that during the epidemic, the sleep latency, sleep duration, sleep efficiency and daytime function of PSQI were affected. Sleep restriction has been proven to be effective in insomnia patients (Holbrook et al., 2000). During the isolation period, patients have irregular work schedules and rest time. It is difficult to limit rest time, making it difficult to fall asleep. What’s worse, it is difficult for patients to fall asleep when they should fall asleep, which affects sleep latency and sleep continuity, thus affecting sleep quality. Patients sleep poorly at night and their social functions are affected during the day. At present, insomnia treatment is mainly drug treatment. Follow-up found that the use of hypnotic drugs at 4 weeks was significantly more than the initial period (p < .001), while the difference in the use of hypnotic drugs at 8 weeks was not statistically significant. The use of hypnotic drugs is basically consistent with the fluctuation of the epidemic. In February, the number of cases increased sharply. During home isolation, patients were worried and panic obviously, which increased the possibility of the use of hypnotic drugs. Around 8 weeks, the epidemic in China gradually improved.
During quarantine, the whole house was isolated. Chronic insomnia patients had more anxiety symptoms than before. On one hand, they were affected by the epidemic. The virus broke out globally, and many cases of asymptomatic infections were reported. Worried about the virus lurking around. On the other hand, due to home isolation and limited range of activities, patients were passively discontinued, and the short-term withdrawal reaction may make patients worsen their insomnia and anxiety symptoms. During home isolation, all patients in the group were difficult to go out to dispense, which may reduce the use of hypnotic drugs. If the medicine is stopped suddenly, 15%–44% would have withdrawal symptoms such as anxiety, insomnia, tinnitus and gastrointestinal reactions (Ashton, 1991), making it more anxious.
The patients’ panic about the epidemic is mostly a lack of knowledge about disease prevention and control. Studies have shown that in the face of major emergencies (Y. N. Wang & Luo, 2003; Zheng, 2003), most of the public lack the ability to analyze and distinguish rationally. To eliminate panic and rumors, the most effective way is to disclose information. A timely, credible and accurate information release system is helpful to guide the public to eliminate panic, calmly treat the epidemic and truly play an early warning role. Through distance education and training, you can use the network to quickly publicize the epidemic situation and the main points of prevention and control and provide timely information to ordinary people. This mode has proved to be effective during the SARS period in 2003 (P. Wang, 2003). In future research, we can further observe the effect of using network to remotely treat chronic insomnia patients under public health events (Wright & Caudill, 2020).
As with all studies, this study had some limitations. Anxiety can affect sleep quality, and poor sleep can also cause anxiety, and even increase anxiety. The current research is difficult to determine the causal relationship, and further research will be needed to determine causality. In this study, all of these were evaluated through a subjective scale, subjective deviations, and objective indicators should also be considered. For example, sleep quality can be assessed by polysomnography.
Conclusion
Given that people already know the close link between poor sleep and severe anxiety during the epidemic, interventions are needed to improve the sleep quality of patients with chronic insomnia. These results show that the use of existing sleep hygiene, sleep restriction and other cognitive behavioral treatments, combined with a wider range of methods, can also enable chronic insomniacs to better manage their sleep during home isolation. This provides an opportunity to use the Internet to remotely promote chronic disease patients to strengthen self-management in the event of an acute public health event.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by funding from the Hangzhou Science and Technology Commission project named ‘application research of insomnia diagnosis and treatment technology based on big data’ (project number: 20191203B119) and the Zhejiang Nature Foundation’s public welfare project named ‘insomnia assisted diagnosis system based on medical image and artificial intelligence analysis’ (project number: LDF20H090004).