
Abstract
Background:
Since the 21st century, humans have experienced five public health emergencies: the severe acute respiratory syndrome (SARS), type A H1N1 influenza (H1N1), Middle East respiratory syndrome (MERS), Ebola virus disease (EVD), and the new coronavirus pneumonia (COVID-19). They caused a large number of casualties and a wider psychological crisis, which might cause severe consequences such as post-traumatic stress disorder and suicide.
Aims:
To reveal the law of formation of public psychological crisis in public health emergencies, and draw lessons from it. To provide ideas for effectively deal with these psychological crisis problems and fundamentally curbing the occurrence of public health emergencies.
Method:
Through the method of literature research, ‘public health incidents’, ‘psychological crisis’, ‘mental health’, ‘psychological intervention’, ‘SARS’, ‘H1N1’, ‘MERS’, ‘EVD’, and ‘COVID-19’ were used to search literatures in the databases such as PubMed, Springer, and Sciencedirect, and the literatures were summarized, sorted, and studied.
Results:
(1) The public health emergencies caused a universal psychological crisis. The main manifestations were depression, compulsion, despair, etc. The people involved mainly include patients, suspected isolated patients, medical staff, and the general public in the epidemic situation. (2) People’s psychological state often experienced stress stage, shock stage, acceptance, and reorganization. Only some susceptible individuals couldn’t complete effective psychological reconstruction, resulting in serious psychological disorders. Individual susceptibility is related to genetic factors, adversity, and traumatic stimuli experienced in early life.
Conclusion:
To reduce these psychological crisis problems, we should establish and improve the psychological crisis intervention or rescue system of public health emergencies, it was still necessary to live in harmony with nature, get rid of the inappropriate habit of preying on wild animals, in order to prevent the cross-species transmission of the virus between wild animals and humans, and to fundamentally avoid the occurrence of major infectious diseases.
Introduction
In recent years, the frequency of public health emergencies around the worldwide has been on the rise. Only in the first 20 years of the 21st century, humans have experienced five public health emergencies caused by major infectious disease, they were the severe acute respiratory syndrome (SARS) in 2003, type A H1N1 influenza (H1N1) in 2009, Middle East respiratory syndrome (MERS) in 2012, Ebola virus disease (EVD) in 2014, and the new coronavirus pneumonia (COVID-19) at the end of 2019. Public health emergencies not only caused a large number of property losses and casualties, but also caused a series of psychological crisis. How can public health emergencies occur so frequently? Will humans encounter similar public health incidents in the future? How to deal with it effectively? These issues are worthy of our consideration. This paper summarized the psychological crisis in these five public health incidents from the perspective of psychiatry, and obtained three important enlightenments, in order to provide help to curb the occurrence of public health emergencies, or to reduce impact of public health emergencies on people’s mental health as much as possible.
Materials and methods
Data sources and retrieval strategies
The English literatures published between January 2000 and July 2020 were retrieved in databases such as Pubmed, Springer, and Sciencedirect using ‘public health incidents’, ‘psychological crisis’, ‘Mental health’, ‘Psychological intervention’, ‘Social psychology’, ‘SARS’, ‘H1N1’, ‘MERS’, ‘EVD’, and ‘COVID-19’ as the keywords. The literature retrieval formula was as follows: (‘public health incidents’ or ‘SARS’ or ‘H1N1’ or ‘Middle East respiratory syndrome’ or ‘Ebola virus disease’ or ‘COVID-19’) and (‘psychological crisis’ or ‘Mental health’ or ‘Social Psychology’ or ‘Psychological intervention’).
Literature inclusion criteria
Inclusion criteria: (1) Research on the psychological crisis, mental health, and psychological intervention of patients, medical staff or the general public in public health incidents; (2) Research on the psychological crisis, mental health, and psychological intervention of persons involved in post-disaster incidents (such as wars, earthquakes, terrorist attacks, etc.); (3) The viewpoint and topic of literature were novel, and the full text could be consulted.
Exclusion criteria: (1) The literatures that were published or detected repeatedly; (2) The literatures lack of access to the full text; (3) The literature lack of scientific research methods.
Literature selection and quality assessment
After the authors of the paper completed the retrieval of all the literatures and excluded duplicate literatures, two members of the research group who had been engaged in general psychology and social psychology for a long time conducted a second selection and cross-examination of the titles and abstracts of all literatures, and comprehensively evaluated the quality of the literatures. Finally, by reading the full text, the literatures that met the requirements were selected strictly according to the inclusion and exclusion criteria. The controversial literatures were discussed by the members of the research group to decide whether to include them.
Results
Results of literature inclusion
After preliminary retrieval, 1,057 English literatures were obtained. By excluding duplicate literatures and reading titles and abstracts, 219 literatures were selected. Through reading the full text, 119 articles were finally included. The literature retrieval processes, inclusion and exclusion were shown in Figure 1.

Literature retrieval process.
Psychological crisis in public health emergencies
The psychological crisis in the SARS
The severe acute respiratory syndrome (SARS), which broke out in Guangdong Province in 2003, spread to many countries and regions around the world, causing at least 8,096 infections and 774 deaths (World Health Organization, 2004). It was not only a serious public health incident, but also a serious psychological stress for everyone. The SARS had a serious impact on the mental health of the general public, patients, and related medical staff.
Impact on the psychological health of the general public
Post-hoc studies has shown that the impact of the SARS on the public’s mental health far outweighed its physical impact. Statistics showed that the number of infected persons during the SARS epidemic was only 1/10,000 or 2/10,000, but those with panic and other psychological problems caused by the SARS might reach one tenth or two-tenths at the peak. The common psychological problems of the public mainly included hypochondria, compulsive psychology, fear and anxiety, etc. A survey of 1,083 middle school students from China found that middle school students had psychological disorders such as depression, fear, compulsive anxiety, hypochondria, and neurasthenia during the SARS. The mental health level of the Chinese public was worse than that before the SARS. According to a survey of the elderly in Hong Kong community, the suicide rate of the elderly in Hong Kong dropped from 40 per 100,000 in 1986 to around 29 to 31 per 100,000 in 2002, but increased to more than 40 per 100,000 during the SARS epidemic in 2003. The reasons for the increase of suicide rate in the elderly might be related to social isolation, the increase of mental stress and anxiety during the SARS epidemic (Yip et al., 2010). The World Health Organization believed that suicide and mental illness were the main public health problems during the SARS epidemic.
Impact on the psychological health of the SARS patients
In addition to paying attention to the mental health of the general public, the impact of the SARS epidemic on the psychological state of patients was also the focus of social attention. Reports showed that the SARS patients, in addition to medical treatment, had to undergo strict hospital isolation. They worried about the deterioration of their condition and whether they had transmitted the virus to their relatives and friends. Therefore, the SARS patients bore tremendous mental pressure while facing with death threats, their psychological health was worrying (Cheng & Wong, 2005). A survey study of 669 SARS patients showed that many SARS patients suffer from psychological crisis such as extreme anxiety, panic, depression, and despair during the epidemic due to forced isolation, away from family, and friendship support and other factors, they urgently needed psychological support and help (Li et al., 2006). Another study found that the SARS patients still suffer from serious psychological health in a short period of time, even after being cured, mainly manifested as pain, anxiety, depression and other psychological symptoms (Cheng et al., 2004). Studies also found that life quality of the SARS survivors was still lower than that of uninfected people of the same age, even in the first year after being cured (Hui et al., 2005). Many survivors and their caregivers were often discriminated against by neighbors and employers, marginalized and excluded in the workplace, schools, and other social groups (Lee et al., 2005). According to a survey from Hong Kong, 16.2% of the public believed that the SARS patients might still spread the virus to others even after 18 months of being cured, another 16.6% of the public involuntarily avoided contact with the SARS patients (Lau et al., 2006). It could be considered that the stigmatization of the SARS survivors seriously delayed the psychological recovery of these survivors in the later stages of the epidemic, and was one of the important factors leading to the psychological crisis and low life quality of the SARS survivors.
Impact on the psychological health of medical staff
During the SARS epidemic, the majority of medical staff had always been in the first line of fighting against the epidemic, becoming a high-risk group of infection (Wenzel & Edmond, 2003). During the SARS epidemic, the infection rate of Chinese medical staff was 18.38%. Medical staff accounted for 57% of all SARS patients diagnosed in Canada (Booth et al., 2003). At the beginning of the outbreak, due to the lack of understanding of the nature, harm, transmission mode of the SARS virus, as well as the lack of diagnostic criteria and treatment measures, medical staff also experienced uncertainty, fear of being infected, and possible infection to their families in addition to psychological pressure at work (Maunder et al., 2003), these factors could become stressors and lead to physical and psychological discomfort (Lazarus, 1993). A survey study involving 1,257 medical staff from Taiwan, China showed that, in the initial stage of the SARS outbreak, when the infection spread rapidly, health-care professionals generally had feeling of extreme vulnerability, uncertainty, and life threat, and exhibited physical and cognitive symptoms of anxiety (Chong et al., 2004). Research from Singapore also showed that the mood and spirit of medical staff were severely affected during the SARS epidemic, doctors had a higher risk of post-traumatic stress disorder (PTSD) than nurses, and single medical staff had a higher risk of PTSD than married workers (Chan & Huak, 2004). The results suggested that medical institutions should pay attention to the psychological health of medical staff while treating patients during the epidemic, and it was necessary to provide them with basic social psychological support and intervention.
The psychological crisis in the H1N1
The H1N1 influenza that broke out in Mexico and the United States in March 2009 also spread to 214 countries and regions around the world with 1.3 million people infected and more than 18,000 people died (World Health Organization, 2009). The impact of H1N1 influenza on global public psychological health was still serious (Chan et al., 2009). Pfefferbaum et al. (2012) believed that the H1N1 was a serious public psychological and behavioral health crisis. A survey from Greece showed that more than half of the medical staff at a tertiary hospital in Greece felt moderate or even high levels of anxiety and psychological distress during the H1N1 pandemic in 2009 (Goulia et al., 2010). A number of surveys in China also found that both quarantined and non-quarantined college students had different degrees of depression, hypochondria, fear, neurasthenia, compulsion, anxiety, and other psychological stress problems during the H1N1 epidemic. Similar problems were found in the psychological health of medical staff. In short, the H1N1 had a significant impact on medical staff and public psychological health, and the impact was related to the extent of the epidemic, the residents in the area seriously affected by the epidemic might be more vulnerable and have more serious psychological crisis.
Psychological crisis in the MERS
The Middle East Respiratory Syndrome (MERS) that broke out in Saudi Arabia in 2012 caused 1,401 infections and 543 deaths worldwide (World Health Organization, 2018). The psychological impact of the MERS on patients, the general public and medical staff should not be ignored. A randomized crossover experiment from Korea showed that the MERS seriously affected the psychological health of patients, and the assessment of depression risk factors could determine whether mental care was needed during hospital isolation (Kim et al., 2018). Jeong et al. (2016) investigated 1,656 general persons quarantined after contacting with MERS patients and found that 7.6% of the respondents still had obvious anxiety, even if they were not infected, and the proportion of respondents with anger was as high as 16.6%. About 4 to 6 months after the quarantine was lifted, the proportion of the above two psychological states decreased to 3.0% and 6.4% respectively. A cross-sectional survey of 358 ordinary persons from Saudi Arabia showed that 57.7% of the respondents still had a moderate anxiety even in the absence of the MERS virus infection (AlNajjar et al., 2017). Another report from South Korea showed that stigmatization caused medical staff to bear different degrees of psychological pressure and severe stress psychology during the MERS epidemic (Park et al., 2018). Recently, Usher et al. (2020) analyzed 11 research papers from 8 countries (including 32,049 subjects), and the results showed that whether the current global epidemic of COVID-19 or the MERS and H1N1 could cause psychological symptoms such as anxiety, mental distress, PTSD, and anger among general public and medical staff.
Psychological crisis in EVD
As early as 1976, there occurred cases of hemorrhagic fever in southern Sudan and northern Zaire (now the Democratic Republic of Congo), and caused deaths (Feldmann & Geisbert, 2011), but it did not attract the attention of the international community at that time. In 2014, Ebola hemorrhagic fever caused by Ebola virus once again hit many countries in West Africa including Guinea, Liberia, and Sierra Leone, at the same year, the WHO declared Ebola virus disease (EVD) was ‘public health emergency of international concern’ (PHEIC) (World Health Organization, 2014). During the period 2014 to 2016, the EVD epidemic caused 11,310 deaths in West Africa alone, with mortality rate as high as 50% to 90% (World Health Organization, 2016). A large number of studies showed that EVD survivors, people affected by EVD, medical staff and epidemic prevention personnel participated in the rescue had different degrees of physical and mental health problems (Betancourt et al., 2016; Wilson et al., 2018). During the EVD outbreak, fear-related behaviors had a severe pathological effect on public psychology at all stages after epidemic, increasing the suffering and mental symptoms, and thereby increasing indirect mortality due to causes other than Ebola (Shultz et al., 2016).
The survey data showed that 27.5% to 83.3% of the people affected by EVD still had obvious anxiety symptoms (Howlett et al., 2018; Waterman et al., 2018), and 12% to 75% were diagnosed with depression (Kamara et al., 2017; Lehmann et al., 2015; Wilson et al., 2018). Several other studies showed that symptoms such as post-traumatic stress disorder (PTSD), obsessive-compulsive disorder (OCD), psychological distress, sleep disorder, suicidal ideation, drug abuse, and social anxiety were very common among people exposed to the EVD epidemic (Cénat et al., 2020; Ji et al., 2017). A meta-analysis study also showed that EVD was associated with depression, anxiety, PTSD, obsessive-compulsive disorder, and other adverse psychological symptoms (Cénat et al., 2020). Green et al. (2018) made a survey on 201 Liberian children’s parents before and after EVD epidemic in 2014, and the results showed that parents exposed to EVD-related diseases or deaths preferred to impose harsh disciplinary requirements on their children, and EVD exposure could also increase family conflicts and parents’ anxiety. Cénat et al. (2019) believed that EVD had multiple adverse effects on the mental health of survivors, relevant families, communities and workers fighting the epidemic, and emphasized the important role of psychological work in fighting the EVD epidemic. In short, the EVD epidemic was also a serious psychosocial stress incident, especially the high mortality caused by Ebola virus might be the source of anxiety and pain of EVD survivors and medical staff (Mohammed et al., 2015), and the serious physiological symptoms were also related to the production of bad psychology (Etard et al., 2017). The patients infected with Ebola virus had fever, headache, muscle pain, weakness, fatigue, diarrhea, vomiting, abdominal pain, unexplained bleeding, and other physical symptoms (Epstein et al., 2015), which might also be the cause of adverse psychology.
The psychological crisis in the COVID-19 epidemic
The COVID-19, which broke out in Wuhan, Hebei, China at the end of 2019, was considered to be the most widespread, infected and harmful public health emergency since the new century. By September 9, 2020, a total of 27,486,900 cases had been diagnosed worldwide (World Health Organization, 2020), with 894,900 deaths and a mortality of 7.07%, the severity of the COVID-19 far exceeded H1N1 and SARS (Anjum et al., 2020). The COVID-19 had a profound impact on all fields of social life, and it also caused a series of psychological and mental health problems. WHO once pointed out ‘At present, the main psychological impact of the epidemic is to increase the incidence of psychological stress and anxiety’.
The impact of the COVID-19 on the psychological health of the general public
In the early stage of the COVID-19, the lack of understanding the virus’ nature, transmission and latent period, the lack of effective prevention and treatment measures, strict social isolation, and ‘closing the city’, ‘closing the country’ and so on all affected seriously people’s normal life and psychological health (Cascella et al., 2020; Peeri et al., 2020). Reports indicated that, as of March 25, 2020, schools and educational institutions in 150 countries had been closed worldwide, directly affecting more than 80% of students in the world. Some countries had closed schools in local areas (Bedford et al., 2020). Large-scale social blockade could easily cause people to have adverse emotions such as boredom, irritability, and disappointment (Brooks et al., 2020; Li et al., 2020), as well as feelings of isolation, helplessness, and abandonment. Furthermore, the adverse impact of the COVID-19 on the global economy and society, as well as the false or bad information spread in society during the epidemic further exacerbated feelings of insecurity and anger (Ornell et al., 2020; Wang et al., 2019). A survey of 2091 general public showed that, 1 month after the COVID-19 outbreak, the morbidity rate of PTSD among residents in mainland was 4.6%, and the proportion was as high as 18.4% in high-risk areas (Wuhan). Similar results were also reported by Torales et al. (2020). Two weeks after the COVID-19 broke out, Liang et al. (2020) made a cross-sectional survey on the psychological health of 584 Chinese adolescent, and the results showed that nearly 40.4% of adolescent were prone to psychological problems, and 14.4% of them had PTSD symptoms. An online psychological health survey of 2,458 ordinary American also showed that, compared with that before the COVID-19 epidemic, the level of public psychological health after epidemic was generally lower (Sønderskov et al., 2020). Research by Japanese scholars also found that the COVID-19 could cause a wide range of public psychological health problems, including painful reactions (insomnia, anger, extreme fear of disease), health risk behaviors (increased use of tobacco and alcohol, social isolation), psychological health disorders (PTSD, anxiety, depression, somatization), and reduced health level (Shigemura et al., 2020). A survey of college students in the United States showed that 71% of 195 students surveyed said that the COVID-19 increased personal stress and anxiety (Son et al., 2020). Tan et al. (2020) investigated the immediate psychological state of 673 employees who returned to work during the COVID-19 epidemic and found that 10.8% of them met the diagnostic criteria for PTSD. For patients who suffered from related diseases before the epidemic, the original diseases were worsened during the COVID-19 epidemic. For example, a survey of 32 patients with eating disorders showed that 38% of them further aggravated during the COVID-19 epidemic, and 56.2% of them increased additional anxiety (Fernández-Aranda et al., 2020). Another study also showed that 20.9% of patients with mental disorders were worse during the COVID-19 epidemic (Zhou et al., 2020). Even for some patients with common flu, the stress, and fear due to similar illnesses could cause mental distress, and further worsen the original mental symptoms (Park & Park, 2020). It was also reported that the clergy members were not able to be physically present with the patients in their final moments, or the bereavements could not say goodbye to their loved ones due to the limitation of the funeral during the COVID-19, which aggravated the grief, guilt, and pain of the patients and bereavements (Burrell & Selman, 2020; Corpuz, 2021). In addition, stigma and xenophobia also increased the psychological burden on the public. Stigmatized groups and individuals were often ostracized, avoided, criticized, isolated, physically abused, and even discriminated against in employment, residence, education, and health services (Xiang et al., 2020).
The impact of the COVID-19 on the psychological health of patients and suspected patients
Studies showed that the mental impact of the COVID-19 on patients was very serious although the ratio of diagnosed and suspected cases were relatively low, most cases were asymptomatic or mildly infected and the mortality rate was relatively low (Epidemiology Working Group for NCIP Epidemic Response, Chinese Center for Disease Control and Prevention [EWG], 2020). In addition to suffering from illness and isolation, patients diagnosed and suspected of the COVID-19 would also have extreme fear of the consequences of infection, which led to serious psychological problems (Xiang et al., 2020). The common psychological problems were loneliness, boring, anxiety, denial, insomnia, despair, fear, anger, depression, and so on (Brooks et al., 2020). After some suspected patients were quarantined, concerned about their own health or suspicion of infection, as well as the uncertainty of whether they would die or had transmitted the virus to families and friends and so on could all lead to irritability, panic, anxiety (Maunder et al., 2003), and even OCD, such as hand washing over and over again, repeated disinfection, taking temperature frequently, or adhering to near-critical precautions. Zhang et al. (2020) investigated the psychological health of 57 COVID-19 patients and 50 quarantined persons and found that the proportion of patients with depression was 29.2% and that of quarantined persons was 9.8%, the former was significantly higher than the latter (p = .016), but there was no significant change in anxiety between the two groups. Bo et al. (2020) investigated the psychological health of 714 hospitalized and stable COVID-19 patients and found that 96.2% of them had posttraumatic stress symptoms (PTSS). There were also studies suggested that the COVID-19 could cause further psychological trauma to patients and medical staff, and even cause delusions and suicidal behavioral psychology (Pereira-Sanchez et al., 2020). Therefore, in addition to giving necessary medical treatment to COVID-19 patients and suspected persons, it was also necessary to actively adopt psychological methods to intervene and treat their psychological trauma in time.
The impact of COVID-19 on the psychological health of medical staff
The COVID-19 epidemic was a major test for the global public health system, especially in the early stage of the epidemic. Due to the sharp increase in infected and suspected cases as well as the relative shortage of medical resources, medical staff often needed to undertake high workloads in the face of infection. They wore protective clothing and worked in a relatively closed environment. Many inconveniences in life and heavy work pressure could easily cause fear, fatigue, sleep problems and emotional disorders (Kang et al., 2020). Zhang et al. (2020) found that, compared with non-medical staff, the proportion of medical staff suffering from insomnia, anxiety, depression, somatization, and OCD increased significantly after the COVID-19 broke out, and the most common risk factors were living in rural areas, women, and contact with COVID-19 patients. Chen et al. (2020) and Mao et al. (2020) also showed that the proportion of medical staff suffering from depression increased after the COVID-19 broke out. In the early stage of the COVID-19 epidemic (January 29, 2020 to February 3, 2020), Lai et al. (2020) made a survey-based cross-sectional and regional stratified study on the psychological health of 1,257 medical staff in 34 hospitals in China, the proportions of depression, anxiety, insomnia, and pain were 50.4%, 44.6%, 34.0%, and 71.5%. Studies in Greece also showed that (Tsamakis et al., 2020), due to limited medical resources and patients’ unwillingness to cooperate or comply with safety instructions and so on, medical care professionals were often faced with tremendous psychological pressure and the incidence of mental illness was high. In addition, Tsamakis et al. (2020), Stelnicki et al. (2020), and Tan et al. (2020) made surveys on the psychological state of medical staff in Brazil, Canada, and Singapore, and also obtained the similar findings. In addition, due to restrictions of funerals during the COVID-19 epidemic, the bereavements were often unable to attend the funerals rites (Cardoso et al., 2020), medical staff must work farewells to the dead, and comfort the family members to prevent excessive grief, which virtually increased their work and mental burden (Araujo Hernández et al., 2021). It could be considered that if these psychological health problems were not alleviated in time, it would not only affect the attention, understanding, and decision-making ability of medical staff, but also reduce their quality of life and ultimately reduce their ability to overcome the COVID-19 epidemic. Therefore, the psychological health of medical staff should also get social attention.
The state of psychological crisis in five public health emergencies was shown in Table 1.
Schedule of five major public health emergencies in the new century and their impact on psychological health.

The global spread scope of the five public health emergencies was shown in Figure 2.
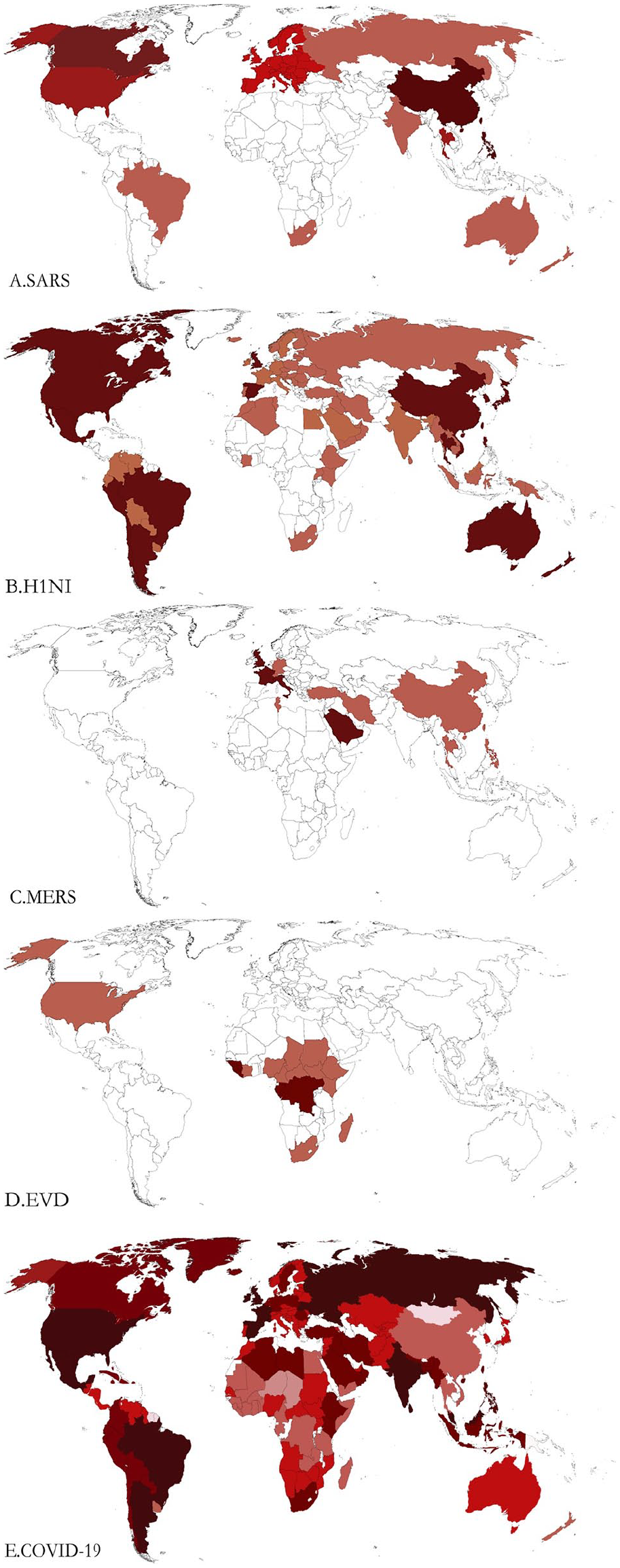
The global spread scope of SARS, H1N1, MERS, EVD, and COVID-19.
Analysis on the law of social psychological crisis in public health incidents
Looking back at these five major infectious diseases epidemics since the new century, we found that they were not only serious public health incidents, but also serious social and psychological stress incidents. Under this powerful stressor, most people could quickly adjust their emotional psychology, recover from anxiety, fear, numbness, and panic, and quickly adapt to this stress stimulus. But some people suffered from bad psychological states such as pain, anxiety and fear for a long time, and even suffered from PTSD and depression, which could also lead to suicidal behavior in severe cases. Why did the same kind of stressor make such a big difference in different individuals? This needed to explore the law of human psychological changes under stress. Under normal circumstances, people’s psychological state would roughly undergo three stages: stress stage, shock stage, acceptance, and reorganization. During the stress stage, people would experience numbness, fear, doubts, and other emotional psychology. Acute stress disorder (ASD) referred to an acute psychological disorder that occurred within 2 days to 4 weeks after the occurrence of a stress incident, which was characterized by general symptoms such as anxiety, anger, and increased anxiety-alertness, was a common psychological feature in the stress stage. During the shock stage, the person concerned seemed to understand something after going through a certain psychological process, but he did not accept everything lost, and often showed the psychological and behavioral characteristics of denial, compulsion, avoidance, loneliness, and so on. During the stage of acceptance and reorganization, most people could accept reality, return to life, complete psychological reconstruction, and their psychological crisis problems could also heal themselves. However, some individuals were unable to complete psychological reconstruction, resulting in serious psychological crisis problems such as PTSD and depression. It should be emphasized that under the same stress incident, there was no obvious time limit and distinction point between the three psychological stages of individual performance. The greater the threat and uncertainty that some individuals felt about the incident, and the higher the perceived risk, the more serious the degree of psychological crisis, and the longer each stage lasted. There was a problem of vulnerability. Some highly susceptible individuals would have strong negative emotional responses even in the face of neutral or mild stress stimulation, and these emotional responses would last for a long time. If they were faced with strong catastrophic stress stimulation, they often had serious psychological crisis and negative emotional responses. Without effective psychological intervention, they would not be able to complete effective psychological reconstruction. Individuals with weaker susceptibility could effectively cope with strong stress stimulation, their psychological stress response was weak, the duration was short, and the self-healing was fast. Therefore, depending on the level of stress and individual susceptibility, there was a continuum of mental health changes between adverse emotional reactions and severe psychological disorders. In this continuum, as individual susceptibility increased, the level of stress stimulation required to induce psychological crisis gradually decreased (Figure 3) (Dean & Keshavan, 2017).
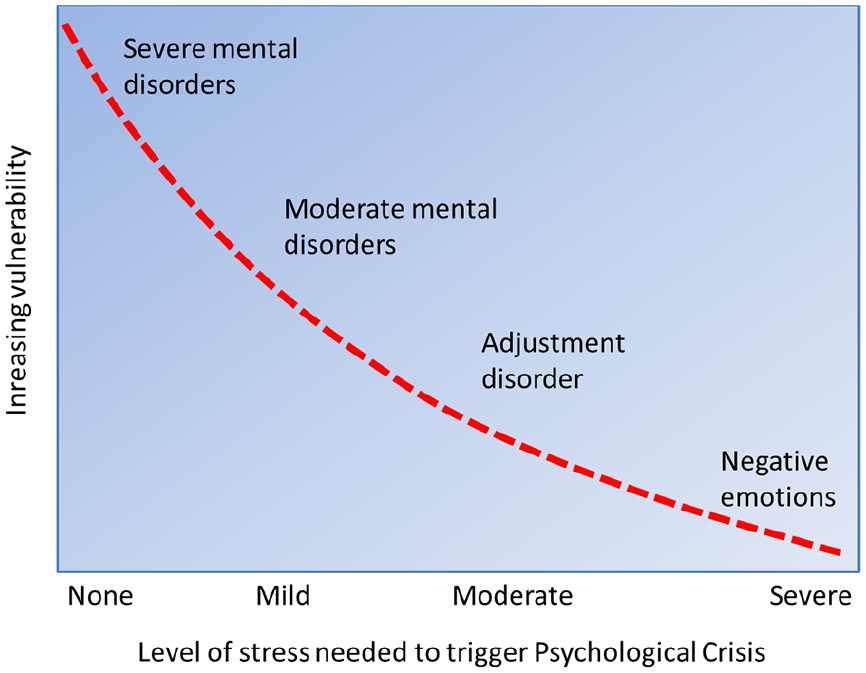
Stress-susceptibility model of psychological crisis.
Neurobiological findings also supported differences in susceptibility among different individuals. For example, individuals with smaller hippocampus were at greater risk for depression than individuals with normal hippocampal volume (Booij et al., 2015). The hippocampus was one of the important brain areas in the emotion regulation loop. Brain-derived neurotrophic factor (BDNF) played an important role in neurogenesis, survival, and neuroplasticity, the interaction between BDNF gene polymorphism and early stress incidents could increase the risk of late depression (Carver et al., 2011), the abnormal expression of serotonin 2A receptor gene (HTR2A) (Zhao et al., 2014), and tryptophan hydroxylase 2 gene (TPH2) (Haghighi et al., 2008) could also increase the risk of depression. In addition, lower birth weight was also a risk factor for depression in adults (Gale & Martyn, 2004). In addition, studies have found that childhood abuse, loss of parents, malnutrition, and discordant family environments could increase the risk of bad mood in adulthood (Nanni et al., 2012; Pechtel & Pizzagalli, 2011). In short, the above-mentioned risk factors could increase the susceptibility of individuals to various psychological crisis, which often produced excessive emotional responses to stress incidents. Even objectively mild stressors could cause them to produce serious psychological crisis. However, whether these factors were the determinants of psychological crisis of some people in these five public health incidents remained to be further studied.
Important enlightenment
To establish a long-term rescue system for the psychological crisis of major infectious diseases from a macro perspective
Looking back at these five public health emergencies since the beginning of the new century, we could find that both the EVD epidemic, which had a high mortality rate and the SARS and COVID-19 epidemic, which were high infectious, had a relatively limited impact on human physiology, because there were very few infected people. However, the impact of epidemic on the public psychology was more common, and what was important was that the impact of epidemic on public psychology was often not given due attention by the government. In addition, developing countries such as India and Pakistan lacked practical psychological support and intervention systems due to limited resource. In the face of sudden and major public health emergencies, being able to control the epidemic, detect, and cure the infected people became the greatest success. As for the relief of public psychology, there was no time to take into account (Anjum et al., 2020). Even if the developed countries such as the United States and Australia had advanced medical standards and complete psychological assistance system, they were also very vulnerable in the face of the sudden COVID-19 epidemic. Controlling the epidemic and treating the infected patients were still the first priority, and the psychological treatment of patients was often inadequate. The Chinese government departments attached great importance to the psychological crisis in public health emergencies. As early as January 26, 2020 and March 18, 2020, two important documents, ‘Guiding Principle for the Intervention of Emergent Psychological Crisis in New Coronavirus Infected Pneumonia Epidemics’ and ‘Work Plan for Psychological Counseling of New Coronavirus pneumonia Epidemics’ were issued respectively, aiming to comprehensively strengthen and scientifically guide the psychological crisis intervention and psychological counseling related to the COVID-19 epidemic in various localities. However, there were still some practical problems such as insufficient attention of individual local government, weak strength of psychological health work team and inadequate implementation of psychological rescue work and so on, and the effect was not ideal. Facing the current situation of normalized prevention and control of the COVID-19 epidemic, and the new major infectious disease epidemic caused by an unknown virus that humans might face in the future, it was urgent to establish a long-term rescue system for the psychological crisis of major infectious disease epidemics at the national level. The specific measures should include: (1) When dealing with major public health emergencies, the experts engaged in public psychological health should be included into the policy decision-making group and their opinions and suggestions should be actively adopted; (2) Establish a complete public psychological health intervention or rescue system, which could draw lessons from the measures of some developed countries. For example, the disaster psychological health service network in the United States played an important role in the incident on Sept. 11, which was a reference for countries with relatively weak public psychological health intervention or rescue systems; (3) Train and reserve public psychological health workers. The relative shortage of professional psychological health workers was a common problem in all countries, especially in developing countries, which required intensifying the training of talents in peacetime and encouraging more professionals to engage in public psychological health work; (4) Use big data to screen susceptible populations, focus on family members with frustrations, single-parent families, and divorced parents in their early years and give them more social care and support in peacetime to improve their adaptability and psychological resilience to stress stimulation; (5) Targeted interventions should be carried out for groups with psychological crisis in public health incidents, and their psychological health states should be continuously tracked and detected. Smart disease surveillance systems could be used to monitor and evaluate the psychological state of patients in real time and provide targeted intervention countermeasures; (6) On the basis of ensuring information transparency, government departments should strengthen the management and control of bad information on network media, block the bad information that might cause social panic in time, and open psychological rescue hotline, response to hot issues of social concern in time, to ensure open channels for information exchange between the public and the government.
To explore the social psychological intervention methods which are operable, universal, and individualized from the micro level
Since the new century, with the increase in the frequency of major infectious diseases, the social psychological crisis during the epidemic had also aroused the widespread concern. However, there still existed practical problems such as insufficient methods of psychological crisis intervention, lack of operability, and pertinence in reality. According to the published literatures, there were many studies on psychosocial investigations during the epidemic period, while studies on psychosocial intervention countermeasures were very rare. Cognitive behavior therapy (CBT) was the sum of a series of intervention methods, which had a good intervention effect on anxiety, depression, and other psychological health problems and mental diseases (Bonilla-Escobar et al., 2018). However, during the epidemic, especially under the condition of social blockade, how to effectively use CBT requires further research. Critical incident stress debriefing (CISD) was also a common psychological crisis intervention, which could speed up the process of individual psychological rehabilitation in disaster (Mitchell et al., 2003), but there had been no reports of applications in public health emergencies. Yoga and breathing regulation exercise also had a good effect on alleviating insomnia, anxiety, depression and other bad behaviors and psychological crisis during the COVID-19 epidemic (Lai et al., 2020). However, the application in practice was very limited at present. Sports was also considered to be one of the effective ways to promote psychological health, and it had a good intervention effect on depression, anxiety, and other bad emotions (Matta Mello Portugal et al., 2013), whose role in social psychological reconstruction and rehabilitation after disasters such as earthquakes had been confirmed. Recent studies have shown that there was a positive correlation between physical activity and psychological health during the COVID-19 epidemic (Jacob et al., 2020). However, for different psychological problems such as anxiety, depression and PTSD, what kind of exercise and exercise intensity should be used for intervention? Was the same exercise effective for different psychological problems? Where was the window period for exercise to intervene social psychological crisis? These specific problems needed more empirical research to be solved from the micro level.
Stopping the occurrence of major infectious diseases was the best way to avoid public psychological crisis
Since the new century, human beings have experienced five public health emergencies caused by major infectious diseases. Why did the epidemics occur so frequently? Where did these viruses come from? With the progress of virus traceability, these problems were gradually revealed. After sequencing the Tor2 isolate of SARS-CoV, Marra et al. (2003) in Canada found that it was moderately associated with other known coronaviruses (including OC43 and 229 E). The results showed that the SARS-CoV was not recombined from known coronaviruses, but from animal viruses of unknown hosts. After sequencing the genetic sequence of the new coronavirus (2019-nCoV), it was also found that the homology between it and the bat coronavirus RaTG13 was as high as 96.2% (Fernández-Aranda et al., 2020). The results suggested that 2019-nCoV might come from wild animals in nature. Although the natural and intermediate hosts of 2019-nCoV had not yet been finalized, it was an indisputable fact that the cross-species transmission of 2019-nCoV from wild animals to humans eventually caused a full-scale outbreak of COVID-19. This was very similar to the early spread of HIV in humans. Therefore, to avoid the occurrence of public psychological crisis, the best way was to fundamentally block the virus cross-species transmission between wildlife and human beings, and finally to curb the occurrence of major infectious diseases. There had long been a vague balance between nature and human beings, but in the past century, as the global population continues to increase, the destruction of nature by humans was also increasing. The environment was polluted, natural forests were extensively destroyed or occupied by humans, and the balance between nature and humans was disrupted. In particular, the habitats of some wild animals continued to decrease, causing them to be forced into the living space of humans, which increased the risk of transmitting the virus to humans. In addition, people in certain areas still had the habit of preying on wild animals (Peeri et al., 2020). Some wild animals that had not been quarantined (snakes, bats, civet cats, gorillas, etc.) were likely to be the natural hosts of a certain virus. Eating these wild animals was bound to expose humans to the risk of direct infection. Therefore, to protect the natural environment, to eliminate the inappropriate habits of eating wild animals and to live in harmony with nature might be the fundamental way for people to avoid the recurrence of the epidemic and ultimately avoid psychological crisis.
Conclusion and prospect
Since the new century, human beings have experienced five major epidemics of infectious diseases caused by viruses. By sorting out these five major epidemics, it was not difficult to find that the natural hosts of these viruses came from wild animals. The cross-species transmission of the virus between wild animals and humans was the common cause of these five major epidemics, leading to a large number of casualties and severe public psychological crisis was the common result. Of course, it was undeniable that public health events had a positive impact on human behavior and psychology. For example, after the outbreak of COVID-19 epidemic, large-scale social isolation allowed people to have more leisure time, family members could enjoy the warm time of reunion in the family, scientific researchers could have sufficient time to sort out research materials, and professional staff’s work and social intercourse also decreased accordingly. A recent study reported that the COVID-19 epidemic could cause people to produce two cognitive model of post-traumatic symptoms (PTS) and post-traumatic growth (PTG) (Vazquez et al., 2021). PTG could enhance people’s primal beliefs about the beautiful world, as well as openness to the future and identification with humanity. Another study at the national level also showed that the COVID-19 pandemic led to higher levels of psychological well-being and high identification with all humanity predicts resilience (Valiente et al., 2021). However, these positive effects were insignificant compared with the general psychological crisis in public health events. Mankind should draw useful lessons from these five major epidemics to prevent the recurrence of similar infectious epidemic in the future. Looking forward to the future, we believed that to reduce the psychological crisis in public health emergencies, in addition to establishing and improving the psychological crisis intervention or rescue system of public health emergencies, and enriching the professionals of public psychological health, it was also necessary for all countries to work together and unite to eliminate the virus, overcome the epidemic and minimize the harm caused by the epidemic. But fundamentally speaking, it was still necessary for humans to live in harmony with nature, get rid of the inappropriate habit of preying on wild animals, in order to prevent the cross-species transmission of the virus between wild animals and humans, and to avoid the occurrence of zoonotic diseases.
Of course, as an important manifestation of disastrous stress events, major public health emergencies were often sudden and unpredictable, which required the general public to master some of the most basic psychological rescue or psychological intervention methods. Under normal circumstances, it was necessary to take primordial, primary, and secondary interventions according to different stages of people’s psychological changes in disastrous stress events. For example, after just experiencing a disaster event, people’s psychology was still in stress stage, at this time, we should focus on primordial intervention, pay attention to the changes of patients’ emotional state and behavior details, and give them careful care to prevent the occurrence of harmful events such as suicide and self-harm; In the stage of psychological shock, after a certain psychological process, the parties seem to understood something, but did not accept everything lost. At this time, we should focus on primary psychological intervention, pay attention to listening to patients, help them understand the facts and let them vent their unhealthy emotions, and establish a good personal relationship with them to build their confidence in life; In the stage of acceptance and reorganization, we should focus on secondary psychological intervention, provide necessary psychological counseling and mental health education for patients, or select some specific and targeted treatment measures according to the different actual conditions of patients to help them regain self-awareness and return to normal life as soon possible.