
Abstract
Background:
Public funded outreach services for persons with severe mental disorders (SMDs), a norm in developed nations, is non-existent in India. We share our pilot experience with an indigenous model named ‘Care at Doorsteps’ (CADs) for persons with SMDs who dropped out from clinical care of District Mental Health Program (DMHP) at three sites of Karnataka, a south Indian state.
Aim:
The objectives of this study were to identify the reasons for drop outs from routine care and to assess the burden of illness and disability after the intervention.
Methodology:
Six-month prospective observational study on patients aged 18–60 years, diagnosed as Schizophrenia or bipolar disorder was conducted. Three home visits were made by the team and provided medications, also offered brief psychoeducation and counselling. Care-givers were interviewed to identify the reasons for drop outs and their expectations from the treating team. Patients were also assessed using the Clinical Global Impression Scale (CGI), Indian Disability Evaluation and Assessment Scale (IDEAS) and Burden Assessment Schedule (BAS) during each visit.
Results:
Ninety-six patients (50 males and 46 females) were followed up, of which 85 had a diagnosis of schizophrenia and 11 with bipolar illness. Common reasons for drop out were: single caregiver (breadwinner) unable to accompany the patient, loss of faith in medical treatment and financial constraints. Symptomatic improvement and restoration of productive work were the priority expectations. Over the course, the mean CGI-S showed significant reduction (4.81 ± 1.57, 4.46 ± 1.32 and 4.11 ± 1.39 respectively; p = 0.001). Mean score on BAS showed a significant reduction (85.76 ± 12.15, 83.46 ± 11.30, 84.27 ± 11.82; p = 0.04). Mean total IDEAS scores did not show significant change (13.27 ± 4.78, 12.82 ± 4.24, 13.17 ± 4.40; p = 0.16).
Conclusion:
Meaningful assertive outreach care is feasible in India and is found to be useful for persons with SMDs by utilising the already existing public sector resources.
Introduction
Severe Mental Disorders (SMDs) are chronic highly burdensome medical disorders requiring lifelong care (Ruggeri et al., 2000; Collins et al., 2011). Though there are multiple reasons that contribute to burden of illness, treatment non-adherence, dropouts from care and frequent relapse are some of the important reasons (Kumar et al., 2016; Robinson et al., 1999). Dropout rates after the initial assessment in a rural psychiatric clinic in India has been found to be as high as 50% (Kulhara et al., 1987) and further 25% of the patients drop out within the next two visits (Agarwal, 2012). Assertive outreach services for persons with SMDs did infact start to address these factors particularly (El-Mallakh & Findlay, 2015). These services though named differently, includes in a nutshell, various degrees of services offered to patients at their doorsteps. Case management, Assertive community treatment (ACT), crisis resolution, Community Treatment Orders (CTO; Burns et al., 2013) are some examples of such care. These assertive outreach services have been shown to improve patient outcomes. For example, ACT which involves a coordinated team to work at the community reduces hospitalisation rates and improves quality of life of patients. In UK, high fidelity ACT did not demonstrate superior clinical outcomes over community mental health team (CMHT) but patient satisfaction was found to higher with ACT (Bond et al., 2001). Increased medication adherence is thought to result in reduced hospitalisations in ACT (Killaspy et al., 2009). Importantly, all these outreach services offer a range of time-unlimited services with low patient-staff ratio with high overall cost of management which cannot be replicated in resource constrained settings such as India. The modus operandi of such services needs to be tweaked to suit the local resources. Care at Doorstep (CAD) model is one such attempt that utilises the existing District Mental Health Program (DMHP; the operational arm of the National Mental Health Program of India) resources. CAD was piloted in three districts of Karnataka State of India. Each DMHP team of Karnataka consists of one Psychiatrist, one clinical psychologist, one social worker, two nurses, one record keeper and one office assistant co-ordinating and carrying out various clinical, capacity building and information (and) education activities within the district. In this paper, we attempt to summarise the pilot effort of providing care at doorsteps of patients with SMDs who dropped out of the outpatient DMHP care.
Methodology
Setting
The study was conducted in three districts of Karnataka state of India, where the District Mental Health Programs (DMHPs) are fully functional. DMHP services include (1) provision of clinical services for new as well as follow up patients, in predominantly outpatientclinics spread across the district (district hospitals, taluk hospitals, community health centres, and primary health centres) (2) Training and capacity building of medical officers, para medical staff, teachers, firemen, Anganwadi worker and ASHAs worker as part of capacity building and (3) Information, Education and Communication (IEC) activities to create awareness about mental illness and reduce stigma. Along with these, there are targeted interventions like School mental health programme, College counselling programme, Workplace stress management programme etc (Balamurugan et al., 2019). The following DMHPs were chosen conveniently for the purpose of this pilot study.
1. Urban arm: Two Centre’s
a. Bengaluru Urban: There are total of four zones as Bengaluru South, Bengaluru East, Bengaluru North and Anekal taluk. Bengaluru Urban DMHP covers an area of 804.83 km2 with total population of 5.6 million.
b. Bengaluru BBMP: The Bruhat Bengaluru Mahanagara Palike (BBMP) is the administrative body responsible for civic amenities and some infrastructural assets of the Greater Bangalore metropolitan area which is divided into south, east and west zones, which has a population of approximately 6.8 million in an area of 741 km2. The DMHP of BBMP covers whole of this area.
2. Rural arm: One Centre
a. Ramanagara: Ramanagara is a district situated 50 kilometres from Bengaluru comprising of four taluks of Ramanagara, Channapatna, Magadi and Kanakapura. It has a population of about 1.2 million and 75% belong to the rural sector. Total area of the district is 3556 km2. The DMHP of Ramanagara covers the whole of this district.
Sample selection
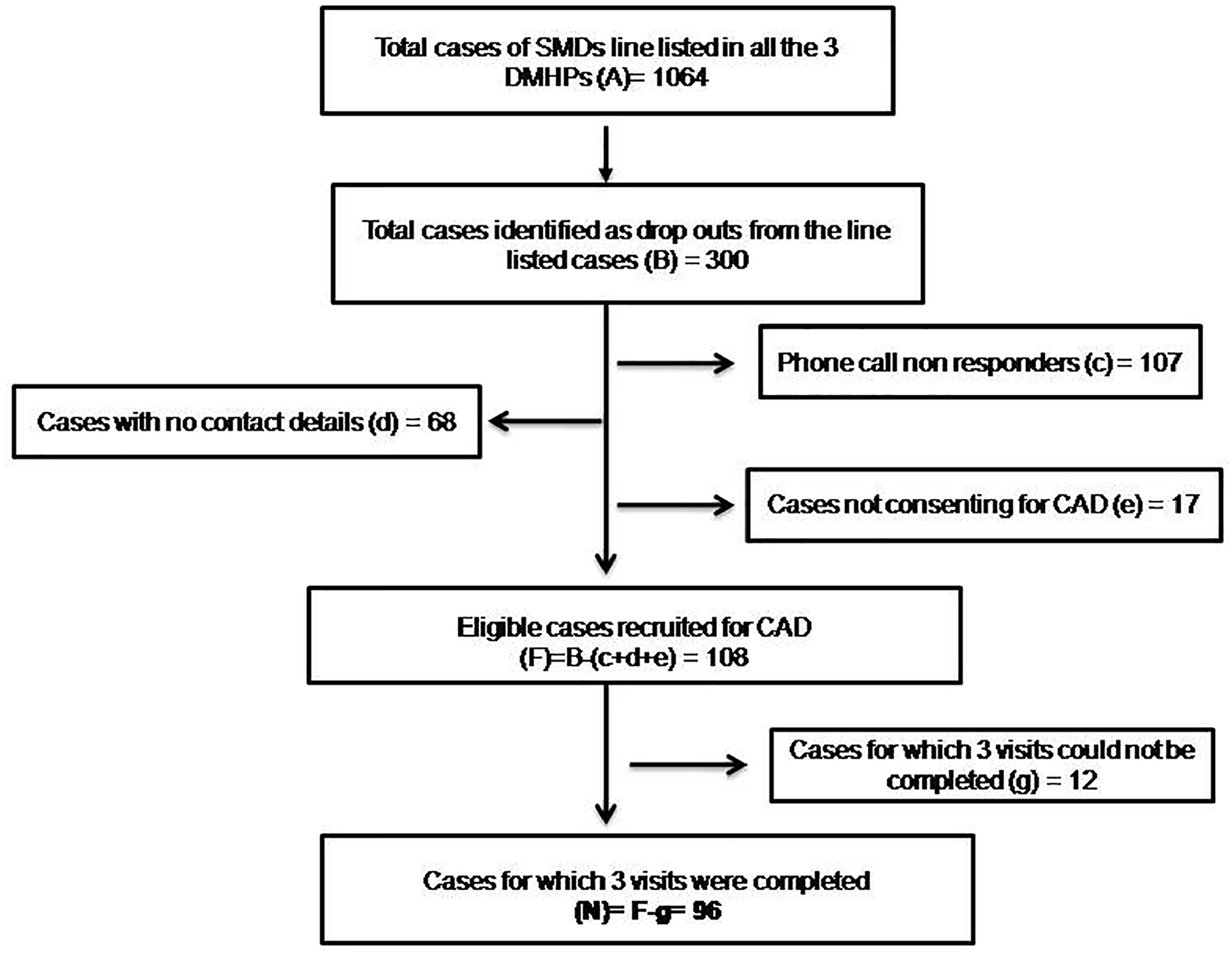
Patients with a diagnosis of schizophrenia/schizoaffective disorder or Bipolar Affective Disorder (according to ICD-10 or DSM-IV) by treating psychiatrist, aged 18–60 years of either gender, who dropped out from regular follow-up despite medical advice since full inception of the DMHP services from January 2016 were line-listed and contacted telephonically (when details were available). Dropouts were considered as patients who had completely disengaged from clinical services after their baseline index visit or the first follow-up (Grover et al., 2018). The formal recruitment of consenting families for the CAD began in May 2018 and completed by September 2018. The details regarding the recruitment are represented in Figure 1.
Procedure for recruitment to CADs.
A team of one social worker and one psychiatric nurse visited their homes under supervision of Psychiatrist. Total of three home visits were done at 2 months intervals. During home visits, assessments were done, medicines given to patients/families (including administration of parenteral medications if necessary) and psycho education provided based on need/issues identified during home-visits. Misbelieves about illness, concerns about side-effects of medications and perceived stigma were addressed as part of the intervention. The parenteral medications were given as per schedule prescribed by Psychiatrist by the psychiatric nurse (such as fortnightly) while other interventions and assessments were done only at 2-month intervals. The treatment plan was discussed with Psychiatrist over telephone by the CAD team.
Tools for assessments
Statistics
Clinical and Socio-demographic characteristics of the sample were analyzed by descriptive statistics and represented as mean with standard deviations and percentages. For the assessment scales used, a general liner models for repeated measures as multivariate analyses of means were performed using the level of statistical significance at p < 0.05. We categorised the outcomes as ‘worsened’, ‘unchanged’ and ‘improved’ depending on the difference between the scores on the respective outcome variable between visit 1 and visit 3. We conducted one-sample chi-square tests with null-hypotheses of equal proportion of patients being categorised into these three categories.
Results
The socio demographic details of the participants are given in Table 1. There were 85 patients with a diagnosis of schizophrenia and 11 had bipolar affective disorder. Table 2 gives details of the CADs pilot program. About a quarter of patients/family members reported they were not even aware that continued follow-up is essential. As regards to the family issues contributing to dropouts, non-availability of dedicated care giver to accompany the patient to the hospital, other family members not willing to accompany an uncooperative patient and loss of faith in medical treatment due to minimal improvement while on medications, seeking alternate magico-religious treatment and perceived stigma about attending a psychiatric OPD were some of the explanations given by caregivers. Financial issues included not having enough money to travel, visit to hospital meant loss of wage for that day for the primary care giver. Symptomatic improvement and restoring productive work functioning were the two notable expectations from the health care services as reported by the patients/family members.
Socio-demographic details of participants (n = 96).

Reasons for drop out a and service user’s expectations (n = 96).

Dropouts in this table pertain to only 96 patients who took part in the study. Reasons for not including the remaining 202 are described in the flowchart.
Judgment exercised by the team members after discussion with patients/caregivers.
Symptoms, disability and burden of care
There was significant improvement in the illness severity at end of the third visit when all patients were considered (n = 96). Family burden too showed significant reduction. Disability did not change however (Table 3). Same trend was observed when proportions of change was analysed over these three visits. As regards to family burden, when compared to the baseline, 51%, 16% and 29% had improved, remained unchanged and worsened at the end of 3rd visit respectively [χ2(1, N = 96) = 19.56, p < 0.001]. As regards to symptoms, 47%, 33% and 16% had improvement, remained unchanged and worsened respectively [χ2(1, N = 96) = 15.6, p = 0.001]. However the disability did not change: only 23% had shown improvement while 57% had scores unchanged and 15% had worsened at end of the third visit [χ2(1, N = 96) = 31.41, p < 0.001].
IDEAS and BAS scores across the three visits (n = 96).

Note. Mean (SD).
p < .05 (two-tailed).
For those with schizophrenia alone (n = 85), symptoms decreased significantly in every domain of CGI scale. CGI-Positive symptoms: 4.67 (1.87), 4.43 (1.30), 4.13 (1.28) during first, second and third visit respectively and F = 7.34, p = 0.001. Similarly, CGI-Negative symptoms scores were 4.53 (1.45), 4.23 (1.33), 3.98 (1.23) and F = 7.56, p = 0.001. The CGI-depressive symptoms severity scores were 4.34 (1.70), 4.24 (1.30), 3.92 (1.28) and F = 5.11, p = 0.008. The CGI-Severity of cognitive symptoms scores were 4.78 (1.63), 4.61 (1.34), 4.30 (1.40) and F = 4.97, p = 0.009. The overall symptoms severity CGI-S among patients with schizophrenia were 4.81 (1.61), 4.52 (1.28), 4.18 (1.36) and F = 7.60, p = 0.001
Discussion
To our knowledge this is the first prospective study (in India) to document the feasibility and utility of assertive outreach services for persons with SMDs utilising the existing resources of DMHP. Following the pilot study, the DMHP has successfully carried out the CADs, providing service to about 6000 patients with SMDs during the financial year 2019–2020 (Satheesh et al., 2019). The participants were chosen from both urban and rural background who had utilised the DMHP services at least once before. Rates of patients on irregular follow up ranged from 17.3% in rural setting to up to 43.8% of the urban patients, which is similar to the rates reported in other Indian studies done in out-patient settings (Gill et al., 1990; Kaur et al., 2009). Since financial issues and family related issues were the commonest reasons for drop out which is similar to previously conducted prospective follow up study in North India (Singh, 2015), through CAD it was possible to overcome those barriers and establish pathways for continuity of care.
Significant reductions in scores of clinical severity and family burden were on the expected lines (Chatterjee et al., 2009). However, there was no change in the ‘disability’. It is well known that 6 months is less to assess any meaningful change in disability (Srinivasamurthy et al., 2005). CAD for 1 or 2 years might give us more evidence in improvement across all dimensions. Only one patient needed referral to a higher centre for care, which is similar to the evidence-based ACT model, with an added benefit of having lesser strain on human resources. Though formal cost-effective analysis was not done, it intuitively appears to carry this benefit as well.
One third of patients who were irregular to follow-up returned to treatment with a phone call from the health care provider. The proportion is much higher in rural areas (more than 50%). This is a low cost and high impact intervention which is feasible in all set-ups. In some cases, families may postpone follow-up due to some other priorities (a few pills remaining, harvest season when family earns income in rural areas, other important work, social gatherings etc.). In most instances as found in our study, the primary caregiver of patient may not be aware about the scheduled follow-up. In such cases, a telephonic reminder ensures that patient is brought for follow-up. In our study while recruiting participants, almost 20% of irregular patients couldn’t be contacted due to lack of adequate contact details recorded at time of registration. With recent entry of a telecom operator with aggressive tariffs, many have two Subscriber Identification Module (SIM) cards. The old SIM registered with multiple purposes is used for incoming calls and receiving important messages. Recently, it has been mandated to do a minimum monthly recharge to keep the SIM active. A proportion of people are unaware about this and it is difficult to reach out to them in old number. It is important to take 2–3 numbers for each patient to help reach out to them. Telepsychiatry is another method to ensure continuity of care. The recently gazetted telemedicine guidelines is facilitatory to both audio as well as video consultations (Medical Council of India, 2020, ‘Telemedicine Practice Guidelines’).
In 3%, patient/family refused CAD without assigning any reasons. It is likely that there are complex family dynamics which are responsible for same (Reddy et al., 2014). In many poor families, the priority is to ensure survival for basic needs and seeking treatment for patient is not the first priority (Villeneuve et al., 2010).
Many patients drop-out of treatment due to financial and logistic constraints (inability to travel long distances, lack of caregiver to accompany to hospital, monetary constraints to pay for consultations and medications; Jain et al., 2017) and our experience also showed similar experience, except accessibility as an issue was reported only by 2% of them. This may be due to availability of DMHP services as community based setting and the local camps being organised by DMHP.
Though formal cost effectiveness analysis has not been done, the service is bound to be largely cost-effective. There are a couple of important reasons for the same. (a) CAD services do not require additional funds as they will be conducted with the available (already sanctioned) funds and (b) from the perspective of the families, as the services reach their door-steps, there is a huge saving in terms of the travel cost. Not to mention that if patients remain in recovery phase, the financial gain that can potentially occur because of their employment. However a formal analysis of cost effectiveness was not carried out in this study.
Further, CAD team couldn’t reach out to 3% patients due to logistic issues like difficulty in getting DMHP vehicle/other transport arrangement, inaccessibility by road, difficulty in locating house, preference for home visit in early morning or late evening so that their work is not disturbed. In some cases, CAD staff (2 ladies) did not feel safe to visit places which were remote or deserted.
Conclusion
This pilot study by the DMHP team in three different settings shows that delivering care at door step with the existing resources of DMHP is possible both in urban and rural setting and range of services such as administering depot injections to psychosocial interventions can be done with no compromise in quality of care. With adherence to treatment, improvement in symptoms and reduction in disability with decrease in care giver burden is possible (Danzer & Rieger, 2016).
Future directions
Formal cost-effectiveness analysis of such model of care, including the financial savings for the patient’s family and long term benefits needs to be done and also feasibility at all centres can be known only if such study is replicated at other centres.
Footnotes
Acknowledgements
The authors would like to acknowledge:
a. Patients and their families who consented and participated in the study.
b. Ms. Jayashree C, Ms Manjula and Ms. Padma Rekha S, Psychiatric Social Workers of the DMHP of Bengaluru BBMP, Urban and Ramnagara respectively.
c. Ms. Anitha BK, Mr. Solomon and Ms. Pavithra M, Community nurses of the DMHP of Bengaluru BBMP, Urban and Ramnagara respectively.
d. The District Mental Health Officers (District Level Officers; DLOs) of Bengaluru BBMP, Urban and Ramnagara.
e. Gautham S, Projector coordinator, Telemedicine Centre, National Institute of Mental Health and Neurosciences, Hosur road, Bangalore, India.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No dedicated funding for the purpose of the study. The study was conducted utilising the routine funds made available to run the ‘District Mental Health Program’ at Ramanagara and Bangalore Urban district.