
Abstract
Psychological distress is associated with a range of negative outcomes including lower quality of life and an increased risk of premature all-cause mortality. The prevalence of, and factors associated with, psychological distress among middle-aged and older Canadians are understudied. Using the Canadian Longitudinal Study on Aging (CLSA) baseline data, this study examined factors associated with psychological distress among adults between 45 and 85 years, including refugee status and a wide range of sociodemographic, health-related and social support characteristics. Psychological distress was measured by Kessler’s Psychological Distress Scale-K10 scores. Bivariate and multivariable binary logistic regression analyses were conducted. The prevalence of psychological distress was significantly higher among the 244 refugees (23.8%), compared to 23,149 Canadian-born Canadians (12.8%) and 4,765 non-refugee immigrants (12.6%), despite the fact that the average time the refugees had lived in Canada was more than four decades. The results of the binary logistic regression analysis indicated refugees had twice the age-sex adjusted odds of psychological distress (OR = 2.31, 95% CI: 1.74, 3.07). Even after further adjustment for 16 potential risk factors, a significant relationship remained between refugee status and psychological distress (OR = 1.56; 95% CI = 1.12, 2.17). Other significant factors associated with psychological distress included younger age, female gender, visible minority status, lower household income, not having an undergraduate degree, multimorbidities, chronic pain, and lack of social support. Policies and interventions addressing psychological distress among Canadians in mid- to later life should target refugees and other vulnerable groups.
Keywords
Introduction
Psychological distress is an important but neglected mental health issue. Psychological distress, a state of emotional suffering, is included as a diagnostic criterion for several psychological disorders (e.g. depressive disorders, anxiety disorders) and as a marker of symptom severity (Phillips, 2009). Between one in five (Caron & Liu, 2011) and one in eight Canadians (Enticott et al., 2018) experience psychological distress and there is a strong negative association between psychological distress and quality of life (Atkins et al., 2013). Psychological distress is more prevalent among those with serious physical health problems including back pain (Power et al., 2001), coronary heart disease (Rasul et al., 2005), myocardial infarction and stroke (Jackson et al., 2018), and Alzheimer’s disease (Wilson et al., 2003). It is also associated with an increased risk of premature all-cause mortality (Batty et al., 2017; Russ et al., 2012).
The prevalence of psychological distress is higher among women (Matud et al., 2015; Stallman et al., 2010) as well as individuals who are unemployed (Reneflot & Evensen, 2014), without a partner (Darghouth et al., 2015), with a lower level of education (Miech et al., 2007) and with low income (Orpana et al., 2009). Some studies indicate that younger adults report a higher level of psychological distress than older adults (Chittleborough et al., 2011), while other research has found that older age is associated with a greater risk of experiencing distress (Atkins et al., 2013; Goulia et al., 2012). Other studies have reported a U-shaped relationship between age and distress, suggesting that the prevalence of mental distress is highest among younger and older age groups (Cairney & Krause, 2005; Schieman et al., 2001).
Among older adults, access to appropriate resources and perceived social support is protective against psychological distress (Sharpley et al., 2015). Greater perceived social support is significantly associated with lower levels of distress among White Americans, but this relationship is not found among African Americans (Morin & Midlarsky, 2016). Women are more likely to pursue emotional support than men (Matud & García, 2019). The positive impact of social support on psychological distress appears to vary among different groups and populations, suggesting additional research is needed.
When compared to the general population, a number of studies reported that immigrants are more likely to experience higher levels of psychological distress (Chen et al., 2017; Honkaniemi et al., 2020; Li & Anderson, 2016; Ryan et al., 2008; Torres & Wallace, 2013). While many studies did not differentiate between refugees and non-refugee immigrants, some studies did suggest that those who are forced to migrate are particularly prone to psychological distress (Ryan et al., 2008; Torres & Wallace, 2013). Recent studies from the USA, New Zealand, Australia, Italy, Germany, and Malaysia indicate that the prevalence rates of psychological distress are high among refugees (Alemi & Stempel, 2018; Guajardo et al., 2016; Ryan et al., 2008; Shaw et al., 2019; Walther et al., 2020). A German study found that more than two in five of the refugees they surveyed had psychological distress (Walther et al., 2020). An Italian study on asylum seekers and refugees found that more than one-third of the participants (36%) showed clinically relevant psychological distress (Nosè et al., 2018). The higher levels of psychological distress among refugees may be a result of pre-migration trauma they experienced in their country of origin (Alemi & Stempel, 2018; Chen et al., 2017; Li & Anderson, 2016). Post-migration resettlement stressors such as long periods of resettlement (Guajardo et al., 2016), the inability to speak a host country’s language (Singh et al., 2015), difficulties in having foreign credentials and work experience recognized, settlement arrangements, employment, and racial, ethnic and/or religious discrimination (Alemi & Stempel, 2018; Honkaniemi et al., 2020; Kim et al., 2018; Shaw et al., 2019) may also negatively impact mental health and wellbeing among refugees.
Only a few studies have investigated psychological distress among specific refugee populations in Canada. One study of Sudanese refugees in seven cities in Ontario reported that economic hardship was associated with greater psychological distress (Simich et al., 2006). A study of Sri Lankan Tamil refugees in Canada showed that the level of psychological distress was associated with pre-migration trauma, the number of children in a family, and daily stressors (George & Jettner, 2016). More work is therefore needed to investigate the unique factors that impact refugees’ mental health and wellbeing.
Grounded in the social determinants of mental health framework (Allen et al., 2014; Hynie, 2018), which suggests that an individual’s mental health culminates from the interplay of various social, economic, and physical environments operating across the lifespan (World Health Organization and the Calouste Gulbenkian Foundation, 2014), the current study aims to explore the relationships between a range of social characteristics and psychological distress among refugees, non-refugee immigrants, and Canadian-born adults in mid-to-later life. The following research questions will be addressed:
(1) Do both refugees and non-refugee immigrants in Canada have a higher prevalence of psychological distress compared to those born in Canada?
(2) Are there demographic, economic, health-related, and social factors that attenuate the association between refugee status and psychological distress?
(3) What factors are significantly associated with psychological distress after accounting for refugee and immigrant status?
Methods
Participants and procedure
The detailed methodology has been previously published (Lin et al., 2020). To summarize, this study used the comprehensive cohort data from the baseline Canadian Longitudinal Study on Aging (CLSA, n.d.), a 2012 population-based study of Canadians aged 45 to 85 years who will be followed for 20 years (Raina et al., 2009). The comprehensive sample consisted of 30,097 respondents. Information was gathered via in-home interviews and physical assessments drawn from dedicated data collection sites. Telephone interviews were conducted 18 months after the initial assessment to maintain contact. This study used data from the In-Home Questionnaire and Data Collection Site Questionnaire and the Maintaining Contact Questionnaire. Those who did not report their mental health status, refugee/immigration status, marital status, multi-morbidities, and or social support availability were excluded (n = 1,939), yielding a final sample size of 28,158. The excluded subjects did not differ significantly from the main group with respect to demographic characteristics. Further details about the study protocol can be found at www.clsa-elcv.ca.
Measures
Outcome variable
Psychological distress was measured using the Kessler Psychological Distress Scale (K10) (Kessler et al., 2002), a 10-item screening questionnaire that yields a global measure of non-specific distress based on questions about anxiety and depressive symptoms experienced in the previous four weeks. The overall K10 score (range: 10–50) was obtained by summing the individual response values that range from “all of the time” (score of 5) to “none of the time” (score of 1) (Andrews & Slade, 2001). A cut-off score of 20 or more (K10 score ⩾ 20) was used to categorize those who had a mild mental disorder (Vasiliadis et al., 2015). K10 has been reported to have good sensitivity (0.80) and specificity (0.81) for any depressive and/or anxiety disorder (Sakurai et al., 2011).
Main independent variable
Refugee/immigrant status was classified into three levels: (1) Canadian-born residents; (2) non-refugee immigrants; and (3) refugees. Because the CLSA did not include specific questions about refugee status, a proxy measure for refugee/immigrant status was created based upon self-reported information of being an immigrant, country of birth, year of arrival in Canada, religion, cultural background and parental ethnic background to match the demographics of historic refugee cohorts (see Table 1). Among refugees (n = 244), the average time since arrival in Canada was 43 years (SD ± 16.2 years). Only 2.5% of refugees (n = 6) had arrived in Canada in the 10 years preceding baseline CLSA data collection and 37.3% (n = 91) had arrived 50 or more years before they were surveyed.
Refugees’ regions of origin and era of immigration (n = 244).
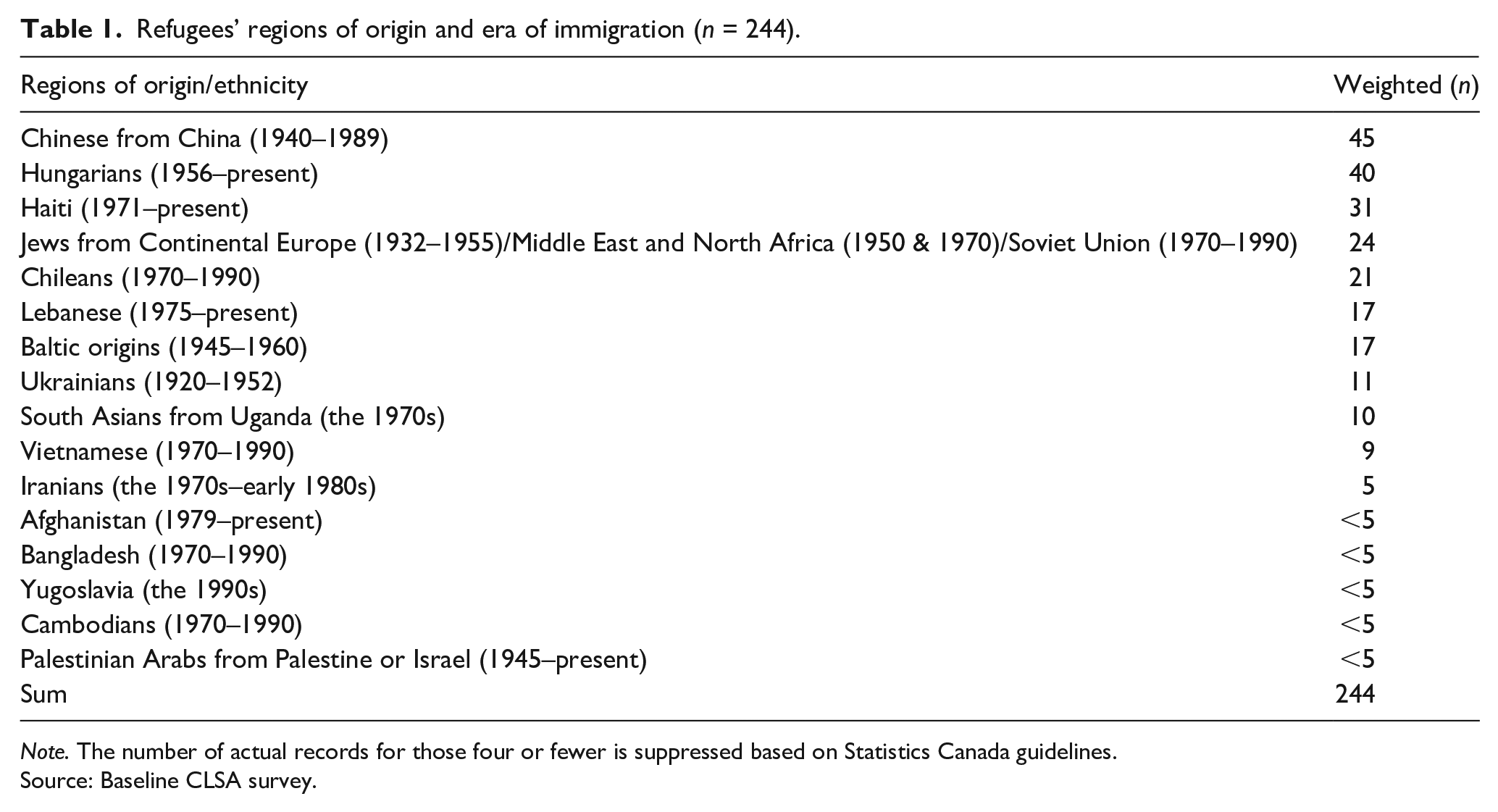
Note. The number of actual records for those four or fewer is suppressed based on Statistics Canada guidelines.Source: Baseline CLSA survey.
Covariates
Besides refugee/immigrant status, other demographic covariates such as age, sex, and marital status were controlled in the core block, because they influence the chances of being exposed to stressful events (Fenta et al., 2004). In addition to the demographic correlates, five different clusters of potential effect modifiers were examined separately to determine the independent contribution of each additional block.
The cluster of socioeconomic factors included annual household income, education level, and subjective report of retirement status.
The cluster of health status and behaviors, consistent with prior operationalization (Davison et al., 2019, 2020), measured multi-morbidities (no condition/one health condition/two health conditions/ three or more health conditions), chronic pain (free of pain/ have pain/no answer), drinking habits in the previous year (non-binge drinker/binge drinker/no answer), and physical activities in the previous seven days (never or seldom/sometimes or often/no answer).
The cluster of social connections captured both social isolation and online social networking. The social isolation index was derived from two indicators measuring social contacts within and outside of the household from the social networking questionnaire (CLSA, n.d.). First, the responses were grouped into three isolation levels according to the time frame of last face-to-face contact with family members (children/siblings/other relatives), friends, and neighbors who live outside of the household, ranging from not isolated (have contacts in the past week or two); mildly isolated (have contacts in the past month but not in the past week or two); to extremely isolated (no contact in the past month). Second, these three isolation categories were divided into six groups stratified by their living arrangements (live alone or not) in the household: (1) not living alone, nor isolated; (2) living alone, but not isolated; (3) not living alone, but mildly isolated; (4) living alone and mildly isolated; (5) not living alone, but extremely isolated; and (6) living alone and extremely isolated. Online social networking was based on the frequency of using social networking sites through the Internet to stay in touch or make plans with family or friends. It was classified into four groups: (1) active use (daily or weekly); (2) moderate use (monthly); (3) mild use (less than monthly); and (4) no answer.
The cluster of social support availability was measured by three binary items modified from the self-administered Medical Outcomes Study (MOS) Social Support Survey (Sherbourne & Stewart, 1991). In the MOS, questions were asked regarding having someone: (1) to advise on a crisis; (2) to confide in or talk to, and (3) who shows love and affection. These three indicators have been identified as key social support indicators for health outcomes in previous studies (Sarason et al., 1997). The response options were dichotomized into two levels: (1) none/a little/some of the time; and (2) most/all of the time.
Race was measured by a binary variable indicating whether the respondent reported he/she was white or visible minority/ Indigenous living in Canada (hereafter called visible minority).
Data analysis
All analyses were completed using SPSS Version 22 (IBM). The weights provided by CLSA were normalized to produce population-representative estimates corrected for the sample size. Bivariate analyses based on Chi-square tests using weighted means were conducted to describe the sample. Adjusted odds ratios (aOR) were calculated using binary logistic regression analyses to examine associations between refugee/immigration status and psychological distress while adjusting for the covariates. A series of binary logistic regression analyses were conducted. The first and all subsequent binary logistic regression analyses included refugee/immigrant status, age, sex and marital status (Model 1). In model 2, socioeconomic factors were included. In Model 3, health status and health behaviors were added to model 1. Subsequent clusters included social isolation and online social networking (Model 4), social support (Model 5), and racial minority status (Model 6), respectively. The final model was adjusted for all of the aforementioned variables (Model 7).
Ethics approval
The study protocol of the CLSA has been approved by 13 research ethics boards across Canada. This secondary analysis of CLSA data was approved by the University of Toronto’s Health Sciences Research Ethics Board (Protocol number: 34065).
Results
Description of sample
Table 2 presents the descriptive characteristics of the total sample by level of psychological distress and refugee status. The prevalence of mild to severe psychological distress was higher among younger respondents, women, visible minority members, those who were not married, those with low income and without a high school diploma. People with three or more health conditions, who reported that they were experiencing chronic pain, and who did fewer physical activities, had a higher prevalence of psychological distress. However, people who were less socially isolated and did more frequent online networking, and those with a higher frequency of social support, had a lower rate of psychological distress.
Description of overall sample (n = 28,158) according to distress status and immigrant/refugee status.
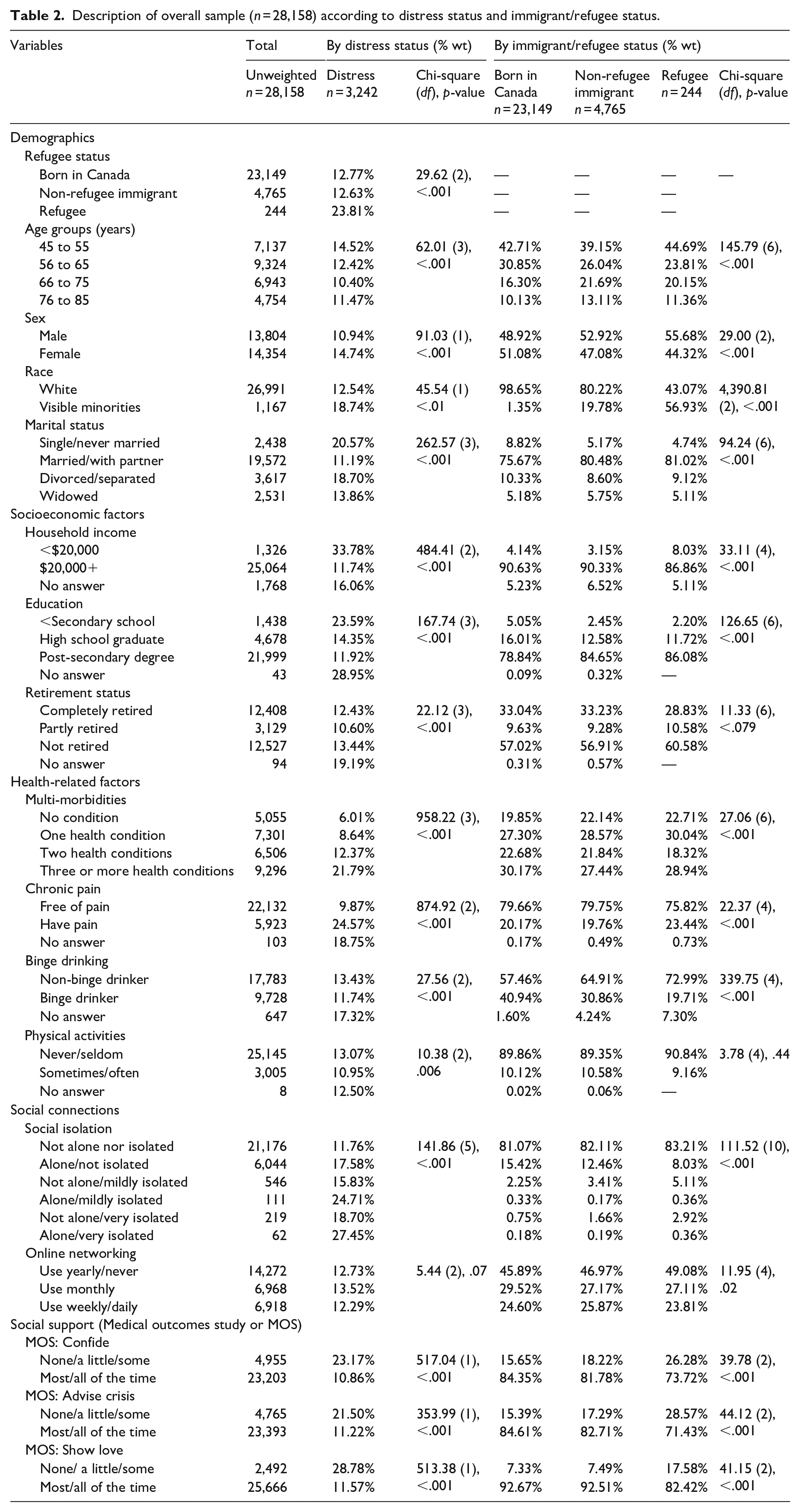
Additionally, the distribution of most of the main variables and covariates were similar between the total sample and the three refugee/immigrant subgroups (Canadian-born residents, non-refugee immigrants, and refugees) except for sex, race, and multi-morbidities. Both non-refugee immigrants and refugees had a higher percentage of women than men (non-refugee immigrant women = 53%, refugee women = 56%). There were also more visible minorities in the refugee group than Whites (visible minority refugees = 57%; Visible minority non-refugee immigrants = 19.8%; visible minority born in Canada = 1.4%). Moreover, non-refugee immigrants and refugees showed a slightly lower prevalence of having two or more health conditions (non-refugee immigrants = 49%, refugees = 47%) than Canadian-born residents (53%).
Multivariable analysis
Objective 1: Do both refugees and non-refugee immigrants in Canada have a higher prevalence of psychological distress compared to those born in Canada?
The results of the bivariate analysis showed that the prevalence of psychological distress was significantly higher among the 244 refugees (23.8%), compared to 23,149 Canadian-born Canadians (12.8%) and 4765 non-refugee immigrants (12.6%) (See Table 2). Results from the binary logistic regression models (see Table 3) further indicated that the odds of experiencing psychological distress were consistently higher for refugees compared to the Canadian-born (aORs from 2.31 (model 1 to 1.56 fully adjusted model). However, the odds of psychological distress among non-refugee immigrants hovered around 1.00, and in all but one analysis, were not statistically significant (non-refugee immigrants: aOR=0.97 to 1.11).
Adjusted odds ratios for psychological distress based on binary logistic regression.
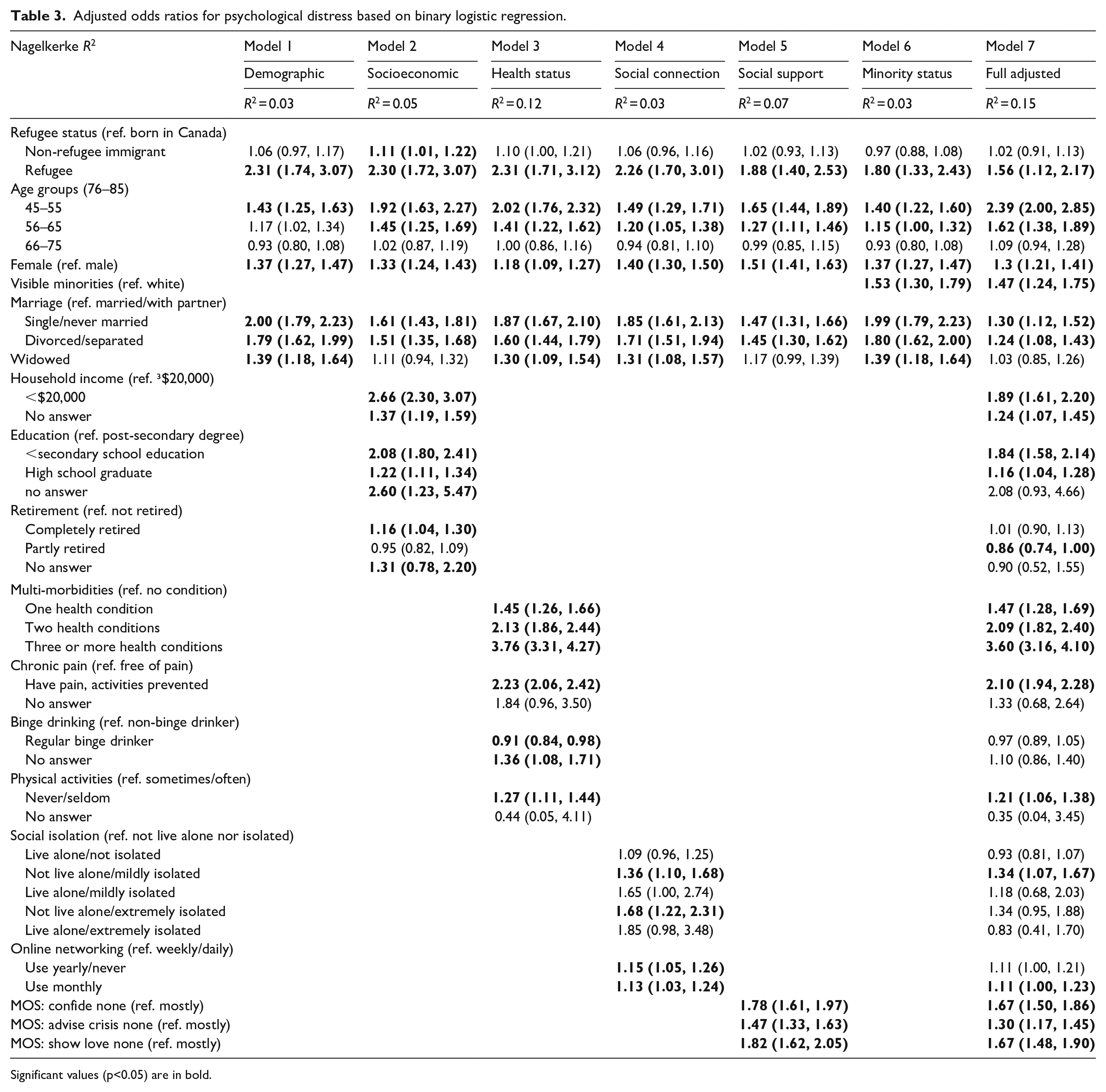
Significant values (p<0.05) are in bold.
Objective 2: Are there demographic, economic, health-related, and social factors which attenuate the association between refugee status and psychological distress?
As shown in Table 3, in the baseline model 1, the odds of experiencing psychological distress was more than twice as high for refugees as they were for those born in Canada (aOR = 2.31, 95% CI: 1.74–3.07) when only age, sex, and marital status were taken into account. After adjusting for a wide range of known risk factors for distress in the final model (Model 7), the odds of experiencing psychological distress were slightly decreased but still significant (aOR = 1.56, 95% CI: 1.12–2.17).
Objective 3: What factors are significantly associated with psychological distress after refugee and immigrant status were taken into account?
The results outlined in Table 3 show that the odds of experiencing psychological distress was higher for people who were 45–65 years of age when compared to those who were 66 years of age and older (45–55 years: aOR = 2.39, 95% CI: 2.00–2.85; 56–65 years: aOR = 1.62, 95% CI: 1.38–1.89). Females (aOR = 1.30, 95% CI: 1.21–1.41) and visible minorities (aOR = 1.47, 95% CI: 1.24–1.75) had higher odds of psychological distress than males and Whites. When compared to people who were married or with a partner, those who were single/never married (aOR = 1.30, 95% CI: 1.12–1.52) or divorced/separated (aOR = 1.24, 95% CI: 1.08–1.43) had higher odds of experiencing psychological distress. Lower household income (aOR = 1.89, 95% CI: 1.61–2.20) and lower educational attainment (secondary school or under: aOR = 1.84, 95% CI: 1.58–2.14) were also associated with higher odds of psychological distress when compared to people who had higher income and a post-secondary degree. People who were semi-retired were less likely to experience psychological distress (aOR = 0.86, 95% CI: 0.74–1.00).
In terms of health status, we observed a graded association between the number of health conditions and psychological distress. Specifically, the odds of psychological distress were more than three times higher for people with three or more health conditions compared to those with no health conditions (aOR = 3.60, 95% CI: 3.16–4.10). Similarly, those who reported having chronic pain were more likely to experience psychological distress (aOR = 2.10, 95% CI: 1.94–2.28) compared to those without chronic pain. Those who seldom or never participated in physical activities in the previous seven days were also at higher risk of experiencing psychological distress compared to those who did physical activities sometimes or often (aOR = 1.21, 95% CI: 1.06–1.38).
In comparison to those who lived with others and were not socially isolated, those who lived with others but were either mildly social isolated from others outside the household had higher odds of psychological distress (aOR = 1.34, 95% CI = 1.07–1.67). These results suggest that people without someone to confide in (aOR = 1.67, 95% CI: 1.50–1.86), to advise them if they have a crisis (aOR = 1.30, 95% CI:1.17–1.45), or to show love and affection to (aOR = 1.67, 95% CI: 1.48–1.90) have higher odds of psychological distress when compared to people who have these social supports most of or all of the time.
Discussion
Psychological distress is an under-recognized and undertreated mental health issue (Drapeau et al., 2012). This study found that refugee status is associated with almost twice the prevalence of psychological distress compared to those who are Canadian-born. This strong association remained statistically significant even when demographic, economic, health and social factors were taken into account. The observed high prevalence of psychological distress is in keeping with studies of refugees in many OECD countries. When compared to the general population, studies from different countries including USA, Canada, Australia, Ireland, Sweden, all reported that refugees and immigrants are more likely to experience higher levels of psychological distress despite that the fact that the levels vary by measures and contexts (Chen et al., 2017; Honkaniemi et al., 2020; Li & Anderson, 2016; Ryan et al., 2008; Torres & Wallace, 2013). For example, a Swedish study found that nearly one quarter of non-OECD migrants and one-fifth of OECD migrants reported having psychological distress. These levels are much higher than the one-eighth of Swedish-born participants who were in distress (Honkaniemi et al., 2020). The higher levels of psychological distress among refugees may possibly be due to traumatic experiences that motivated them to leave their country of origin in the first place. Non-refugee immigrants did not have elevated odds of psychological distress in this study. Resettling in a new country presents challenges including trying to adapt relatively quickly to a new social, cultural, and geographic environment, experiencing discrimination and poverty, having limited or no social networks and social support, and experiencing social isolation (Hynie, 2018; Stewart, 2014). These factors, however, should have been equally relevant for immigrants as well as refugees. Therefore, we hypothesize that the psychological distress experienced by refugees may be largely a function of the pre-migration trauma which may have resulted in their need to seek refugee status and leave their country of origin (Chen et al., 2017; Jurado et al., 2017; Li & Anderson, 2016). Refugees often experience pre-migration political or religious oppression, war, genocide, forced displacement, human trafficking, sexual assault, famine, loss of family members, and various forms of abuse (Chen et al., 2017; George & Jettner, 2016; Li & Anderson, 2016). The cumulative effect of premigration trauma and distress can persist long after resettlement (Makwarimba et al., 2013; Singh et al., 2015).
Refugees’ higher psychological distress levels may also be attributed to the lack of cultural sensitivity and tolerance in Canadian refugee policies (Rousseau et al., 2002). Many policies are highly Eurocentric and are not applicable to the diverse cultural, social, and political experiences of refugees (George, 2010). However, refugees are still viewed positively in Canada. Eighty percent of Canadians say refugees are “made to feel very or somewhat welcome by the local population” (Smith, 2019). Programs are in place to help refugees gain English language skills, retrain and locate jobs, access health care and to help their children integrate into the Canadian education system (Government of Canada, n.d.). Future research is therefore needed to address how elements of pre-migration trauma, refugee status, and post-migration challenges influence psychological distress.
The findings also indicate those who were visible minority members had significantly higher adjusted odds of psychological distress compared to those who were not people of color. This is possibly due to the fact that visible minority members may experience higher levels of discrimination and unfair treatment (De Maio & Kemp, 2010; Montazer, 2019), greater difficulty affording appropriate housing (Murdie, 2003), and challenges associated with accessing culturally appropriate mental health services (Reitmanova & Gustafson, 2009).
Consistent with the findings from other research, the results of this study reported that the odds of psychological distress were higher among women (Matud et al., 2015; Stallman et al., 2010), as well as those who were single, divorced or widowed (Darghouth et al., 2015), who had lower household income (Orpana et al., 2009) and lower levels of education (Miech et al., 2007), who had more comorbid health conditions, experienced chronic pain (Rice et al., 2016), and reported lower levels of physical activity (Perales et al., 2014). The results of this study indicated that middle-aged adults (45–65 years) had a higher level of psychological distress than older adults (75 years+), while previous research findings have not reported consistent associations between age and psychological distress (Cairney& Krause, 2005; Chittleborough et al., 2011; Goulia et al., 2012; Schieman et al., 2001). Additional research is needed to understand what mechanisms underlie the observed associations.
Previous studies have indicated that social support is protective against psychological distress (Bøen et al., 2012). The findings of the present study also indicate that those who reported having someone to confide in, provide advice to in a crisis, and having someone to show love to are less likely to experience psychological distress. However, the association between greater online social network use and lower psychological distress was only modest. Future research should continue to investigate these relationships because online social networking is growing in importance, even among older adults. Most research to date has focused on younger generations (Chen & Lee, 2013; Marino et al., 2018). Internet use may be a tool to reduce social isolation and increase social connectedness and interactions (Chen & Schulz, 2016; Cotten et al., 2011) and reduce the probability of depression among older adults (Chopik, 2016; Cotten et al., 2014). This may have particular relevance to social distancing measures that are instituted to control the spread of communicable diseases such as COVID-19.
Limitations of the study and implications
Findings of this research need to be considered in the context of the following limitations: First, the causal relationship between psychological distress and the various social determinants cannot be inferred as the data was cross-sectional. Second, refugee status was conceptualized based on year of arrival in Canada and country of origin. CLSA did not include questions on formal refugee status nor type of sponsorship. Therefore, a number of refugees in the analysis may have been missed. Third, although race and ethnicity may influence levels of psychological distress (Bratter & Eschbach, 2005; Park et al., 2018), the small sample of refugees in the current research prohibited a more nuanced analysis.
The findings of the study are based on the CLSA data which was collected in 2012 and all respondents had to speak English or French. Thus, these findings exclude refugees who could not speak either of Canada’s official languages and cannot be generalized to that group. Since the data were collected, there has been a surge of refugees resettled in Canada. Between 2015 and 2018, more than 58,000 Syrians arrived (Government of Canada, 2018). In 2018, Canada accepted 28,000 refugees, which was the largest number of any country in the world (Government of Canada, 2018). Syrian refugees are younger and have a higher percentage of families consisting of a couple with children when compared to refugees from other countries. Syrian refugees are less likely to speak English or French and had lower educational attainment, which suggests that they might at risk of socioeconomic vulnerability (Houle, 2019). More studies should be conducted examining the mental health of these newly arrived refugees.
Despite these limitations, the fact that almost one-quarter of refugees in this sample were in distress, even decades after settlement in Canada, suggests the need for creative public policy to address mental health problems as soon as possible after arrival. In light of the strong link observed in the current study between a lack of social support and distress, programs that improve social connectedness are worth considering. One particularly promising Canadian strategy for refugee resettlement, which may be worth adopting in other countries, is the privately sponsored refugees (PSRs) program. In this program, networks of volunteers from churches, mosques or other social groups provide refugee families with financial assistance for the first year after arrival, in addition to very extensive assistance locating health care, accommodation, furnishing and clothing, language training, suitable jobs, and help with registering children for school. The emotional support these groups provide can be very helpful and may mitigate subsequent distress. Syrian refugees who arrived under the PSR scheme are more likely to report they are employed and that they have help with daily errands. They are also less likely to report unmet needs in comparison to refugees who were resettled in Canada under the traditional government sponsored program (Hanley et al., 2018; Immigration, Refugees and Citizenship Canada, 2016; Kaida et al., 2020). To improve resilience and decrease mental illness among refugees, an additional strategy is to provide trauma-informed care to vulnerable refugees. Aspects of trauma-informed care for refugees include regularly screening for trauma and related distress, adoption of a strength-based focus, provision of health and mental health care by culturally and linguistically similar providers, and provision of multigenerational care (Miller et al., 2019). Trauma-focused cognitive behavioural treatment is a very promising intervention for refugees with mental health challenges (Miller et al., 2019).
The findings have substantial policy and practice implications for improved screening, outreach, and service provision to refugees and other vulnerable groups. By targeting modifiable variables such as education, income, social capital, and lifestyle factors that contribute to chronic diseases, the wellbeing of refugees and all mid-life and older Canadians can be better supported.
Footnotes
Acknowledgements
This research was made possible using the data collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation. This research has been conducted using the CLSA Baseline Comprehensive Dataset version 4.0, under Application ID 170605. The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland.
Author’s contributions
EFT, KMD, KK, HT, and LS developed the analysis plan. KMD and LS conducted the analysis with the direction of EFT. HT, LS, and YL wrote the first and subsequent manuscript drafts; all team members provided feedback. HT, YL, SA and EFT made the final revisions. EFT supervised all components of the project.
Disclaimer
The opinions expressed in this manuscript are the authors’ own and do not reflect the views of the CLSA administrators.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Part of this study was funded through EFT’s Sandra Rotman endowed chair funds and KMD’s Fulbright Canada scholarship.