
Abstract
Background:
South Africa is a low and middle income country facing many challenges in public mental health care and implementation of recovery.
Aims:
To contribute to what barriers and facilitators to recovery might be for service users in South Africa, from the perspective of service users, carers and service providers from three psychiatric hospitals in the Western Cape province.
Method:
Interviews and focus groups were conducted with service users, carers and service providers. Interviews and focus groups were transcribed and analysed using atlas.ti software and reflexive thematic analysis, from the bottom up.
Results:
The barriers, environment, family, public mental health services, stigma and service users’ attitude or behaviour generated, were found to be the most salient. The facilitators to recovery generated were support, family or friends, service providers, structure and empowerment. The need for support was identified as an underlying component to all these themes.
Conclusion:
Barriers and facilitators to recovery seemed to have both intrapersonal and external sources that intersect at times. Recovery needs to be supported at an individual level, especially through an under-utilised resource such as peer support work, but in conjunction with the development of recovery-enabling environments in services and communities in South Africa.
South Africa is a low and middle income country, faced by challenges, such as poverty, limited resources, inequality, obstacles in access to mental healthcare, a lack of governmental priority given to mental health care (De Wet et al., 2019; De Wet & Pretorius, 2020; Kleintjes et al., 2013; Lund, 2018; Lund et al., 2012) and a struggle for social cohesion. In particular, South Africa’s public mental health services are not sufficiently provided for in health care budgets and are still delivered mostly on an institutional basis, through tertiary psychiatric hospitals (De Wet et al., 2019; De Wet & Pretorius, 2020; Docrat et al., 2019). Within public mental health services, only very few programmes, that are specifically based on recovery principles, exist yet (De Wet et al., 2019; The Spring Foundation, 2017). This, despite recovery having been mandated in the National Mental Health Policy Framework and Strategic Plan 2013-2020 (South African Department of Health, 2013). Added to the limited financial resources and health care staff in public mental health services, it creates an environment in which many service providers (SPs) want to, but are often unable to provide service users (SUs) with the care required to support them fully in their recovery (Jacob, 2015; Kleintjes et al., 2013; Lund et al., 2012; Parker, 2012; Stein, 2014; Sunkel, 2014). Having to navigate the above context in their recovery, SUs are challenged by many barriers.
The focus of the larger study, from which the data reported on here originate, was the development of a measure of individual recovery for public mental health SUs in South Africa. It is one of the first such studies in South Africa. Data on the understanding of recovery (De Wet & Pretorius, 2020) and the development of the recovery measure are reported elsewhere. Through the initial study results we formulated the recovery definition for the South African context: An on-going, gradual, iterative and long-term process for service users (in collaboration with service providers and carers), after being in an acute mental illness state, which may include one or more themes such as relating to self, others, or the world, moving positively forward, (re-)gaining strengths, awareness of difficulties and a clinical understanding to support personal recovery (De Wet & Pretorius, 2020, p. 8).
We mapped the first five themes of this definition onto the recovery processes, called the CHIME framework, of Leamy et al. (2011), but we found the last two themes, awareness of difficulties and a clinical understanding to support personal recovery, to be distinct from the CHIME framework (Leamy et al., 2011). Furthermore, the theme, awareness of difficulties, comprised barriers, on which participants elaborated. Participants also described facilitators to recovery. Here we discuss some barriers and facilitators to recovery for SUs, from our study, given the general and mental health care context in South Africa.
Method
Participants
Data were collected in 2018 and 2019 by the first author through interviews and focus groups with (1) SUs, who could speak English or Afrikaans (a local language), with a severe or chronic psychosocial disability and had cumulatively, over their mental health treatment history, spent six or more months at a tertiary public psychiatric hospital in the Western Cape province of South Africa and participated in some mental health programme at the hospital, (2) their SPs and (3) their carers (relatives). Thirteen interviews were with SUs, 12 with carers (all relatives of SUs who met inclusion criteria) and 12 with SPs. We held three validating focus groups, one with each cohort of participants, that is, one with four SUs, one with three SPs and one with three carers. In Table 1 we provide participant descriptions and inclusion criteria.
Participant descriptions and inclusion criteria.
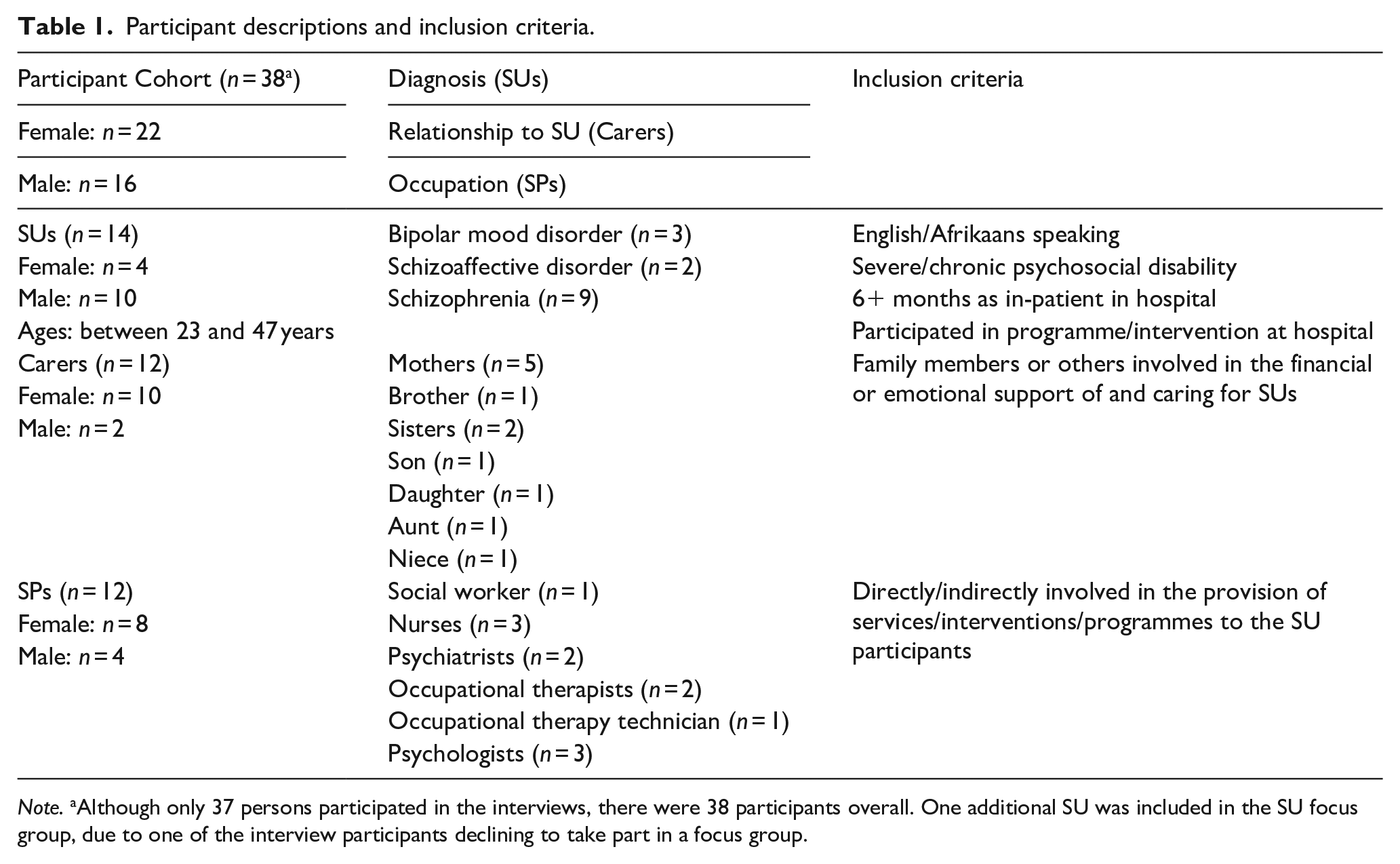
Note. aAlthough only 37 persons participated in the interviews, there were 38 participants overall. One additional SU was included in the SU focus group, due to one of the interview participants declining to take part in a focus group.
Procedures
We obtained ethical approval from Stellenbosch University’s Research Ethics Committee: Human Research (Humanities) (Reference number PSY-2017-1711) and the Western Cape Provincial Department of Health (Reference number WC_201801_032). Recruitment took place through the Department of Health, who appointed contact persons at the three hospitals. We were not allowed to approach SUs directly. SPs, to whom the duty to assist us had been delegated, identified and introduced us to SUs who met inclusion criteria. For SPs, we invited them at the hospitals to participate. Carers were identified either by SUs or SPs. The study was explained to all participants, who could ask questions, decline to participate and had to sign an informed consent form of which a copy was offered to them. Participants were assured of confidentiality of their identity. Interviews and focus groups were audio-recorded with participants’ consent. Interviews were conducted, depending on the participant’s preference, in English or Afrikaans; the latter being the most widely spoken home language in the Western Cape (Statistics South Africa, 2011).
The interviews and focus groups were in-depth and semi-structured, using an interview schedule and focus group interview guide, and explored participants’ understanding of recovery and what hinders and what helps recovery. The interviews lasted between 33 and 87 minutes and focus groups between 52 and 93 minutes. Data saturation was reached.
Data analysis
Interviews were transcribed and quality checked. We used atlas.ti data analysis software (Atlas.ti, Version 8.4.4) and reflexive thematic analysis (Braun & Clarke, 2006, 2019) to analyse the data, bottom up. The first author created quotations, annotated quotations, coded quotations and then generated themes of barriers and facilitators. The authors discussed the quotations, codes and themes throughout analysis to ensure trustworthiness and refine results. The themes were checked against the transcriptions to ensure that the themes related well to the original data.
Results and discussion
The theme, awareness of difficulties, from our South African recovery definition (De Wet & Pretorius, 2020), comprised certain barriers. Participants discussed these barriers, including setbacks, loss and the intermittent and iterative nature of the recovery process, which could all prove to be challenging. These barriers were to be expected in a demanding socio-economic context such as in South Africa where the majority of the population, reliant on public mental health services, encounter obstacles and limited resources, not only in their communities but also in receiving mental health care (De Wet, et al., 2019), which may influence mental health negatively (Schneider et al., 2016).
Barriers
Of the barriers that participants discussed, environment, family, public mental health services, stigma and SUs’ attitude or behaviour were found to be most salient. The two barriers mentioned the most by far were environment and family.
Environment
It is not surprising that the environment was mentioned frequently, given the challenging study context described earlier. A recovery non-conducive environment was identified both at hospitals and in communities. We discuss the community environment here. The hospital environment is discussed under public mental health services. On a basic level, barriers such as lack of food and accommodation, because of a lack of work and resulting income, as well as a lack of refuge, were cited. One male SU said, ‘So I have no symptoms now and I have no place to stay’. This quote is illustrative of many other participants’ statements, that families often do not accommodate SUs upon discharge, leaving SUs in institutional care, because SPs cannot discharge them without refuge in the community. Poor social conditions, with ‘lack of . . . supportive structures in community. . .’, indicated by a female occupational therapist, and over-crowding, that are often characteristic of the impoverished communities of origin of most SUs in this study, were additionally cited as factors detracting from recovery. These results are in line with previous studies that indicate that such psychosocial disability of, or barriers to, service users negatively affects their ability to engage in their own mental health care (Kleintjes et al., 2013), which includes recovery. In their communities, many SUs were further challenged by substances, especially methamphetamine, being easily available and thus tempted into using these substances upon discharge. Substance use has been linked to the revolving door phenomenon of re-admissions (Petersen & Lund, 2011) and mental illness (Jacob & Coetzee, 2018) being very prevalent in the study context.
As Kleintjes et al. (2012) have pointed out before, these environmental factors exacerbate the general challenges of mental health conditions and thus affect SUs’ recovery adversely.
Family
Family should be a refuge of acceptance and support (Kleintjes et al., 2012). Yet, participants often cited it as an obstacle to recovery.
Participants reported feeling isolated, partly because of an absence of contact or communication with family when in hospital, whether because of stigma, financial constraints or other reasons, that prohibit family from visiting. One female social worker said that SUs often confided in her, ‘I think my family don’t love me’. in response to families’ lack of involvement or visits.
Expectations by relatives of SUs also added to pressure and judgement SUs experienced in the family context. A female SU expressed this by relating what her aunt said, ‘. . .everything depends on me [SU] to become healthy, for my children’s sakes’. These expectations might be due to the lack of knowledge about mental illness and recovery by family members, who often expect SUs to not experience any symptoms upon discharge.
Upon discharge, SUs also felt they were questioned or watched by family and not trusted. A male SU said, ‘So that thing doesn’t work in terms of recovery, you know, they watch each and every movement that you’re doing at home. . .’
In a 2015 systematic review on the recovery barriers and facilitators in schizophrenia by Soundy et al., similar to these study findings, disengaged relationships were identified as a barrier.
Public mental health services
Especially SPs, confessed that SUs often had to be discharged to make space for others SUs awaiting treatment. A female psychologist acknowledged their limited resources created an environment where almost only those SUs struggling with severe symptoms receive attention, ‘You almost like have to earn your place. . .’ Too early discharge has been described as a cause of regular re-admission of SUs in this context (Docrat & Lund, 2019, October 9; Petersen & Lund, 2011).
SPs also recognised that high turnover in staff created challenges for SUs, who wished for SPs to remain in their positions. One male psychologist expressed SUs’ dismay as, ‘You’re [SP] not going to leave us [SU] again’.
Participants also emphasised SUs’ lack of agency while in hospital; being told what to do and when to do it. A male SU described it practically as, ‘Even the TV time, like 5 pm they lock us in and then you’re going to be able to watch TV at 8 pm’. This lack of decision-making power can lead to institutionalisation for SUs. In a country, such as South Africa, where public mental health services are still delivered largely on an institutional basis, with resource-constraints, uniform treatment of SUs and given the social context that requires some SUs to stay in mental health care longer than necessary, institutionalisation is prevalent and, in turn, not only aggravates the lack of agency, but can result in dependence, helplessness and (self-)stigmatisation. A female psychologist summarised it, ‘. . .the longer they’re here, the more they perceive themselves as this crazy person. That’s all they are. That’s all they can ever be’.
These factors, together with the lack of sufficient support from government for mental health services (Petersen & Lund, 2011) and resultant pressure on such services (Lund et al., 2012), contribute to a public mental health service which does not support recovery adequately. Mental health services need to be strengthened on every level (Jacob & Coetzee, 2018).
Stigma
‘Like, nobody’s got faith in me. Or I’m like a demon. . .’ indicated one male SU’s high self-stigmatisation. Being institutionalised was closely linked to stigma in the study context. A female carer (sister of a SU) expressed it plainly as, ‘. . .we didn’t want to have her institutionalised. A lot of stigma goes with that’.
Other general challenges that most South Africans faced, like getting work, was even greater for SUs, because of stigma. A male SU explained, ‘Some other jobs I don’t think they can accommodate people that have disability, not unless that company is willing to do that’. Another male SU elaborated on the effects of stigma, They heard you’ve got mental illness and it’s a sickness for life. And then that’s where they have doubts about you being friendly, or being communicative or, landing up lending something or borrowing you something and they’re like distancing themselves from you. And your life suddenly changes. It’s like you’re blindfolded. There’s nobody you can count on, then the hopeless starts taking place and you feel like a nobody. That’s what I experience.
As the quote above indicates, stigma can lead to feelings of hopelessness and insignificance, as Kleintjes et al. (2012) pointed out too, which can counter the recovery gains that may have been made by SUs. Stigma has been previously identified as a barrier in a scoping review of systematic reviews of personal recovery (Van Weeghel et al., 2019).
SUs’ attitude or behaviour
Some participants regarded SUs’ attitude or behaviour as standing in the way of their own recovery, at times. Although identified as a barrier, it is necessary to emphasise that it does not exist in isolation, but is influenced by the impact of social, environmental or institutional factors, some of which have been mentioned, on the SU. Examples of such attitudes or behaviour are aggression, lack of self-care, negativity, lack of trust of others, lack of awareness and lack of responsibility. A male psychologist regarded ‘. . .a negative attitude . . . towards the recovery process’ in the first instance as a barrier. One male SU expressed responsibility required as, ‘. . .patient must work [on] himself for a recovery’. Prioritisation of mental health resources by health departments and the fostering of further and more, sincere collaboration between SPs, carers and SUs could adjust the attitudes or behaviours of SUs to support recovery.
Peer support work (PSW) is the facilitation of a SU’s recovery process through the assistance by other SUs (Puschner, 2018). PSW is an under-utilised resource in South Africa (Vally & Abrahams, 2016). Despite the wide-ranging results of the effectiveness of PSW interventions (Vally & Abrahams, 2016), in our opinion implementing PSW can potentially play a role to mitigate the described barriers to recovery, by counteracting the lack of supportive structures in communities, reducing re-admissions and assist in addressing stigma and SUs’ attitudes or behaviour.
Facilitators
Despite the presence of potentially debilitating barriers, participants discussed many facilitators too. The most salient of these were support, family or friends, SPs, structure and empowerment.
Support
The biggest identified facilitator of recovery was support of SUs by family, friends and SPs. Support encompassed care for, genuine interest in, compassion for, belief in, encouragement or motivation of, and non-judgement of SUs. Many participants echoed this succinct sentiment of a male nurse, ‘Recovery is support’. A female occupational therapist emphasised the positive influence of family participation, ‘. . .the more family we have involved, or family support we have, the better’.
Participants mentioned that spirituality, such as attending church, praying and faith or belief in a higher power, also supported SUs by providing hope, meaning, acceptance and motivation to overcome isolation and negativity. ‘So, it [believing] helps me in a sense that make me want to think positive and not in a negative way’, said a male SU. A carer sister described her brother’s faith, ‘That [faith] has also been a support in his life. . .’ and confirming that ‘It [faith] does plays a role in his recovery. . .’ A psychiatrist was convinced that, ‘. . .if people believe in something, they have a better chance’.
Support has been found to contribute to a healthy, stable environment for SUs in which they could be recovering safely and securely (Kleintjes et al., 2012). The results of the present study re-iterate the findings of several other studies worldwide that support is an important facilitator of recovery (Garverich, 2020; Van Weeghel et al., 2019). In a previous, similar South African study, support was regarded as possibly the most significant facilitator of recovery (De Wet et al., 2015).
Family or friends
An important facilitator of recovery, and closely linked to support, was family and friends. Participants referred to them positively using words such as ‘honesty’ of relationships between SUs and friends or family, ‘knowledge’ of carers, being vigilant for relapses, ‘role model’ of friends or family members, ‘connection’ between SU and friends or family, and ‘trust’. A female occupational therapist stated that, ‘. . .family’s an asset to recovery. . .’
When asked what supports him to not give up on his recovery, a male SU said, ‘My friends and my sister. For them, when they are giving words that they trust me. When they show that they trust me. I tend to have that courage’. The same SU also referred to his trust in others, ‘having someone to talk to that you [SU] trust’, which is accompanied by his trusted others being honest with him.
Connection for SUs was regarded as one of the important aspects of recovery by a female occupational therapist, ‘Re-connection to self, re-connection to on, on, on many levels. . .’ Knowledge of illness by families was also cited as supportive, by preparing SUs for relapses.
These results confirm the results in previous studies that positive family and service provider relationships play a facilitative role in the South African context (Brooke-Sumner et al., 2014).
Service providers
The attitude of SPs towards SUs was regarded as crucial to recovery. A male psychologist explained the need for SPs acknowledging their common humanity with SUs, ‘They [SUs] are human, ja. Umm. . . We [SPs] are human. Umm. . . and I think that, that’s what make the difference. Cause that’s how we [SPs and SUs] need to relate to each other’. This humane approach (Farkas, 2007) is an echo of South African studies that have advocated for it before (Kleintjes et al., 2012).
Recovery-oriented hospital interventions that some participating SPs facilitated, like a market garden project and sharing life stories amongst SUs, seemed to have anecdotal beneficial effects on SUs’ recovery. SUs received a stipend for their work in the market garden and, ‘. . .immediately it raises. . .your [SU’s] position in the. . .household’, confirmed a female occupational therapy technician. She also speculated on how acquisition of skills in the market garden project could make SUs feel, ‘And it [acquired skills] makes you feel in terms of the mental illness that you have, you can live with it, because you can also do something’. According to another female occupational therapist participant, sharing life stories amongst SUs ‘. . .can be the basis for the rest of their recovery process’, which again emphasised the positive role that PSW can play.
Except for the role that family and friends and SPs play separately, the collaboration between SPs and family, which is necessary to facilitate recovery (Kleintjes et al., 2012), was also confirmed by participants.
Structure
Structure included routine and order to support SUs’ recovery. One male SU was adamant that routine and structure was essential to his recovery, ‘Doing like a timetable or a roster for myself what I’m going to do during the week. Like going to drumming or wake up and exercise, drumming, going to library, printing my stuff, my CV and handing [CV] over. . .’ A female SU felt getting up at a certain time every morning assisted her, ‘. . .every day I get up at more or less the same time’ as well as ‘. . .do[ing] more or less the same thing every day’. These excerpts emphasise the predictability in routine and structure for SUs helping them in their recovery. This female SU’s carer, in a later interview, re-iterated routine providing a sense of control to the SU. One female psychiatrist linked routine with responsibility, which, in turn, gave SUs purpose and built self-esteem.
We regard structure as the scaffolding necessary for the recovery process of SUs.
Empowerment
Referring to empowerment, participants highlighted the need for some independence or sense of agency for SUs in their recovery. One male carer expressed it as, ‘So, that independence I think is also important for his recovery’. A female psychologist highlighted the empowering role the multidisciplinary team can have in encouraging SUs to voice their needs, ‘. . .a part of the multi-disciplinary team’s work is very much empowering them to be able to voice, to give them a voice’.
A male psychologist referred to the empowerment of SUs that comes from sharing experiences with other SUs, ‘When they come back [SUs from a leave of absence from hospital] and we’re in a group, a group setting sometimes you [returning SU] perhaps want to share what your experience has been like. And, in that way they [rest of the group] can also perhaps somehow feel empowered’. This confirms the empowerment potential of PSW (Lund et al., 2012), which could be a powerful resource given the great financial and resource constraints faced in South Africa.
Systematic reviews (Soundy et al., 2015; Wood & Alsawy, 2018) and a scoping review of systematic reviews and meta-analyses of recovery literature (Van Weeghel et al., 2019) emphasised certain additional barriers, such as substance use, lack of confidence or hope, effects of medication, as well as facilitators, such as acceptance, keeping busy, hope and self-determination, to the ones in the present study. Although participants in the present study also referred to many of these barriers and facilitators, we only discussed the most salient barriers and facilitators. The presence of these barriers and facilitators in the findings from the systematic reviews and scoping review and the present study encouragingly substantiates the possible universality of certain barriers and facilitators for SUs in varying contexts.
The barriers to recovery, even the SUs’ internal attitudes or behaviours, which were influenced by environmental factors, seemed to stem, to a large extent, from intersecting external sources related to interpersonal (family), community, institutional, and societal factors, as pointed out by Van Weeghel et al. (2019). The facilitators, in turn, seemed to centre not only around relational factors, predominantly in the form of support, but also around systemic factors through empowerment and structure. It is our opinion that recovery is facilitated where SUs are aided to develop their own strength to recover, but importantly, in conjunction with enabling environmental factors (Kleintjes et al., 2013; Van Weeghel et al., 2019). Public mental health departments should invest in recovery-enabling service environments, that are SU-oriented, to involve them in their recovery meaningfully (Farkas, 2007), and develop formal PSW, the latter of which can be done collaboratively with community organisations to work towards more recovery-enabling environments within communities through which other barriers, such as stigma, can be addressed too.
Limitations
The small number of participants limits generalisability. However, it is not the aim of qualitative research to be generalisable, but rather to provide a rich description of the participants’ experiences, to saturation, which we achieved. In so far as the results can potentially be representative, they may however not be representative of other parts of South Africa. The public mental health spend per capita in the Western Cape is the highest in South Africa. In other provinces, this spend has ranged from only 19% up to 82% of the amount spent in the Western Cape (Docrat et al., 2019). This may also influence the experiences of SUs in other provinces.
Recommendations
Since this was a small-scale study and barriers and facilitators might differ for SUs in other locations, it is recommended that the study be replicated in other South African provinces to determine whether experiences are similar in such other locations. The results from the study point to the benefits that could be gained from the implementation of PSW, which could, on the one hand, counteract barriers to recovery, such as lack of supportive structures in communities, reducing re-admissions (Davidson et al., 2012), addressing stigma and SUs’ attitudes or behaviour, and, on the other hand, support facilitators, such as empowering service users (Davidson et al., 2012) and peer support workers, and potentially reducing the cost burden for health departments through fewer re-admissions. It is recommended that the further development of PSW in the South African context be investigated as an additional resource for SUs to curb barriers and enhance facilitators in the recovery process.
Conclusion
The barriers and facilitators discussed seemed to link with each other and we found it difficult to discuss one without finding overlap with another. This indicates how individual (SUs and SPs), social (family, friends and community), institutional (overall mental health services and government) and societal (social conditions) factors weave an intricate web of conditions and create intersections, which make the recovery process particularly complex, and challenging, for SUs in South Africa. However, the need for support seemed to cut across all these factors. In South Africa, a largely untapped, potential recovery resource, PSW, could be developed further with proper regulation of who delivers PSW, how PSW is delivered and evaluated (Vally & Abrahams, 2016) as well as appropriate training programmes for peer support workers (PSWs) in the context (Pathare, 2018). As the need for support was an underlying component to all the barrier and facilitator themes, PSW could address it very well. PSW could not only support SUs’ recovery, but also lend support to SPs and mental health services in relieving the overwhelming burden of care that they carry, provide previous SUs (who become PSWs) with meaningful work and much-needed income, and address stigma through more wide-spread mental health knowledge in communities. Ultimately, PSW could also benefit health departments financially (Moran et al., 2020).
Footnotes
Author note
This manuscript is based on research supported through a scholarship awarded to the first author by the National Institute for Humanities and Social Sciences (NIHSS) in collaboration with the South African Humanities Deans’ Association (SAHUDA). The first author acknowledges that opinions, findings and conclusions or recommendations expressed in any publication generated by the research are those of the author, and that the NIHSS and SAHUDA accept no liability whatsoever in this regard. We wish to thank the participants for their involvement in the interviews and focus group discussions, without which the data and the results would not have been possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript is based on research supported through a scholarship awarded to the first author by the National Institute for Humanities and Social Sciences (NIHSS) in collaboration with the South African Humanities Deans’ Association (SAHUDA). The first author acknowledges that opinions, findings and conclusions or recommendations expressed in any publication generated by the research are those of the author, and that the NIHSS and SAHUDA accept no liability whatsoever in this regard.