
Abstract
Background:
According to the WHO, detainees attempt suicide ten times more than the general population.
Aims:
To investigate the impact of migration trauma on Suicidal and Self-Harm Behaviours (SSHB) of migrants in jail and to explore how substance use and other psychiatric features affect this relationship.
Methods:
Prospective cohort study, conducted at the ‘Sant’Anna’ jail in Modena (Italy) between February 2017 and September 2019. Socio-demographic, psychiatric features and records of previous SSHB were collected. Experience of migration-related trauma was assessed with the LiMEs (List of Migration Experiences) checklist. Participants were followed-up for the occurrence of further SSHB. Survival analysis was performed and Cox’s Hazard Ratios (HR) were used as a measure of association of comparisons.
Results:
Amongst the 112 subjects (96% male, median age 33), the prevalence of any mental disorder was 26% and of substance abuse 59%. History of SSHB was present in 36% of the sample. Median follow-up time was 80 days. During follow-up, 11 events were observed (of which three were suicide attempts). Cumulative survival probability was 85%. Having experienced trauma related to war and violence was significantly associated with SSHB, HR: 7.05. No SSHB were recorded amongst subjects without substance abuse.
Conclusions:
Migrants in custody who experienced trauma in the post-migration period, attempt SSHB seven times more frequently than those without traumas at any time. War trauma and post-migration trauma due to exposure to violence seem to be more strongly associated with SSHB, also controlling for psychiatric diagnosis, ongoing psychopharmacological therapy and substance abuse. Further research and possible intervention programs should focus on addressing post-migration living-difficulties.
Keywords
Introduction
Suicidal and self-harm behaviours (SSHB) are international issues in correctional settings and rate of suicides amongst prisoners is higher than in general populations. Many countries in northern and western Europe have prison suicide rates of more than 100 per 100,000 prisoners per year (Fazel et al., 2017). According to the most recent Italian data, prisoners are 16 times more likely to commit suicide than the general population (Antigone Association et al., 2020; Italian Ministry of Justice, 2020a, 2020b). Incarcerated individuals also display higher rates of self-harm behaviours (SHB), estimating that 7% to 48% of offenders have a lifetime incidence of SHB, versus 4% in the general population (Briere & Gil, 1998; Chapman et al., 2005; Lader et al., 2003). SHB are the most common reason for mental health interventions in jail, with relevant consequences in terms of human and economic resources (Dixon-Gordon et al., 2012). The relationship between SHB and suicides is widely discussed; though SHB are not necessarily motivated by the intention of dying, they nevertheless perpetuate a cycle of maladaptive coping and put an individual at risk for accidental death. Nearly 50% of people who commit suicide have a history of SHB; a history of SHB is a well-known predictor of suicides amongst the prison population (Hawton et al., 2014).
Prisoners are exposed to more risk factors for suicide than the general population, which include a higher prevalence of mental disorders, substance abuse, and socioeconomic deprivation (Bland et al., 1998; Fazel & Danesh, 2002; İlgün et al., 2020). These circumstances are faced by almost all prisoners, whereas only a part of them attempt suicide. With the aim to identify more specific risk factors for SSHB, many variables were analysed, including the aspects of crime and the sentence structure (e.g. the charge for a violent offence or the prospect of a life sentence; Borrill & Taylor, 2009; Fruehwald et al., 2004). Psychological and psychiatric individual characteristics were also included, such as avoiding coping styles, interpersonal conflict, impulsivity, history of child abuse, past and current mental disorders or substance abuse, ongoing psychotropic therapies (Dixon-Gordon et al., 2012; Fruehwald et al., 2004), and previous SSHB (Dixon-Gordon et al., 2012; Fazel et al., 2017; Fruehwald et al., 2004). Notably, depression and hopelessness have been found to adequately predict SSHB in a sample of offenders (Perry & Gilbody, 2009). Finally, there may be risk factors related to the prison environment, such as overcrowded habitats, absence of job placement programs, low levels of hygiene, bad socio-cultural frame, high HIV/AIDS prevalence, and scarce access to either general or mental health services.
Nonetheless, a comprehensive association between SSHB rate and prison-related-factors has not been fully demonstrated.
Focusing on the migrant population in prison, data are even more impressive: the rate of suicide amongst foreign detainees was exactly two times the rate in the Italian prison population in 2018, and the SSHB rates were no less alarming (Antigone Association et al., 2019). Specific risk factors deriving from a combination of migration- and detention-related variables may explain such finding. Migration is known to impact massively on mental health and suicidal behaviours (Bhugra, 2004; Bhugra & Becker, 2005). Moreover, language barriers, separation from family, lack of information on the health care system, loss of status, loss of social network, and acculturation were identified as possible triggers for suicidal behaviours (Forte et al., 2018).
A large number of studies estimated the prevalence of substance abuse in jail population, with varied results ranging between 10 to 48% for males and 30 to 60% for females; even higher prevalence rates were reported by more recent studies, widely exceeding those of the general population (Fazel et al., 2006, 2017; Kanato, 2008). Substance misuse is known to worsen the prognosis of comorbid psychiatric disorders, and to increase criminal relapse rates and premature mortality rates after prison release (Merrall et al., 2010). Furthermore, drug use has emerged as a predictive factor both for SSHB in prison and for post-release suicide (Kariminia et al., 2007; Verdolini et al., 2017).
The aim of the study was to evaluate SSHB associated with migration and detention. The primary goal was to investigate the impact of migration-associated trauma on SSHB in detained migrants.
Secondarily, to assess how drug abuse and the presence of other psychiatric features (i.e. psychiatric diagnosis, ongoing psychotropic medication, and history of previous SSHB) affect the risk of SSHB in the same population.
Materials and methods
Study design and measures
Prisoners that were included in the study met the following inclusion criteria: adult (⩾18 years old) Migrants Newly Imprisoned (MNI), not born in Italy, with a final sentence, admitted to the Prison ‘Sant’Anna’, in Modena, North of Italy, between 01/02/2017 and 30/09/2019, sufficiently fluent in the Italian language and providing valid informed consent to the study.
The Prison ‘Sant’Anna’ has an official capacity of 369 prisoners yet, on December 31st, 2019, hosted 528 people (63.4% of those were migrants). On March 8th, 2020, prisoners set fire to the jail, protesting against the overcrowding. The jail is still undergoing to refurbishment, and the total capacity is currently reduced (Italian Ministry of Justice, 2020a, 2020b).
Subjects eligible were enrolled during the psychological assessment at admittance. This is usually held within 48 hours from admission by the clinical psychologist of the prison clinic. During this psychological assessment, a thorough psychopathological examination is conducted, and psychiatric diagnoses are made, if relevant, according to the ICD-10 code system (WHO, 2004).
After signing the informed consent, socio-demographic features (i.e. age, gender, marital status, years of schooling, employment) and information on duration and length of the migratory journey, current legal status (i.e. legal refugee, seeker or illegal immigrant, previous detention[s] or offend[s]), psychiatric history (i.e. current or past psychiatric disorder and substance[s] abuse, previous SSHB both in community and in jail) were collected.
Further psychometric evaluation was performed for each subject, by the administration of the following validated tests:
- List of Migration Experiences (LiMEs), version in different languages, short version, by Aragona (Aragona, 2014): self-administered, 22-item questionnaire, assessing migration-related trauma. Traumatic experiences are conceptually grouped according to time of occurrence (pre-/during-/post-migration) and to kind of trauma: (a) generic trauma (items 1, 6, 11, 12): serious injuries, being close to death, accidents, natural hazards; (b) intentional trauma (items 2, 3, 4, 5, 7, 8, 9): physical abuse, rape or sexual abuse, torture, brain-washing, imprisonment/detention, lost or kidnapped, forced isolation from others; (c) war-related trauma (items 10, 17, 18, 19, 20): combat situation, murder of strangers, forced to harm others, witnessed violence to others, destruction of personal properties; (d) family-related trauma (items 13, 14, 15, 16, 48, 49): murder of family or friend, unnatural death of family or friend, forced separation from family members, loss or separation from family members, worries about family back home, unable to return home in an emergency.
- Jail Screening Assessment Tool (JSAT), by Nicholls et al. (2005): semi-structured interview, conceived to support the initial assessment of a subject entering in the penitentiary setting, including the following: socio-demographic information, legal situation, violent behaviour, social background, use of substances, psychiatric diagnosis/treatments, current suicidal/self-harm risk, mental status as assessed by the Brief Psychiatric Rating Scale (BPRS). This full assessment took around 60 minutes, on average: 20 minutes for JSAT, and 40 minutes for BPRS, gleaning useful information also from the clinical records, when available.
- Barratt Impulsiveness Scale (BIS-11), by Patton et al. (1995): 30-item, self-administered, questionnaire used for assessing personological and behavioural features related to impulsivity. The score ranges from 30 (low level of impulsivity) to 120 (high), with a cut-off of 74 or more as clinically significant (suggesting an ‘impulse control disorder’).
All psychometric tools were administered by the same researcher (C.A.).
Recruited subjects were followed-up until a particular SSHB was committed (see description of survival analysis in the next paragraph) or up to the end of the study. Episodes of SSHB were identified by researchers after clinical discussions during the weekly staff meetings and by a systematic search of medical reports of the enrolled subjects. For each SSHB occurred, time-to-event (exact time, expressed in days of follow up) and information on lethality and outcome of the gesture were collected. Subjects that quit the study for reasons not linked to SSHB (e.g. if they were transferred to another prison or released) were handled as censored time.
Statistical analysis
Survival analysis was performed using SSHB as the outcome (Sedgwick & Joekes, 2015). All survival times, exact and censored, were used to plot the overall survival function, according to the Kaplan–Meier estimator, and the log-rank test was used for making comparisons between groups identified based on trauma experiences, substances abuse, and psychiatric morbidity, used as independent variables. Univariate and multivariate Cox’s regression analysis were performed, under the assumption of Proportional Hazards (PH) tested by examining Schoenfeld’s residuals (p = .3082), to determine survival trends adjusted for the aforementioned explicatory variables (Zhang et al., 2018).
The level of statistical significance considered for the rejection of the null hypothesis was alpha = 0.05 (therefore p < .05).
Statistical analyses were performed with Stata 15 (StataCorp LLC, College Station, Texas, USA).
Statement of ethics
The study was approved by the local Ethics Committee (Prot. AOU 0005155/19). Every patient enrolled in the study signed a detailed written informed consent. The study was carried out according to the Declaration of Helsinki, to the Good Clinical Practice principles for medical research and the current regulations relating to the protection and processing of personal and sensitive data.
Results
Descriptive analysis of the sample
The sample was made up of 112 MNI, almost all (95.6%) were males, the median age was 33 years; subjects were married or engaged and with at least one child in the majority of cases (58.5 and 54.4%, respectively). More than half of the sample (N = 60, 53.6%) had 8 years of schooling (completed secondary school). Only 31 subjects, namely 27.7% of the sample, reported to have been employed before detention, and about a third of the sample (N = 33, 33%) were illegal immigrants.
Most subjects of the sample hailed from Africa (61.9%), in particular from Morocco and Tunisia (28.6%, N = 32 and 16.1%, N = 18, respectively), followed by Eastern-Europe countries, such as Albania 13.4% (N = 15) and Romania 8.9% (N = 10). The average length of stay in Italy was 14 years (SD = 8.1), ranging from a minimum of 1 year and a maximum of 49 years. The tenth percentile for the length of permanence in Italy was 4 years. The majority of the sample (65.5%) was fluent in Italian.
Smoking habits were present in 70.5% of the sample, history of substance abuse was positive in 58.9%, with 39.3% of the total sample declaring to have used/abused more than one substance.
The beginning of drug consumption has more frequently occurred after the arrival in Italy. Despite a high percentage of subjects with a history of drug abuse, only 30.3% of them reported having received treatments for the addiction in the period before the current detention.
Prevalence of any psychiatric disorder was 26.6% (N = 30), with personality disorders (N = 16, 53.3% of all psychiatric diagnoses) and depressive disorders (N = 10, 33.3%) as the most common diagnoses. History of SSHB was present in 24.8% (N = 28), and at least one suicide attempt was carried out by 11.5% (N = 13) of the sample. Of these, 76.9% (N = 10) engaged in SHB during a previous detention.
One out of three subjects (N = 38, 33.9%) were taking psychopharmacological therapy, in all cases, this consisted of benzodiazepines, commonly as a monotherapy (N = 14, 47%).
Trauma assessment was performed with the LiMEs checklist. Most experiences of trauma were accounted for occurring in the post-migration period, except for war-related traumas that were mainly reported as occurred before the migration. Family-related traumas were the most reported across the sample (65.5%). These may include murder or unnatural death of family member or friend, forced separation or loss of a family member, worries about family members in the country of origin, impossibility to go back home in case of emergency.
Survival analysis
The median time of follow-up was 80 days (mean 87.7 days, SD = 47.7), ranging from 30 to 214 days.
During follow-up, nine subjects engaged in at least one SSHB, with one of these that acted three SSHB in total, thus the total number of SSHB was 11. Specifically, these were three suicide attempts (by hanging) and eight episodes of self-injury (superficial cuts, ingestion of batteries, stitching the lips by wire, and self-provoked burns). None of these resulted in complete suicide.
Furthermore, 19 subjects (17%) quit the study because they were released from prison. Then, nine exact times and 103 censored times were obtained at the end of the study and used to plot the overall survival function (Figure 1).
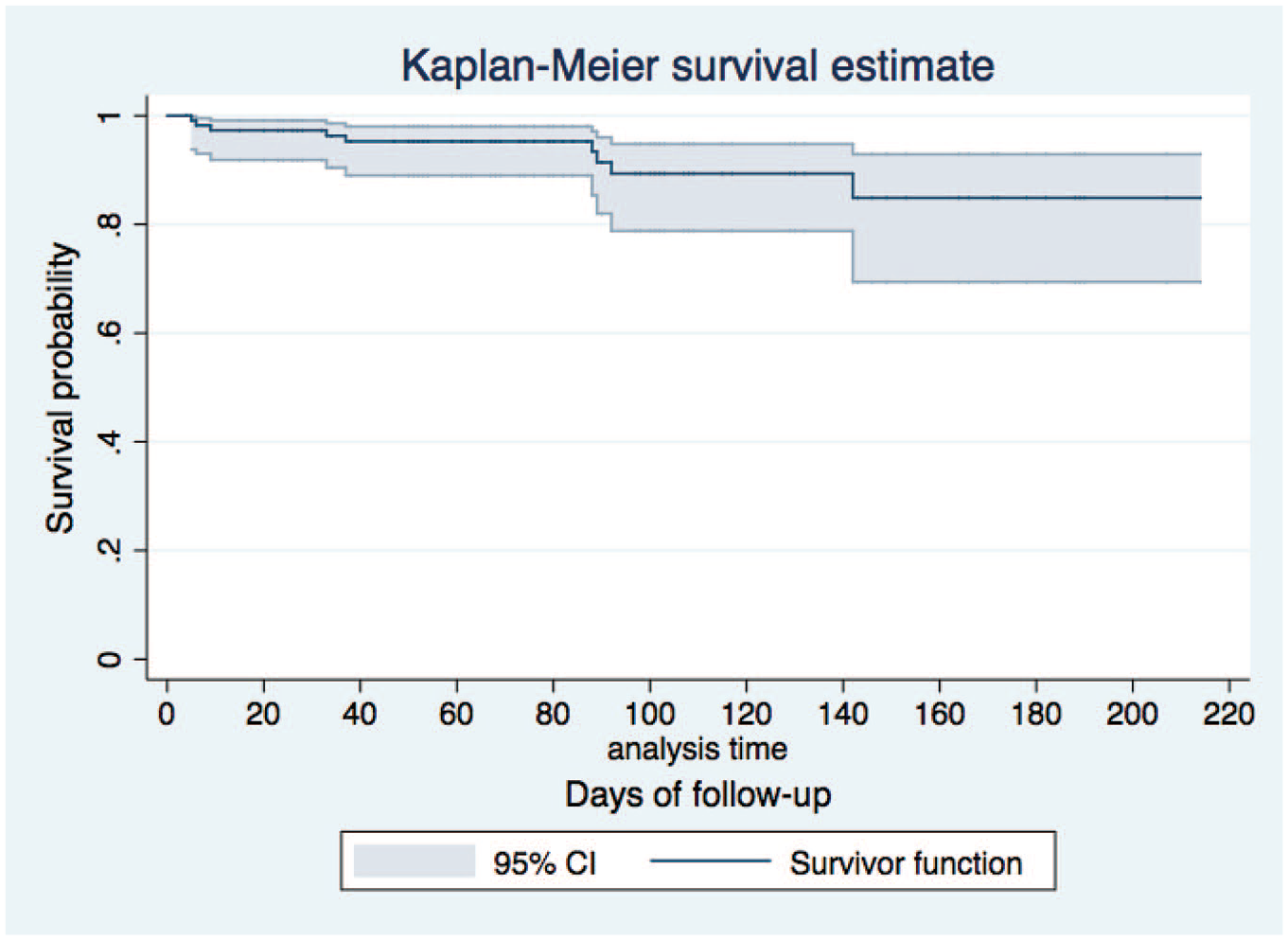
Kaplan–Meier plot of the overall survival function.
As Figure 1 shows, the probability of cumulative survival at the end of the follow-up was 85%.
Table 1 shows percentiles of the survival functions for all subjects and according to the presence/absence of potential explanatory variables (experience of war trauma after migration, substance abuse/multiple abuses, previous SSHB). The percentiles of survival were statistically lower at the log-rank test for subjects with post-migration experience of war-related trauma (p = .0027), substance abuse (p = .0165), psychiatric morbidity (p = .0021) and previous SSHB (p = .0239). The Kaplan–Meier plots for these groups are shown in Figures 2, 3, 4, and 5, respectively.
Percentiles of survival.

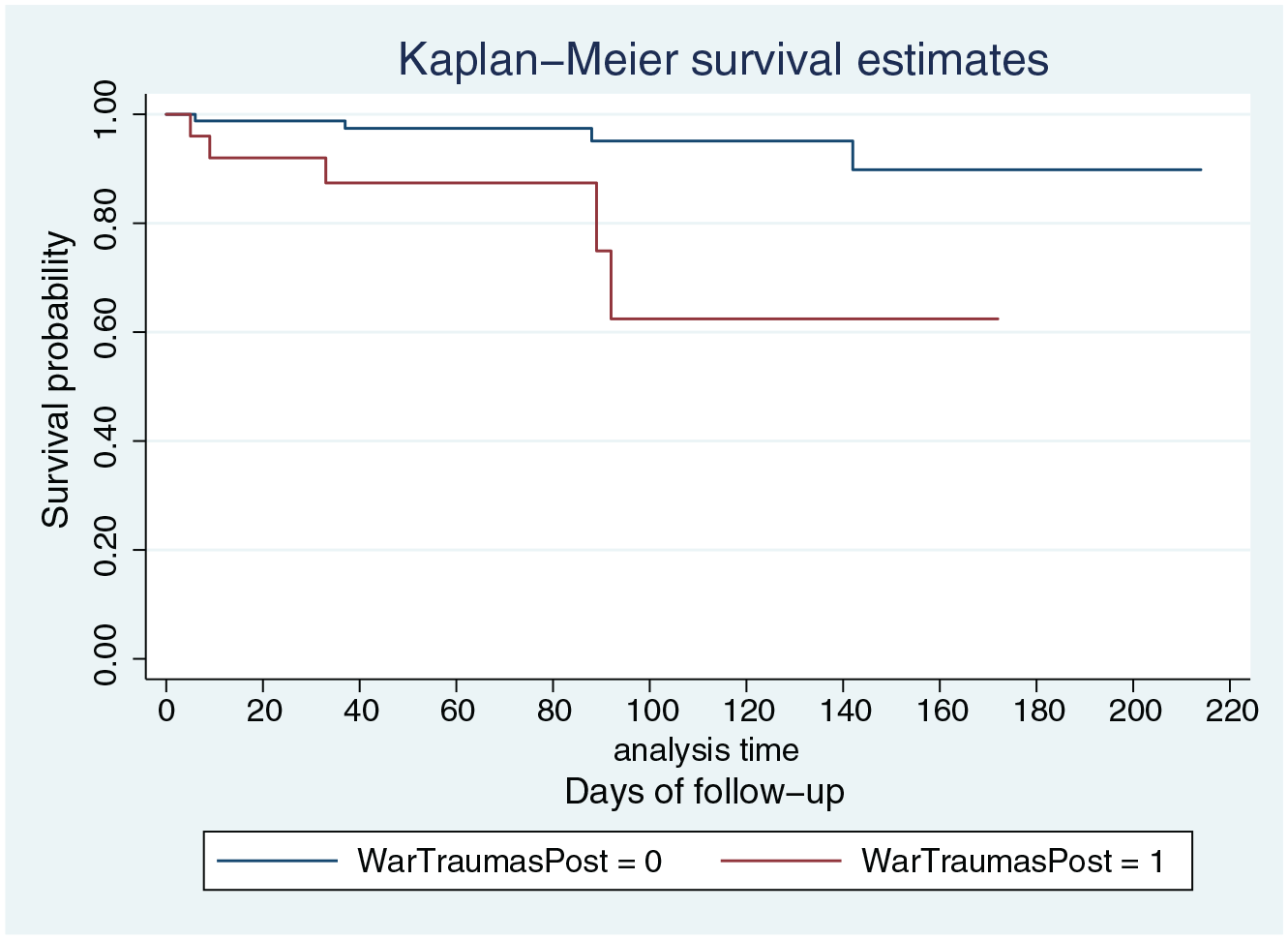
Kaplan–Meier plot of comparison between groups with and without experience of post-migration war-related traumas.
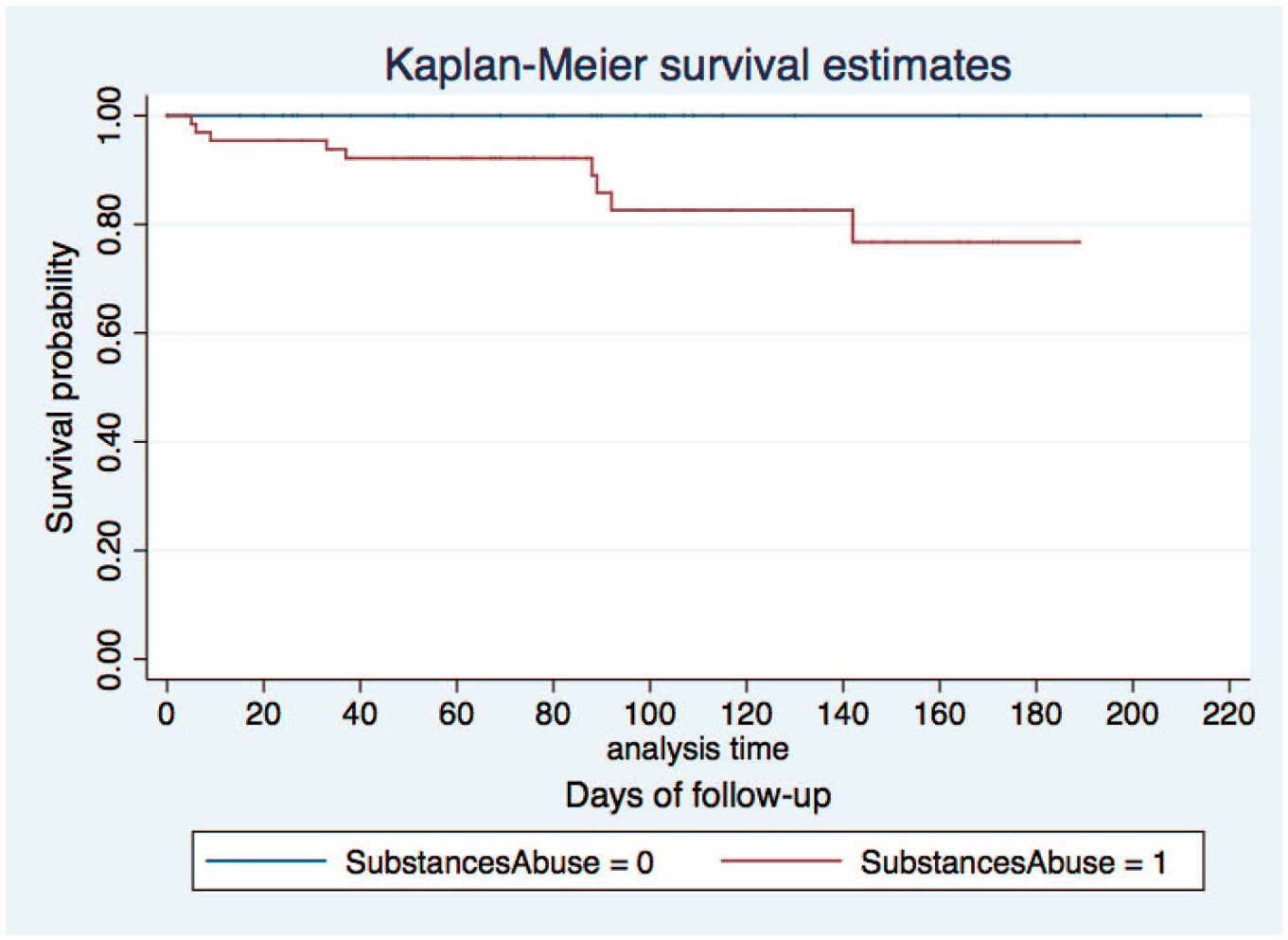
Kaplan–Meier plot of comparison between groups with and without substance abuse.
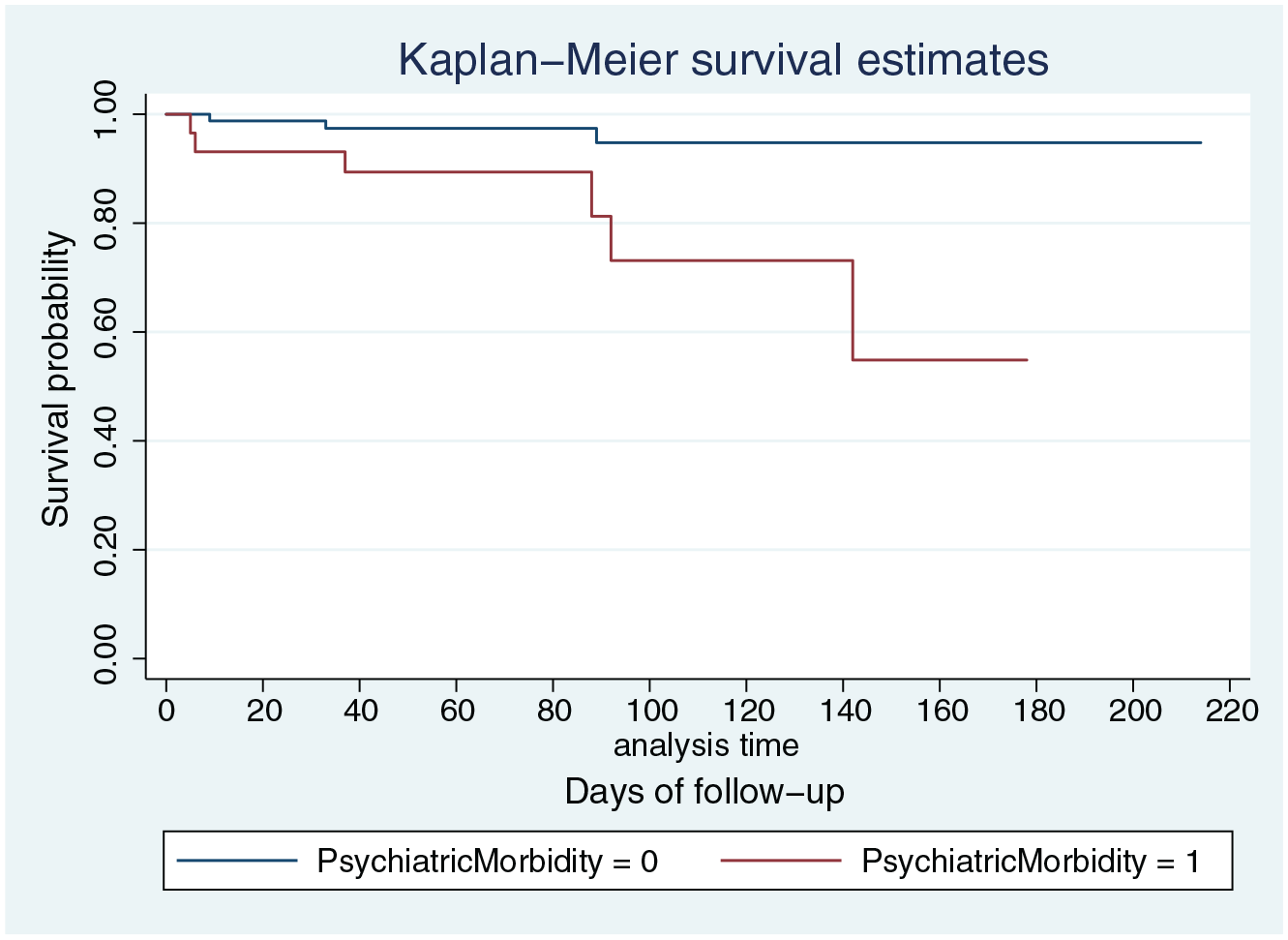
Kaplan–Meier plot of comparison between groups with and without psychiatric morbidity.
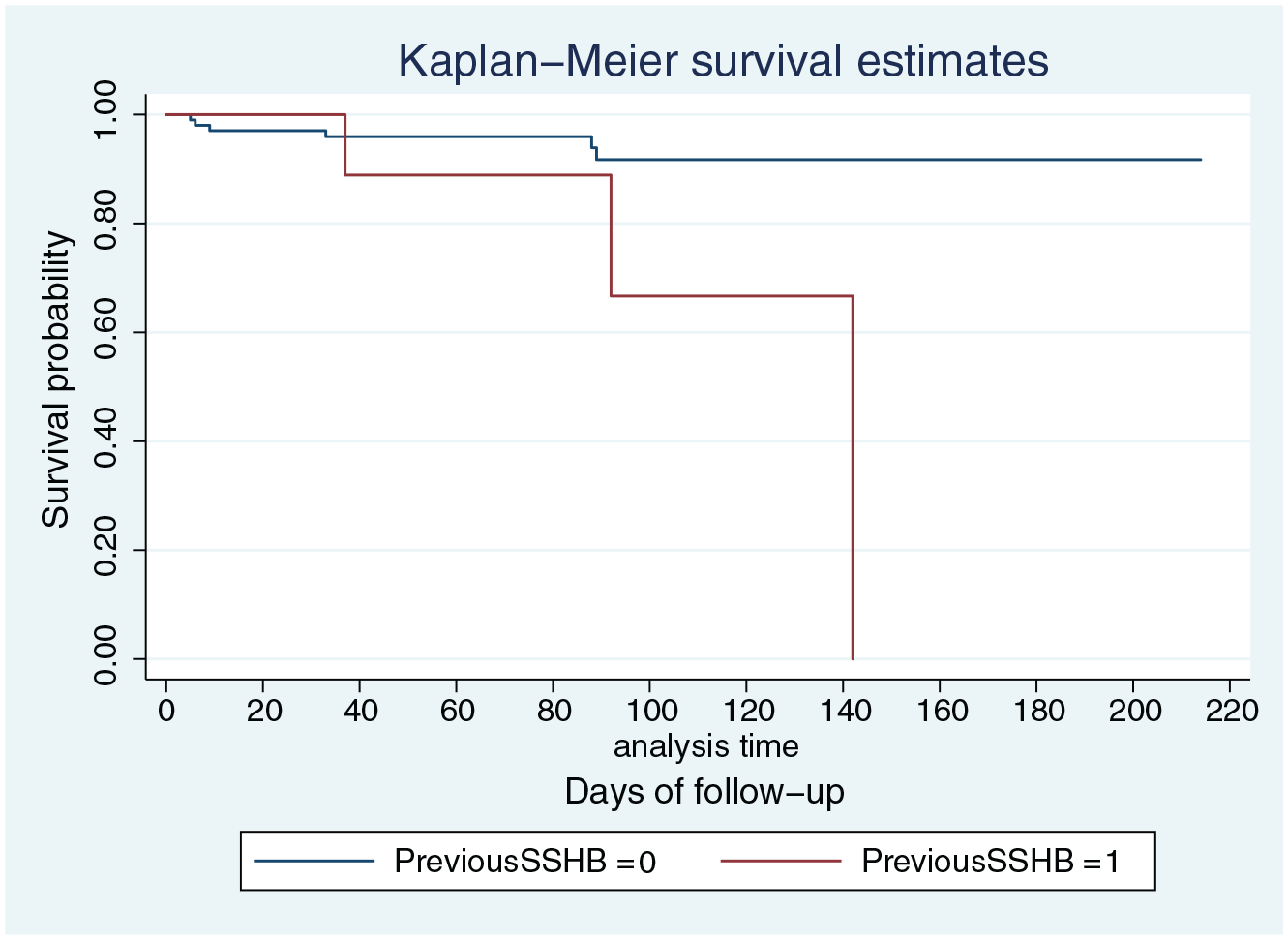
Kaplan–Meier plot of comparison between groups with and without previous SSHB.
Noticeably, none of the subjects with a negative history of substance abuse committed SSHB during the follow-ups, whereas all subjects that already had SSHB in the past repeated the gesture during the current jail stay, within the 142nd day of follow-up.
Univariate HR are shown in Table 2. For those subjects without substance abuse, who did not commit SSHB during the follow-up, the denominator in calculating HR is zero, with HR, therefore, tending to infinite.
Cox’s univariate analysis.

HR = hazard ratio; Std. Error = standard error; z = z-score; 95% CI = 95% confidence interval.
Multivariate HRs were then calculated to determine survival trends adjusted for the aforementioned explicatory variables and for the ongoing psychotropic medication.
Results of this analysis are shown in Table 3. Notably, the post-migration experience of war-related trauma and psychiatric morbidity remained significantly associated with the engagement in SSHB during the follow-up (HR = 7.05, 95% CI [1.47–33.82], p = .015; HR = 5.91, 95% CI [1.07–32.58], p = .042, respectively).
Cox’s multivariate analysis.

HR = hazard ratio; Std. Error = standard error; z = z-score; 95% CI = 95% confidence interval.
Discussion
The aim of this prospective, observational, cohort study was to establish the impact of exposure to migration trauma on the risk of SSHB occurring during jail detention in a sample of MNI. Also, the contribution of substance abuse and different aspects of psychiatric morbidity (psychiatric diagnosis, psychotropic medication, previous history of SSHB) on the risk of SSHB was assessed.
The sample shared the same socio-demographic features previously described in similar populations of foreign prisoners in Italy, except for data concerning marital status: more subjects reported being in a stable relationship, though many also reported to have few or no regular contacts with their families (Italian Ministry of Justice, 2020a, 2020b). Similarly, few subjects reported receiving support of friends/acquaintances or from religious communities. The condition of isolation during imprisonment has been confirmed to increase the risk of suicide by itself (Roma et al., 2013). Many other data contributed to a general description of the sample in terms of vulnerability and social precariousness: about a third of the cohort were illegal immigrants and two-thirds reported to have never been employed before detention. Social instability and marginality are well-known risk factors for involvement in criminal networks (Archuleta et al., 2020). It could be assumed that since illegal migrants cannot have access to most of the welfare programs, and particularly to ones related to work and health-care, nor to alternative measures to the detention in case they offend, a vicious cycle of further social detriment self-perpetrates.
Furthermore, such struggles may lead to the onset and increased prevalence of maladaptive coping strategies such as SSHB (Forte et al., 2018). The median time of follow-up was 80 days; since SSHB are severe events, with low incidence, these did not occur in at least half of the sample, therefore it was not possible to estimate a median survival time (Sedgwick & Joekes, 2015). Instead, the cumulative survival probability at the end of the follow-up was calculated: the overall SSHB rate at the end of the present study was 15%. This estimate is significantly higher if compared to that calculated in a recent Italian study on a sample with 40% of foreigner individuals, that was about 5% after 1 year of follow-up (Bani et al., 2019). However, previous evidence reported higher self-harm rates amongst foreigner detainees than Italian ones, consistent with our results (Antigone Association et al., 2019).
The MNI who took part in the study reported different migration trajectories and, on average, they have been living in Italy for quite a long time, a mean of 14 years. Consistently, the sample generally reported few or no experience of trauma occurred in the intra-migration phase: this may be the consequence of having faced the process of migration in periods when the Italian immigration policies were milder, and the logistic organisation of migration was easier.
The highest number of traumatic events reported referred to the category encompassing either concerns or trauma suffered by family members (called ‘family-related traumas’ in the LiMEs) and occurred in the post-migration period (65.5%). It is unclear, and it lies outside the aim of this study to state, whether the on-going detention status of respondents may have played a role in overestimating this result (migrant detainees cannot easily communicate with their family members in the countries of origin).
Respondents reported to have been exposed to traumatic events more in the post-migration period for all but war-related traumas that were more frequent before the start of the migration than afterwards (30% vs 23.6%). However, according to the results of this study, the post-migration exposure to trauma that were related to wars and conflicts has highlighted a six-fold increase to the risk of SSHB, at any time during the follow-up (HR = 6.23; 95% CI [1.61–33.82]; p = .008). This finding that may be difficult to understand considering that Italy is not at present interested by wars, is due to the comprehensive definition of war-related trauma used by the authors of the LiMEs checklist, which includes also experiences of violence in general. Even though the wide definition of war-related trauma used in the LiMEs may lack in specificity, it could be noted that this dimension embrace trauma characterised by a close proximity to death and destruction. Other studies have suggested an association between violence of the offence-psychological suffering-suicide attempts in the jail population (Hawton et al., 2014; Rabe, 2012). Our results are consistent with these findings. Also, given the higher prevalence of war-related trauma in the pre-migration phase, it may be hypothesised that post migration war-related trauma may have acted as a trigger, exacerbating feeling of cultural bereavement and failure of the migration plan, that may be source of psychological distress (Bhugra & Becker, 2005; Eisenbruch, 1990).
The high incidence of trauma in the post-migration period and their impact on psychological wellbeing is included in the so-called concept of ‘post-migration-living-difficulties’ (PMLD). In the period following the journey, migrants struggle due to issues related to many different stressing experiences such as precarious working and economic conditions, obstacles in accessing to health-care services and many others (Abraham et al., 2018). PMLD are closely related to mental health outcomes, including drug abuse (Aragona et al., 2012). Indeed, in our sample, the consumption of any drugs was more likely to have been started during the post-migration phase. This finding may be either due to the PMLD or to the very young age at the beginning of the migration journey (mean = 19 ± 8.2 years): it seems unlikely that subjects may have already begun the drug abuse when they still were in their country of origin. Developing a substance abuse, then, usually is closely related to involvement in drug-dealing, leading to legal problems and imprisonment.
Substance abuse, either current or past, is a well-known relevant risk factor for suicidal behaviours in the context of prison (Gates et al., 2017). This was confirmed by the data here discussed: first of all, no SSHB were counted amongst the migrants with a negative history for drug abuse, who were anyway not so less (41%) than substance abusers in the total sample; moreover, multiple-substance abusers were located in lower survival percentiles than mono-abusers.
A positive history for previous SSHB is acknowledged as the single most significant risk factor for SSHB in general as well as in specific populations (Wasserman et al., 2012). This was confirmed in the present study: having acted any kind of SSHB in the past was found to increase five-fold the risk for SSHB at any time during the follow-up, and all of those who have acted SSHB in the past repeated them during the current detention, within 142 days from its start.
Psychiatric comorbidity was found to be very common in the sample (26.6%) and consisted most frequently of personality disorders and depression. Our finding is in line with that of Voller et al. (2011) on an Italian jail population of both Italians and foreigners (29.3%), and higher than the prevalence calculated in the general Italian population (11.6%), thus confirming detention in jail as a risk factor for mental health problems, though the causal connections between the two is complex and possibly bidirectional. A little even higher (one-third of the sample) is the prevalence of imprisoned migrants receiving psychotropic medication, in most cases benzodiazepines, often as single prescriptions. This finding, though similar to previous findings in the same sub-population, is also consistent with the wide-spread use of sedatives in the general population, and with the high prevalence of substance abuse in this sample (Joukamaa et al., 1995). In our sample, suffering from any psychiatric disorders increased by six times the risk of SSHB at any time during the follow-up. Psychiatric morbidity is a well-established risk factor for SSHB, but the power of this association seems to be even more marked in the jail population here described (Wasserman et al., 2012). Moreover, the association remained significant after adjusting for ongoing psychopharmacotherapy (univariate HR of psychiatric morbidity = 6.60, p = .008; multivariate HR of psychiatric morbidity adjusted for ongoing psychotropic medication = 5.91, p = .042), suggesting that the latter can mitigate the effect, but only partially, as elsewhere also reported (Ritter et al., 2016).
Finally, looking at the Kaplan–Meier plots, it may be empirically noted a step down, at around 80 days. This may suggest that after the initial period, where newly-imprisoned people undergo strict monitoring, according to Italian regional guidelines (Mental Health Service et al., 2012), some prisoners still remain at risk for SSHB, and the findings of the present study could help prison clinicians and directors to stratify inmates according to their risk profile, identifying those who need more intensive support.
Limitations
One significant limitation was that the study was conducted in a single prison institution, and only subjects with a final sentence of imprisonment were enrolled, since the legal procedure to ask for permission to include also less permanently detained subjects would have required to contact a great number of interlocutors (competent judging courts) across the national territory, which for the sake of feasibility we decided not to do. This excluded from the sample many subjects with high-risk factors for mental health and suicidality, such as those waiting for a sentence or directly arriving in jail from a condition of freedom: the self-harm risk, which may be particularly high in the initial stage of detention, may have been underestimated.
Furthermore, for some subjects, sensitive information was not available (e.g. current visa status, or reason for the current detention) and some items in the psychometric questionnaires were not filled. Notwithstanding, the sample size was satisfying, and our results are in line with previous evidence in the literature.
A further limitation may be related to the choice to use the LiMEs checklist: though the scale is well-suited for studying migratory trauma amongst refugees, our sample had a rather long time of residence in Italy (14 years). Thus, it could be argued that other evaluation tools more focused on the PMLD than on migration-related trauma may be more useful in this population.
Conclusion
Migrants in custody who experienced trauma in the post-migration phase were found to attempt suicide up to seven times more frequently than those not reporting trauma. War-related trauma, in particular, seem to be strongly associated with suicide attempts, also after controlling for psychiatric diagnosis, ongoing psychopharmacological therapy and substance abuse. The risk for SSHB was also increased by any form of psychiatric comorbidity, substance abuse and having attempted SSHB previously.
SSHB are a major health issue in the prison context: though a certain amount of unpredictability is unavoidable when dealing with suicidal behaviours, specific primary and secondary screening pathways have to be implemented amongst the migrant population in jail (Pistone et al., 2019). These interventions should consider the role of PMLD.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.