
Abstract
Background:
The study was conducted to determine the relationship between self-stigmatization and perceived social support in caregivers of schizophrenia with patient.
Methods:
A cross-sectional study design was used. The study sample consisted of 84 participants who cared for schizophrenic patients registered in a community mental health center. In the data collection, the ‘Self-stigmatizing Scale for Families’ and ‘Multidimensional Perceived Social Support Scale’ were used. The data were analyzed via frequency, mean, standard deviation, Cronbach’s alpha analysis, linear regression, Pearson correlation analysis, independent samples t-test, and ANOVA test.
Results:
Self-stigmatization (32.48 ± 15.15) and perceived social support (44.36 ± 22.88) were found to be moderate in caregivers. Self-stigmatization was found to be higher in caregivers who do not work; have a spouse, mother, or father; have a disease; do not receive support from their family and have not received any education about schizophrenia (p < .05). It was determined that, with increasing age, perceived social support decreases, and the perception of social support increases in caregivers who are high school graduates, working, having children, have no illness, and are educated about schizophrenia (p < .05). It was determined that, as the level of perceived social support increases in caregivers, self-stigmatization decreases (p < .05).
Conclusion:
It was determined that, as the perceived social support increases in caregivers, self-stigmatization decreases. We recommend providing informative support about schizophrenia, to increase hope and social-skill training, and to implement interventions that include caregivers in the fight against stigma.
Introduction
Patients with schizophrenia are perceived as stigmatized by society, anxiety inspiring, disorderly, and aggressive. They are expected to exhibit different behaviors and are excluded from society (Yilmaz & Okanli, 2015). In schizophrenia, stigmatization affects not only patients, but also family members of patients (Kaşlı et al., 2020; Yıldız et al., 2019). Stigma is considered one of the most important problems faced by schizophrenia patients and their caregivers (Ergetie et al., 2018; Singh et al., 2016). Caregivers who encounter stigma behaviur can easily stigmatize themselves by internalizing this behaviur over time (Chang et al., 2017; Guan et al., 2020a). Research suggests that self-stigma is as damaging for relatives as it is for patients with schizophrenia, causing psychological distress, hopelessness, less social support (Guan et al., 2020b) worthless, is ashamed of herself or himself, is socially withdrawn, and as a result, her or his help-seeking behavior and caregiving capacity decreases (Amering & Schmolke, 2009; Clement et al., 2015). The self-stigmatization of individuals who care for patients with schizophrenia may cause shame, low self-esteem, a decrease in quality of life, and a decrease in caregiving capacity (Wong et al., 2018). In a study conducted by Yin et al. (2014), it was stated that caregivers of patients with schizophrenia experienced significant stigmas associated with inadequate perceived social support. In addition, it is stated that caregivers of patients with schizophrenia in general avoid telling others that their relatives are being treated for schizophrenia and move away from their social environment due to stigma. Caregivers of patients with schizophrenia are exposed to shame, low self-esteem, low perceived devaluation, low social self-efficacy, and social isolation due to perceived stigma. Perceived devaluation and discrimination by caregivers of patients with schizophrenia cause them to use ineffective coping methods such as social withdrawal and concealment (Ergetie et al., 2018). The caregivers of patient with schizophrenia beliefs that most people will be little them, ignore, and avoid making friends with them, or would be hesitant to communicate with them could stop them from seeking help and social support when needed (Clement et al., 2015).
Self-stigmatization of the caregivers of schizophrenia patients has a negative effect on perceived social support (Korkmaz & Küçük, 2016). In a studies conducted by Guan et al. (2020a) and Yin et al., (2014) reported that self-stigmatization is associated with low social support in caregivers of patients with schizophrenia. Previous studies have revealed the protective function of social support in the development of self-stigmatization (Chronister et al., 2013; Geffner et al., 2017; Livingston & Boyd, 2010). Although social support has a positive effect in combating stigma, perceived social support in caregivers of schizophrenic patients is insufficient (Chen et al., 2016; Chronister et al., 2013; Yu et al., 2020). Interventions that provide social support for these caregivers can be an effective method to reduce self-stigmatization (Guan et al., 2020a; Shi et al., 2019). Therefore, it is important to examine the relationship between self-stigmatization and perceived social support in caregivers who provide continuous care to patients with schizophrenia. The novelty of this study is the use of a measurement tool that provides a multidimensional approach to determining self-stigmatization in these caregivers and examining the relationship between self-stigmatization and social support perception. The aim of this study is to determine the level of self-stigmatization and perceived social support in caregivers of schizophrenia patients and to reveal the relationship between self-stigmatization and perceived social support. The research questions we intend to evaluate are (1) What is the level of self-stigmatization and perceived social support of the caregivers of schizophrenia patients? (2) Is there a relationship between the sociodemographic characteristics of these caregivers and the level of self-stigmatization and perceived social support?
Methods
Participants and procedure
This cross-sectional study was conducted between January 2019 and January 2020 at the Atatürk State Hospital Community and Mental Health Center (CMHC) affiliated with Antalya Provincial Health Directorate. This center was founded in 2015 for support out-patients with schizophrenia and their family caregivers. CMHC provides psychosocial support, follow-up, treatment, and social rehabilitation services to patients with schizophrenia and family caregivers. CMHC has a therapy room, reading room, patient observation room, occupational therapy rooms, music and painting room, interview room and resting room. In addition, vegetables and fruit are grown for the purpose of occupational therapy in the garden of the middle. The center offers care every day, except on weekends, for schizophrenia patients in remission. In this quantitative study, three designs were used: descriptive, causal-comparative, and relational designs. The study sample consisted of 84 caregivers enrolled in CMHC and diagnosed with schizophrenia according to DSM-5 criteria. The sample was determined as 84 participants, taking a 5% margin of error, 80% power, and a tolerance rate of 0.05 (Chen et al., 2016; Malone et al., 2016). The selected caregivers were 18–65 years old, literate, and did not have mental retardation or any current psychiatric disorder or neurological disease that might affect their judgment and had served as caregivers for at least 1 year.
Data collection
Participants in the study were informed that participation in the study was voluntary and that the research data would only be used for scientific purposes. All research participants received informed consent including a detailed explanation of the study. Those who confirmed their participation were asked to sign these forms. The required explanations were made verbally before the forms used in the present study were given, and attention was paid to creating a quiet atmosphere where the stimuli were few. It took an average of 15 to 20 minutes to complete the survey form. Each caregiver signed an informed consent form, stating that they had received and confirmed all information related to this study. The results of the present study were reported in accordance with the STROBE guidelines.
Measures
The study’s outcome variables were defined as self-stigmatization and perceived social support. The independent variable of education level was defined by the categorical variables: literate, primary school, and high school. Control variables included the age, gender, working status, caregiver period, degree of proximity, physical health condition, and education about schizophrenia, because these factors are related to the risk of schizophrenia caregivers.
Self-stigma inventory for families
Self-Stigma Inventory for Families (SSI-F) was developed by Yıldız et al. (2019) to enable the evaluation of self-stigmatization or internalized stigmatization in the families of schizophrenia patients. The scale consists of a total of 14 items and three sub-dimensions: social withdrawal (items 1–6), concealment of the illness (items 7–9), and perceived devaluation (items 10–14). The answer to each item was graded on a five-point Likert scale as ‘do not agree (1 point)’, ‘slightly agree (2 points)’, ‘moderately agree (3 points)’, ‘generally agree (4 points)’, ‘totally agree (5 points)’. The total score is obtained by summing up the items in each sub-dimension. The lowest score that can be obtained from the scale is 14, and the highest score is 70. Higher scores indicate that self-stigmatization has increased in family members. The Cronbach alpha value of the scale was reported by Yıldız et al. (2019) as .93. It was determined that the internal consistency of Cronbach’s alpha values for SSI-F was .857 in this study.
Multidimensional scale of perceived social support
The Multidimensional Scale of Perceived Social Support (MSPSS) was developed by Zimet et al. (1988) and is aimed at determining the social support factors perceived by individuals. MSPSS validity and reliability studies were conducted by Eker and Arkar in Turkey in 1995 and Eker et al. in 2001 (Eker & Arkar, 1995; Eker et al., 2001; Zimet et al., 1988). The 12-item scale subjectively evaluates the adequacy of social support from three different sources. It is a 7-point Likert scale, ranging from ‘Very Strongly Disagree’ to ‘Very Strongly Agree’. The scale has three subscales consisting of four items each to determine the support of family (items 3, 4, 8, and 11), friends (items 6, 7, 9, and 12), and private persons (items 1, 2, 5, and 10). The possible range for each subscale is from 4 to 28. The possible range for the whole scale is from 12 to 84. A high score indicates that perceived social support is high (Eker & Arkar, 1995; Eker et al., 2001). The Cronbach alpha value of the scale was reported by Eker et al. (2001) to be .89. It was determined that the internal consistency of Cronbach’s alpha values for MSPSS was .878 in this study.
Ethical approval
All human studies have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. This study was approved by the Akdeniz University Faculty of Medicine Clinical Research Ethics Committee (Decision No: 451; Date: 27.06.2018). Institutional approval was obtained from the Antalya Provincial Health Directorate and CMHC.
Statistical analysis
The data of the study were evaluated using the Statistical Package for Social Sciences 25.0. After data preparation and inspection, sociodemographic items, and test scores on percentages, means, and standard deviations were summarized using descriptive statistics. The suitability of the data for normal distribution was evaluated using the Kolmogorov–Smirnov test. As the scales and measurements showed normal distribution, parametric tests were used in statistical evaluations. An independent sample t-test was applied to test whether scores obtained from two unrelated samples differed significantly from our quantitative variables. The Pearson correlation test was used for the calculation of correlation between the scales. Then, linear regression was applied to examine the associative factors for self-stigmatization and perceived social support in caregivers of schizophrenia patients. The results were evaluated at a confidence interval of 95% and a significance level of p < .05.
Results
Demographic characteristics
Considering the introductory characteristics of the participants (n = 84), it was determined that the average age was 56 with an average caregiving period of about 16 years, and most were women, primary school graduates, not working, and living in a nuclear family. The majority of the participants were the mothers of the individuals diagnosed with schizophrenia and had other family members who were also responsible for their care, and 71.4% of the caregivers did not receive any education about schizophrenia (Table 1).
Sociodemographic characteristics of caregivers of schizophrenic patients (N = 84).
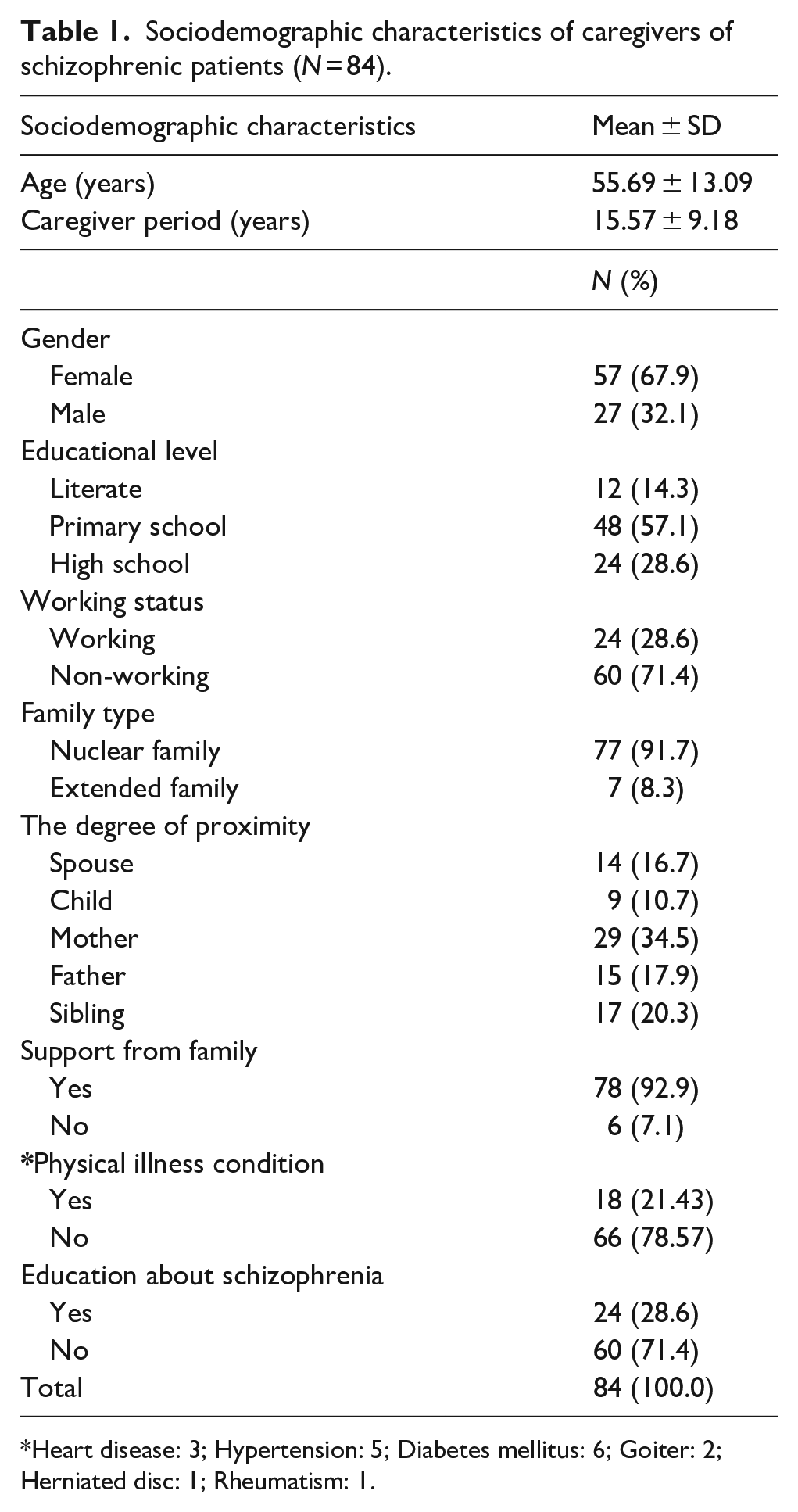
Heart disease: 3; Hypertension: 5; Diabetes mellitus: 6; Goiter: 2; Herniated disc: 1; Rheumatism: 1.
Self-stigma inventory for families and perceived social support measures
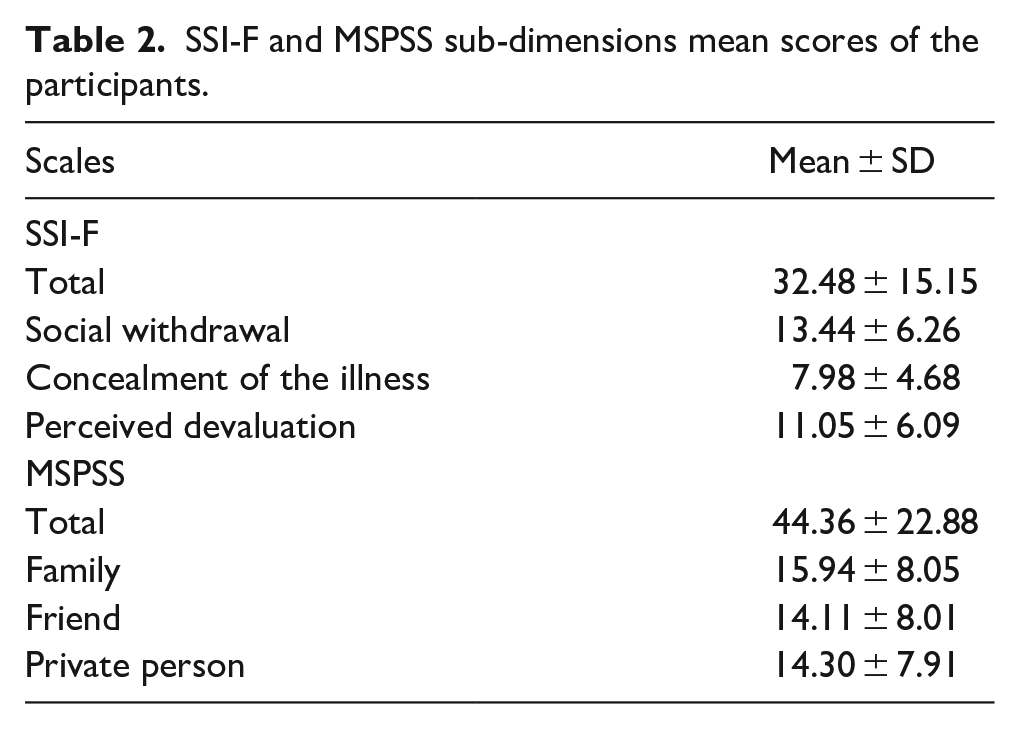
The average total score of the participants on the SSI-F scale was 32.48 ± 15.15, and the average total score on the MSPSS scale was 44.36 ± 22.88 (Table 2). The mean scores of the SSI-F scale sub-dimensions according to the sociodemographic characteristics of the participants in the study are presented in Table 3. There was no statistically significant difference between the SSI-F scale total and the sub-dimension mean scores according to the age, gender, and caregiver period (years) of the participants (p > .05). A statistically significant difference was found between the mean score for concealment of the illness according to the education level of the participants (p < .05). The mean score for concealment of the illness was found to be statistically significantly higher in primary school graduates than in high school graduates. A statistically significant difference was found between the SSI-F overall score average, social withdrawal, concealment of the illness, and perceived devaluation, according to the working status of the participants (p < .05). The mean scores of the non-working group were found to be statistically significantly higher than those of the working group. A statistically significant difference was found between the overall SSI-F score average, concealment of the illness, and perceived devaluation, according to the degree of proximity of the participants (p < .05). The mean scores of the participants who are spouses, mothers, and fathers were found to be statistically significantly higher than those of children participants. A statistically significant difference was found between the overall SSI-F score average, social withdrawal, concealment of the illness, and perceived devaluation, according to the physical illness condition of the participants (p < .05). The mean scores of the group with physical illness were found to be statistically significantly higher than the group without physical illness. A statistically significant difference was found between the overall SSI-F score average, social withdrawal, and perceived devaluation, according to the support from the family of the participants (p < .05). The mean scores of the participants who did not receive support from the family were found to be statistically significantly higher than those with support from the family. A statistically significant difference was found between the overall SSI-F score and concealment of the illness, according to the participants’ education about schizophrenia (p < .05). The mean score of the group that did not receive education about schizophrenia was found to be statistically significantly higher than the group that received such education.
SSI-F and MSPSS sub-dimensions mean scores of the participants.
Comparison of mean scores of SSI-F and sub-dimensions according to the introductory characteristics of the participants (continued).
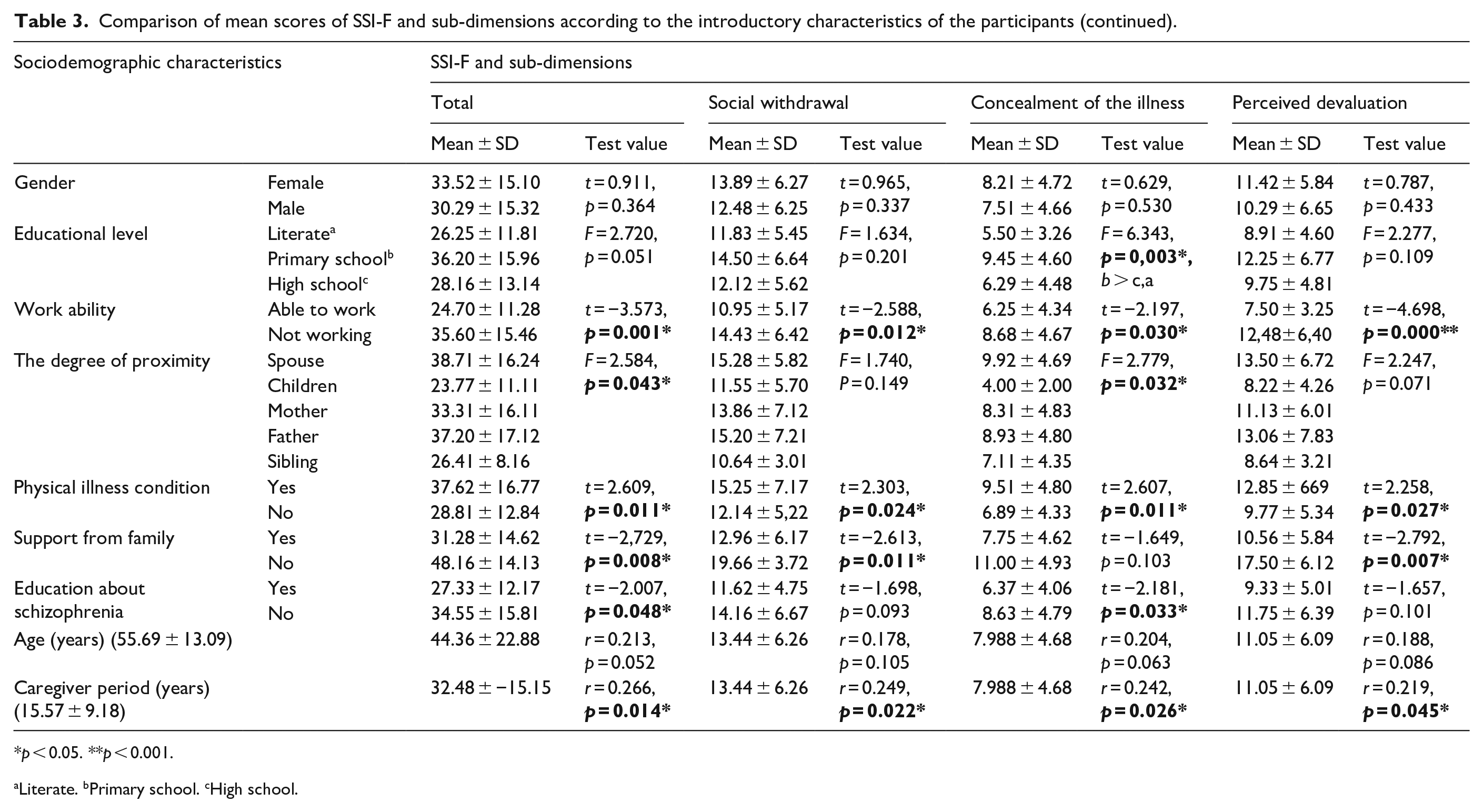
p < 0.05. **p < 0.001.
Literate. bPrimary school. cHigh school.
The mean scores of the MSPSS scale sub-dimensions according to the sociodemographic characteristics of the participants in the study are presented in Table 4. There was no statistically significant difference between the total MSPSS score and the sub-dimensional mean scores according to the caregiver period (years) and support from the family of the participants (p > .05). A statistically weak negative correlation was found between the participants’ mean age and the MSPSS total and sub-dimensional mean scores. A statistically significant difference was found between the mean overall MSPSS scores and sub-dimensions, according to the participants’ educational status, working status, degree of proximity, physical illness condition, and education about schizophrenia (p < .05). A statistically significant difference was found between the mean overall MSPSS scores and sub-dimensions according to the participants’ educational status, employment status, degree of affinity, physical illness, and education about schizophrenia (p < .05). Perceived social support mean scores of working participants were found to be statistically significantly higher than those of non-working participants. The perceived social support score average of the group with a child degree of closeness was found to be statistically significantly higher than the participants who were spouses, mothers, and fathers. The perceived social support score of the participants without physical illness was found to be statistically significantly higher than that of participants with physical illness. The perceived social support scores of the participants who received education about schizophrenia were found to be statistically significantly higher than those of participants who did not receive education about schizophrenia.
Comparison of mean scores of MSPSS and sub-dimensions according to the introductory characteristics of the participants.

p < .05. **p < .001.
Literate. bPrimary school. cHigh school.
The relationship between MSPSS subscale mean scores is shown in Table 5. An intermediate statistically negative correlation was found between the SSI-F scale total and social withdrawal mean scores of the participants, and the overall MSPSS score average, friend, and private person mean scores. A weak negative correlation was found between the SSI-F scale social withdrawal dimension mean scores of the participants and the MSPSS family dimension mean scores. There was a high level of negative correlation between the mean scores of the SSI-F dimension concealment of the illness and the mean MSPSS total score, friend, and private person mean scores, and an intermediate negative relationship to the family mean scores. There was an intermediate statistically negative relationship between the mean scores of the SSI-F dimension perceived devaluation and the MSPSS total and friend mean scores and a statistically weak relationship between the family and private person mean scores.
Relationship between SSI-F and MSPSS sub-dimensions mean scores.
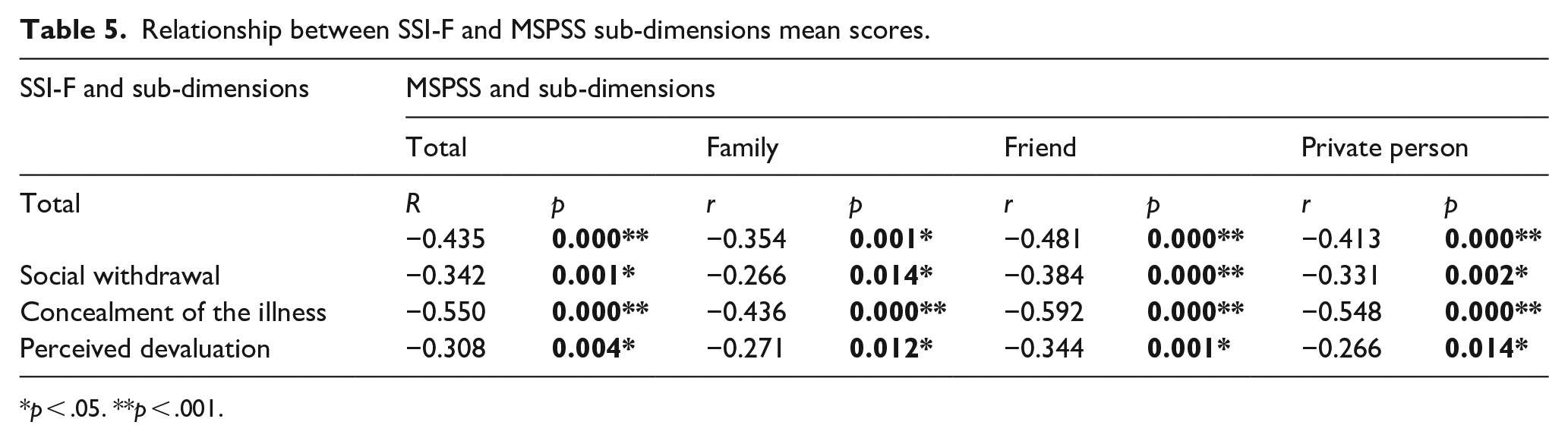
p < .05. **p < .001.
Considering the β coefficient, t value, and significance level of perceived social support (β = .066), it has a statistically significant effect on self-stigma in caregivers of schizophrenic patients (p < .001). In this case, it could be argued that, as the score obtained from perceived social support increases, the score from self-stigma in caregivers of schizophrenic patients will decrease. The results show that 18% of the change in self-stigma in caregivers of schizophrenic patients could be explained by perceived social support (regulated R2 = 0.180) (Table 6).
Regression analysis of SSI-F scale and MSPSS mean scores.

p < .001.
Discussion
In this study, the self-stigmatization score was found to be intermediate in caregivers. In the study conducted by Guan et al. (2020), it was determined that 24% of the caregivers of schizophrenia patients had intermediate self-stigmatization. In a meta-analysis study conducted by Shi et al. (2019), it was reported that self-stigmatization is high among caregivers of schizophrenia patients. In other studies (Allerby et al., 2015; Koschorke et al., 2017; Singh et al., 2016) it was reported that self-stigmatization was high in caregivers of schizophrenia patients. Karamlou and Mottaghipour (2013) that cultural differences can affect the experience of stigmatization in the caregivers of patients with schizophrenia in areas such as traditional social beliefs about patients, limitation in work and education, concealment of the illness, perceived devaluation, and gender differences in their caregivers. Studies performed in Turkey have reported that patients’ family members experience self-stigma (Korkmaz & Küçük, 2016; Yıldız et al., 2012, 2019). In this study, we determined that self-stigmatization was higher in caregivers who did not receive education about schizophrenia. A similar result was reported in a study by Sing et al. (2016). Contrary to this study, some studies (Girma et al., 2014; Hasson-Ohayon et al., 2011) reported more self-stigmatization in caregivers with high levels of knowledge and education about schizophrenia. On the other hand, some studies (Chang et al., 2016; Koschorke et al., 2017) reported that there is no relationship between caregivers’ knowledge level about schizophrenia and self-stigmatization. Improving caregivers’ knowledge about disease and disease management is one of the most important factors in reducing negative perceptions of the disease. For this reason, increasing the knowledge level of caregivers is vital in making positive contributions to the recovery process of the patient with schizophrenia. Self-Stigma inventory for families subscales on social withdrawal were significantly associated with caregiver period, physical illness condition and support from family. In this study the mean scores of social withdrawal was moderate (13.44) level. Previous studies reported the importance of the social withdrawal in the phenomenon of stigmatization (Caqueo-Urízar et al., 2019; Gerlinger et al., 2013). Self-stigmatization of caregivers may lead to unhappiness and despair, perceived devaluation, concealment of the illness, withdrawal from social relations, avoidance of the patient, and lack or delay in seeking treatment (Maiocco et al., 2017; Singh et al., 2016). Self-Stigma inventory for families subscales on concealment of the illness were significantly associated with caregiver period, level of education, work ability, degree of proximity, physical illness condition, and level of education about schizophrenia. Self-stigmatization of caregivers can reduce help-seeking behavior, thus negatively affecting the healing process of schizophrenia patients. Contrary to this finding, some studies (Chang et al., 2016, 2017) reported that the education level and work status of caregivers (Guan et al., 2020a) were not associated with self-stigmatization. This result can be explained by the social and economic restrictions of non-working caregivers, feeling lonely, and having higher self-stigmatization. In this study, caregivers who are spouses, mothers, and fathers had higher self-stigmatization than other caregivers. In a study by Yin et al. (2014), it was reported that children stigmatized themselves less as caregivers. This may be due to young adults knowing more about schizophrenia and seeking help from their social environment more easily. Self-Stigma inventory for families subscales on perceived devaluation of the illness were significantly associated with caregiver period, work ability, physical illness condition and support from family. In a meta-analysis, conducted by Pascoe and Richman (2009) it was stated that the perception of discrimination and devaluation was negatively linked with both mental and physical health and stigma may also increase distress by decreasing the sense of social support. Self-stigma of the caregivers of patient with schizophrenia generally occurs as devaluation, decreased self-esteem, social withdrawal, and concealment of the illness (Bipeta et al., 2020). In a study performed in Turkey it was showed that caregivers of patient with schizophrenia were unwilling to communicate with their close friends, neighbors, or relatives, lower self-esteem, ideas about failure, senses of uselessness, thoughts about feeling unable to be happy, and thoughts about their inability to fulfill their duties were seen as the perceived devaluation of the perceived devaluation of the caregivers (Yıldız et al., 2019). We think that perceived devaluation might be a explain with culture-specific properties.
In this study, it was found that caregivers who do not receive family support stigmatize themselves more. Perceived social support is low in caregivers with a high level of self-stigmatization (Koschorke et al., 2017). Carrying out care without social support can cause stress and ineffective coping. In this study, it was determined that perceived social support in caregivers was at an intermediate level. Similarly, previous studies (Lök & Bademli, 2020; Razali & Hariani, 2015) have reported that perceived social support in caregivers was moderate. Although social support has a positive effect on coping with the difficulties experienced by caregivers of schizophrenia patients, this social support is insufficient (Chen et al., 2016; Chronister et al., 2013). In this study, it was found that the social support of caregivers decreased in those with high ages, low education levels, are non-working, and are not educated about schizophrenia. In some studies (Ribé et al., 2018; Yu et al., 2020), it has been reported that perceived social support increases in caregivers with high levels of education, working, and family support. In a study conducted by Lee et al. (2006), it was reported that social support protects mental health in caregivers of schizophrenia patients and has positive effects on coping with stress and seeking help. Consistent with the findings of previous studies, this study shows that self-stigma among caregivers of patients with schizophrenia was negatively related with social support (Guan et al., 2020a; Korkmaz & Küçük, 2016; Yin et al., 2014). In this case, it could be argued that, as the score for perceived social support increases, the score for self-stigma will decrease. Some studies (Guan et al., 2020a) reported that self-stigmatization is associated with low social support in caregivers of schizophrenia patients. The self-stigmatization of these caregivers has a negative effect on the perception of social support (Korkmaz & Küçük, 2016). Some studies (Chronister et al., 2013; Geffner et al., 2017; Livingston & Boyd, 2010) revealed that social support has a protective function in the development of self-stigmatization. In a study conducted by Guan et al. (2020b), it was reported that internalized stigma significant factors of distress among family caregivers of persons living with schizophrenia. Increasing social support interventions for caregivers of patients with schizophrenia may be effective in dealing with difficulties and stigmatization.
Limitations
Despite the contributions of the current research, there were limitations. The first limitation of the study is its cross-sectional design, so causal inferences cannot be made. If we try to investigate the causal inferences of SSI-F and MSPSS, then a follow-up study, rather than a cross-sectional one, would give more reliable results. A second limitation of the study is its sample size. Regarding the fact that our study was conducted in only one community mental health center, the results cannot be generalized to the entire population. In this study, the relationship between self-stigmatization and perceived social support in caregivers of schizophrenic patients was revealed, but qualitative studies are needed to investigate the causes of self-stigmatization. Depending on self-reported data gathering forms might be another limitation. Further studies should include variables related to the patient with schizophrenia and the caregiver. Third, this study included only caregivers of actively continuing schizophrenia patients in CMHC, so further studies should include larger samples to confirm these results.
Conclusions
In this study, we determined that as the perceived social support for caregivers of patients with schizophrenia decreases, self-stigmatization increases. In psychoeducational intervention programs, it is recommended to provide caregivers with informative support about schizophrenia, to increase hope and social skills training, and to implement interventions that include caregivers in the fight against stigma. We recommended that caregivers should seek professional help when they cannot cope and be encouraged to participate in family-to-family support programs. Interventions to increase the internal resistance to stigmatization in caregivers, support individual development, develop coping skills for self-protection, increase psychological resilience, and increase social skills are recommended.
Footnotes
Acknowledgements
We sincerely appreciate the support of nurse Orhan Al on the study and the hard work of all managers and personnel at the CMHC. We thank all the respected caregivers of patients with schizophrenia for participating in the study.
Authors’ contributions
All authors contributed to the study conception and design. Conceptualization and methodology: Yeliz Karaçar and Kerime Bademli. Material preparation, data collection and analysis were performed by Yeliz Karaçar. The first draft of the manuscript was written by Yeliz Karaçar and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Availability of data and material
The data that support the findings of this study are available from the corresponding author, (Karaçar, Y), upon reasonable request.
Ethics approval
All human studies have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. This study was approved by the Akdeniz University Faculty of Medicine Clinical Research Ethics Committee (Decision No: 451; Date: 27.06.2018) and in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Institutional approval was obtained from the Antalya Provincial Health Directorate and TRSM. Participants who were reached at the center on weekdays from 09:00 to 16:00 on the dates of the study were informed that participation in the study was voluntary and that the research data would only be used for scientific purposes. All research participants received informed written consent including a detailed explanation of the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent to participate
Participants were fully informed provided with key information about the study that they can consider before deciding whether to take part. All research participants received informed written consent including a detailed explanation of the study.
Consent for publication
Participants who were reached at the center on weekdays from 09:00 to 16:00 on the dates of the study were informed that participation in the study was voluntary and that the research data would only be used for scientific purposes. All research participants received informed written consent including a detailed explanation of the study.