
Abstract
Background:
Domestic violence, childhood physical and sexual abuse, and gang violence are prevalent and growing problems for Guatemalan youth, particularly in low socioeconomic (SES) areas. Resources in the community for psychosocial support are greatly lacking. Schools often serve as the main source of support for these highly vulnerable adolescents. Yet, many teachers lack the training to manage the psychological distress of their at-risk students and to properly engage, assess, and manage the psychological needs of their students. We developed a brief risk assessment and management training for teachers to address this gap.
Aims:
We present the acceptability and preliminary effectiveness of the training at increasing teacher’s knowledge and understanding of how to engage and work with their at-risk students around their thoughts and feelings of suicide.
Method:
Twenty-two teachers from a school in a low SES community in Guatemala participated in the training program. Mixed methods were used to explore effectiveness, acceptability, and satisfaction with the training. Primary outcomes assessed were changes in self-reported knowledge and understanding of engaging and working with students at risk of suicide.
Results:
Participants reported increased knowledge and understanding of all training targets (p < .05). Acceptability was high as no participants dropped out and all participants rated the training as useful for their professional development, meeting their expectations, and as highly satisfying.
Conclusion:
Brief, focused training on suicidality can be effective and is acceptable to lay professionals. Further examination of the effectiveness of the training in a larger sample is required to assess the long-term impact of the training and its transportability to other communities.
Background
Studies consistently demonstrate that family, peers, school, neighborhood, and community play a central role in the emotional lives of young people. When those relationships are characterized by violence, and/or abuse, risk of depression and suicidality is increased, particularly among adolescents (Alonzo & Gearing, 2018; Hornor, 2010; Johnson et al., 2002; Park, 2015; Puac-Polanco et al., 2015; Randell et al., 2006; Wells et al., 2012). These issues are particularly relevant in Guatemala. A divided law enforcement system; government corruption; family and community fragmentation; a pervasive criminal culture; endemic poverty; discrimination; gender-based violence; the high prevalence of illegal drugs and gangs; and, fear, intimidation, and distrust in government and public officials resulting from 36 years of armed civil conflict have contributed to create a highly fractured society (Alvarado & Massey, 2010; Branas et al., 2013; Garcia, 2004; Rodriguez et al., 2002). Studies have noted that as much as 40% of Guatemalan territory is largely beyond the control of the police and the central government (Brands, 2011; Gavigan, 2009). Rates of domestic and familial violence are the highest in Latin America and some of the highest in the world (Ogrodnik & Borzutzky, 2011). Twenty-eight percent of women and 26% of men reported witnessing parental violence, and at least half of these reported receiving beatings as children (Speizer et al., 2008). Twenty-six percent of mothers and 20% of fathers reported using corporal punishment with their children (Speizer et al., 2008).
Given the widely established association between violence, abuse, and mental illness (Hillberg et al., 2011; Lagdon et al., 2014; Trevillion et al., 2012), it is not surprising that recent studies indicate high rates of mental illness in Guatemala (Branas et al., 2013; Puac-Polanco et al., 2015). One study found that one in five Guatemalans have experienced serious violent events, and violence was significantly associated with subsequent mental health problems especially for vulnerable groups such as women, indigenous groups, and the urban poor (Puac-Polanco et al., 2015). Prevalence estimates of 40.7% for depression, 23.3% for alcohol-related disorders, and 50% for PTSD have been reported in Guatemala (Branas et al., 2013). Among the people directly affected by the armed conflict, depression rates have been found to range between 38.8% and 41.8%; for anxiety symptoms, rates range between 27.7% and 54.4%; and posttraumatic stress disorder (PTSD) rates range from 2% to 52% (Herrera et al., 2005).
In terms of suicide, some research indicates that there is one suicide a day in Guatemala and 2.47 suicides per 100,000 inhabitants (WHO, 2016). Rates among youth have been increasing over since 2000 (Pengpid & Peltzer, 2019). Additionally, it is estimated that approximately 51% of those suicides were between the ages of 10 and 29. Among adolescents, the prevalence of past 12-month suicide attempt was 16.6% overall with, 12.2% among boys and 20.2% among girls (Pengpid & Peltzer, 2019). However, it is noted that suicide rates are significantly underestimated due to under-reporting and/or misclassification (Mijangos et al., 2017; Pengpid & Peltzer, 2019; WHO, 2014). For example, few national statistics exist on suicide in Guatemala, largely because deaths due to suicide are generally recorded in terms of their ultimate cause, such as poisoning, strangulation, or shooting, without necessarily indicating that the death was caused by suicide (Mijangos et al., 2017; WHO, 2014).
This is especially concerning as mental health treatment utilization is particularly low among Latino populations (Alonzo et al., 2016; Alonzo & Gearing, 2018; Cauce et al., 2002; Derr, 2015; Keyes et al., 2012). Several factors have been found to be associated with service utilization in this population. Attitudes about mental health treatment, such as receptivity to care, embarrassment, and stigma have been linked to limited mental healthcare help-seeking and to lower utilization of formal mental health treatment. (Alonzo et al., 2016; Alonzo & Gearing, 2018; Cauce et al., 2002). Contextual and systemic factors, including the availability of services within the community and social networks that can provide referrals to them also impact utilization rates (Cauce et al., 2002). Social norms play a critical role as they dictate whether a behavior is deemed acceptable and desirable or deviant and cause for concern (Cauce et al., 2002). In a neighborhood characterized by familial and gang violence, parents may not consider their adolescent’s aggressive or withdrawn behavior as concerning or out of the norm. Further, an adolescent experiencing depression and suicidal thoughts or behaviors in response to this violence may be less likely to disclose such thoughts and feelings out of fear of appearing weak or unable to cope the way the rest of one’s peers in the community do.
Further contributing to the limited utilization of mental health treatment among at risk youth is the scarcity of resources for receiving mental health treatment in Guatemala, especially in the poorest communities (Godoy-Paiz, 2005). The few organized mental health services that do exist in the country are not readily accessible to the majority of the population and most often are inadequate (Godoy-Paiz, 2005). In low-income areas where risk of mental illness is highest, the minimal charge for a therapist is 50 quetzales per hour (approximately $6 USD), a rate equivalent to 2 days of work. In wealthier neighborhoods, experienced clinical psychologists charge three times that amount or the equivalent to close to a week’s pay for a laborer, farm worker, or maid (Godoy-Paiz, 2005), rendering the utilization of mental health care cost-prohibitive above and beyond other structural barriers such as having to travel long distances to find a mental health care provider.
Under such conditions of limited formal mental healthcare help-seeking, utilization, and resources, schools often become the main de facto providers of mental health services for youth despite not being designed or equipped to manage students’ mental health problems (Atkins et al., 2010; Burns et al., 1995; Cauce et al., 2002; Farmer et al., 2003; Rones & Hoagwood, 2000). Within this setting, teachers are in the best position to affect change and support students as they have the most contact with them and they control the classroom setting where children and youth spend the majority of their time (Atkins et al., 2008).
However, in order to be effective in taking on this role, teachers need the knowledge and understanding to engage and work with at risk students. This requires specialized, focused training. This study aimed to examine the acceptability and effectiveness of a new training program for teachers, Formacion CUIDAR_E (Comunidades Unidos para Individuales De Alto Riesgo para Educadores)/CARE_E Training (Communities United for Individuals at High Risk for Educators), to improve knowledge and understanding of how to engage and work with youth at risk of suicide.
Method
Procedures
We conducted an uncontrolled trial of Formacion CUIDAR_E/CARE_E Training in Peronia, Guatemala. Participants received an 8-hour training over the course of 2 days focused on: (1) key developmental issues related to adolescent mental health; (2) core components of an effective suicide risk assessment; and (3) evidence-informed strategies for managing adolescent suicidality. Training material was delivered in a workshop format comprised of lectures, role-plays, and small group exercises. Primary outcomes were changes between pre- and post-training on self-reported knowledge and understanding of how to engage and work with students at risk of suicide.
The authors served as the trainers for this study. Both are PhD level professors from a large urban University in New York City, USA. The first trainer has approximately 20 years of research and clinical experience working with individuals at risk for suicide, developing interventions aimed at increasing treatment engagement of at-risk individuals, and has conducted trainings nationally and internationally focused on suicide prevention, assessment, management, and intervention. She is also founder and director of the Suicide Prevention Research Program that focuses on cross-disciplinary efforts to improve suicide risk identification and develop new interventions aimed at reducing suicide risk. The second trainer has over 20 years of experience in international development and community capacity building as well as extensive research on domestic violence, violence against women, and women’s rights. She has developed several international trainings for community partners, focusing on community capacity building, domestic violence, violence against women, and program evaluation for community-based organizations.
Participants
Twenty-two teachers participated in the training. Inclusion criteria included current employment/teaching at a school. The school is located in Peronia, a ‘red zone’ district outside of Guatemala City. ‘Red zone’ districts are characterized by overcrowding, pollution, and violence of multiple types. Violent crime, including armed robbery and murder, is common. Gang activity, such as extortion, violent street crime, and narcotics trafficking, is rampant. Abuse and neglect occur at high rates. Access to electricity and water is limited, and sporadic cable and Wi-Fi, if any, is available, yet not reliable even when available.
We developed the training protocol to address the needs of non-mental health care professionals engaging with at-risk youth in a community where formal services do not exist and they may serve as the only source of support. We focused on: (1) key developmental factors in childhood and adolescence that impact mental health to provide an understanding of the context contributing to the onset of mental health issues among youth; (2) psychological and behavioral responses to exposure to violence and abuse highlight the contribution and impact of this highly common situation in this community; (3) risk and protective factors for suicide to aid in risk identification; (4) core components of suicide risk assessment to inform engagement and assessment efforts; (5) identifying personal beliefs and values regarding suicide to highlight their role in the engagement and assessment process; (6) strategies for engaging at risk youth and their care-takers to provide concrete steps that they can take to serve as an effective support; and (7) tools for managing at risk youth (i.e., safety planning and key CBT techniques) to provide techniques they can use effectively without requiring significant training in clinical practice.
The training consists of five core lectures focused on: (1) key considerations in adolescent development related to depression and suicidality (cognitive development; autonomy; relatedness, competence, self-direction; adverse childhood experiences); (2) warning signs, risk, and protective factors for suicide; (3) suicide assessment strategies; (4) CBT: theory, strategies, and techniques; and (5) safety planning. Total lecture time is 5 hours. Role-play exercises of assessment strategies and small group exercises (four to five participants per group) examining case vignettes of at risk youth are used to reinforce the concepts in the lectures and to highlight attitudes, assumptions, and biases regarding suicidality. Large group discussions led by the facilitators are used to review material and debrief on exercises. Total exercise and discussion time is 3 hours.
Training topics included in Formacion CUIDAR_E/CARE_E are evidence informed. Research suggests that helping professionals are generally hesitant to work with individuals at-risk of suicide. They most often report fear, discomfort, a lack of confidence, and feeling ill-prepared to work with at-risk individuals (Feldman & Freedenthal, 2006; Jacobson et al., 2004; Singer & Slovak, 2011; Ting et al., 2011). In addition, they tend to use negative non-verbal behavior and judgments when working with this population (Pompili et al., 2005; Sethi & Shipra, 2006, Tapola et al., 2016). This fear, hesitancy, and discomfort have a clear and direct impact on the at-risk client’s experience of help-seeking. Therefore, for any training to effectively improve the likelihood that helping professionals will successfully engage with individuals experiencing suicidal thoughts and behaviors, it is essential to equip them with the knowledge and skill needed to feel comfortable, confident, and prepared to address suicide risk. Operationalizing this has been done in a number of different ways across various gate-keeper training programs based on setting and participant background (both mental health professionals and lay professions [i.e., educators, nurses, etc.]). However, it is generally recommended that providing information regarding background factors contributing to the onset of suicidal thoughts/behaviors; knowledge of warning signs and risk/protective factors; how to conduct an accurate assessment of risk; and providing basic, evidence-based intervention strategies (i.e., safety-planning) are essential for helping professionals to feel confident and prepared to engage, assess, and intervene (Brodsky et al., 2018; Gould et al., 2013; Kitchener & Jorm, 2002; Osteen et al., 2014; SAMHSA, 2020; Van der Feltz-Cornelis et al., 2011).
Further, we utilized an approach grounded in a deep understanding of local problems and assets in an effort to improve the feasibility and acceptability of the training. As such, the training material centered on culturally relevant risk and protective factors for suicide among youth in Guatemala (i.e., an emphasis on intra-familial and community violence). Additionally, the assessment and management strategies included were based on the cultural and familial values and norms of the population (i.e., machismo, familismo).
Measures
Acceptability and satisfaction
Acceptability of was assessed by participants’ self-reported ratings of the usefulness of the training; satisfaction with the training; the degree to which the training met their expectations; and by the rate of completion of the training.
Baseline characteristics
A questionnaire developed by the study PIs and used in other trainings programs was used to assess sociodemographic characteristics of the participants. Sociodemographic variables gathered included participants’ age, sex, level of education, and years of professional experience.
Teachers’ opinions regarding the role of educators and the education system in relation to youth mental health were assessed with two items rated on a 5-point Likert scale (1 = not at all; 5 = a great deal) including: ‘Based on your experience, is adolescent mental health a critical issue for educators?’, and ‘In your opinion, to what extent is adolescent mental health a priority in national education policy?’
Pre- and post-test knowledge
Knowledge was assessed at pre- and post-test by five items on which participants rated their knowledge and understanding of various developmental and psychological concepts related to youth suicidality on a 5-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree. Items included, ‘I am confident in my knowledge about the role of risk and protective factors in adolescent mental health’, ‘I am confident in my knowledge about the role of cognitive development and autonomy in adolescent mental health’, ‘I am confident in my ability to engage with adolescents to address their needs’, ‘I am confident in my ability to engage parents in the process of supporting their adolescent children’, and, ‘My understanding of the meaning of resiliency’.
To capture qualitative data regarding learning derived from the training, teachers were also asked to respond to one open-ended question regarding knowledge gained. More specifically, teachers were asked to answer the open-ended question, ‘Please indicate one key learning point you take from this training’.
Data analysis
Quantitative analysis
All statistical analyses were conducted using SPSS version 20. Descriptive statistics, including means, standard deviations, and skewness were calculated for all variables. Paired t-tests were used to analyze mean differences in pre-test and post-test scores. p-values equal to or less than .05 were considered statistically significant. Missing data were replaced with the mean. Replacing missing values with the mean is a standard method used to estimate missing values (Tabachnick & Fidell, 2001).
Qualitative analysis
Theme-based content analysis of the qualitative data was the primary analytic approach used. Participants’ responses were reviewed by all authors to identify recurring themes. Using an inductive approach, these units were then collapsed to create a set of preliminary categories. The categories were then clustered and themes identified. Following this, all coders then compared and discussed their results and consensus was reached on the final set of themes. Initial coding was conducted independently after which team meetings were held to review the categories and idiosyncratic and/or redundant responses were removed. In the case of discrepancies, definitions of the categories were clarified and rating was repeated until inter-rater consistency of at least 80% for these items was reached, per standards in the literature (Shek et al., 2005). Quotations that reflect the major identified themes are reported in the findings section in addition to the summary, description, and interpretation of the themes.
Results
Participants were largely female (68.2%) with a mean age of 32.41 (SD = 10.07). Participants’ had on average 9.82 (±8.31) years of experience as teachers for grades one to six. The majority of participants had a degree in teaching. Teachers reported a belief that mental health was a critical issue for educators (Mean 4.56 [SD = 0.824]), yet, it was not strongly perceived as a national priority (Mean 3.12 [SD = 1.472]) (see Table 1).
Sociodemographic characteristics of the sample.
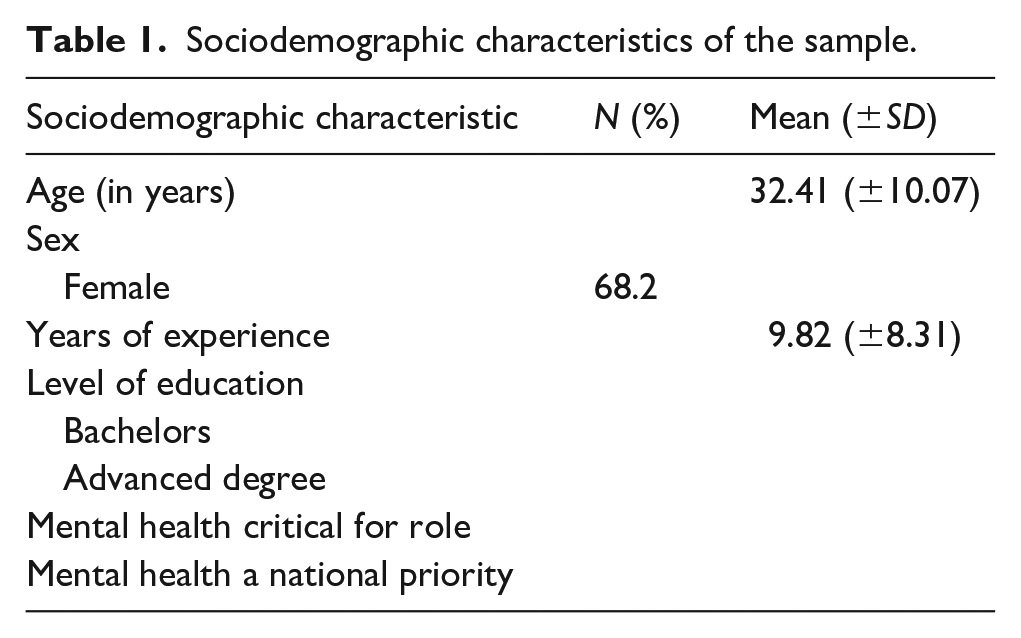
Table 2 shows the change in total outcome scores. Participants experienced significant self-reported increase in knowledge as a result of the training (t = 2.46, p = .05, Cohen’s d = 0.56). Additionally, the Cronbach’s alpha for knowledge scale was .864, indicating a high internal consistency of all scale items.
Results of paired t-test indicating change in scores from pre-test to post-test.

High retention rates were achieved with 99% of participants completing the training, demonstrating high acceptability of the program. Table 3 reports the results regarding the participants’ ratings of acceptability of and satisfaction with the training. Participants reported that the program met their expectations (Mean 4.80 [SD = 0.414]); was useful for their work and professional development (Mean 4.93 [SD = .267]); and, that they were satisfied with the training they received (4.93 [SD = .258]), indicating high acceptability of and satisfaction with Formacion CUIDAR_E.
Self-reported learning outcomes by frequency.

Results of the qualitative analyses showed that participants identified several key learning areas resulting from the training including Assessment, Reducing Stigma, and Engaging with At-risk Adolescents. The single most identified learning point was risk factors for suicide, identified by 27% of participants (see Table 3).
The most frequently endorsed area of learning identified was the area of assessment, representing 40% of learning points identified. Comments from participants related to this area indicated that they felt they learned: ‘Tips about understanding suicide risk’, ‘Signs of suicide’, ‘Questions one should ask during assessment’, ‘Understanding suicide risk’, ‘Factors impacting suicide risk’, and ‘Better understanding of the situations of my students and how they impact them’.
The next identified area of learning was the importance of reducing stigma, representing 33% of learning points identified. Participants commented: ‘Suicide should not be taboo’, ‘We should talk about suicide’, ‘We need to leave prejudices behind’, ‘Mental health of youth needs to be understood’, and ‘Mental health should be a school priority’.
The third identified area of learning was how to engage and work with adolescent students around their mental health issues, representing 27% of all learning points identified. Comments in this area included: ‘How to be an adequate support to students who need emotional help’ and ‘How to support and create a pleasant learning environment for at-risk adolescents’, ‘How to be an adequate support for students who need help’, and ‘Understanding that even though adolescents don’t act like it, they still want to be cared for’.
Discussion
This is the first study to examine the effectiveness of a culturally relevant training for teachers in Guatemala focused on developing their knowledge and skills regarding suicide risk assessment and management and to improve their ability to engage with high-risk youth experiencing suicidality. Our results indicate that Formacion CUIDAR_E/CARE_E Training is acceptable among teachers and is effective at increasing knowledge and understanding of youth at risk of suicide.
Our results are consistent with previous research examining teachers’ role in relation to at-risk youth. This research identifies schools as an important resource for promoting positive mental health and facilitating the pathway into mental health treatment for adolescents. Teachers report that while they believe addressing students’ mental health needs is part of their role, they describe an overall lack of experience and training needed to adequately support their students’ mental health needs (Mazzer & Rickwood, 2015; Nadeem et al., 2011; Reinke et al., 2011).
Current research also indicates that youth with mental health needs often experience less supportive teachers (Ball & Anderson-Butcher, 2014; Holen et al., 2018; Kidger et al., 2009; Moses, 2010; Roeser & Midgley, 1997). This highlights the critical importance of increasing teachers’ understanding of the factors that contribute to the mental health of their students in order to have a direct impact on their ability to support youths’ emotional health and well-being (Graham et al., 2011; Kutcher et al., 2013).
Overall, training on youth mental health in general and suicide risk assessment and management in particular can help teachers to feel better prepared to effectively and appropriately engage with at-risk students. At present, this type of training focused on providing teachers with the skills and knowledge needed to be willing and able to engage, assess and manage suicidal youth is largely lacking in high-risk communities in Guatemala and throughout most of Latin America. Even in the United States, most school-based interventions target school mental health professionals (i.e., school social workers, school psychologists). These types of interventions are limited in their impact as they do not serve to equip key non-mental health care professionals, such as teachers, with needed knowledge and skills to support their students. They also can only be implemented in schools that have specialized mental health care providers in-house, which overlooks many of the schools in the poorest neighborhoods who lack these resources and where the need is extremely high. Formacion CUIDAR/CARE Training addresses this gap and provides teachers with the training they need to effectively carry out their role and serve as a support to their students.
Limitations
This study has some limitations worth noting. First we did not utilize a randomized control trial (RCT). Further testing of the training using an RCT would be important for a more robust evaluation effectiveness. However, as this was a pilot study, an uncontrolled design to explore acceptability and preliminary effectiveness is reasonable. Further, we did not use a standardized pre- and post-test to evaluate the training instead opting to customize our evaluation items to the community, setting, and participants. Our approach, however, is supported by research suggesting such an idiographic approach to treatment and, by extension, clinical research, can lend to greater understanding (Sales & Alves, 2012) and emphasizes the benefit of developing a unique evaluation tool that is both meaningful and important to participants (Lingham et al., 2006). This is a consideration for future studies. Additionally, at-risk youth were not assessed for their opinion regarding whether the training improved the care they receive. Future studies may want to explore the client perspective to better understand the impact of the training. Additionally, we did not control for teachers’ attitudes towards working with youth struggling with mental health issues and expressing suicidality. An important next step would be to assess if attitudes change a result of the training or if they interfere with the implementation of the knowledge and understanding gained via the training. Additionally, teachers from a wide range of grades were included in the trainings. This limits our ability to assess with age of the student has any impact on the effectiveness of the training. Lastly, the long-term effects of the training were not assessed. Additional studies are needed to determine if the improvements reported by the participants are implemented and maintained over time.
Conclusion
In the face of scarce resources and low utilization of available mental health services, school, and teachers in particular, often serve as a primary source of support for youth struggling with depression and suicidality. Results of our study demonstrate that our training is acceptable effective program for non-mental health professionals to develop the knowledge and skills they need and to increase their ability to support their at-risk young students around their mental health needs. Future research should explore the effectiveness of the training at ameliorating the psychological distress of at-risk adolescents, the long-term impact of the trainings, including the contribution of such training in building local capacity to better respond to risks of harm and self-harm among children and youth in Guatemala, the attitude of teachers to serve in the gate-keeper role and the effectiveness of the training at improving motivation and willingness to do so, and the generalizability of the training to other high-risk settings and populations.