
Abstract
Background:
Individuals with mental illness, as they are stigmatized by society, are also stigmatized themselves, and this process is internalized. This may adversely affect the recovery process.
Aims:
This study was conducted to investigate the relationship between internalized stigmatization and subjective recovery in patients with schizophrenic.
Method:
This research was performed for patients with schizophrenia at rehabilitation centers registered with the community mental health center. The survey was performed out with 94 patients in the recovery phase who met the inclusion criteria and who going to the center. Sociodemographic information form, internalized stigmatization scale and subjective recovery assessment scale were used in the collection of data.
Results:
In the study it was found that there is a relationship between internalized stigmatization and subjective recovery. Increased levels of internalized stigma patient outcome would decrease the level of recovery.
Conclusion:
It is recommended that nurses perform intervention programs to reduce internalized stigmatization in patients with schizophrenia.
Keywords
Introduction
Schizophrenia is a chronic mental illness that may negatively have an effect on the regions of thinking, social interaction, motor behavior, attention, mastering, and perception (O’Donnell & Martin, 2016) and causes impairment in functionality of individual (Dima et al., 2015). The people with schizophrenia can be regarded by society as a dangerous, aggressive, vulnerable, and inadequate by the society (Yılmaz & Okanlı, 2015). Individuals with serious mental illnesses often act in behaviors that may be frightening, disturbing, disruptive or at least annoying and may be excluded from society and may be excluded from the society (Çam & Yalçıner, 2018). The patients with schizophrenia, who face stigmatizing behaviors by society, may easily stigmatize themselves by internalizing this behavior (Çam & Çuhadar, 2011; Noyman-Velsker et al., 2013; Segalovic et al., 2013). Internalized stigmatization may cause schizophrenic patients to restrict their interaction with society, detach themselves from social interactions and experience feelings such as anxiety, shame, lack of self-confidence, helplessness, and weakness. Patients face many adverse effects, such as reduced self-esteem, unemployment, income loss (Omori et al., 2014; Vidovic et al., 2016; Bukhari et al., 2019). Internalized stigmatization prevents the help seeking behaviors of the patients with schizophrenia and their compliance with psychosocial treatment, poses a risk for hospitalization and may negatively affect the recovery (Wahl, 2012). In a study conducted by Temesgen et al. (2020) also found a direct relationship between subjective recovery and internalized stigma.
Recovery considered an outcome involves the remission of symptoms and the achievement of psychosocial milestones. Recovery has been defined as process involving many aspects of self-experience related variables, such as sense of identity (Leonhardt et al., 2017). Nowadays, the concept of mental illness recovery is not characterized as the absence of disease symptoms and the complete functioning of individuals, but it is characterized as the fact that patients find their lives meaningful and worth living, are aware of their ability and abilities, given the disease’s limitations, and make attempts to assess them and assign hope to life (Çam & Yalçıner, 2018). The concept of subjective recovery in patients with schizophrenia can be defined as having a personally meaningful and satisfying life, being able to take one’s own life goals and care decisions, to have hope for the future, being at peacewith oneself, having a valued sense of integrity, well-being and self-respect (Liberman, 2012). The patients with schizophrenia may have difficulty in complying with the treatment along with internalized stigmatization, their self-efficacy decreases, they cannot lead a satisfactory life, and their perceptions and processes of recovery may be negatively affected (Beldie et al., 2012; Park et al., 2013; Tsang et al., 2016; Thibodeau et al., 2018). Internalized stigmatization and perception of subjective recovery in patients with schizophrenia may have an adverse effect on the continuation of the illness. This study was conducted to identify the concepts of internalized stigmatization and subjective recovery in schizophrenic patients, and to determine their associations with each other.
Method
This is a descriptive cross-sectional study conducted to explore the association between internalized stigma and understanding of subjective recovery in patients with schizophrenia.
Sample and setting
This research was performed at the community mental health center. The survey was performed out with 94 patients with schizophrenia in the recovery phase who met the inclusion criteria.For the inclusion of patients in the sample, consideration was given to the criteria consisting of having reached the age of 18, having diagnosed schizophrenia with DSM-V diagnostic criteria and being in the remission phase of the disorder. The exclusion criteria of the study were determined as having barriers such as hearing, seeing, understanding and perception, and being in the relapse period of the disease. The socio-demographic information form, the internalized stigma of mental illness scale, and the subjective recovery assessment scale were used in the collection of data.
Socio-demographic Information Form: The socio-demographic information form, which was developed by the researchers in line with the literature, included 12 questions evaluating the situations of thinking of getting improved and believing in recovering, in addition to questions including the socio-demographic characteristics of patients such as age, gender, educational status, marital status, income status, employment status, time of diagnosis, and presence of other diseases.
The Internalized Stigma of Mental Illness Scale (ISMI): The ISMI, which wasoriginally developed by Ritsher et al. (2003), is a self-report scale consisting of 29 items and evaluating internalized stigmatization. The scale has five subscales consisting of (1) Alienation (six items), (2) Stereotype Endorsement (seven items), (3) Perceived Discrimination (five items), (4) Social Withdrawal (six items) and 5. Resistance to Stigma (six items). The items in the ISMI are answered on a four-point likert type scale as “I strongly disagree” (one point), “I disagree” (2 points), “I agree” (3 points), and “I strongly agree” (4 points). The study in which the validity and reliability of the ISMI in our country was evaluated was carried out with 203 patients with different diagnoses admitted to psychiatry clinic. While Cronbach’s alpha coefficients of the ISMI’s subscales varied between 0.63 and 0.87, Cronbach’s alpha coefficient for the whole scale was calculated as 0.93. The total ISMI score obtained by summing the scores of the five subscales ranged from 4 to 91 points. Higher scores obtained from the scale indicate that the internalized stigmatization of the person is negatively more severe (Ersoy & Varan, 2007).
Subjective Recovery Assessment Scale: It is a 17-item likert-type self-report scaledeveloped by Yıldız et al. (2018). Each item is scored from 1 to 5. Higher scores obtained from the scale indicate that the patients’ perceptions of subjective recovery are increased. The Cronbach alpha coefficient of the scale was calculated as 0.98, and the item total score correlation coefficient was calculated between 0.83 and 0.94. The scale had a single-factor structure as result of construct validity. Test-retest reliability was found to be (r = 0.98). The score obtained from the scale is between 17 and 85, and it is understood that the perception of subjective recovery increases as the score obtained increases (Yıldız et al., 2018).
Ethical Dimension of the Study: Permission was obtained fromYıldız and Ersoy, who are the responsible authors of the Internalized Stigma of Mental Illness Scale and the Subjective Recovery Assessment Scale, by contacting them via e-mail before the study in order to use the scales in the study. Ethical approval was obtained from Health Sciences University, Antalya Training and Research Hospital Clinical Research Ethics Committee in order to carry out the study. The necessary legal permissions of the institution where the study was carriedout, and informed consents of the patients participating in the study were obtained.
Data Analysis: The data obtained as a result of the study were evaluated by using the SPSS 20 package program on computer. Number and percentage distributions, independent samples t-test and Pearson correlation coefficient methods were used in the evaluation of data.
Results
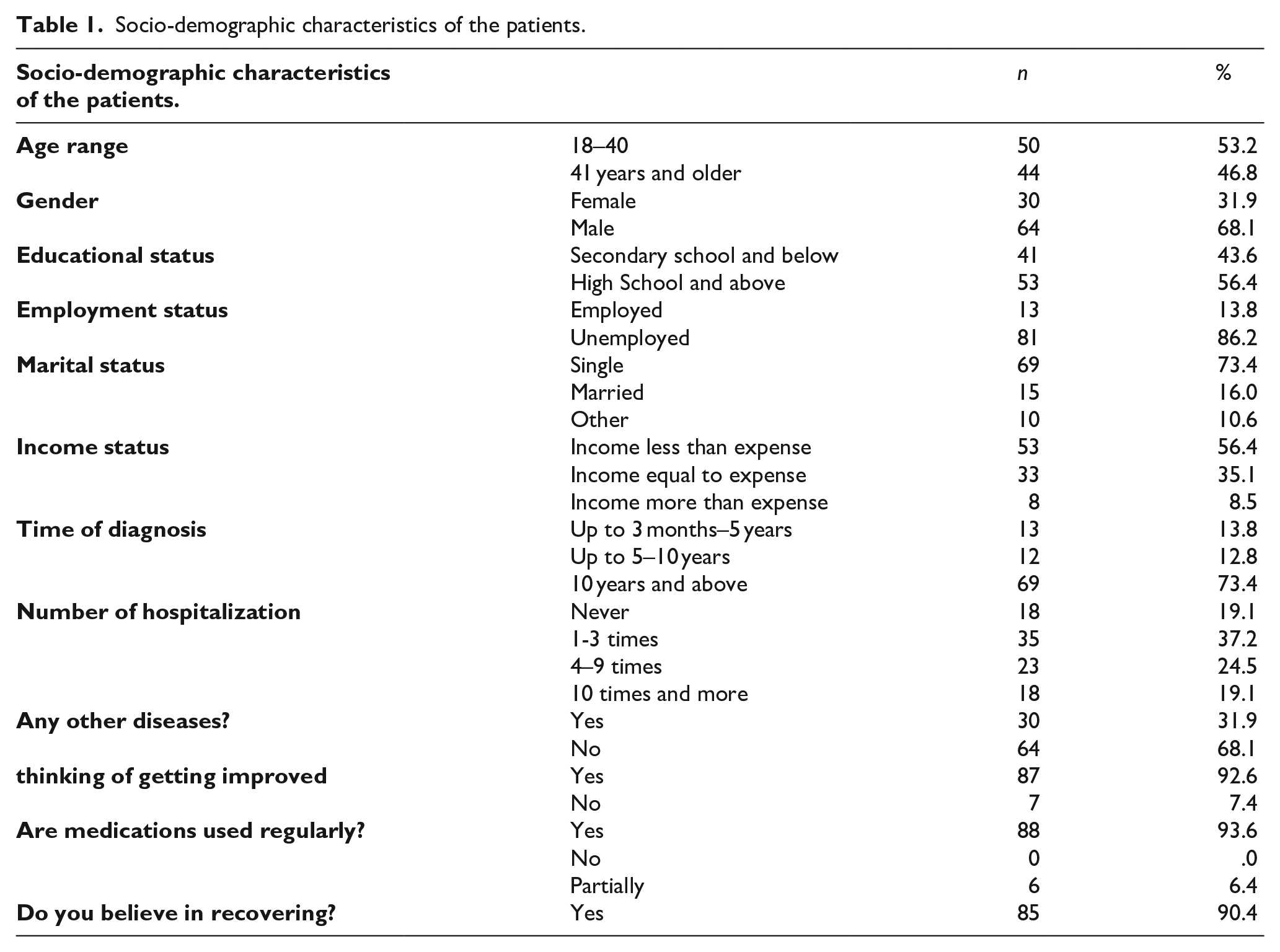
Of 94 patients participating in the study, 31.9% were female, 68.1% were male, 13.8% were employed, 86.2% were unemployed, and 86% were single. According to their answers, 92.6% of the patients participating in the study thought that they improved and 90.4% of them believed that they would recover. The socio-demographic characteristics of the patients are presented in Table 1.
Socio-demographic characteristics of the patients.
While the patients’ mean score of the subjective recovery scale was 57.07 ± 14.21, it was determined that their mean scores obtained from the sub-dimensions of the internalized stigma of mental illness scale were 14.35 ± 3.46 for the alienation sub-dimension, 15.90 ± 3.93 for the stereotype endorsement sub-dimension, 12.95 ± 3.57 for the perceived discrimination sub-dimension, 15.24 ± 3.95 for the social withdrawal sub-dimension, and 10.94 ± 2.97 for the resistance to stigma sub-dimension (Table 2).
Scores of patients from scales.

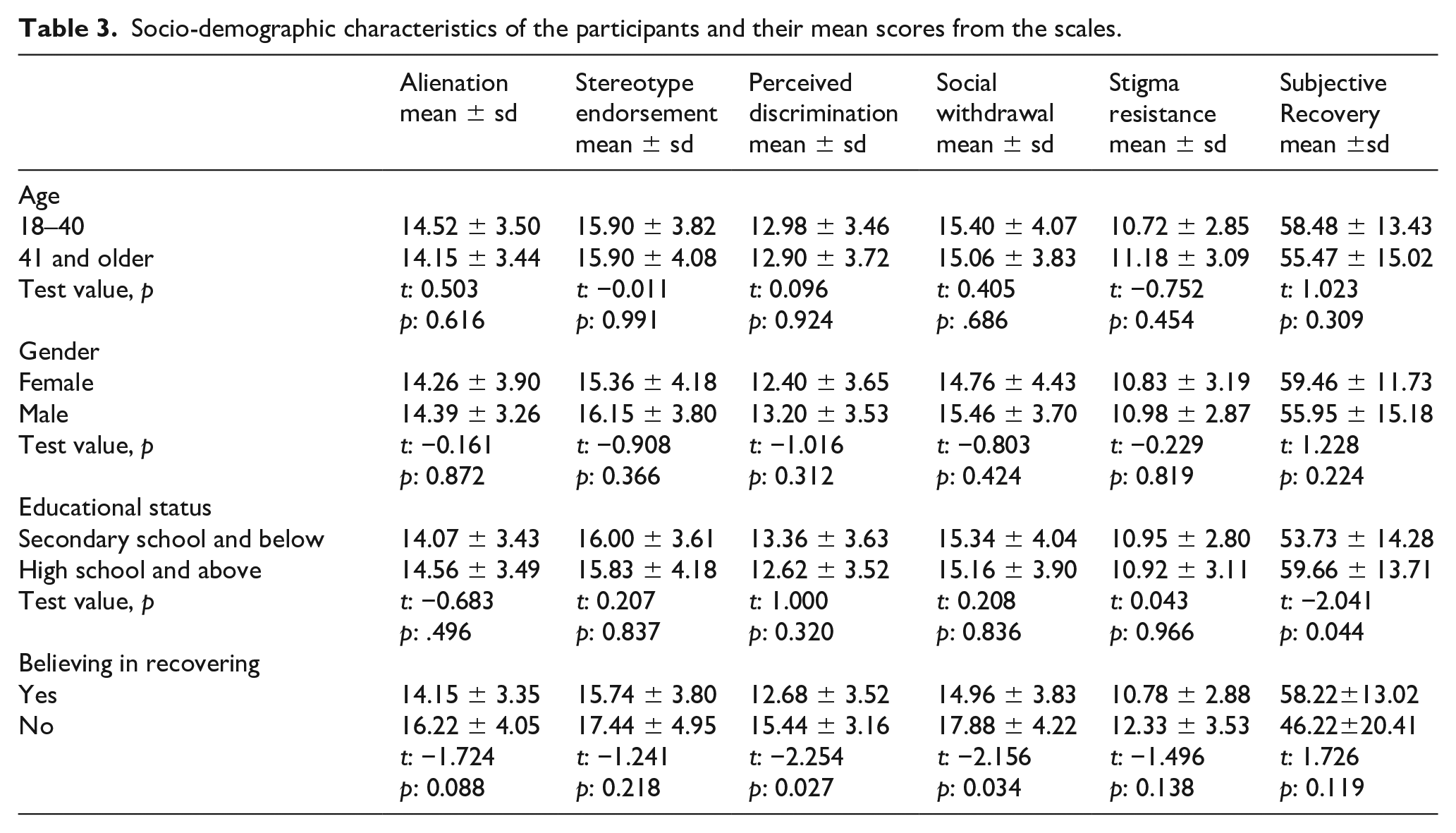
When participants’ mean scores of the sub-dimensions of the subjective recovery assessment scale and the internalized stigma of mental illness scale were evaluated according to their socio-demographic characteristics, it was determined that age and gender did not affect alienation, stereotype endorsement, perceived discrimination, social withdrawal, resistance to stigma, and subjective recovery (p > 0.05). It was determined that educational status was significant in subjective recovery, and subjective recovery was found to be significantly higher in those with an educational status of high school and above. The effect of believing in recovering on the perceived discrimination and social withdrawal was found to be statistically significant (Table 3).
Socio-demographic characteristics of the participants and their mean scores from the scales.
In the correlations between the scales, a negative significant high correlation (Cohen, 1988) was found between the subjective recovery scale and the stigma of mental illness scale. In the sub-dimensions of the subjective recovery and the internalized stigma of mental illness scale, a moderately negative significant correlation was found between subjective recovery and alienation and social withdrawal. A negative significantly high correlation was found between subjective recovery and stereotype endorsement, perceived discrimination and resistance to stigma (Table 4).
Correlation between the scales.

p < 0.005.
Discussion
In this study, the correlation between internalized stigmatization and perceptions of subjective recovery of the patients with schizophrenia was examined, and it was revealed that internalized stigmatization influenced subjective recovery. In the international studies carried out with patients with schizophrenia, it was also found that patients had high levels of internalized stigmatization (Assefa et al., 2012; Bukhari et al., 2019; Caqueo-Urízar et al., 2019; Hill & Startup, 2013; Hofer et al., 2019; Lv et al., 2013; Park et al., 2013; Vrbova et al., 2018). In this study, the subjective recovery and internalized stigmatization of the participants were evaluated with their socio-demographic data, and it was observed that educational level was effective in the perception of subjective recovery. With respect to believing in recovering, it was observed that perceived discrimination and social withdrawal were significantly higher in those who did not believe. Although the perception of subjective recovery is a subjective concept, it is affected by the individual’s lifestyle, peer support, and experiences with mental illness (Rossi et al., 2018). In this study, it was determined that educational status was significant in subjective recovery, and the perception of subjective recovery was found to be significantly higher in those with an educational status of high school and above. Similarly, in the study evaluating the indicators affecting the recovery in schizophrenia, it was stated that educational level was a factor in subjective recovery and that high educational level had a positive effect on recovery (Austin et al., 2013).
In this study, internalized stigmatization was observed in approximately 69.3% of the participants. In the literature, there are different studies indicating internalized stigmatization in patients with schizophrenia. In a study carried out by Lv et al., 2013, it was reported that the ratio of internalized stigmatization was around 70%, similar to our results. In a study carried out by Brohan et al. (2010), it was indicated that the ratio of internalized stigmatization was around 41.7%. In another study, internalized stigmatization in patients with schizophrenia in Czech was reported to be around 64% (Holubova et al., 2016). Although there are cultural differences between countries, patients experience similar internalized stigmatization.
In this study, it was found that the perceived discrimination and social withdrawal had a negative effect on individuals’ belief in recovery. Fighting discrimination and stigmatization is important in facilitating recovery in schizophrenia (Zhang et al., 2019). Similarly, in the study carried out by Muñoz et al. (2011), it was found that the perceived discrimination decreased personal recovery expectations. In the study carried out by Soundy et al. (2015), it was determined that close social ties with family and friends were important for the recovery process in patients with schizophrenia. It indicates the importance of evidence-based anti-stigmatization interventions designed to eliminate discriminatory behaviors in schizophrenia.
In the studies on internalized stigmatization and recovery (Chan &Mak, 2014; Chronister et al., 2013; Yılmaz &Okanlı, 2015; Zhang et al., 2019), although the correlation between internalized stigmatization and the adverse consequences of disease, and both psychosocial and psychiatric outcomes related to recovery were examined, the results on subjective recovery were slightly evaluated. In the correlations between the scales in this study, a negative significant high (−0.581) correlation (Cohen, 1988) was found between the subjective recovery scale and the stigma of mental illness scale. Similarly, in the study carried out by Zhang et al. (2019), a negative correlation was found between internalized stigmatization and recovery. This study had a cross-sectional design, therefore, inability to test cause-effect relationships was one of the limitations of the study. Further studies using a longitudinal cohort design are required to examine the effects of internalized stigmatization on outcomes related to subjective recovery. Furthermore, there are also other variables that may play an important role in understanding internalized stigmatization, such as self-esteem, were not included in this study, and it is necessary to carry out further studies including these variables.
Limitations
Despite the contributions of the current research, therewere limitations. The first limitation of the study is its sample size. Regarding the fact that our study was conducted in only one community mental health center, the results cannot be generalized to the all population. Depending on self-reported data gatheringforms might be another limitation.Time and a sequential progression are needed for someone to perceive subjective recovery and to feel internalized stigmatization.If we try to investigate relation of these two process-based concepts, then a follow-up study instead of a cross-sectional one would give more reliable results. Therefore, another limitation of this study is its cross-sectional design.
Conclusion
In the study, it was found that there was a correlation between internalized stigmatization and the perception of subjective recovery. It can be said that patients’ subjective recovery levels will decrease along with the increase in their internalized stigmatization levels. It is recommended that nurses should perform intervention programs aimed at decreasing internalized stigmatization in patients with schizophrenia.