
Abstract
Background:
Mental Health professionals often have to deal with at-risk individuals in crises and lack specialized training on suicide risk assessment and intervention. This study examined mental health professionals’ attitudes toward at-risk individuals and their perceptions of the quality of training and treatment available for assessing and intervening with this population.
Methods:
A total of 32 mental health professionals (13 psychiatrists, 16 psychologists, 2 psychiatric nurses; 1 social assistant) from highly vulnerable communities in Lima, Peru discussed their perceptions in four focus groups conducted by the authors.
Results:
Participants reported glaring deficiencies in all areas explored including training, knowledge and skills regarding suicide assessment and management. In addition, using ground theory analysis, three domains of findings emerged representing barriers and facilitators of treatment engagement, risk and protective factors of suicide and pros and cons of the current mental health care system including micro-, mezzo- and macro-level factors. The most frequently identified barrier was the perception that suicide is illegal; facilitator was family involvement; risk factor was poor parenting; protective factor was religious beliefs; pro of mental health care system was establishment of community-based services and con of mental health care system was lack of access to psychiatrists.
Conclusion:
The lack of specialized training available in the institutions that are designed to prepare mental health professionals for working with at-risk individuals is notable and has a direct and known impact self-identified by helping professionals. The need and desire for targeted training is palpable and essential to address growing rates of suicide, particularly among youth, in Peru.
Introduction
Although suicide rates have been historically lower in Latin America than other parts of the world (World Health Organization (PAHO, 2014), they have been increasing in recent years, especially among youth, and have become a cause for concern (Mascayano et al., 2015). It has been noted that suicidality is one of the greatest public mental health challenges for the next decade in Latin America and the Caribbean (LAC; Mascayano et al., 2015). Currently, there are an estimated 45,800 completed suicides a year in LAC and over 75% occur in low- to middle-income countries (Mascayano et al., 2015).
Peru, in particular, a country that has had among the lowest rates of suicide in South America (Teti et al., 2014), has seen substantial increase in suicide rates in recent years. For example, suicide rates among males in Peru have increased at an average annual rate of 65.79% from 2009 to 2015 (Human Development Report, 2017). Furthermore, an epidemiological study on mental health in Metropolitan Lima and Callao, Perú 2012 reports that 8.9% people had thoughts and wishes to end their life and 2.8% had suicide attempts (Instituto Nacional de Salud Mental, 2013). These data are thought to be an under-estimate as the Health Ministry (2018) of Perú reports that for every 10 suicides only 4 are reported. Furthermore, it has been estimated that 1 in 5 Peruvians are affected by a mental disorder (Castillo, 2012). The Health Ministry (2018) in Peru reports that 20.7% of the population aged 12 years and over suffers from a mental disorder. Yet, only approximately 31% of people who expressed having a mental health problem seek mental health treatment. Other data indicate that rates of those failing to engage in treatment are as high as 69% in Lima and 93.2% in other provinces (Health Ministry, 2018).
Numerous factors have been identified as contributing to this mental health gap among at-risk individuals in Peru, including systemic factors such as an insufficient budget allocated to mental health care and a lack of the integration of mental health care into primary care; societal factors, including, stigma, lack of information regarding mental health symptoms and treatment, lack of confidence in medical personnel and individual-level factors including at-risk individuals thinking they can solve their problems independently, considering themselves incapable of help; viewing their problems as not important, lacking awareness of where to seek mental health treatment, previous negative experiences with formal care and financial and/or time constraints (Health Ministry, 2018).
Further complicating the matter is the general lack of mental health care providers and services available in the country. The most recent research demonstrates that in Peru, for a population of nearly 30 million people, there were 1.71–3.2 psychologists and 0.57–1.4 psychiatrists per 100,000 residents (Health Ministry, 2018; WHO, 2011).
An additional yet often overlooked barrier is the important role that the clinician plays in the mental health treatment receipt of at-risk individuals. Research demonstrates that there is a direct link between the quality of specialized training on suicide assessment and intervention mental health professionals receive, their attitude and willingness regarding working with at-risk individuals and the likelihood that at-risk individuals engage in mental health services and receive the treatment they need to mitigate their risk (Alonzo et al., 2017; Alonzo & Gearing, 2017). Specialized training on suicide risk assessment and intervention is largely unavailable across mental health training programs in Peru. Understanding the impact of this lack of specialized training from the provider perspective is essential for informing the development of an effective suicide prevention and intervention program.
To address this gap in our understanding, we explored the perspective of mental health professionals (psychiatrists, psychologists, psychiatric nurses, social assistants) working in highly vulnerable communities in Lima, Peru regarding the nature of their training, knowledge and skills regarding suicide assessment and intervention; barriers and facilitators of engaging at-risk individuals in mental health treatment; risk and protective factors for suicide from the clinician perspective and gaps in the provision of current services for at-risk individuals.
Method
Practice setting
Mental health professionals currently practicing in highly vulnerable communities around Lima, Peru participated in the focus groups. These communities are characterized by high rates of crime, limited social/community resources and limited access to high quality formal health/mental health care. The districts are considered among the poorest, most highly populated communities in Lima.
Services provided by the helping professionals in these communities are largely within hospital settings, community centers and schools.
Recruitment
Convenience sampling was used to identify participants, a commonly used and acceptable method for identifying hard-to-reach groups and for gathering community-based data (Ahmadzadehaz & Ariasepehr, 2010; Naderifar et al., 2017; Polit-O’Hara & Beck, 2006). The Director of Psychological Services at the Universidad Antonio Ruiz de Montoya in Pueblo Libre, Lima, contacted practicing mental health professionals in local organizations (i.e., schools, hospitals) with which the University collaborates to request participation in a group discussion regarding the state of mental health care in Peru, their personal mental health training experiences and their practice experience with individuals at risk of suicide. The individuals contacted were asked to identify other individuals in their organizations across disciplines, stages of training and with varied years of practice experience who may be interested in participating in the focus group discussion. No remuneration for participation was offered and participation was strictly voluntary with no impact on the clinician’s standing with their respective employers. They were able to leave the focus group at any time or to refrain from answering any questions they so wanted. All organizations/individuals invited to participate agreed. Informed consent to participate was sought from all clinicians before the focus groups were held.
Participants
In total, 4 focus groups were held. Participants included 32 mental health professionals (13 psychiatrists, 16 psychologists, 2 psychiatric nurses, 1 social assistant). Focus groups were conducted in the mental health professionals place of employment or at the University. Average years of practice experience of participants were approximately 8 years.
Study design
This study was conducted as part of a program called !PEDIR!. !PEDIR! is a specialized brief training program developed to address mental health professionals’ attitudes toward at-risk individuals and provide intensive, targeted training on suicide assessment and intervention across mental health helping professions and individuals studying in graduate mental health programs. ¡
The study employed a grounded theory approach for the qualitative data gathered (Charmaz, 2006; Charmaz & Belgrave, 2012; Strauss & Corbin, 1998), a widely utilized qualitative research method often used in focus group studies (Abrams et al., 2009; Wong et al., 2010). Within the framework of the grounded theory approach, focus group participants are encouraged to openly discuss and examine their experiences and to share their perceptions and opinions. Shared ideas, unique concepts and themes of interest are then identified and coded using open coding, axial coding and attention to process (Strauss & Corbin, 1998).
Data collection
The focus groups were conducted in Spanish and were facilitated by the authors. The primary author has a PhD in social work and has worked as a bilingual mental health clinician in the United States and researcher in the field of suicide and treatment engagement for over 20 years with extensive experience moderating groups. She is a Professor of Clinical Social Work and Founder and Director of a program focused on suicide prevention and intervention. The second author is the Director of psychological services and Professor at a University in Lima, Peru. She has direct experience facilitating groups and detailed knowledge of the health care system in Peru and the organizations for which the focus group participant’s work.
Groups lasted 1.5 hours on average. Data were collected using a semi-structured interview. The following general topics were explored: (1) type of training on suicide assessment and intervention received in educational program; (2) identifying barriers to and facilitators of treatment engagement among at-risk individuals; (3) risk and protective factors for suicide in the populations they serve and (4) quality of services available for at-risk individuals. Participants were encouraged to address additional topics they felt were important/relevant.
Specific questions that were posed to each focus included (1) What kind of training did you receive on working with suicidal clients? (2) Do you feel you had the knowledge and skills you needed to be effective with suicidal clients? (3) What specific barriers do you identify that impact the treatment engagement of suicidal clients? (4) What do you consider to be the key risk factors for suicide in the client population you serve? (5) What are the key protective factors against suicide in the population you serve? (6) What potential facilitators can you identify that may improve the treatment engagement of suicidal clients? (7) What are the pros and cons of existing mental health treatments for clients experiencing suicidal ideation and behaviors (i.e., medications or specific therapeutic interventions)? The participants/interviewees were encouraged to suggest any additional questions that they thought relevant.
Data analysis
Detailed field notes were taken by the principal investigator (PI) during the focus groups. Field notes are widely accepted in qualitative research as a means of documenting contextual and process information (Phillippi & Lauderdale, 2018) and are considered to provide rich context for analysis (Creswell, 2013; Lofland et al., 2005; Mulhall, 2003; Patton, 2002). Field notes were taken in accordance with established guidelines for the collection, integration and dissemination of field notes for focus groups (Phillippi & Lauderdale, 2018).
The field notes for the four groups were transcribed and checked for accuracy and authenticity by the primary author and a graduate research assistant. Each reviewed the transcription multiple times to identify units of information that referred to the same content. Using an inductive approach, these units were then collapsed to create a set of preliminary categories. The categories were then clustered and themes identified. To ensure for analytic and methodological integrity, the PI and research assistant analyzed data separately, generated themes from the data independently and compared results to reach agreement and achieve consistency during the course of the analysis (Polit-O’Hara & Beck, 2006). To ensure inter-rater consensus, debriefing inter-rater reliability meetings were held throughout the study and raw data verification was utilized for comparing analyses with the original words of the participant when disagreement was present (Lincoln & Guba, 2000).
Results
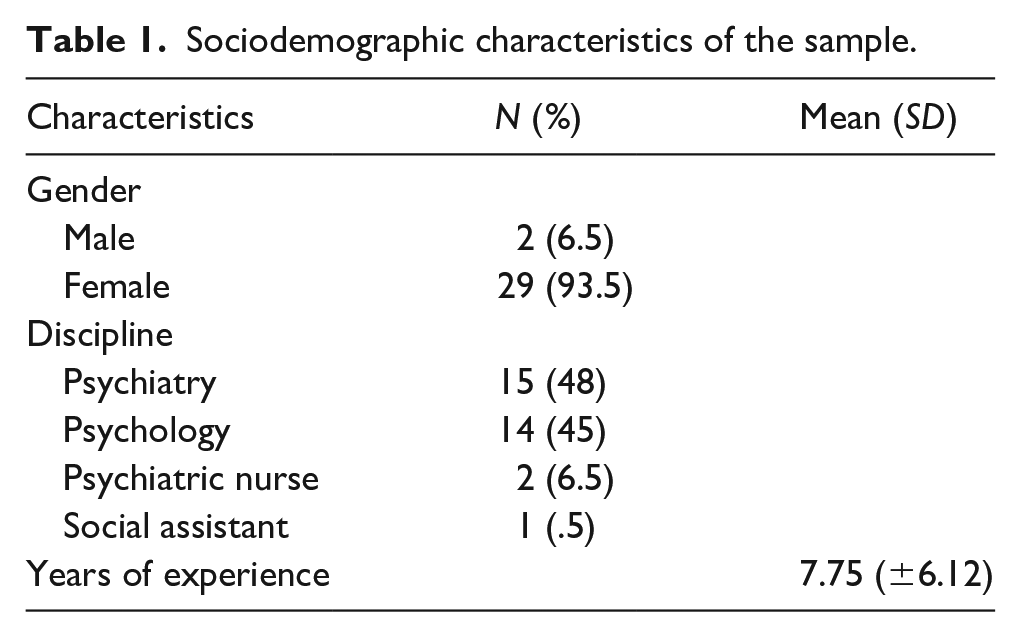
Table 1 presents the sociodemographic characteristics of the participants. The majority of the sample was female (94%). Most participants were psychiatrists. Average of years of clinical experience was 8 years.
Sociodemographic characteristics of the sample.
Training
All participants reported a significant lack of training focused on suicide prevention and intervention. Consistently, across mental health disciplines (psychiatry, psychology, nursing) and stages of training, participants reported that no specialized training exists and that they received no specialized training during their program, internship or residency. Participants comments included: ‘You have to find it on your own because education programs do not offer it’, ‘I wouldn’t even know where to go to find it’, ‘most primary care doctors are not willing to be trained on mental health issues’, ‘Suicide may be identified as a symptom of other problems like depression or trauma but it is never the focus’ and ‘I may have received some supervision if I had a case of a patient that had attempted suicide or was thinking about it but no formal training as part of my residency program’.
Skills and knowledge
Again, participants were consistent in their responses and reported feeling that they lacked the skills and knowledge they needed to work effectively with individuals struggling with suicidal thoughts and feelings. Participant comments included, ‘I have developed my open way of determining risk but from my own experience’, ‘I am not aware of specific interventions to target suicide’ and ‘I just try to listen and be supportive but other than that there is not much I can do’ and ‘I try to consult with my colleagues to get advice on how to manage these kinds of patients. We can support each other with suggestions for managing cases’. That said, participants consistently agreed that listening and demonstrating caring were basic skills that are helpful across patient presenting problems, including individuals at-risk of suicide.
Identified themes across categories
Three key themes emerged from the participants’ discussions of barriers and facilitators of treatment engagement, risk and protective factors for suicide and the pros and cons of the current mental health care system. These included (1) micro-, (2) mezzo- and (3) macro-level variables. Micro-level factors are defined as those characteristics related to the individual patient. Mezzo-level factors are defined as those related to the family and/or community. Macro-level factors are defined as socio, political and economic issues.
Treatment engagement
There was a high degree of consensus among participants regarding the factors that impact treatment engagement. Five (5) main barriers to treatment engagement and three (3) key facilitators of engagement were identified across the focus group.
Barriers to treatment engagement
The majority of identified barriers were mezzo-level variables (60%) followed by macro-level variables (40%). Table 2 reports the identified barriers in order of frequency.
Clinician identified barriers and facilitators to treatment engagement.
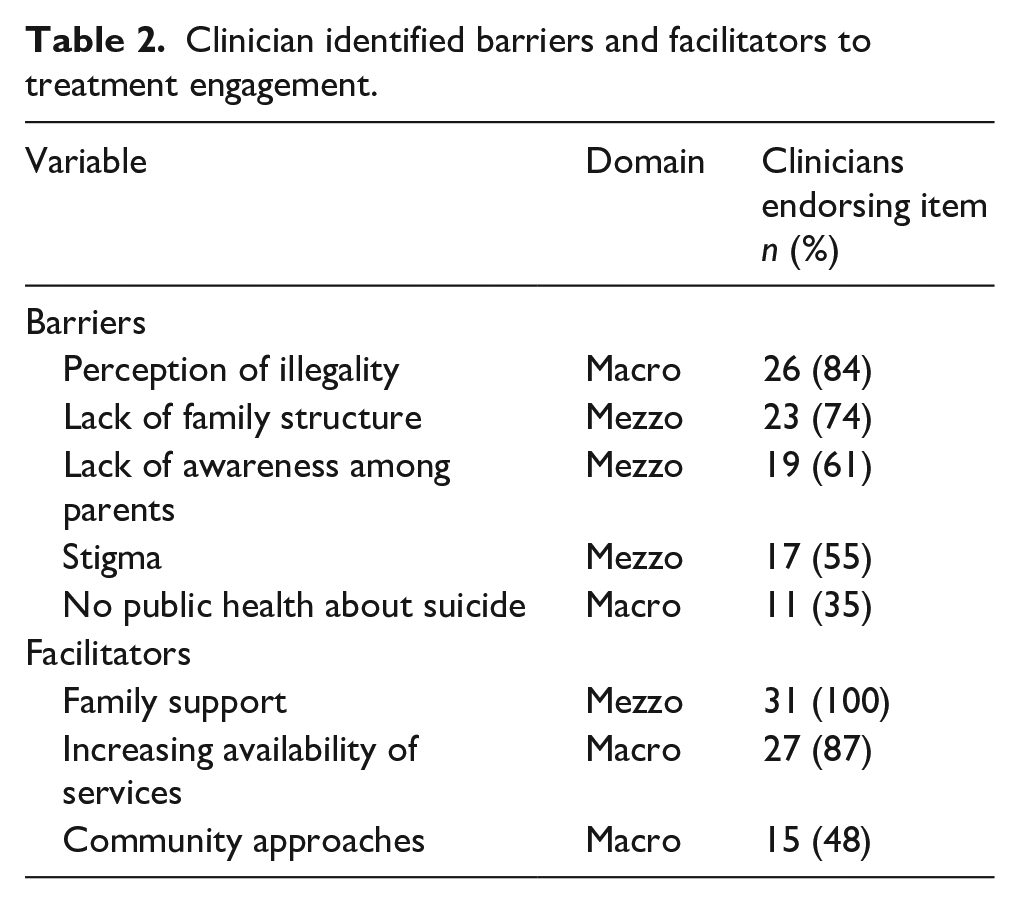
Participants noted that, ‘Because suicide is still illegal in Peru, it is very hard for people to admit that they have attempted or even thought about it because they are afraid of the consequences. People will even say an attempt was “an accident” because otherwise they could be arrested or held against their will’, ‘the disintegration of the family is a major problem because no one is paying attention to youth and they miss they signs’, ‘individuals who are struggling would rather see a psychologist for therapy because seeing a psychiatrist and taking medications means you are really crazy’ and ‘there is no effort to educate the public about suicide. We see campaigns against bullying and against violence but nothing for suicide. Every zone has center for women and children but only to protect them against abuse not to treat their mental health needs’ (see Table 2 for the rate each factor was endorsed by participants).
Facilitators of treatment engagement
Far fewer facilitators of treatment engagement of at-risk individuals were identified. One (1) of the three factors identified was a macro-level factor (33%) and the remaining two were mezzo-level factors (67%). See Table 2 for protective factors identified in order of frequency.
Participants felt strongly that family, particularly parental, support for and involvement in treatment was the strongest facilitator of treatment engagement among at-risk individuals noting,
When family members, especially parents, demonstrate that they agree that treatment is important it is a good sign that the patient will adhere to treatment. Unfortunately, all too often, individuals feel their families are unsupportive or will turn their back on them completely for seeking help. Those patients tend to drop out.
Other noted, ‘As more treatment centers become available, it is easier to think about going for help because the burden of having to travel far and find the time to get to the clinic is no longer part of the decision’ and
the community health teams have made a big difference. They are able to screen for problems immediately and direct people to the proper level of care. This way, fewer people are having to wait long periods for care and those that really need it get identified. This makes it somewhat more likely that people will go for help.
Risk and protective factors
Participants were more readily able to identify risk as compared to protective factors (78% vs. 21%). They identified 12 prevalent risk factors for and 3 key protective factors against suicide. Of the risk and protective factors, the most highly endorsed factor was a protective factor, specifically religious beliefs, identified by 100% of participants.
Mezzo-level risk factors were identified most frequently (50%), followed by micro-level factors (33%) and finally by macro-level factors (17%). Specific risk identified by participants is reported in Table 3.
Clinician identified risk and protective factors for suicide.
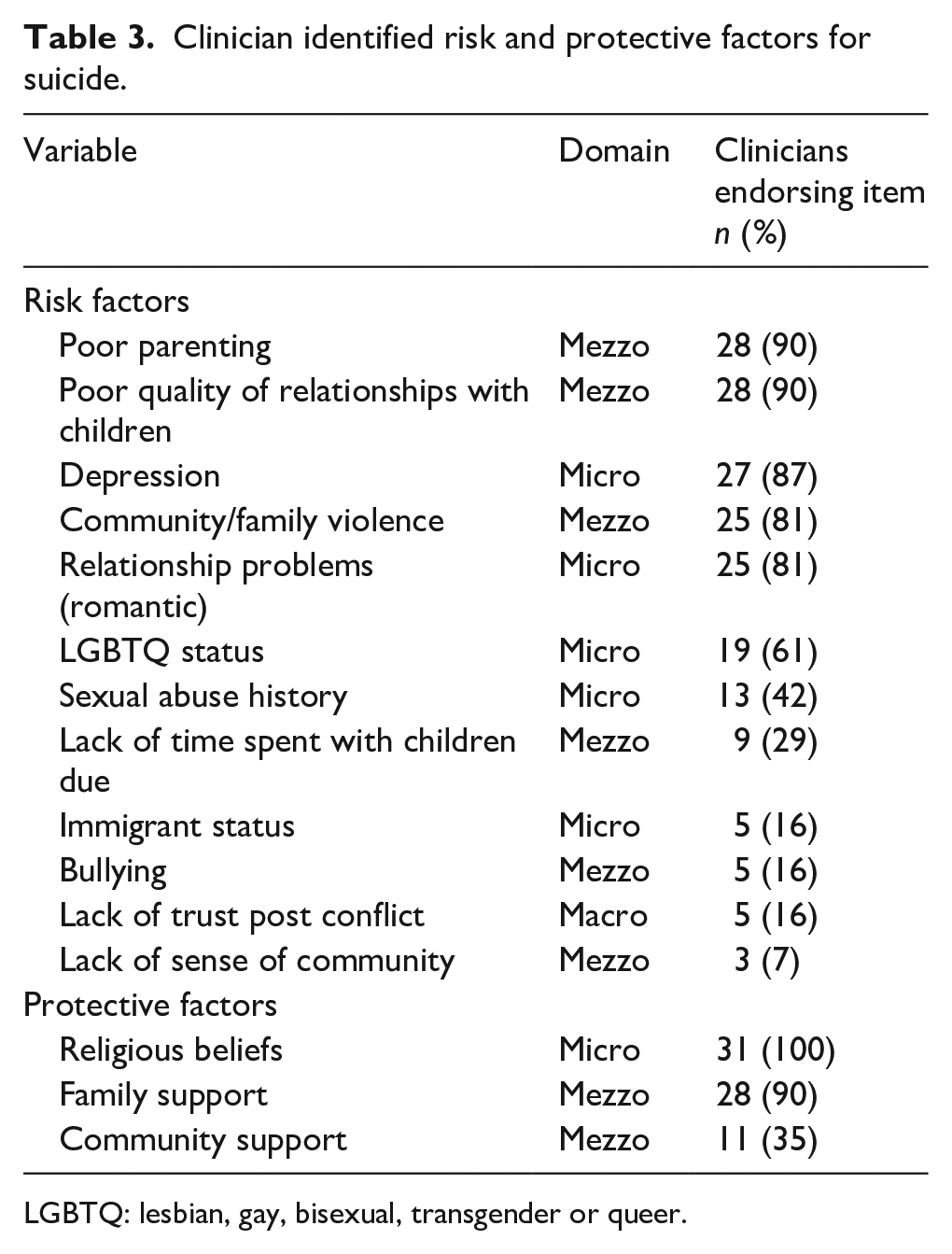
LGBTQ: lesbian, gay, bisexual, transgender or queer.
Participants explained, ‘Domestic violence is a huge issue and even though there is more public awareness about this problem and most communities have a center for abused women to receive services, they don’t address their mental health needs’, ‘Medications are so costly that clients cannot actually afford to use them consistently even when they want to’, ‘Parents are unable to spend the time they need to with their children because they are working multiple jobs’, ‘parents don’t understand that when their children are acting out they may be expressing depression or anxiety or struggling with suicidal thoughts’ and ‘In provinces where family structure could be a whole town, the period of conflict interrupted this and now the younger generation now doesn’t have anyone to look up to and learn from’.
In terms of protective factors, one of the three factors identified was a micro-level factor (33%) and the remaining two were mezzo-level factors (67%). Protective factors identified in order of frequency are reported in Table 3. Interestingly, no macro-level factor was identified as serving as a support against suicide risk, further emphasizing the lack of adequate mental health care services available that was noted as a risk factor.
Participants commented, ‘Having family support can make all the difference’, ‘when family is supportive of treatment then the individual is more likely to acknowledge their thoughts and feelings and to get help for them’ and ‘often patients share that their religious beliefs are the only thing keeping them alive’.
Pros and cons of existing services
In terms of the quality and nature of existing services for the treatment of individuals at-risk of suicide, participants struggled to identify any benefits of the existing mental health system, but had identified several areas that required improvement/attention. Cons to current mental health care system were also more consistently agreed upon than the pros (100% vs. 87%).
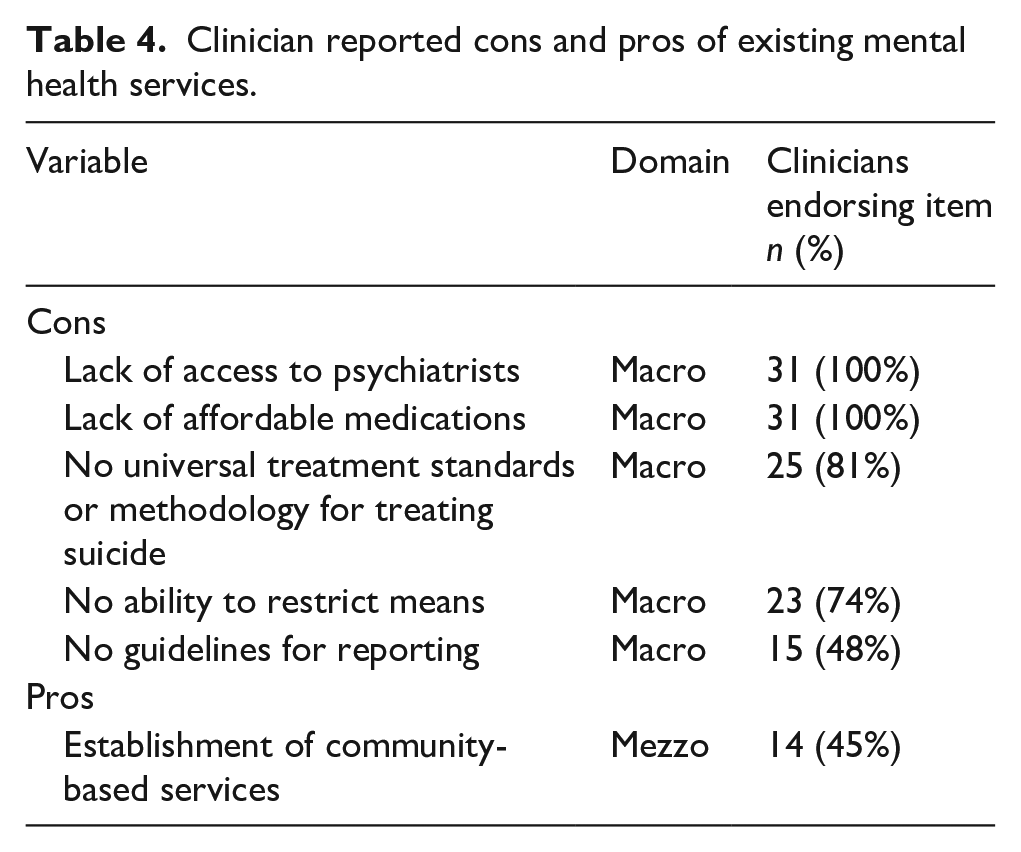
Participants reported that the establishment of community-based mental health teams, a mezzo-level variable, was the only pro of the current mental health system (endorsed by 45% of participants). Comments included, ‘The best thing that has happened has been that community teams are now available to increase access to services’, ‘Community teams help to reach people who might not wait for appointments or come in at all but there just aren’t enough of them’ and ‘The community teams can facilitate triage and identify the cases that are low risk or need some kind of immediate care’.
In terms of cons to existing mental health services for individuals at risk of suicide, clinicians identified multiple concerns. All were macro-level factors (100%). Cons to existing services in order of frequency identified are reported in Table 4.
Clinician reported cons and pros of existing mental health services.
Participants noted, ‘means restriction is virtually impossible in certain regions. Like the Amazon, for example, they may use natural plants that are poisonous and there’s no way to control that’, ‘Most clinics don’t even have a psychiatrist to prescribe medications even if a person was willing to take them and a private psychiatrist costs more than most people can afford’ and ‘Even when psychiatrists are available they prescribe meds that are so costly that clients cannot actually afford to use them consistently even when they wanted to’.
Discussion
According to the WHO (2005), interventions aimed at improving engagement in treatment would provide a significant positive return on investment through primary prevention of risk factors and secondary prevention of adverse health outcomes. Increasing the effectiveness of interventions that facilitate treatment engagement may have a far greater impact on the health of the population than any improvement in specific medical treatments. One key consideration that should inform these efforts targeting individuals at risk of suicide is the role of the mental health clinician including their knowledge and skills regarding suicide assessment and intervention; clinician perspectives regarding barriers and facilitators to treatment engagement; risk and protective factors for suicide from the clinician perspective and gaps in the provision of current services for at-risk individuals from the provider perspective. To our knowledge, this is the first study to examine mental health professionals’ perspective of the quality and nature of their training regarding suicide assessment and treatment; barriers to and facilitators of engaging at-risk individuals in outpatient treatment, risk and protective factors for suicide and pros and cons of existing mental health services.
Our results indicate that across mental health disciplines (psychiatry, psychology, psychiatric nursing), years of training and treatment setting (school, hospital, community based center), there is a general consensus that training specific to suicide assessment and management is largely non-existent in training and education programs. Furthermore, it was also agreed that they did not possess the knowledge and skill needed to effectively work with this population, noting a lack of guidelines for reporting, a lack of universal practice recommendations for this population and a lack of a universally accepted and/or utilized intervention for treatment of at-risk individuals. Clinicians indicated that they felt training was needed, important and wanted yet they did not know where to go to get it. Informal support, mainly conferring with colleagues, is the most common form of guidance received for working with at-risk individuals. These results are consistent with other reports examining training on suicide assessment and management across Latin America and the United States (Alonzo et al., 2017; Kohn et al., 2018; Schmitz et al., 2012; Tellez-Vargas & Forero-Vargas, 2012; WHO, 2014).
Given the rising rate of suicide in Peru, these findings are particularly concerning as research consistently demonstrates that as a result of working with mental health providers who have not received proper training in assessing and treating suicide, at-risk individuals often prematurely end treatment, become discouraged about talking with mental health professionals and may even resist future help-seeking, leaving them without the treatment they need to mitigate their risk (Grimholt et al., 2014; Taylor et al., 2009; Wingate et al., 2004). Research also demonstrates that brief evidence-based trainings focused on suicide prevention and intervention can improve mental health professionals’ risk assessment skills and management of suicidal clients and that such improvements are maintained over time (Schmitz et al., 2012), suggesting that delivering this type of training in this setting could have a meaningful impact.
Importantly, no clinician-related characteristics were identified as related to treatment engagement. Despite the fact that clinicians readily identified and strongly agreed that they lacked the skills and knowledge needed to work effectively with at-risk individuals, they do not identify that this relates to the degree of client engagement in treatment. Our findings are consistent with prior research demonstrating that clinicians tend to underestimate their role as serving as a barrier to treatment (Klein et al., 2003; Murdock et al., 2010; Pulford et al., 2008). This is particularly concerning as research also demonstrates that above and beyond clients’ level of insight and their degree of motivation for treatment, the quality of the therapeutic relationship with the clinician is a much greater predictor engagement in treatment (Alonzo et al., 2017; Ardito & Rabellino, 2011; Zilcha-Mano et al., 2015). Research has further found that treatment outcomes are directly related to the therapists’ interpersonal capacities such as their ability to convey empathy, to provide affirmations and to avoid judgmental, negative comments and responses (Andersen et al., 2009; Beutler et al., 2004; Bohart et al., 2002; Horvath & Bedi, 2002; Safran et al., 2002; Sandell et al., 2007; Vocisano et al., 2004). Our findings suggest that clinicians may lack awareness regarding the impact their lack of training, knowledge and skill has on the engagement process and the likelihood that their at-risk patients remain in treatment. Helping clinicians to understand this connection should be part of any training program focused on improving knowledge related to working with at-risk individuals and suicide assessment and management skills.
Results also seem to indicate that participants believe addressing change at the mezzo level could have a significant impact on the treatment engagement of at-risk individuals. More specifically, the participants were rather positive regarding the establishment of community mental health teams. They identified several ways in which the community teams improve the likelihood that at-risk individuals receive the help they need including triaging cases, providing referrals and offering support to less severe cases. Nevertheless, they also identified that, at this point, there are not enough of these centers to make a meaningful impact. For example, at the primary care level, it was noted that doctors could serve as a source of referral to mental health treatment; however, at present, they often lack the knowledge and skills needed to identify mental health issues and do not have the time to assess for such symptoms even when they have the knowledge and therefore are not facilitating access to mental health care. Many zones still lack a community health team and at-risk individuals in those communities have to seek help at the hospital and experience long wait times and receive only one to two sessions a month due to high patient loads. In 2018, for example, the Health Ministry estimated that Perú needed 315 community mental health teams and up until that time only 31 such teams existed (Health Ministry, 2018).
Also at the mezzo level, our results suggest that participants view the role of family as critically important as the majority of factors cited by participants as contributing to treatment engagement, quality of care and degree of risk and protection against suicide were at the mezzo level. Our findings are consistent with research that has found that family support has a powerful influence on well-being and that when family is included in a client’s treatment, rates of treatment engagement are increased (Mueser et al., 2009). In addition, research has found that receiving support from family is associated with an increased likelihood of help-seeking, even when clients have a low perception of need (Bonabi et al., 2016; Gulliver et al., 2010; Jorm, 2000; Ozbay et al., 2007). Efforts at increasing awareness regarding mental illness and suicidality within families and among parents is important to increase the likelihood that at-risk individuals receive needed treatment.
Participants also felt strongly that macro-level change was needed if at-risk individuals are going to benefit from changes at the mezzo level and increasing community-based health teams. They noted that because suicide is believed to be illegal, many individuals may hide their thoughts and feelings about suicide, explain away prior attempts as ‘accidents’ to avoid prosecution and do not present for treatment. Participants noted their beilef that individuals would be more likely to utilize the community-based health teams being established if they knew their information would be kept confidential and they would receive assistance without fear of facing legal consequences from disclosing their behaviors. In private practice settings, for example, often this type of information is not reported and individuals may be more likely to disclose in this type of setting knowing they will be able to return home without sanctions. Research in this area supports this idea finding that there are no data indicating that decriminalizing suicide is associated with increased suicide rates. In fact, the reverse has been found with suicide rates tending to decline in countries after decriminalization and that decriminalization may lead to increased reporting of suicides once the fear of a legal consequence for suicide is eliminated (Mishara & Weisstub, 2016). However, what is most notable about this finding is that it is actually not illegal to attempt suicide in Peru. Rather, euthansia and physician assisted suicide are illegal (Ministry of Justice, 2016). As such, when an individual seeks treatment following a suicide attempt, the attending professional is mandated by law to report the incident to the police not because suicide itself is illegal but to ensure that the suicide attempt was not pressured, forced or assisted in some way. That mental health professionals have this perception and report that many patients and their famiies also share this belief indicates a need for psychoeducation at the macro level regarding individual’s right and protections as they pertain to suicidal behavior and mental health care.
Strengths and limitations
This study has a number of strengths. To begin, mental health professionals across a number of mental health disciplines participated in the focus groups providing a broad perspective on the targeted issues. A wide range of settings was also represented including schools, hospitals and community mental health teams. Furthermore, participants had a wide range of years of practice experience representing varied views according to the timing and content of their training and education. A number of limitations should also be noted. First, only mental health professionals participated in this study. Future research may consider interviewing high-risk clients regarding their perspectives on barriers and facilitators of treatment engagement and risk and protective factors for suicide to understand how they compare to the clinician perspective. In addition, including physicians in future studies regarding their perspectives/beliefs and training would be very important as they are often the first point of contact for at-risk individuals. In addition, as is the case with all qualitative studies, there is a degree of interpretation inherent in qualitative research even though established guidelines for ensuring methodology in qualitative research were followed.
Conclusion
Overall, this study provides insight into the mental health professional’s perspective on the quality and nature of the training they received on suicide assessment and management and on providing mental health services to individuals at risk for suicide in high-risk communities in Peru. We identified a serious lack of training across mental health disciplines and self-reported lack of knowledge and skills needed to work with at-risk individuals. We also identified key barriers to and facilitators of treatment engagement across multiple domains and key risk and protective factors related to suicide to inform the development and utilization of engagement focused interventions. Future research should focus on the development, testing and implementation of culturally relevant, brief training programs targeting knowledge and skills regarding suicide assessment and intervention to improve the effectiveness of mental health providers and increase the treatment engagement of at-risk individuals.