
Abstract
Background:
The diagnosis and treatment of an illness using traditional medicine is in most cases culture-specific and based on beliefs in the community. The majority of mentally ill patients prefer to attend to traditional healers because of the trust problems in the system, affordability, accessibility, and ease of the service.
Aim:
To assess the role of traditional healers among the pathway of psychiatric services of OCD patients, and to highlight its clinical correlates.
Methods:
we assessed 93 patients with OCD after confirmation of the diagnosis with fifth version of MINI semi structured interview, using a questionnaire designed and accustomed by authors to assess help seeking behavior in OCD patients and its sociodemographic and clinical correlates. Type of symptomatology and its severity were assessed using Y-BOCS.
Results:
A total of 39.8% sought traditional healers help, 94.6% were before psychiatric advice, main symptoms related to traditional healers seeking were religious and sexual obsessions. Main causes of traditional healers’ preference were stigma of seeking psychiatric advice in 89.2% of cases, considering disease related to religion in 81.1%, considering that religious commitment help in treatment 75, 7%, and considering disease related to magic and superstitions in 45.9%. Religious origin of illness was the most statistically significant factor related to seeking advice at traditional healers.
Conclusion:
This study shows that a significant percentage of the patients suffering from OCD prefer to approach traditional healers first due to their own beliefs mainly religious, and society acceptance.
Introduction
Traditional medicine is the sum total of the knowledge, skill, and practices based on the theories, beliefs, and experiences indigenous to different cultures, whether explicable or not, used in the maintenance of health as well as in the prevention, diagnosis, improvement or treatment of physical and mental illness (World Health Organization [WHO], 2013)
The diagnosis and treatment of an illness using traditional medicine is in most cases culture-specific and based on beliefs in the community. As healers interpret the type of illness and prescribe how it will be treated, the same illness could be interpreted and treated differently according to another (Mbwayo et al., 2013). Culture plays a critical role in healthcare delivery, as people have different ways of communication, religious beliefs and standards, family structures, and health beliefs and practices that affect how they behave and interact with the medical service (Sherra et al., 2017). Culture has been described as an ‘inherited lens through which individuals and communities perceive and understand the world that they inhabit, and learn how to live within’ (Kleinman, 1997). Failure to bridge the gap between the patient and the physician can result in: (a) improper diagnosis, (b) unnecessary testing, (c) misunderstanding of consent, (d) prognosis, (e) problems with adherence, satisfaction and follow-up, and (f) the outcomes of the disorders (El-Rufaie, 2006). The majority of mentally ill patients prefer to attend to traditional healers because of the trust problems in the system, affordability, accessibility, and ease of the service. This may cause delay in asking for psychiatric services which has a prognostic effect (Assad et al., 2015).
Obsessive-compulsive disorder is a complex disorder with considerable variability and broad spectrum of symptom presentation (Krzyszkowiak et al., 2019). Even though the core symptoms of OCD (e.g. contamination obsessions, checking compulsions) are very consistent across different geographic and cultural settings; many studies indicated that culture can play a role in shaping some OCD symptoms (Yang et al., 2018; Yorulmaz et al., 2010).
Studies on the effect of culture on OCD have examined how culture may influence the phenomenology or expression of OCD symptomatology, yet unfortunately the results were not that clear or satisfying (Yang et al., 2018). Previous Egyptian studies on psychiatric phenomenology have shown a prevalence of culturally determined symptomatology, where religion and prevailing traditions seemed to color the clinical picture of the condition, together with the patients’ attitudes about their disorder (Okasha, 2004).
In an Egyptian project to assess the role of traditional healers among the mental health service pathway for different psychiatric disorders, Assad et al. (2015) found (40.8%) of bipolar affective disorder patients sought advice from traditional healers while Awaad et al. (2020) found (41.81%) of schizophrenic patients consulted traditional healer first.
This study is a part of our fore mentioned project that aimed to assess the role of traditional healers among the pathway of psychiatric services of OCD patients. We aimed also to highlight the relationship between the type of symptomatology and other clinical variables and the help seeking behavior among traditional healers.
Methodology
Participants
All patients fulfilling diagnosis of OCD according to according ICD-10 criteria using mini international neuropsychiatric interview (M.I.N.I.) version 5, aged 18 to 60 years old, both genders, seeking help at inpatient ward or outpatient clinic of the Okasha Institute of Psychiatry, Ain Shams University were referred to research team till completion of the sample. Sample was calculated using PASS (prediction of activity spectra for substances) program, setting alpha error at 5% and confidence interval width at 0.2%, result from pervious study (Al-Hemiary & Al-Hasnawi, 2009) showed that 58.8% of OCD cases sought advice from traditional healers before seeking medical advice, based on this, the needed sample was 93 OCD cases. Patients with other psychiatric comorbidities as well as those who refused to participate or withdrew during the interview were excluded.
All procedures were revised and approved by the Ethical and Research Committee in Faculty of Medicine, Ain Shams University. An informed written consent was obtained from all patients for their participation after explaining in details the study procedures.
Procedures
All study participants’ sociodemographic data was collected, OCD diagnosis was confirmed according to ICD 10 criteria using mini international neuropsychiatric interview (M.I.N.I.) version 5. Severity and type of symptoms were rated by using Arabic version of Y-BOCS. A questionnaire designed by the authors to assess help seeking behavior in schizophrenia, was modified to accustom assessing patients of OCD. Data like motive to visit traditional healers, their explanation for symptoms, their way of treatment, number of visits, and degree of satisfaction of their service were assessed.
Statistical analysis
Data were collected, revised, coded, tabulated and entered to the Statistical Package for Social Science (IBM SPSS) version 23 (IBM Corp. Released 2015). Descriptive statistics: (1) Qualitative variables were presented as number and percentages and (2) Quantitative data were presented as mean, standard deviations, ranges, median and inter-quartile range (IQR). Analytical statistics: (1) Chi-square test was used to compare between groups with qualitative data. (2)
Results
Demographics
The study sample consists of 93 patients diagnosed with OCD according to according ICD-10 criteria. The patients included in the sample lie in range between 18 years and 60 years with mean and standard deviation (29.66 ± 10.77), 53.8% were males, 46.2% were females, 96,8% were Muslims, 3.2% were Christians, most of the patients by 58.1% were college graduates. Most of the patients included in the sample were unemployed (36.6%), the majority were single (59.1%) and were living at urban areas (76.3%).
Regarding OCD symptoms and severity among cases via YBOCS showed that religious (63.4%) and contamination (50.5%) obsessions are the most common obsessions, while cleaning (65.6%) and checking (65.6%) compulsions were the most common compulsions; most of cases (64.5%) ranged between moderate to severe, as 33.3% of cases had severe illness and 31.2% were moderate.
Pathway to traditional healers’ services
By assessment of pathway to traditional healers’ services via designed semi-structured questionnaire: results showed that 39.8% went to traditional healers, 59.5% were males while 40.5% were females, most of them were college graduates 43.2%, unemployed 37.8%, single 56.8%, and living in urban areas 67.6%. Almost all the cases by 94.6% were before psychiatric advice, 45.9% considered disease related to magic or superstitions, while 81.1% considered disease related to religion and 75.7% are considering religious commitment could help in treatment and 89.2% are still experiencing stigma from psychiatry. Most of the patients didn’t have to pay them money, as 43.2% used to pay simple objects and 40.5% didn’t pay money at all.
In addition, 64.9% sought advice at multiple traditional healers, 16.2% were seeking advice at both a psychiatrist and a traditional healer simultaneously. Most of the patients 83.8% were not satisfied by the traditional healers’ service. Only one cases reported improvement of symptoms; 32.4% reported that their last traditional healer visit was from 1 year to less than 5 years ago and 35.1% reported that their last traditional healer visit was 5 years ago or more. Surprisingly, 37.8% were referred by a traditional healer to psychiatric advice. On the other hand, none of the participants are still trusting traditional healers.
Traditional healing consultation was the recommendation of the family members in 81.1% of cases and the patients’ will in 67.6% of cases. Regarding causes of preferring traditional healing, most common cause in 81.1% was pressured by family; in 78.4% they were unsure where to obtain treatment, in 64.9% due to easy accessibility, 48.6% due to social acceptance, 29.7% due to unqualified surrounding mental health services, and 24.3% due to easily affordability.
Seeking advice at multiple traditional healers was reported by 64.8% of patients, 100.0% of cases were due to non-improvement of symptoms, 20.8% due to distant mental health services, 12.5% due to expensive mental health services and none of participants reported using violent treatment procedures.
Traditional healers’ explanation for symptoms was as follows: possession in 78.4%, black magic in 64.9%, and envy in 45.9%, while 32.4% were told that it is a psychiatric illness.
The treatment modality given by traditional healers was: religious rituals in 89.2%, spiritual sessions in 51.4%, counseling in 40.5%, herbs for ingestion in 35.1%, herbs for bathing in 29.7% and none of cases reported cupping, skin abrasions or any surgeries as a modality of treatment; 51.4% were regularly compliant to traditional healers’ treatment or instructions, 94.7% of them were due to directing towards religious commitment, 57.9% due to easy accessibility and 47.4% due to no medications being given, while 100.0% of cases stopped being compliant to traditional healers due to symptoms non improvement.
On assessing the sociodemographic data with the tendency to seek traditional healers’ advice, results showed a statistically significant relation between lower education level and increased tendency to seek advice at traditional healers by (p value .037), while there was no significant relation with age, sex, religion, occupation, marital state and residency (Table 1).
Assessment of seeking traditional healer’s advice among OCD participants according to their sociodemographic data.

Note. • = Independent t-test; * = Chi-square test.
p > .05: Non significant (NS). p < .05: Significant (S*). p < .01: Highly significant (HS*).
On correlating OCD symptoms with seeking traditional healers’ advice, there was no statistically significant relation between seeking traditional healers’ advice and severity of OCD symptoms, while statistically significant relation was found between presence of sexual obsessions (P-value 0.031) and religious obsessions (P-value 0.004) with higher tendency to seek advice at a traditional healer, meanwhile other symptoms types showed a statistically non-significant relation (Table 2).
Relation between obsessive compulsive disorder phenomenology assessed by Yale brown obsessive-compulsive scale (YBOCS) and seeking traditional healers’ advice.
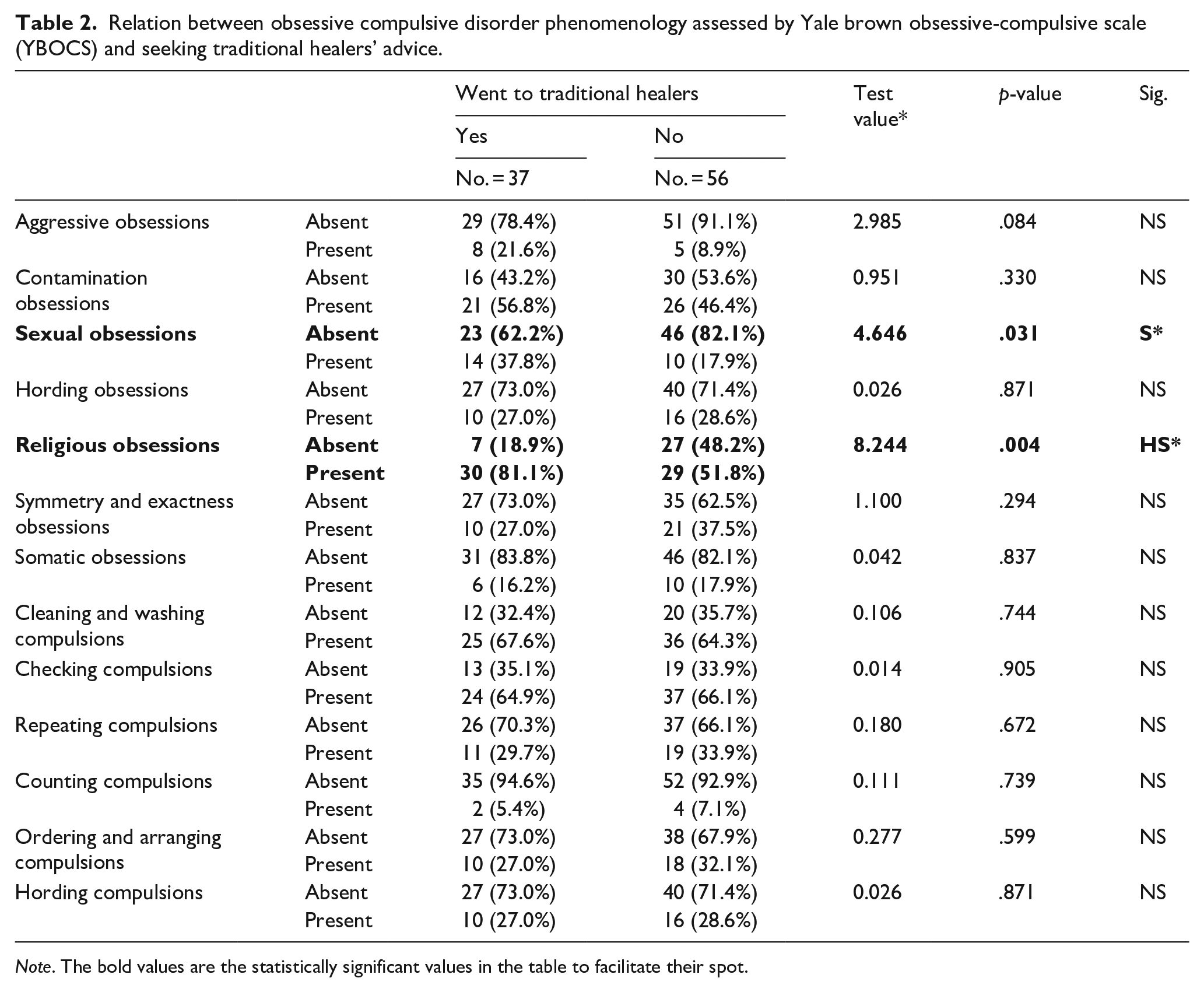
Note. The bold values are the statistically significant values in the table to facilitate their spot.
Regarding causes of preferring traditional healing, the most common was stigma of seeking psychiatric advice in 89.2% of cases, considering disease related to religion in 81.1%, considering that religious commitment help in treatment 75, 7%, and considering disease related to magic and superstitions in 45.9%. All the causes were very highly correlated with seeking advice at traditional healers (P- value 0.000). Also, earlier course of the disease was one of the factors that were related to traditional healing as 40.6% went to them in the first year of illness, while 24.4% went from first year of illness to less than five years of illness, with (p-value 0.011) (Table 3).
Factors of preference of seeking advice at traditional healers.
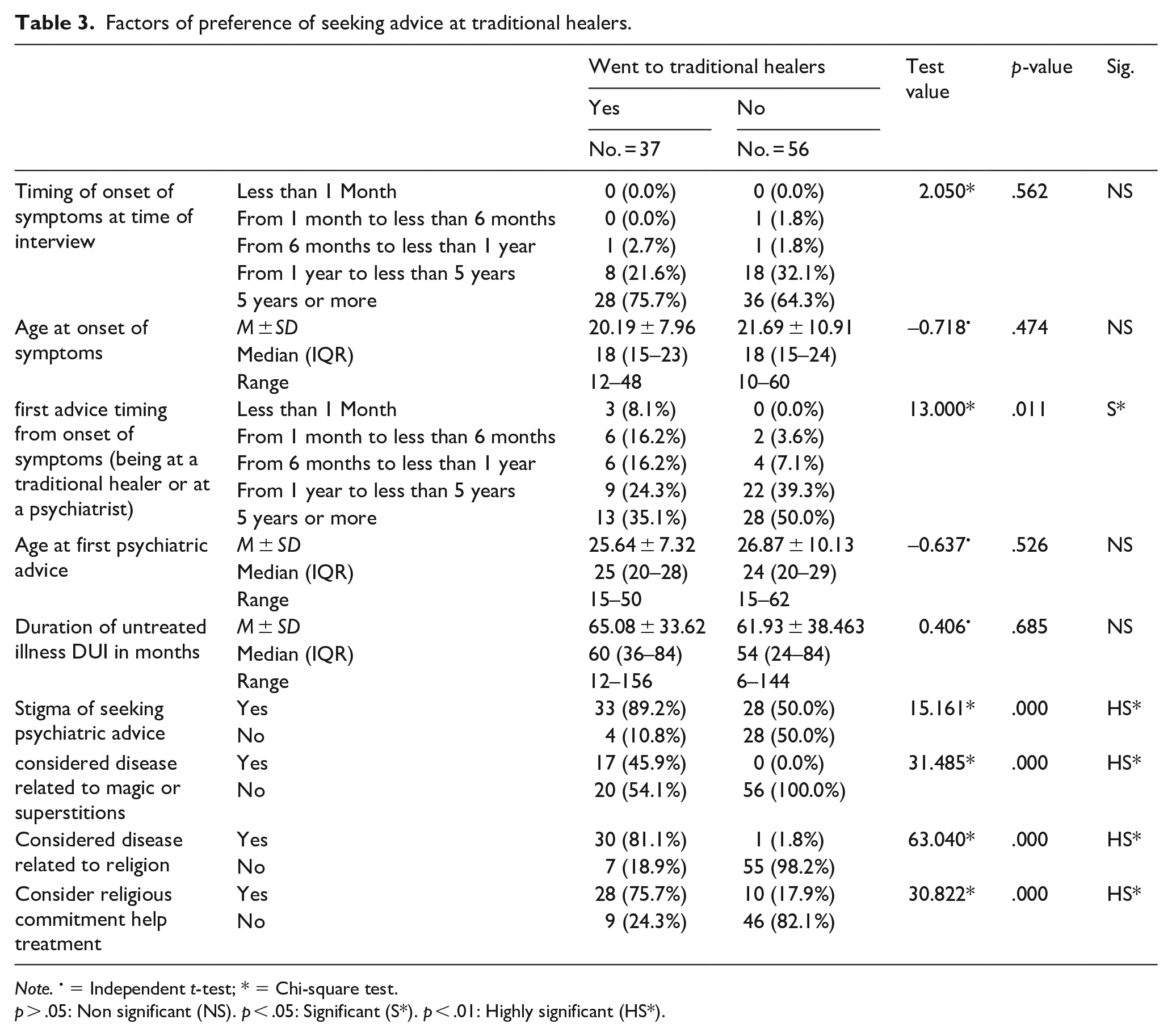
Note. • = Independent t-test; * = Chi-square test.
p > .05: Non significant (NS). p < .05: Significant (S*). p < .01: Highly significant (HS*).
Using Univariate logistic regression showed that sexual obsessions and religious obsessions considered independent factors to have more tendency to seek advice at traditional healers (OR 2.8 (95% C.I.) and 3.9 (95% C.I.) respectively). Also, presence of stigma from psychiatric advice, attributing disease of religion or considering religious commitment help treatment independent factors cause more tendencies to seek traditional healers’ advice (OR 8.2 (95% C.I.), OR 235 (95% C.I.) and OR 14.3 (95% C.I.) respectively). Using multivariate logistic regression showed that having considered disease related to religious origin was the most statistically significant factor related to seeking advice at traditional healers (P-value 0.000) among all factors that where statistically significant using univariate logistic regression (Table 4).
Uni-variate and multivariate logistic regression analysis for factors affecting went to traditional healer.
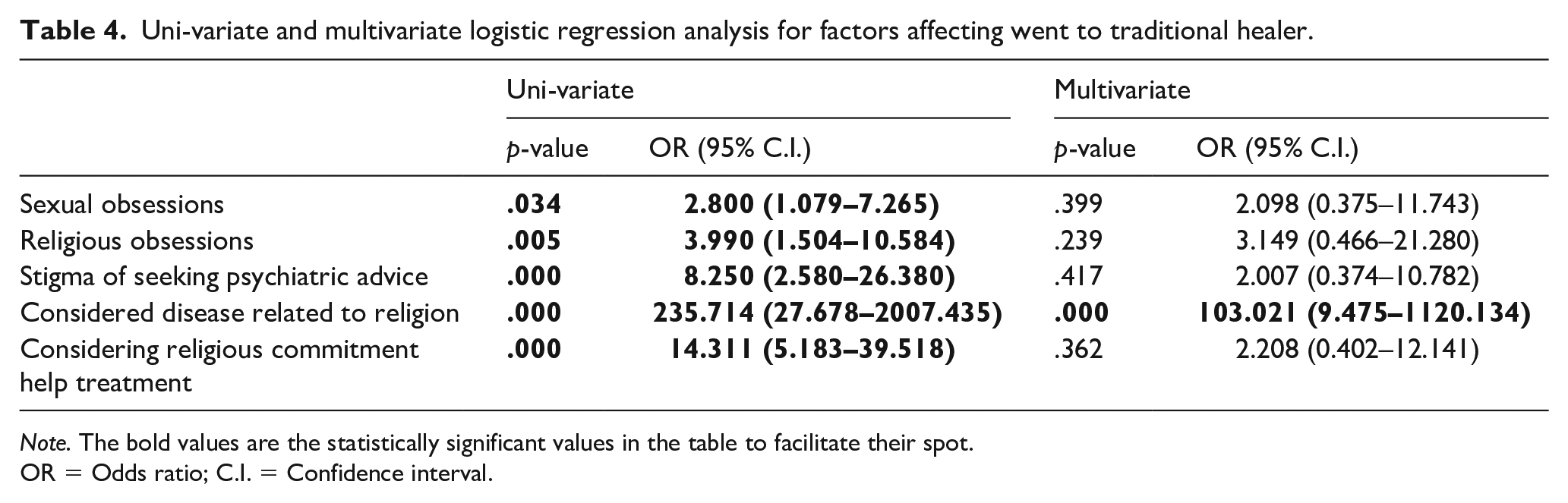
Note. The bold values are the statistically significant values in the table to facilitate their spot.
OR = Odds ratio; C.I. = Confidence interval.
Discussion
Although effective psychiatric treatments exist long ago, many people still delay years before seeking help or never seek it at all (Robinson et al., 2017). The potential role of traditional healers in mental health care has been debated in the literature on global mental health. Patel (2011) identifies the mutual suspicion between the two health care systems and concerns about the ‘unscientific’ practices of traditional healers as obstacles to such collaboration.
The study showed 39.8% of OCD patients sought advice at traditional healers, which is a similar to findings of other Egyptian studies about other psychiatric illness and role of traditional healers, as Awaad et al. (2020) found 41.81 % in schizophrenic patients and Assad et al. (2015)
Religion was a key player in our study, as it affected many aspects: (a) disease interpretation (81.1% considered disease related to religion and 45.9% considering disease related to magic and superstitions), (b) symptomatology (81.1% had religious obsessions), (c) help king behavior (75.7% considered that religious commitment helps in treatment), (d) Considering disease related to religion was the main predictor for traditional healing consultation. Similarly Al-Solaim and Loewenthal (2011) found that their entire study sample was suffering from symptoms in religious domain and all sought advice at traditional healers. Also, Mahgoub and Abdel-Hafiez (1991) examined a conservative Muslim sample in Saudi Arabia and found strong religious themes in their OCD symptomatology, including obsessions related to prayers and washing (50%), contamination (41%), and faith (34%). Religious obsessions related to contamination and purity, as well as compulsions involving washing, had been observed in many studies (Okasha et al., 1994 in Egypt; Saleem & Mahmood, 2009 in Pakistan; Shooka et al., 1998 in Bahrain; Yorulmaz & Işık, 2011 in Turkey).
The fundamental belief in Islam is God is One and He is the Most Powerful. It is written in the Quran which is the Islamic Holy Book, ‘And when I am ill, it is He who cures me.’ (Ash-Shu‘araa’ 26:80). This translates to God being the ultimate healer. By holding on to this belief, prayer to God asking for recovery is the key. However, doctors, medication and even spiritual healing practitioners are instruments of the mercy of God in the healing process (Abdullah et al., 2017).
An emphasis on cleanliness, purity, and religion is normative in Islamic cultures, as al-woodo is a religious practice in which the body must be systematically cleaned before prayer. However, when rituals surrounding these beliefs are committed in excess, and the beliefs become obsessive, they can then become culturally significant aspects of OCD symptomatology. This presentation may be particularly prevalent among Muslims with OCD due to the many cleaning rituals required in Islam (Williams et al., 2017).
In another emphasis on the role of religion, some Islamic scholars have associated cases of OCD (mainly obsessions) to the devil and relate it to religion. This religious implication in OCD in the Islamic culture lies in the term “weswas”, as in Arabic, OCD is called “Alweswas Alqahri”. In the Holy Qur’an there is “Alweswas Alkhanaas”. This term (weswas) is used to refer to the devil (telling people to do sins) as well as a name for obsessions. The use of this term is inspired by the Holy Qur’an that uses this word to refer to evil whispers of Satan; to the inner speech of the soul; or self-talk. So, the confusion can be understood between “obsession” in OCD in psychiatry and “obsession” in Islamic legacy (Okasha, 2004; Abdul Razak, 2014; Mohamed et al., 2015).
Omer and Mufaddel (2018) in Sudan found the majority of OCD participants (55.9%) believe that their psychiatric symptoms are due to evil eye, and 20.7% believe that the symptoms are due to magic. Al-Solaim and Loewenthal (2011) also found that some participants believed that OCD was caused by an ‘evil eye,’ described as being an illness caused by social conflict or the envy of another individual. Even after receiving psychiatric treatment, some patients still consult the traditional practitioners for advice. This sometimes results in poor compliance to treatment as some practitioners’ advice against medical treatment. They attribute the illness to supernatural agents thus implying that medical treatment is not the solution (Abdullah et al., 2017). However, some practitioners know their limits and would suggest the patient to seek medical treatment, which happened with 14 cases (37.8%) of our sample.
Most of our cases (64.5%) ranged between moderate to severe. Similarly, Okasha et al. (1994) found that most of their Egyptian sample was rated on the Y-BOCS as having moderate to severe symptom presentation, which was took as indicative of Egyptian patients’ high tolerance for psychiatric difficulties before seeking help. Native healers, religious people, friends and family elders are the primary caregivers for psychologically disordered individuals. When those interventions fail, seeking out the general practitioner, and then the psychiatrist, are the next resorts Okasha (2004). This goes with our finding that earlier course of the disease was one of the factors that were related to traditional healing as (40.6%) of cases went to them in the first year of illness, while (24.4%) went from first year of illness to less than five years of illness.
Also, another important issue that directed patients toward traditional healers’ advice was stigma from seeking psychiatric help. Similar finding was found in India by Lahariya et al. (2010), where (73%) of patients delayed health seeking due to the fear of stigma, also found that (68.5%) of the cases first consulted traditional healers. In our study 65.6% of patients experienced stigma from psychiatry and 31.2% are still experiencing it, consequently patients would either preferred not seek any advice or go to traditional healers. Burns and Tomita (2015) in a systematic review for African researches, explained that stigma surrounding mental health conditions and mental health services are a considerable barrier for many individuals seeking care and on the contrary, approaching traditional and religious healers is familiar and usually devoid of stigma. Strong social bonds formed though sharing a faith can encourage a sense of security among trusted relatives, and care for fellow members of the faith group. For example, congregations may counsel, sanction, or ‘disfellowship’ individuals with mental illness or substance use disorders because their appearance or behavior deviates from the group’s norms (Peteet, 2019).
The role of cultural factors in dealing with mental disorders needs attention from mental health professionals. It is important to advance new health service policies and legislations that may permit merging the traditional healers’ service into the mental health service system in order to reach maximum patient’s benefit from this collaboration. Mbwayo et al. (2013) suggested creation of a channel of referrals between healers and the health service by educating them the various psychiatric disorders and their manifestations as well as licensing them through helpful and positive engagement. Understanding cultural beliefs about mental illness is basic for proper application of mental healthcare approaches (Gautam & Jain, 2010; Viswanath & Chaturvedi, 2012).