
Abstract
Background:
The pandemic of coronavirus disease (Covid-19) seriously impacts the health and well-being of all of us.
Aims:
We aim to assess the psychological impact of Covid-19 on frontline health care workers (HCWs), including anxiety, depression and stress of threat of the disease.
Method:
The study was a cross-sectional survey among the frontline HCWs in a hospital at Jinan, China. Data were collected through an anonymous, self-rated questionnaire, including basic demographic data, a 10-item Covid-19 stress questionnaire, the Self-Rating Anxiety Scale (SAS) and the Self-Rating Depression Scale (SDS). The risk and rate of anxiety, depression and stress of Covid-19 were estimated.
Results:
Among the 309 participants, there were 88 (28.5%) with anxiety and 172 (56.0%) with depression. Multivariate logistic regression analyses showed that age ⩽ 30 years, age > 30 to 45 years, working in confirmed case isolation wards, and worrying about disinfection measures being not sufficient were independently associated with anxiety with an odds ratio (95% confidence interval, CI) of 4.4 (1.6–12.2), 3.1 (1.1–8.8), 2.3 (1.4–4.0) and 2.5 (1.5–4.3), respectively; age ⩽ 30 years, age > 30 to 45 years, nurse and worrying about disinfection measure being not sufficient were independently associated with depression with an odds ratio (95% CI) of 3.8 (1.8–7.8), 2.7 (1.3–5.7), 2.5 (1.1–5.6) and 2.1 (1.3–3.5), respectively.
Conclusions:
A high prevalence of anxiety and depression was found among frontline HCWs during the COVID-19 outbreak. More psychological care should be given to young staffs and nurses. Measures to prevent professional exposure is important for HCWs’ physical and mental health.
Introduction
Since December 2019, cases of pneumonia of an unknown aetiology, now known as Coronavirus disease (Covid-19) have appeared in Wuhan, China (Li et al., 2020). The disease has rapidly spread from Wuhan to other areas and was declared a pandemic by the World Health Organization (WHO, March 2020). As of May 4, 2020, a total of 3,435,894 laboratory-confirmed Covid-19 cases and 239,604 deaths had been reported globally, with a case fatality rate of 6.97% (WHO, May 2020). The unexpected spread rate and high lethality of the emerging infectious disease impact on the health and well-being of all of us.
Facing this large scale infectious public event, health care workers (HCWs) are under both physical and psychological pressure (Wu et al., 2009). Previous studies showed a significant proportion of HCWs experiencing anxiety, depression, fear and frustration during the outbreak of the severe acute respiratory syndrome (SARS) and A/H1N1 (Chong et al., 2004; Goulia et al., 2010). HCWs, especially those working in hospitals caring for people with confirmed or suspected Covid-19, may be vulnerable to both a high risk of infection and mental health problems. They may experience fear of contagion and spreading the virus to their families, friends, or colleagues. They may also worry about the shortage of protective equipment, and feelings of incapability when they face patients whom were unwilling to be quarantined at the hospital or do not cooperate with medical measures because of panic or a lack of knowledge of the disease (Chen et al., 2020). The mental health care for patients and health professionals directly affected by the Covid-19 epidemic has been under-addressed,
The aim of this study was to investigate the psychological impact of Covid-19 on HCWs including anxiety, depression, and stress and perception of threat of the disease in a designated infectious disease hospital for Covid-19.
Methods
Study participants and measures
The study was a cross-sectional survey which was performed from February 7 to February 21, 2020 at the Jinan Infectious Disease Hospital, Jinan, Shandong Province, China. The hospital is in charge of the diagnosis and treatment of notifiable infectious diseases in Jinan city. Since the outbreak of Covid-19 in December, 2019, the hospital became a Covid-19-designated hospital, in charge of the diagnosis and treatment of Covid-19, and medical observation of suspected cases of Covid-19 (Du et al., 2020). Four isolation wards (two for confirmed cases and two for suspected cases) and one fever clinic were set up for Covid-19. There were 309 medical staffs in the five divisions, including 35 doctors and 274 nurses. The hospital admitted its first confirmed Covid-19 case on January 23, 2020.
Data were collected through an anonymous, self-rated questionnaire distributed to the 309 HCWs over a mobile phone application. Only one response to the questionnaire per person was permitted. The questionnaire consisted of three parts: basic demographic data, a 10-item Covid-19 stress questionnaire, the Self-Rating Anxiety Scale (SAS), and the Self-Rating Depression Scale (SDS). All participants provided their online informed consent. The study was approved by the medical ethics committee of the hospital.
Evaluation of anxiety and depression
Anxiety and depression were assessed using the SAS and the SDS (Zung, 1965, 1971). The two independent self-assessment scales mainly assess the frequency of symptoms of the respondents in the past week, each with 20 items, using a 4-level score (1 for a little bit of the time, 2 for some of the time, 3 for a good part of the time and 4 for most of the time). Five items (Nos. 5, 9, 13, 17 and 19) in the SAS scale are stated using positive words, reverse integration in the order of 4 to 1, and the score is summed up as the total score. Standard score = 1.25 × total score. Anxiety levels were graded as the following: standard score below 50 = no anxiety, 50–59 = mild anxiety, 60–69 = moderate anxiety and above 70 = severe anxiety. Ten items in the SDS scale (Nos. 2, 5, 6, 11, 12, 14, 16, 17, 18 and 20) are stated using positive words, reverse integration in the order of 4 to 1 and the score is summed up as the total score. Standard score = 1.25 × total score. Depression levels were graded as the following: standard score below 53 = no depression, 53–62 = mild depression, 63–72 = moderate depression and above 73 = severe depression.
Stress to Covid-19
Information about stress, adverse experience and perception of risk was collected using a 10-item questionnaire. Upon the epidemic of COVID-19, we developed the 10-item questionnaire to investigate the attitudes to personal protection, social support and working in isolation ward pressure among frontline healthcare works. The Cronbach α of personal protection, social support pressure and working in isolation ward were 0.725, 0.658 and 0.753, respectively. Items were assessed on a five-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = not sure, 4 = agree, 5 = strongly agree).
Statistical analysis
The severity of anxiety, depression and answers to the 10-item Covid-19 stress questionnaire were reported in total cohorts and analysed in subgroups. In further analysis, the five-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = not sure, 4 = agree. 5 = strongly agree) was further divided into two categories: Yes = 3. not sure, 4. Agree, or 5. strongly agree. No = 1. strongly disagree or 2. disagree.
Categorical variables were described as frequency rates and percentages, and continuous variables were described using mean±standard deviation, interquartile range (IQR) and range values. Means for continuous variables were compared using independent group t tests when the data were normally distributed; otherwise, the Mann–Whitney test was used. Proportions for categorical variables were compared using the Chi-square test, or the Fisher exact test when the data were limited. Finally, significant variables were further analysed as the risk variables were analysed for the risks of anxiety and depression using multivariate logistic regression analyses. All statistical analyses were performed using SPSS (Statistical Package for the Social Sciences) version 19.0 software (SPSS Inc). For unadjusted comparisons, a 2-sided α of less than .05 was considered statistically significant.
Results
Characteristics of participants
Of the 309 HCWs in the isolation wards and fever clinic, 100% completed the questionnaire. Participants were 301 (97.4%) women and 8 (2.6%) men, with a mean age of 33.5 ± 9.5 years (IQR 26–41, range 19–57 years). Participants included 274 (88.7%) nurses and 35(11.3%) doctors. 126 (40.8%) of the participants worked in confirmed case isolation wards, 183 (59.2%) of the participants worked in suspected case isolation wards or fever clinic, and 220 (71.2%) were married (Table 1).
Severity of anxiety by SAS score in total cohort and subgroups.
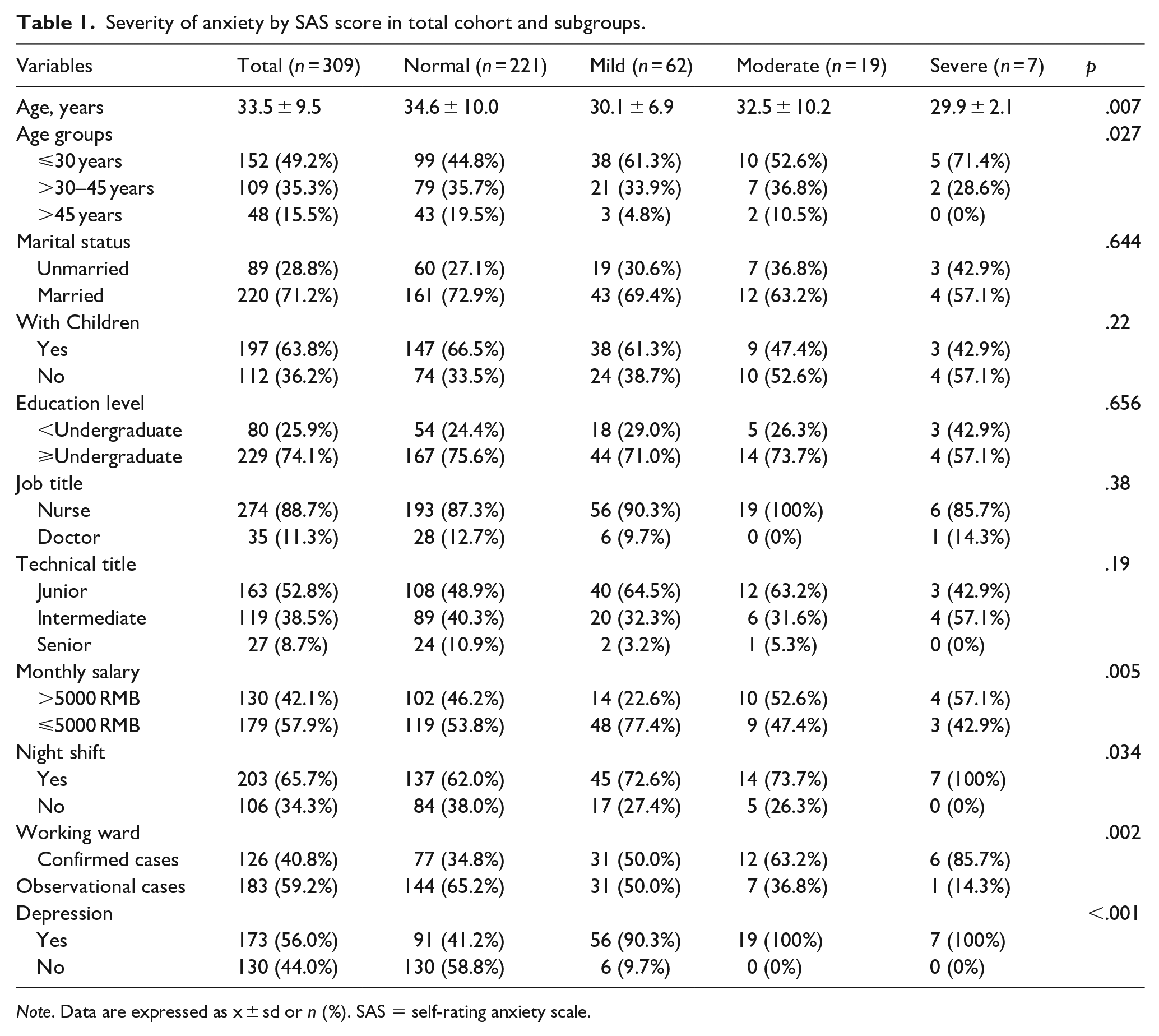
Note. Data are expressed as x ± sd or n (%). SAS = self-rating anxiety scale.
Severity of anxiety by SAS score
Among the 309 participants, there were 88 (28.5%) with anxiety, including 62 (20.1%) mild, 19 (6.1%) moderate and 7 (2.3%) severe anxiety. The mean SAS score was 44.5 ± 10.8 (IQR 36.3–52.5, range 25.8–85.8).The age of participants with anxiety was significantly younger than without anxiety (30.6 ± 7.5 vs 34.6 ± 10.0, p = .001). The prevalence of anxiety was significantly higher in participants with low monthly income, night shift, working in confirmed case isolation wards, and with depression than in those without (33.5% vs 21.5%%, p = 0.02; 32.5% vs 20.8%, p = 0.034; 38.9% vs 21.3%, p = 0.001; 47.4% vs 4.4%, p < 0.001), respectively. Table 1 shows the prevalence of the severity of anxiety in the total cohort and subgroups.
Severity of depression by SDS score
Among the 309 participants, there were 172 (56.0%) with depression, including 137 (44.3%) mild, 34 (11.0%) moderate and 2(0.6%) severe depression. The mean SDS score was 53.1 ± 10.1 (IQR 46–61.3, range 26.3–87).The age of participants with depression was significantly younger than without depression (31.7 ± 8.6 vs 35.8 ± 10.2, p < 0.001). The prevalence of depression in nurses was significantly higher than in doctors (58.8% vs 34.3%, p = 0.007). The prevalence of depression in junior, intermediate and senior medical staffs was 63.2%, 49.5% and 40.7% (p = 0.019), respectively. The prevalence of depression was significantly higher in participants with low monthly income, low education level and with anxiety than those without (70% vs 51.1%, p = 0.004; 63.1% vs 46.2%, p = 0.04; 93.2% vs 41.2%, p < 0.001), respectively. Table 2 shows the prevalence of the severity of depression in the total cohort and subgroups.
Severity of depression by SDS score in total cohort and subgroups.
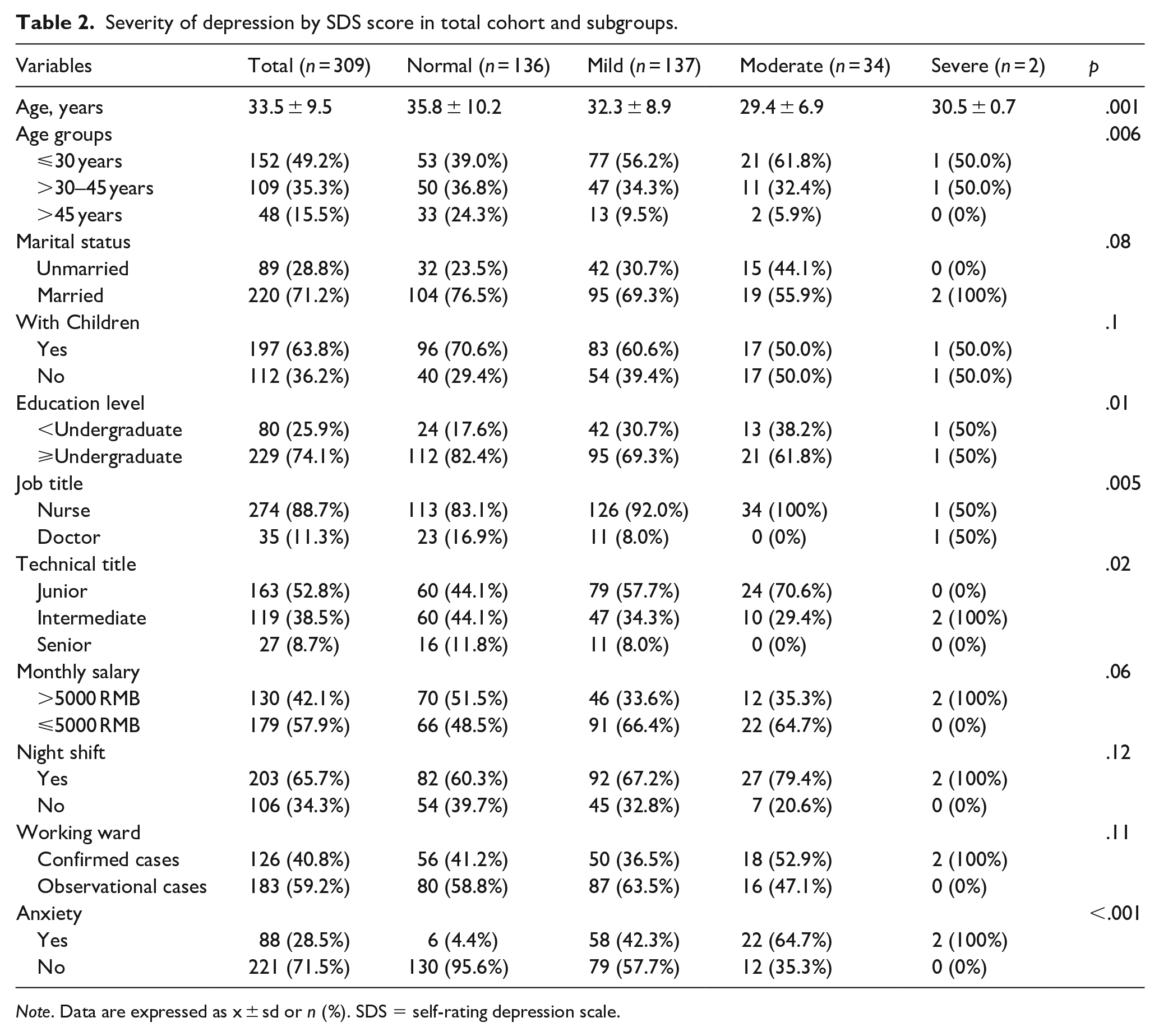
Note. Data are expressed as x ± sd or n (%). SDS = self-rating depression scale.
Stress and perception of threat of Covid-19
Figure 1 shows the answers to the 10-item Covid-19 stress questionnaire in the five-point Likert scale. (1 = strongly disagree, 2 = disagree, 3 = not sure, 4 = agree, 5 = strongly agree)
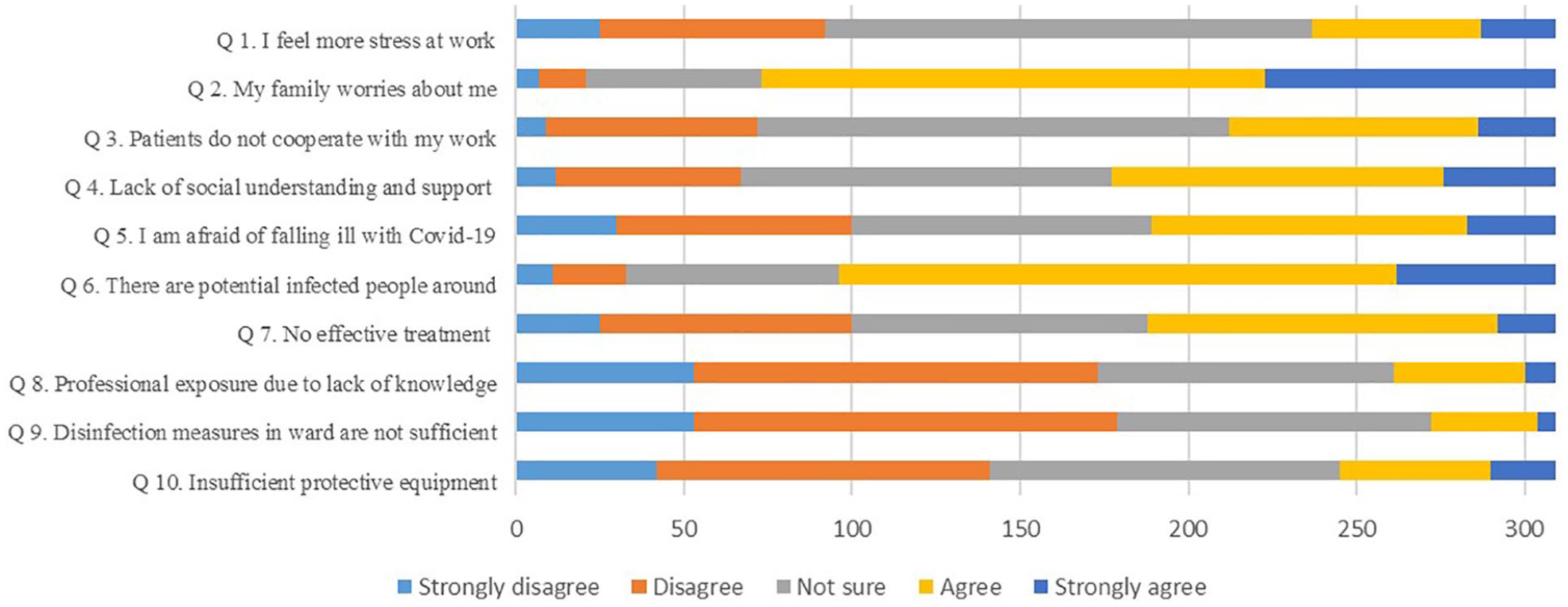
The results of the 10-item Covid-19 stress questionnaire among 309 frontline health care workers.
Table 3 shows the response of the participants to the 10 questions in different subgroups. Only statistically significant results are shown in the table.
Stress and perception of threat of Covid-19 in total cohort and subgroups.
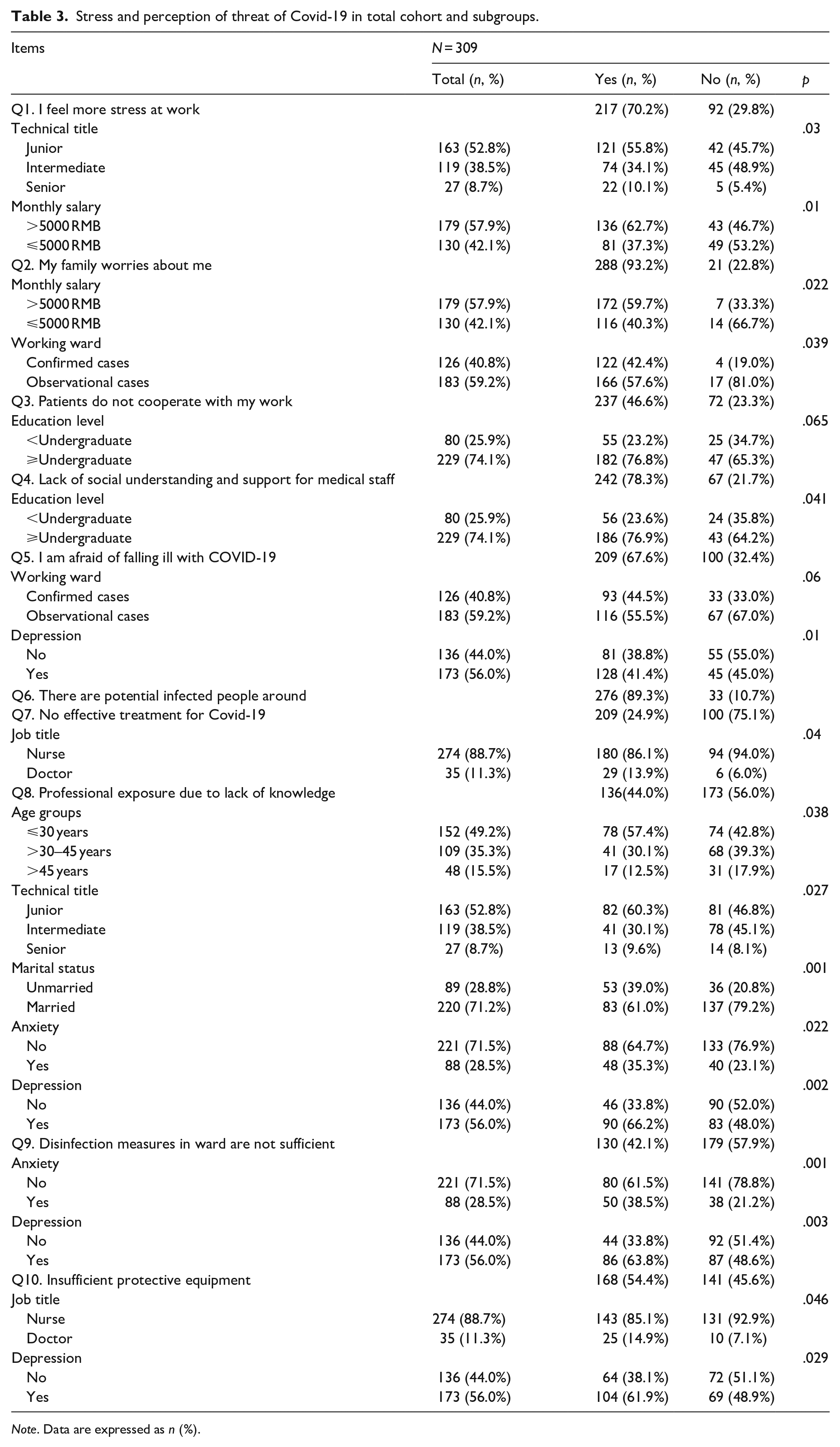
Note. Data are expressed as n (%).
Risk factors for anxiety and depression
Of the 309 participants, 179 (57.9%) had anxiety or depression, 82 had both anxiety and depression, 91 only depression and 6 only anxiety.
The multivariate logistic regression analyses showed that age ⩽ 30 years, age > 30 to 45 years, working in confirmed case isolation wards, and worrying about disinfection measures being not sufficient were independently associated with anxiety with an odds ratio (95% confidence interval, CI) of 4.4 (1.6–12.2), 3.1 (1.1–8.8), 2.3 (1.4–4.0) and 2.5 (1.5–4.3), respectively; age ⩽ 30 years, age > 30 to 45 years, nurse and worrying about disinfection measure being not sufficient were independently associated with depression with an odds ratio (95% CI) of 3.8 (1.8–7.8), 2.7 (1.3–5.7), 2.5 (1.1–5.6) and 2.1 (1.3–3.5), respectively (Table 4).
Risk factors for anxiety and depression identified by multivariable logistic regression analysis.
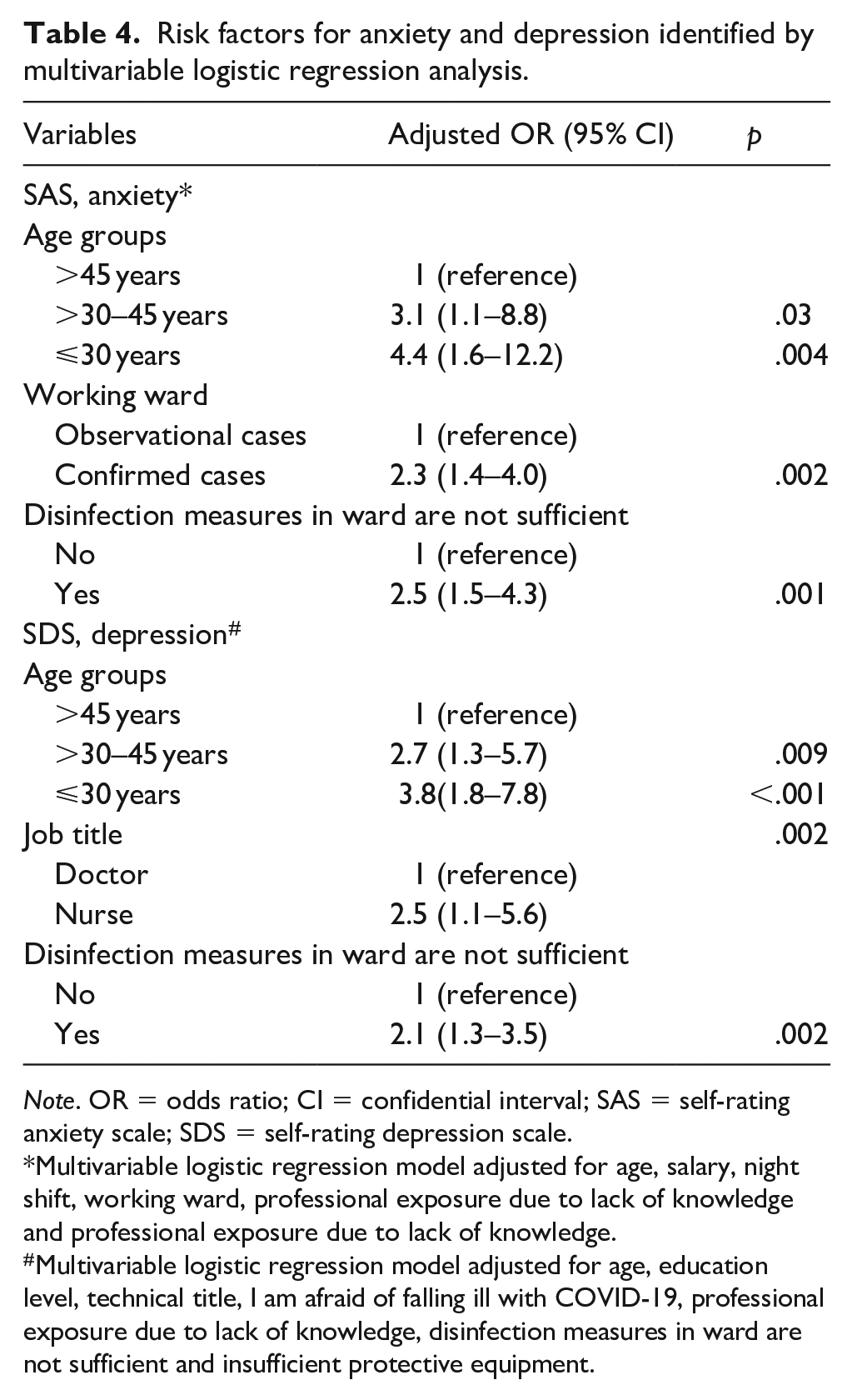
Note. OR = odds ratio; CI = confidential interval; SAS = self-rating anxiety scale; SDS = self-rating depression scale.
Multivariable logistic regression model adjusted for age, salary, night shift, working ward, professional exposure due to lack of knowledge and professional exposure due to lack of knowledge.
Multivariable logistic regression model adjusted for age, education level, technical title, I am afraid of falling ill with COVID-19, professional exposure due to lack of knowledge, disinfection measures in ward are not sufficient and insufficient protective equipment.
Discussion
The present study investigated the anxiety, depression and stress and perception of the threat of Covid-19 in frontline HCWs in a designated hospital during the outbreak of Covid-19 in China. Of the frontline HCWs for Covid-19, more than half (57.9%) had anxiety or depression, which is similar to other studies in frontline medical staffs for Covid-19 (Kang et al., 2020; Lai et al., 2020; Liang et al., 2020), and much higher than that in the general population or other medical staffs (Huang & Zhao, 2020; Wang et al., 2020; Xu et al., 2020). Frontline HCWs are a high-risk group of mental health burden. Identifying the risk factors of mental health and supplying prompt intervention are of great importance.
Working in isolation wards disrupts HCWs’ normal work and life (Thombs et al., 2020). In the present investigation, more than two-thirds of the total participants felt more stress at work. This was more obvious in junior medical staffs. Although there were no critically ill Covid-19 patients in the hospital, they had to have close contact with patients who were infectious, and deal with the emerging infectious disease without effective treatment. Most of them worried about falling ill with Covid-19, due to professional exposure, insufficient disinfection measures in the wards, and shortage of protective equipment, and spreading the disease to family members, colleagues, or friends. Family’s worry and lack of social understanding and support were also sources of stress. In certain cases, HCWs who worked in isolation wards were being labelled as a potential source of infection of Covid-19 by family members, colleagues, and neighbours, and may have been stigmatised. All these damaged the frontline HCWs’ mental health.
Of 309 frontline HCWs, 88 (28.5%) had anxiety. Younger age, low monthly salary, night shift and working in confirmed case wards were risk factors for anxiety. Among medical staffs, being young often means low monthly salary, working on the night shift and lacking experience and knowledge in dealing with severe infectious diseases. About the question ‘Do you worry about professional exposure due to lack of knowledge’, 78/152 (51.3%) in age ⩽ 30 year participant’s answer was ‘yes’, whereas only 41/109 (37.6%) in >30 to 45 year and 17/48 (35.41%) in >45 year participant’s answer was ‘yes’, So, the independent association between younger age and risk of anxiety should not be a surprise. Besides age, another independent risk factor for anxiety was worrying about the insufficient disinfection in isolation wards. Comparing participants without anxiety, a significant higher proportion of those with anxiety worried about the insufficient disinfection in isolation wards (50/88[56.8%] vs 80/221 [36.2%], p < 0.001). Working in confirmed case wards, which may be in continuously stressful, dangerous, or unfamiliar situations for HCWs, was also another independent risk factor for anxiety. Of 88 participants with anxiety, 82 (93.2%) also had depression, a mood disorder that involves a persistent feeling of sadness and loss of interest. It is noteworthy that prevalence of depression was more common than that of anxiety in the participants.
Of 309 participants, 173 (56.0%) had depression. Younger age, nurse, low educational level and junior staffs were risk factors for depression. Compared to doctors, being a nurse often means younger age, lower educational level and junior technical title. In an isolation ward without critically ill patients, nurses had more work tasks and risk of infection than doctors. They had to work in the isolation ward with a thick protective suit in a 4 to 6 hours shift every day, perform intravenous injection, sample collection, faeces disinfection and psychological counselling to the patients. Being a nurse and younger were independent risk factors of depression. Those who worried about ‘falling ill with Covid-19’ (67.6%), ‘professional exposure due to lack of knowledge’ (44.0%), ‘the insufficient disinfection in isolation wards’ (42.1%) and ‘insufficient protective equipment’ (54.4%) had a high risk of depression. Similar to that of anxiety, worrying about the insufficient disinfection in isolation wards was also an independent risk factor for depression. Compared to participants without depression, a significant higher proportion of those with depression worried about the insufficient disinfection in isolation wards (86/173 [49.7%] vs 44/136 [32.4%], p = 0.003).
The SAS and SDS are for primarily tools for screening or assessing/monitoring symptom severity of anxiety and depression, not scales for diagnosis, so the HCWs in our investigation were just showing emotion of anxiety or depression, not patients with anxiety or depression. Besides, anxiety is the feeling of fear that occurs when faced with threatening or stressful situations. It is a normal response when confronted with danger, but, if it is overwhelming or the feeling persists, it could be regarded as an anxiety disorder. Perhaps, the mild anxiety is not completely bad, even beneficial to work among HCWs during COVID-19 pandemic. The present study has limitations. First, the psychological assessment was based on an online survey and on self-reporting tools. Second, since there were only eight men in the study, it is difficult to assess the sex difference in mental health. Third, currently Shandong Province is a low endemic area of Covid-19 in China, and there were no critically ill patients in the hospital.
In conclusion, a higher prevalence of anxiety and depression was found among frontline HCWs during COVID-19, more psychological care should be given to young staffs and nurses. Hospital infection education, adequate protection measures and sufficient isolation ward disinfection to prevent professional exposure is important for HCWs’ physical and mental health.
Footnotes
Acknowledgements
Thanks to Dr. Edward C. Mignot, Shandong University, for linguistic advice.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present work was supported by Jinan Science and Technology Bureau (grant number 202001005).