
Abstract
Background:
Nonsuicidal self-injury (NSSI) is being increasingly identified as an important emerging mental health issue in the West. Yet, NSSI has not been adequately studied in clinical and nonclinical contexts in countries like India.
Aim:
The aim of this study was to compare different features of NSSI between clinical and nonclinical samples in India. We also explored if the strength of the association between NSSI and disturbances in identity formation – a risk factor that can increase vulnerability to NSSI – was similar in the two samples mentioned above.
Method:
For the clinical sample, data regarding NSSI and identity formation were collected from 100 psychiatric patients (47.0% females, mean age = 34.76 years, SD = 12.76, 17–70 years) from an outpatient/inpatient psychiatric department of a large tertiary hospital in Mumbai, India. Nonclinical data were collected from 120 young adults studying in a medical college in Mumbai, India (51.7% females, mean age = 19.7 years, SD = 2.16, 17–28 years). Information regarding NSSI and identity were collected using self-report questionnaires.
Results:
Lifetime prevalence of NSSI in the clinical and nonclinical samples was found to be around 17% and 21%, respectively. Although the prevalence of NSSI did not significantly differ between the two samples, some features of NSSI did differ between the two groups. Finally, multigroup Bayesian structural equation modeling indicated that irrespective of the type of the sample (i.e. clinical or nonclinical), consolidated and disturbed identity significantly (negative and positive, respectively) predicted lifetime NSSI. Additionally, the association between the aforementioned identity variables and NSSI did not significantly differ between the two samples.
Conclusion:
The findings of these studies highlight the need for exploring issues related to identity formation in individuals who engage in NSSI irrespective of whether they suffer from a psychiatric disorder or not.
Keywords
Nonsuicidal self-injury (NSSI) is defined as the deliberate destruction of one’s body tissue without an actual intention to die (Nock, 2009). The common forms of NSSI include self-cutting, self-hitting and self-burning. A history of NSSI is often associated with a range of mental health issues such as elevated levels of distress, anxiety, depression and eating disorder symptoms (Whitlock et al., 2006). Repeated NSSI has been associated with a higher probability of engaging in suicidal behaviors (Whitlock et al., 2006). A meta-analysis by Swannell et al. (2014) of predominantly Western studies indicates that, although the prevalence of NSSI is known to be the highest in adolescents (around 18%), around 13% of young adults and 5% of adults have a history of at least one episode of NSSI. Research indicates that the prevalence in patients with psychiatric disorders may be anywhere between 2% and 20% (Kerr et al., 2010). While NSSI is generally known to be more severe in clinical samples than in their nonclinical counterparts (Nock & Favazza, 2009), some psychiatric disorders are associated with higher rates of NSSI. For example, previous studies have indicated that more than 70% of patients with borderline personality disorder or eating disorders engage in NSSI.
As compared to the West, research on NSSI in India is limited. Gandhi, Luyckx, Maitra, and Claes (2016) identified some empirical and case studies that reported self-harming behaviors that resemble NSSI as defined in this study. However, because of inconsistent definitions of the behaviors examined, predicting the prevalence of NSSI may be difficult. Works of Bhola et al. (2017) and Kharsati and Bhola (2015) – who operationalized NSSI as it is defined in this study – indicate that the 1-year prevalence of NSSI may be around 31%–34%. If confirmed by additional research, the findings of these studies indicate that the prevalence of NSSI may be substantially higher in India as compared to Western countries. Furthermore, although NSSI in the Indian nonclinical samples seems to be getting some attention, the prevalence of NSSI in Indian clinical samples remains unknown.
Apart from research exploring the prevalence of NSSI, research is also needed to understand factors that increase vulnerability to destructive behavior. The age of onset of the first episode of NSSI has been demonstrated to be between 15 and 16 years of age (Gandhi et al., 2018). Among the host of possible developmental factors that can increase vulnerability to NSSI, disturbances in identity formation have been increasingly identified as important (Gandhi et al., 2017). The process of identity formation begins during adolescence and it continues throughout one’s life. According to Erikson’s theory (Erikson, 1968), the main developmental task of adolescents is to solve the crisis of identity synthesis versus identity confusion. Identity synthesis refers to the extent to which various aspects of one’s sense of self fit together. Achieving identity synthesis is associated with a subjective feeling of sameness and continuity across time and situations. On the other hand, the inability to enact and maintain long-term commitments and a lack of purpose and goal-directedness in life may lead to identity confusion (Schwartz et al., 2009). Although identity confusion is often associated with a range of negative outcomes like rebelliousness, depression and anxiety (Demir et al., 2009), it is rarely associated with deep-seated and chronic psychopathology. That is, identity confusion is a normative developmental disturbance rather than a diagnostic category (Erikson, 1968; Kaufman et al., 2014). Erikson (1968) also defined an extreme version of identity confusion called identity diffusion. Identity diffusion represents a sustained incoherence or extreme identity confusion, which leads to an inability to commit to a well-defined self-concept. Sustained identity diffusion has been shown to be associated with feelings of being empty, lack of authenticity, a sense of incoherence and reduced well-being (Bogaerts et al., 2018; Marcia, 2006).
Yet it should be noted that identity formation is a dynamic process. That is, as individuals age, identity resolved during adolescence can get updated according to the changes in the biological and psychological realm (Kroger, 2015). More specifically, identities that are formed during adolescence need to be flexible enough so that content and certainty of one’s identity can be adjusted if and when needed (Luyckx et al., 2006). Consequently, individuals may continue to be vulnerable to mental health issues that may arise due to identity confusion or diffusion even during adulthood (Claes et al., 2015; Sharif & Khanekharab, 2017).
In an attempt to consolidate these different conceptualizations of identity in a single theory, Kaufman et al. (2014) postulate that identity functioning may exist on a continuum that extends identity synthesis – which represents the positive and healthy end of the spectrum to severe identity disturbance – which represents the pathological extreme of lack of identity. Normative identity confusion may lie in between these two ends of the spectrum. It can be hypothesized that as one moves away from the identity synthesis end to more disturbed identities, the severity of mental health symptoms may increase as well (Kaufman et al., 2014). To capture these normative and disturbed forms of identity functioning, Kaufman et al. (2015) developed the Self-Concept and Identity Measure (SCIM). The SCIM measures three concepts: (a) Consolidated identity, like Erikson’s identity synthesis, measures the degree of self-permanency, feeling of being whole, connected to the past and certainty about oneself (Kaufman et al., 2015); (b) Disturbed identity partly captures normative identity confusion (Erikson, 1968) and lack of self-concept differentiation. Self-concept differentiation here refers to an individual’s ability to possess different personality characteristics across different social roles or contexts (Donahue et al., 1993); and (c) lack of identity subscale captures feelings of fragmentation, nonexistence and inner emptiness as described by Erikson (1968) and Marcia (2006).
Existing research indicates that NSSI may be negatively associated with the consolidated identity (synthesis) and positively associated disturbed identity (confusion; Gandhi, Luyckx, Maitra, Kiekens, & Claes, 2016). A longitudinal study by Gandhi and colleagues (2017) in adolescents indicated that the association between the aforementioned variables is likely to be bidirectional. That is, although lower identity synthesis and higher confusion may increase the probability of engaging in NSSI, repeated NSSI may in turn reduce identity synthesis and increase identity confusion. A similar pattern of associations between NSSI and identity formation has also been demonstrated in clinical samples. For example, Claes and colleagues (Claes et al., 2015) demonstrated that patients with an eating disorder who also engaged in NSSI showed significantly more identity confusion and less identity synthesis compared to patients with ED who did not engage in NSSI.
Based on the brief review presented above, several shortcomings in the existing literature on NSSI and its association with identity formation can be identified. First, research is urgently needed to determine the lifetime prevalence of NSSI not only in nonclinical samples but also in clinical samples. Second, extant research on the association between NSSI and identity (especially in cases where identity was operationalized using Erikson’s theory) has heavily focused on identity synthesis and confusion. Therefore, the association between persistent lack of identity (i.e. identity diffusion) and NSSI has remained almost unexplored. Earlier research has demonstrated moderate to strong positive relations between lack of identity and symptoms of anxiety, depression and borderline personality disorder (Bogaerts et al., 2018; Kaufman et al., 2015). Consequently, it can be hypothesized that a moderate to strong positive association may exist between NSSI and a lack of identity. Finally, although some research in the West has attempted to compare the association between NSSI and identity between a nonclinical sample and a clinical sample, such a comparison has not been attempted in an Indian context. Such a comparative approach can provide a much needed insight into the similarities and differences in the process of identity formation between a clinical and a nonclinical sample. In order to remedy some of the drawbacks identified in the previous section, this study had three major objectives. First, we investigated the prevalence (lifetime and 1 year) of NSSI in Indian clinical and nonclinical samples. Second, we investigated if mean differences in consolidated identity, disturbed identity and lack of identity could be observed between the clinical and nonclinical samples. Finally, we examined whether consolidated, disturbed and lack of identity predicted the probability of engaging in lifetime NSSI in both the clinical and nonclinical samples.
Method
Participants
Data were collected from psychiatric patients (i.e. the clinical sample) and medical students (i.e. the nonclinical sample) by means of the nonprobability sampling technique in Mumbai, India. The clinical sample consisted of 100 participants (47.0% females) from the inpatient and outpatient psychiatry department of a public tertiary general hospital. The mean age of the clinical sample was 34.76 years (SD = 12.76, 17–70 years). Based on a diagnostic interview (Lin et al., 2003) of the 100 patients, 22.0% reported to be suffering from a major depressive disorder, 17.0% suffered from an alcohol use disorder, 16.0% suffered from an anxiety disorder and 15.0% suffered from schizophrenia. Diagnosis was unknown in 26.0% of the clinical sample. The student (nonclinical) sample consisted of 120 (out of the total 150) first-year bachelor of medicine and bachelor of surgery students (51.7% females) from a government medical college. The mean age of the nonclinical sample was 19.7 years (SD = 2.16, 17–28 years).
Procedure
Between July 2017 and January 2018, patients visiting the outpatient department or admitted to the psychiatry inpatient department were invited to participate in the study if they did not meet the exclusion criteria. The exclusion criteria were as follows: (1) abnormalities evident in mental status examination that may prevent the patient from giving informed consent or prevent the participant from giving accurate information (e.g. head injury, psychosis, mania, active withdrawal, mental retardation); (2) patients with limited understanding of English, Hindi or Marathi; and (3) patients with court-appointed guardians. Patients who did not meet the exclusion criteria were provided with a study information sheet and an informed consent form (available in three languages: English, Hindi and Marathi). Researchers were available to answer any question from the participants. An additional written consent was taken from the study participants to allow their attending psychiatrist to share their clinical diagnosis with the researchers. Like the clinical participants, the medical students also had to sign a consent form before they participated in the study. The data collection procedure was completed during the college hours using paper-and-pencil self-administered standardized questionnaires. The students who agreed to participate in the study were requested to return the completed forms in a sealed envelope.
No identifying data were collected from the patients or the students who participated in the study. Consequently, it was not possible to follow up with individuals who indicated that they engaged in NSSI. However, both the patients and students were provided with contact details of mental health workers associated with the hospital as well as mental health workers who were working outside the hospital environment. This study was approved by the ethics committees of the Faculty of psychology and educational sciences (KU Leuven) and the Lokmanya Tilak Municipal General Hospital.
Questionnaires
Information regarding NSSI was collected using the modified self-injury questionnaire–treatment-related (Claes & Vandereycken, 2007). Lifetime prevalence of NSSI was investigated using a single YES/NO question (‘Have you ever injured yourself on purpose without intent to die?’). If the participants answered this question affirmatively, they were asked to indicate if they engaged in seven different forms of NSSI (i.e. scratching to draw blood, cutting superficially, cutting, bruising/hitting, burning, pricking with a sharp object and head banging). We additionally investigated if the participants were still engaging in NSSI at the time of data collection, the age of onset of first NSSI and parts of the body commonly injured. Finally, we also inquired about the degree to which the participants endorsed 18 different functions of NSSI (see Table 2 for the complete list of for functions included in the study) on a 5-point Likert-type scale ranging from 1 (not applicable) to 5 (very applicable).
Identity was investigated using the self-administered self-concept and identity measure (SCIM; Kaufman et al., 2015). The SCIM consists of 27 items that are scored on a 7-point Likert-type scale, ranging from 1 (strongly disagree) to 7 (strongly agree). As mentioned in the introduction, the scale has a three-factor structure: consolidated identity, disturbed identity and lack of identity (refer to section ‘Introduction’ for definitions). High scores on the consolidation identity subscale indicate a stronger sense of self, whereas higher scores on disturbed and lack of identity subscales indicate identity confusion and a lack of sense of self, respectively. Prior research has demonstrated that the total SCIM has a high internal consistency (Cronbach’s α = .89), test–retest reliability (α = .93, r = .88; intraclass correlation coefficient = 0.88) and adequate construct validity (Kaufman et al., 2015). Sample items and alpha coefficients of the aforementioned three subscales for both the samples included in this study can be found in Table 1.
Sample items and internal consistency coefficients (Cronbach’s alpha) of the three subscales of the SCIM for the clinical sample and the nonclinical sample.
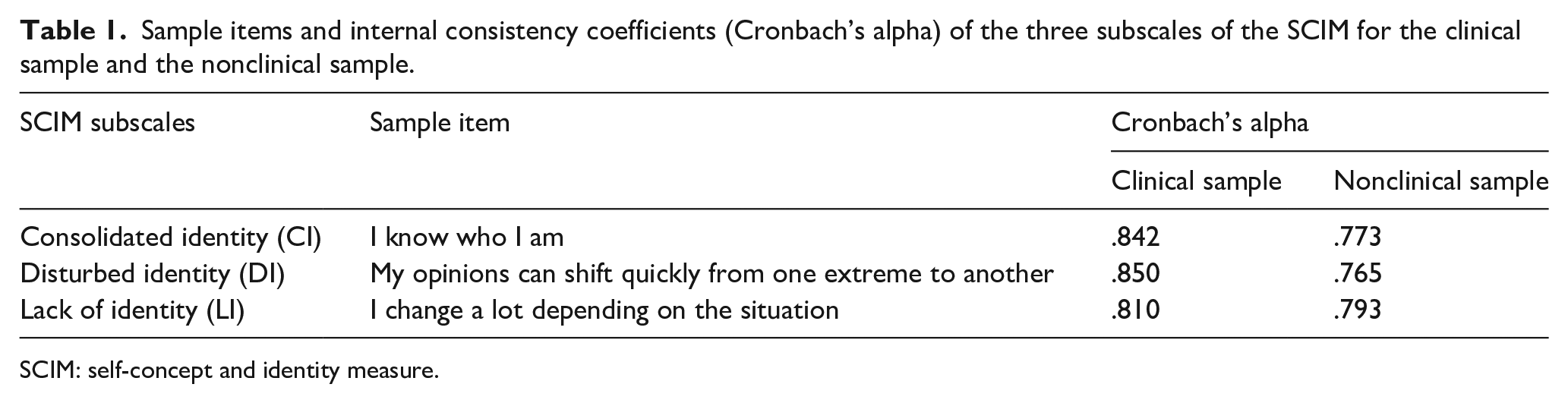
SCIM: self-concept and identity measure.
Both the questionnaires were translated from English to local languages (Hindi and Marathi) by a paid translation service. The translation and back-translation procedures were also carried out by a paid translation service. The appropriateness of the translation was verified by the first author who is fluent in Hindi, Marathi and English.
Statistical analyses
Preliminary analysis
First, we used the chi-square test of independence to investigate if the prevalence of NSSI differed significantly between the two samples. Within each sample, additional chi-square tests of independence were performed to investigate if there were significant gender differences in the lifetime prevalence of NSSI and the endorsement of methods of engaging in NSSI. We used a series of t-tests to investigate group differences in the 18 functions of NSSI. Finally, we also explored mean differences between the SCIM subscales between the clinical and nonclinical samples while controlling for age and gender using multivariate analysis of covariance (MANCOVA). All the aforementioned analyses were performed using SPSS (v25).
Multigroup path model
The associations between the consolidated identity, disturbed identity and lack of identity and lifetime NSSI were investigated using the model shown in Figure 1. This model was simultaneously tested in both the clinical and nonclinical samples using multigroup path analysis in structural equation modeling (SEM). Furthermore, a more parsimonious version of the model (i.e. a constrained model) shown in Figure 1 was tested by fixing
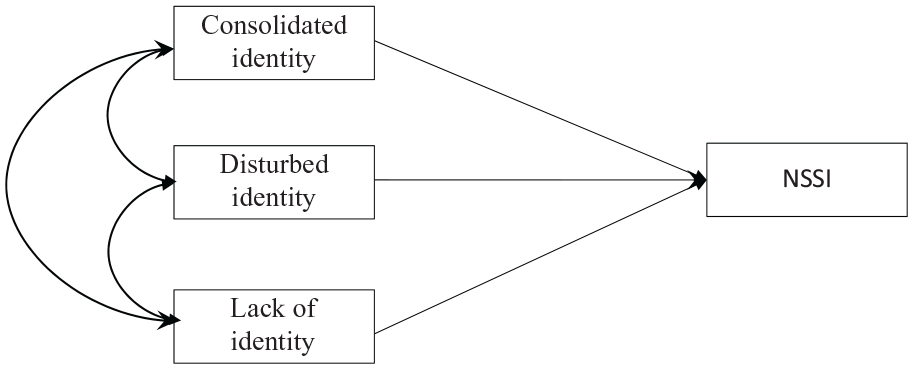
Hypothesized path model modeling the associations between the three SCIM subscales and NSSI.
Results
Preliminary analysis
The lifetime prevalence of NSSI was found to be 17% in the clinical sample and 21% in the nonclinical sample. About 5% of clinical sample and 4.17% of the nonclinical sample indicated engaging in NSSI at the time of data collection. Lifetime NSSI (χ2 = 0.755, df = 1, p = .385) and present NSSI (χ2 = 0.597, df = 1,
Mann–Whitney U tests to investigate group differences in the 18 functions of NSSI.
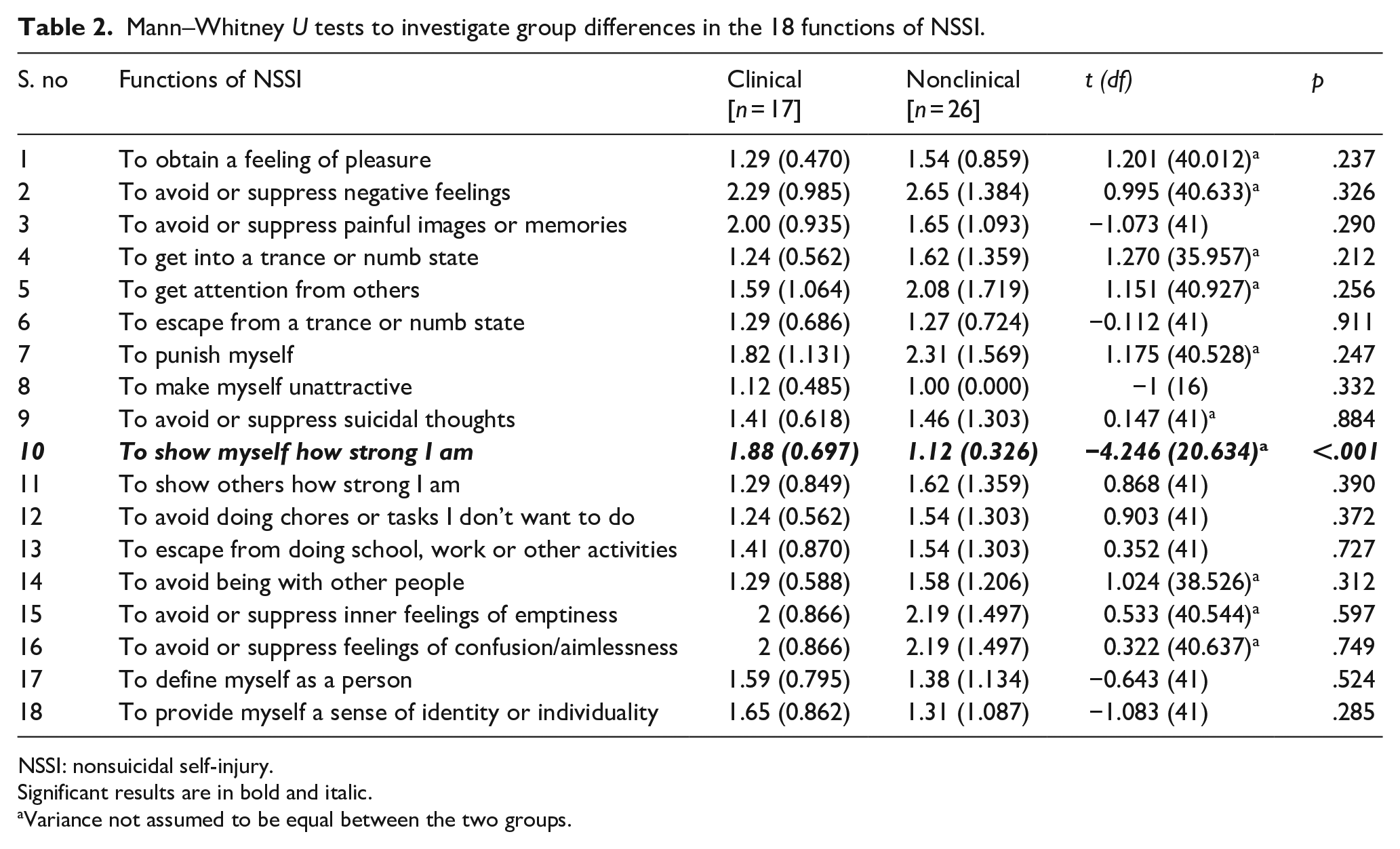
NSSI: nonsuicidal self-injury.
Significant results are in bold and italic.
Variance not assumed to be equal between the two groups.
Mean differences in subscales of SCIM
Findings of MANCOVA (Table 3) indicated that individuals from the clinical sample scored significantly lower on consolidated identity and significantly higher on the disturbed identity and lack of identity subscales as compared to the nonclinical sample.
Estimated marginal (EM) means and standard errors (SE) of the three subscales of the SCIM between the clinical and nonclinical samples when controlling for gender and age (Wilks’ Lambda = .914, F = 5.118, df = (3, 211), p = .002,
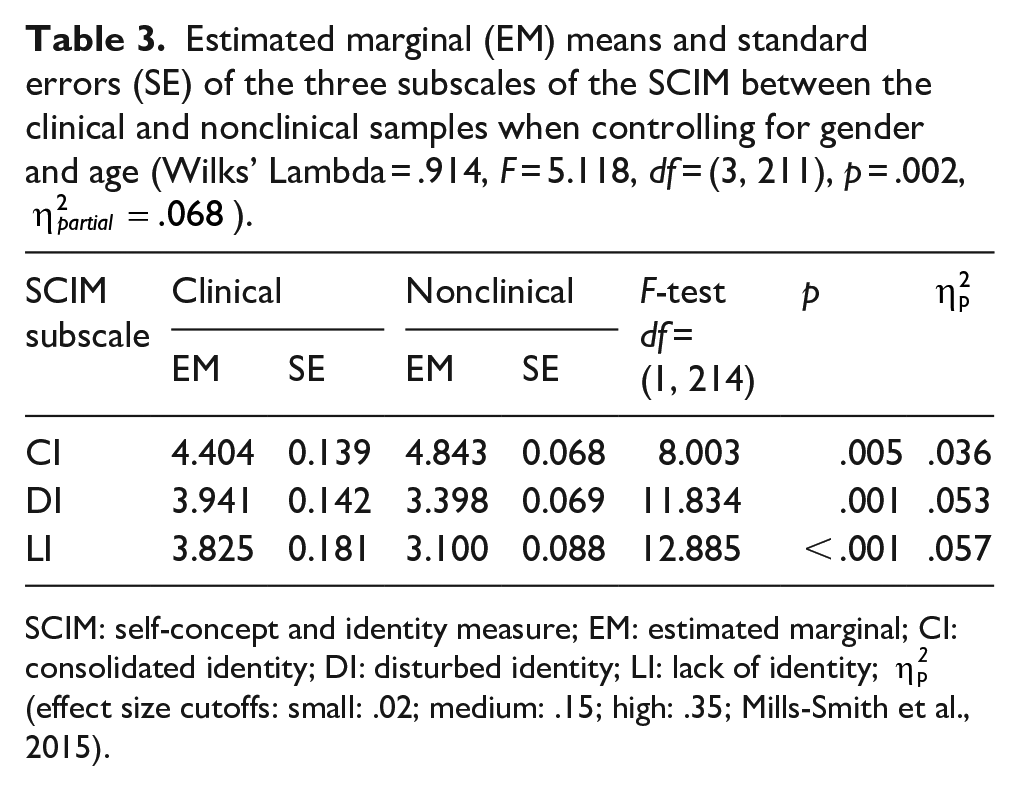
SCIM: self-concept and identity measure; EM: estimated marginal; CI: consolidated identity; DI: disturbed identity; LI: lack of identity;
Multigroup path model
The baseline model (i.e. the model shown in Figure 1 with both age and gender as covariates) had a poor fit to the data (PPP = .031; 95% CI = −1.471, 49.438). The fit of the model obtained by trimming all the covariates from the model was significantly better (PPP = .158; 95% CI = 11.212, 29.693). Next, the pathways from the consolidated identity on NSSI, disturbed identity on NSSI and lack of identity on NSSI were set equal across the two groups. The fit of the constrained model was only marginally worse than the unconstrained model without covariates (PPP = .140; 95% CI = −9.321, 30.645). Therefore, the fully constrained model was chosen as the final model best fitting the data. The fully constrained model had a PSR of 1.001 indicating that adequate convergence was achieved.
Unstandardized estimates, along with posterior SDs and 95% credibility intervals of the association between the identity subscales and NSSI in both the clinical and nonclinical samples are shown in Figure 2. In both the clinical and nonclinical samples, the association between consolidated identity and NSSI was found to be negative and statistically significant. That is, as the level of consolidated identity increased, the probability of engaging in NSSI reduced. On the other hand, the associations between disturbed identity and NSSI were found to be positive and significant. That is, as the score of disturbed identity increased, the probability of lifetime NSSI increased. Associations between the lack of identity and NSSI were found to be nonsignificant in both the samples.

Unstandardized coefficients for a fully constrained model demonstrating the associations between the SCIM subscales and NSSI in the clinical and nonclinical samples. The posterior SD and 95% credibility intervals for each of the unstandardized path coefficients are reported between the parentheses (separated by ‘;’). *Estimates were significantly different from zero.
Discussion
The key findings of this study were as follows: although lifetime prevalence and present NSSI did not significantly differ between the two samples, some phenomenological differences could be observed between the two samples. We further observed that as compared to the nonclinical sample, individuals from the clinical sample scored significantly lower on consolidated identity and significantly higher on disturbed identity and lack of identity subscales. Finally, irrespective of the type of the sample (i.e. clinical, or nonclinical), consolidated and disturbed identity significantly (negative and positive, respectively) predicted lifetime NSSI. All of these findings are discussed in the subsequent sections.
Lifetime prevalence of NSSI in the clinical and nonclinical samples was found to be 17% and 21%, respectively. The prevalence of NSSI in the clinical sample was found to fall within the range suggested by Kerr and colleagues (2010). However, the lifetime prevalence of NSSI observed in the nonclinical sample was found to be higher than to that reported in the international literature (i.e. 13%; Swannell et al., 2014). It is difficult to contextualize the findings regarding the lifetime prevalence of NSSI for the clinical and nonclinical samples found in this study within a larger Indian literature as the lifetime prevalence of NSSI has not been yet established in the Indian samples. Yet it is interesting to note that the prevalence of NSSI in the patient sample did not significantly differ from the prevalence observed in the nonclinical sample. Lack of significant differences between the clinical and nonclinical prevalence of NSSI directly contradicts findings from the international literature (Nock, 2009). A possible explanation for the lack of difference in the prevalence rate of NSSI could be because our clinical sample did not include patients with a borderline personality disorder or eating disorders – psychiatric disorders with a high prevalence of NSSI.
One-year prevalence of NSSI was found to be around 5% in the clinical sample and 4.17% in the nonclinical sample. The 1-year prevalence rates found in this study were found to be significantly lower than those reported in the previous Indian studies (around 31%–34%, Bhola et al., 2017; Kharsati & Bhola, 2015). The differences in the 1-year prevalence of NSSI were likely to have emerged because of the fact that we assessed NSSI using a single (yes/no) question, whereas earlier studies used a checklist of self-injurious behaviors instead. Existing review studies have demonstrated that using behavioral checklists often leads to higher prevalence rate estimates as compared to a single-item measure (Muehlenkamp et al., 2012).
Although the prevalence of lifetime and current NSSI and the age of onset of NSSI did not significantly differ between the two samples, some phenomenological differences were found between NSSI in the clinical and nonclinical samples. More specifically, head banging was more often reported in the nonclinical sample. Additionally, the clinical and nonclinical samples also differed to some extent on the functions of NSSI. More specifically, as compared to the nonclinical sample, individuals in the clinical sample were more likely to engage in NSSI to show themselves how strong they are. It is not clear why these differences exist, and further quantitative and qualitative research may be needed to understand them.
In terms of the association between NSSI and identity, our results indicated that the nonclinical sample scored higher on the consolidated identity subscale and scored lower on the disturbed and lack of identity as compared to the clinical sample. This finding is in line with the observation that most psychiatric disorders emerge as an extreme presentation of normative processes or as a failure to achieve developmentally critical milestones (Cicchetti & Rogosch, 2002; Kaufman et al., 2014). The findings of the path models showed a similar pattern of associations between the identity variables and NSSI. In both samples, a higher consolidated identity was associated with a lower probability of engaging in lifetime NSSI. Similarly, in both the samples, higher scores on disturbed identity significantly predicted lifetime NSSI. Overall, these results are in line with previous research (Claes et al., 2015; Gandhi, Luyckx, Maitra, Kiekens, & Claes, 2016), which have shown that irrespective of the type of the sample (clinical or nonclinical), having a consistent sense of self (i.e. consolidated identity) may be protective against NSSI, whereas the disturbed sense of self may increase the vulnerability to NSSI.
Interestingly, the strength of the association between consolidated identity and NSSI and disturbed identity and NSSI did not significantly differ between both the samples. Additionally, the absence of a unique significant association between lack of identity and NSSI, especially in the clinical sample (but also in the nonclinical sample) was particularly surprising. The aforementioned findings contradicted the results obtained when comparing consolidated, disturbed and lack of identity between the clinical and nonclinical samples. The lack of a stronger association between disturbed identity and NSSI and a nonsignificant association in the clinical sample can be perhaps explained by the fact that this sample did not include patients with eating disorders and personality disorders like a borderline personality disorder, which are known to exhibit severe identity issues. Methodologically, the pattern of associations observed in the clinical sample may be because of the small number of cases engaging in NSSI. It should be noted that the absence of an association between lack of identity formation and NSSI was not surprising in the nonclinical sample. This is because it may be difficult to observe severe identity issues (as captured by the lack of identity subscale) in the nonclinical sample.
Despite making significant contributions to the literature on identity formation and NSSI, the current study is not without limitations. First, the findings of the current study were based on the cross-sectional data. Therefore, no conclusions can be drawn about the directionality of effects. Furthermore, a longitudinal study design may be necessary for studying the directionality of effects among the study variables. Second, as we followed a nonprobability sampling method for collecting data in both the clinical and nonclinical samples, the findings of these studies cannot be generalized to a wider population. Third, in this study, Erikson’s theory was used as the overarching framework to model identity formation. This choice was guided by the fact that the applicability of Erikson’s theory has been extensively explored in an Indian context (Friedman, 2000; Kakar, 1978, 1992). However, further research should consider using more recent and nuanced models of identity formation to develop a more fine-grained understanding of the association between NSSI and identity. Fourth, future research should consider screening the nonclinical participants for mental health issues. Screening for psychiatric comorbidity in all the participants can allow researchers to control their effect during modeling the association between NSSI and identity formation. Finally, given that a small number of individuals indicated to have engaged in NSSI in both the samples, the possibility of type-2 errors cannot be negated. Consequently, replication of our study with larger sample size is recommended.
Despite these limitations, our findings may have important clinical implications. First, irrespective of the type of sample (clinical or nonclinical), helping individuals to develop a consolidated identity and manage their disturbed sense of identity can be helpful in preventing NSSI. For example, therapists can use open-ended exploratory questions (Beck, 2011) to increase the introspective abilities of their clients. Judicious use of such an exploratory process can often facilitate self-exploration, which may contribute to a consistent sense of self. Developing a strong sense of self may help individuals to resolve their disturbed sense of identity and reduce the probability of engaging in NSSI.