
Abstract
Background:
Suicidal behavior remains a pressing problem in the United Kingdom. Continued theory development is a critical step toward designing effective prevention.
Aims:
The present study tested a novel element to suicide theory, the Desire for Control, for its direct and moderating roles within the Integrated Motivational-Volitional (IMV) Model of Suicidal Behavior.
Method:
An online-administered cross-sectional suicide risk survey study (n = 116) was conducted among adults living in the United Kingdom.
Results:
Mean suicidal ideation scores were in the non-clinical range. DOC Leadership and Destiny Control were associated with good mental health. DOC Decision Avoidance was associated with poor mental health. DOC Decision Avoidance also acted as a motivational moderator in which the entrapment-suicidal thinking link was worse among those high in decisional avoidance.
Conclusion:
DOC represents a novel, valuable addition to suicide theory and may inform suicide-specific psychotherapeutic intervention. Additional research is needed to full understand the role of DOC and its factor structures in the IMV.
According to the World Health Organization (WHO, 2019), one person dies from suicide every 40 seconds. Suicide is recognized as a global phenomenon, taking about 800,000 lives yearly. Moreover, there has been an increase in suicide deaths in the United Kingdom. Suicide deaths in the United Kingdom rose by 11.8% during 2018 (Office for National Statistics [ONS], 2019). Scotland has the highest prevalence of suicide in Great Britain, at a rate of 16.1 deaths per 100,000 persons in 2018 (ONS, 2019). In addition to injury or death from suicide, many people, such as friends and family members, are affected by knowing someone who dies by suicide (Centers for Disease Control and Prevention [CDC], 2020). Contrary to myths about suicide being a distinctly clinical or mental health issue, multiple factors put one at risk for suicidal behavior such as loss (e.g. relationship, job), personal history (e.g. family history of suicide), and stress (CDC, 2019; Cramer & Kapusta, 2017). In this way, suicide and its prevention are a problem requiring study among not only clinical, but also general population samples as well. Examining the factors unique to a geographic that put individuals at risk of suicide will help create effective prevention strategies (CDC, 2020). One way to do so is through examination of emerging models of suicidal behavior.
The integrated motivational-volitional model of suicidal behavior
Founded by Scottish scholars, the Integrated Motivational-Volitional (IMV; O’Connor, 2011; O’Connor & Kirtley, 2018) Model of Suicidal Behavior is a theoretical model gaining traction in the United Kingdom and beyond. The IMV model provides a detailed map of the suicidal mind (e.g. Branley-Bell et al., 2019) by including three phases that explain the background factors (e.g. stress; pre-motivational phase) that may lead one to suicidal behavior through a chain of defeat to entrapment to suicidal thoughts. The model also includes stage-specific moderators, which as a result may facilitate or hinder progression to the next phase. The threat-to-self moderators (e.g. ruminative processes, coping) are composed of cognitive factors that might worsen the defeat-entrapment path. Second, the motivational moderators (e.g. thwarted belongingness, burdensomeness) influence emergence of suicidal thoughts from entrapment. Lastly, the volitional moderators (e.g. exposure to suicidal behavior, impulsivity) include factors that impact transition of ideation to suicidal action.
Previous research has used the IMV model to understand suicide in the United Kingdom and other western samples. For example, defeat mediated the connection between negative social comparisons and entrapment, and resilience moderated the relationship when defeat was high (Wetherall et al., 2019). Entrapment also mediated the connection between suicidal ideation and defeat, while resilience moderated the relationship when entrapment was high. Additional studies support the defeat-entrapment pathway. Defeat contributes to feelings of entrapment, and entrapment is able to mediate the relationship between defeat and suicidal ideation (Taylor et al., 2010; Wetherall et al., 2019). Moreover, the link between insomnia and suicidal ideation was mediated by defeat and entrapment (Russell et al., 2018). Support exists for cognitive moderators as well. For instance, thwarted belongingness and perceived burdensomeness significantly moderated the relationship between entrapment and suicidal ideation (Lucht et al., 2020). The moderation effect remained substantial for both external and internal entrapment. Additionally, persons were more likely to experience higher feelings of entrapment if they had great levels of both defeat and brooding (Tucker et al., 2016); a brooding ruminative style strengthened the relationship between defeat and entrapment. The IMV model, therefore, offers a useful framework in which to apply novel cognitively-focused individual differences to understand suicide. One such trait that has not been assessed as a moderator is Desire for Control (DOC).
Desire for control as a moderator within the IMV
DOC represents the degree to which people are driven to control the events in their lives (Burger, 1985). People with a high DOC are characterized by enjoying leadership, being independent and action-oriented. Most DOC work to date stems from a single-factor conceptualization (Burger & Cooper, 1979). The Desirability of Control Scale (DOCS; Burger & Cooper, 1979) is a 20-item inventory assessing DOC. Individuals with a high DOC have higher expectancies for accomplishments and display higher levels of aspiration than the low DOC individuals. Overall, having a high DOC can aid performance, but liabilities are also present. Problems may arise when one believes they have minimal control, but sustains an immense desire to control over the events in their lives. More recent literature depicts nuance in DOC, as it includes three subscales: leadership, decision avoidance, and destiny control (Thomas et al., 2011). DOC leadership is the desire that individuals have to influence others while in leadership roles. DOC decision avoidance is when an individual has a desire to avoid making decisions or favors a lack of choices. Lastly, desire for destiny control refers to the extent of control one wishes to have over their long-term goals and life outcomes.
Modest evidence suggests DOC is linked to metrics of mental health and well-being, suggesting it may be an avenue worth exploring within a suicide framework. For instance, high DOC can increase proneness to depression and learned helplessness under circumstantially limited actual/perceived control, and that individuals are generally more susceptible to depression when control expectations are incongruous with reality (Burger, 1984; Burger & Arkin, 1980). On the other hand, a more recent study demonstrated that a low DOC was associated with depression when perceived control was high (Amoura et al., 2014). Further, total DOC moderates the relationship between technological coupling and mental health, such that those with higher DOC experienced worse mental health while completing the task of technological coupling (Dvash & Mannheim, 2001). Complicating the picture, a higher total DOC is also associated with health-promoting behaviors and attitudes (Lawler et al., 1990; Pointer-Smith et al., 1988). Also, a high DOC is associated with more adaptive coping and problem-solving, whereas low DOC has been linked to avoidant coping strategies (Gebhardt & Brosschot, 2002; Watanabe et al., 2002). The varied way in which DOC functions with health outcomes may depend on alignment with intentions or interest. Ramsey and Etcheverry (2013) found that both low and high DOC individuals performed better on tasks that matched their preference, highlighting the positive impact of this alignment regardless of the level of desired control. Agreement between DOC and reality, therefore, appears to be of critical importance to its psychological impact, with likely implications for suicide.
Importantly, no studies have made use of the multi-dimensional DOC conceptualization, nor examined DOC with the IMV or suicide. The present study does so in a pilot investigation of adults residing in the United Kingdom. Applying the DOC subscales, individuals with a low desire for destiny control may end up desiring suicide since they believed they are not in control of life events. The only study that could be located examining a suicide-relevant outcome was a longitudinal study conducted to gather narrative accounts of patients’ motivations for engaging in Physician-Assisted Dying (PAD) (Pearlman et al., 2005). Desire for PAD was closely related to a long-standing sense of independence and desire to maintain control over future events (i.e. destiny control). Patients with a high DOC also felt a sense of defeat due to experiencing physical changes such as feeling weak and tired because of their illness. In terms of the DOC subscales, the patient’s intense longing for destiny control may motivate them to pursue PAD. Moreover, the theme of defeat suggests a potential connection to the IMV. Decisional avoidance, due to corollary factors such as an external locus of control, may be associated with defeat, entrapment, and suicidal thinking; yet, at the stage of ideation transitioning to a suicidal act, it may actually be the case that low decisional avoidance (i.e. a decisive person) tends to be associated with a suicide attempt.
The present study
The IMV model (O’Connor, 2011; O’Connor & Kirtley, 2018) can test a characteristic as stage-specific moderators of suicide. DOC is a trait that has been linked to depression and a variety of other health-related outcomes (e.g. Amoura et al., 2014; Burger, 1984). Some evidence suggests DOC may be associated with IMV constructs (e.g. Pearlman et al., 2005). Given existing evidence supporting a number of cognitive threat-to-self and motivational moderators (e.g. Lucht et al., 2020; Tucker et al., 2016), we examined DOC, a novel cognitively-oriented individual difference, as a moderator within the IMV model. All three subscales were used to test the following hypotheses:
Hypothesis 1: A high DOC will serve as a threat-to-self moderator that exacerbates the connection from defeat to entrapment.
Hypothesis 2: A high DOC will serve as a motivational moderator that worsens the link from feeling entrapped to suicidal ideation.
Method
Participants
Table 1 contain demographic information and scale internal consistencies for this sample. The sample was majority White, heterosexual, female, and in their late 20s. Over half of the participants were currently employed full time, while a minimal amount were employed as part time.
Sample demographic and individual difference information.
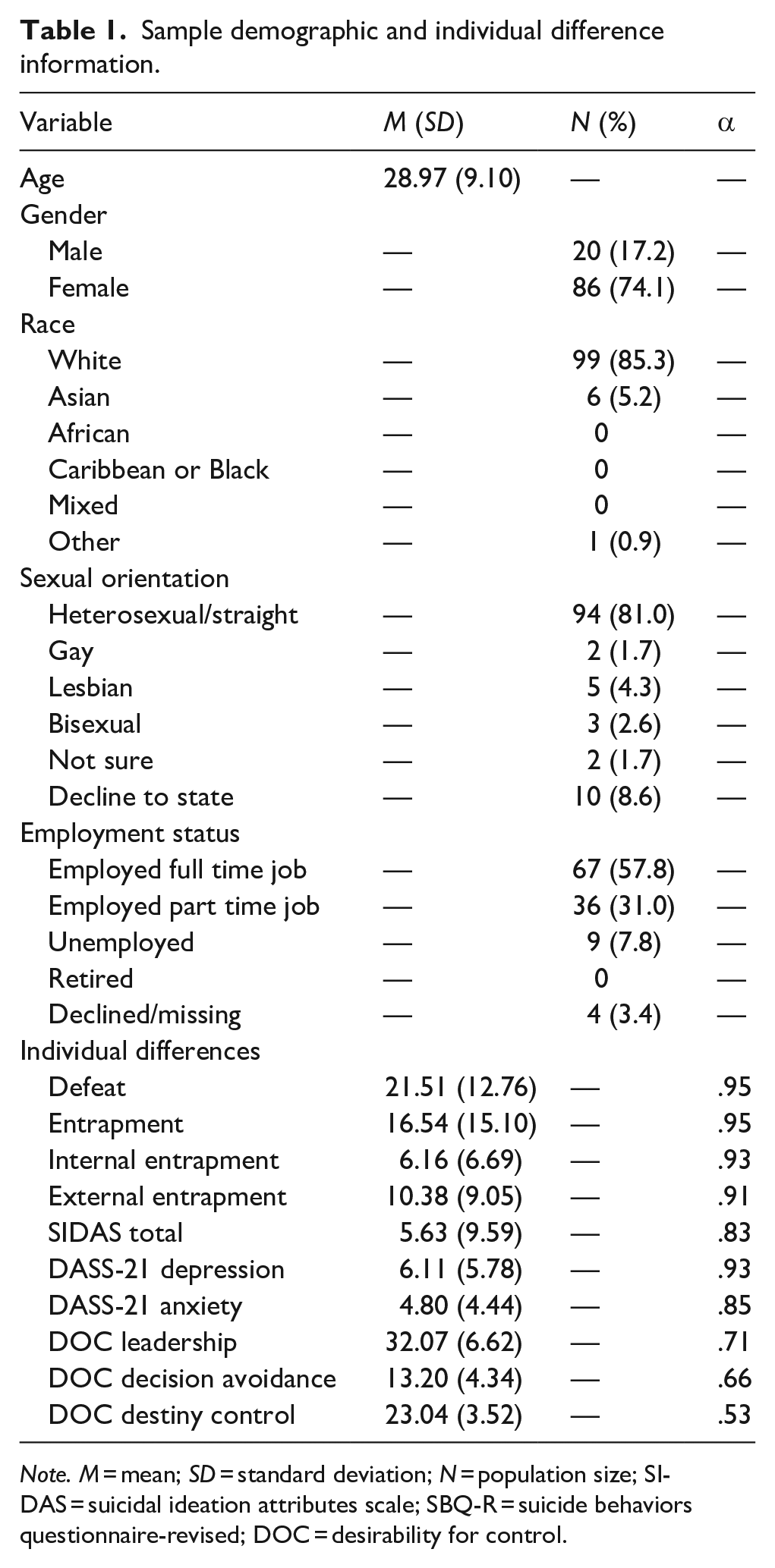
Note. M = mean; SD = standard deviation; N = population size; SIDAS = suicidal ideation attributes scale; SBQ-R = suicide behaviors questionnaire-revised; DOC = desirability for control.
Measures
Demographics
Participants completed a form requesting demographic information including age, gender, race, employment status, and sexual orientation.
Desirability of control
The Desirability of Control Scale (DOCS) is a 20-item Likert-scale assessing the level of desire individuals have for influencing their actions, environments, and life events (Burger & Cooper, 1979). The scale consists of a series of questions with responses ranging from 1 (‘does not apply to me at all’) to 7 (‘Always applies to me’). Higher scores representing an elevated DOC. The DOC total score has an internal consistency of 0.80 and test-retest reliability of 0.75 (Burger & Cooper, 1979). Subscale internal consistency varies: DOC Leadership (seven items; α = .76), DOC Decision Avoidance (four items; α = .62), and DOC Destiny Control (four items, α = .71) (Thomas et al., 2011).
Defeat and entrapment
The Defeat Scale (Gilbert & Allen, 1998) consists of 16 items and asks participants to describe how individuals have felt about themselves over the last 7 days. Each statement is rated on a scale, ranging from 0 (‘Never’) to 4 (‘Always’). The Defeat Scale has an internal consistency of 0.96 and a test-retest reliability of 0.88 (Gilbert & Allen, 1998).
The Entrapment Scale (Gilbert & Allen, 1998) consists of 16 items that requires participants to score the degree to which they believe a statement represents them ranging from 0 (‘Not like me at all’) to 4 (‘Extremely like me’). High scores on the scale represent a higher level of entrapment. The Entrapment Scale possessed an internal consistency of 0.96 and a test-retest reliability of 0.90 (Griffiths et al., 2014). The scale also examines two subscales of entrapment: external entrapment and internal entrapment. External entrapment (α = .93) is the perception of entrapment one holds due to external situations such as financial strain or interpersonal problems (Cramer et al., 2019). Internal entrapment (α = .95) refers to a perception of entrapment one holds due to internal factors such as feelings and thoughts.
Suicidal ideation
The Suicidal Ideation Attributes Scale (SIDAS; Van Spijker et al., 2014) is a Likert-style scale that consists of five items. The SIDAS assesses the presence and characteristics (e.g. controllability) of suicidal ideation. The response for each question includes a scale that ranges from 0 to 10, with varying descriptors for end points of each scale. The internal consistency of SIDAS is high (α = .91).
Psychological distress
The Depression Anxiety and Stress Scale-21 (DASS-21; Osman et al., 2012) is a 21-item scale that will be used to measure psychological distress. Each item on the scale is scored from 0 (‘Did not apply to me at all’) to 3 (‘Applied to me very much or most of the time’) (Osman et al., 2012). The DASS-21 also yields three subscales (seven items each): depression (α = .91–.97), anxiety (α = .81–.92), and general distress (α = .88–.95) (Gloster et al., 2008). Depression and anxiety subscales were used as covariates in the present study.
Procedure
The research was approved by the University of Strathclyde Ethics Committee. Adults residing in Scotland were recruited through a survey advertised via poster displays and social media sites such as Facebook and Twitter. This cross-sectional study was administered through an online Qualtrics survey. Before participants started the survey, they were presented with the Participant Information Sheet and then the Consent Form. If the participant agreed to continue to take the survey, they would then be directed to the questionnaire. The questionnaire took approximately 30 minutes to complete. At the end of the survey participants received a debriefing form containing the contact information of the research team, study information, and mental health support resource information.
Data analysis
The maximum level of missing data on any item of interest was 9.4%. Multiple imputation was employed to handle missing data (Enders, 2017). Bivariate correlations were run prior to hypothesis testing in order to assess DOC subscale associations with IMV and psychological distress factors. Each hypothesis was tested using linear regression. The H1 model included: (1) main effects of defeat and three DOC subscales; (2) two-way interaction term between defeat and each DOC subscale; and (3) covariates of depression and anxiety. The H2 model included: (1) main effects of entrapment and three DOC subscales; (2) two-way interaction term between entrapment and each DOC subscale; and (3) covariates of depression and anxiety. Where significant interactions emerged they were graphed and tested using simple slopes (Bauer & Curran, 2005).
Results
Bivariate correlations
Table 2 contains bivariate correlations; DOC Leadership and Destiny Control were significantly and negatively associated with defeat and entrapment, while DOC Decision Avoidance was significantly and positively associated with defeat and entrapment. DOC Destiny Control was significantly and negatively related to suicidal ideation. As for mental health, DOC Leadership was significantly and negatively associated with depression. DOC Destiny Control was significantly and negatively associated with depression and anxiety. DOC Decision Avoidance, on the other hand, was significantly and positively related with depression and anxiety.
Bivariate correlations.

Note. Bold font denotes p < .001; bold italicized font p < .05.
Hypothesis testing: DOC within the IMV
Table 3 contains regression model statistics for examination of hypothesis 1. The overall model was significant and accounted for large variance in entrapment. However, hypothesis 1 was unsupported. Defeat, DOC Decision Avoidance, and Depression were all significant and negatively associated with entrapment. 1
Hypothesis one linear regression model predicting entrapment.

Note. DOC = desire for control; × = multiplicative for interaction term; F(9, 106) = 49.80, p < .001; Adj. R2 = 0.79.
Table 4 contains regression model statistics for examination of hypothesis 2. The overall model was significant and accounted for large variance in suicidal ideation. DOC Decision Avoidance and Depression were both significant and negatively related with suicidal ideation. Partially supporting hypothesis 2, the entrapment by DOC Decision Avoidance interaction was significant. Figure 1 depicts the interaction. Simple slopes analyses showed that the association between entrapment and suicidal ideation remained significant and positive only at very high (two standard deviations above the mean) levels of DOC Decision Avoidance, t(112) = 2.25, p = .02. 2
Hypothesis two linear regression model predicting suicidal ideation.
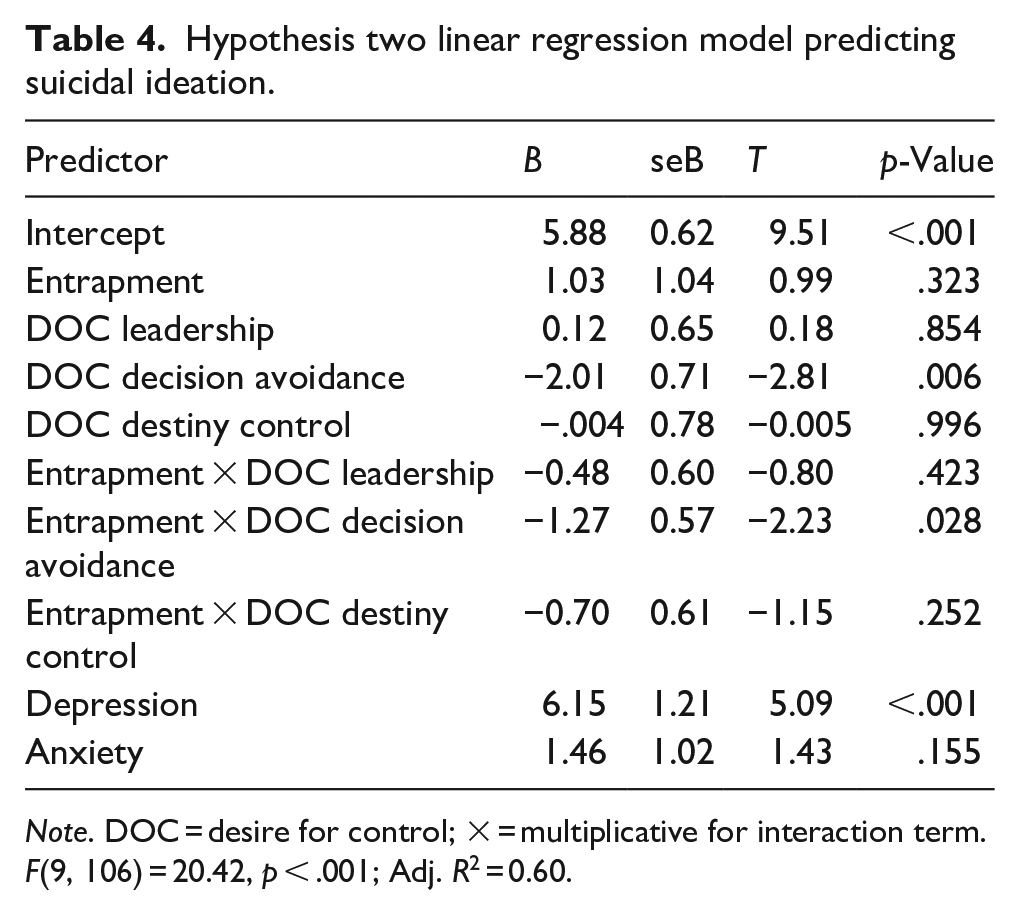
Note. DOC = desire for control; × = multiplicative for interaction term. F(9, 106) = 20.42, p < .001; Adj. R2 = 0.60.

Desire for control as a motivational moderator in the integrated motivational-volitional model.
Discussion
The penultimate purpose of the present study was to investigate the three DOC subscales as moderators within the IMV (O’Connor, 2011; O’Connor & Kirtley, 2018). DOC Leadership and Destiny Control did not influence transition points we tested in the IMV model. Regression model results did uncover a role of DOC Decision Avoidance as a motivational moderator. Supporting hypothesis 2, the entrapment-suicidal ideation association remained significant for those at very high levels of Decision Avoidance. Decision Avoidance as a moderator is novel to the IMV, shedding light under which conditions entrapment may be particularly problematic. Importantly, individuals who avoid making decisions tend to experience greater stress and poor well-being (Bavolar & Orosová, 2015). Further, anxiety has been linked to avoidance behaviors (Pittig et al., 2015), and the preference or act to avoid decision-making may be one such difficulty (Thomas et al., 2011). In the context of the IMV, the combination of high Decision Avoidance and its corollary difficulties may result in a situation where feelings of entrapment appear insurmountable. On the other hand, people with low Decision Avoidance, or decisive individuals, may be more likely to act upon their feelings instead of staying in a stagnant state of entrapment, which may lead to other actions as opposed to contemplating suicide (i.e. ideation).
DOC Decision Avoidance and depression were also direct risk factors for entrapment and suicidal ideation, respectively. The role of depression in understanding both entrapment and suicidal ideation is to be expected. The independent role of Decision Avoidance in regression models builds on prior DOC literature suggesting the DOC total score may impact mental health under varying conditions (e.g. Amoura et al., 2014; Burger, 1984). Decisional avoidance may manifest as becoming trapped in one’s own thoughts (internal entrapment). Moreover, Decision Avoidance may make one more dependent on others to make decisions, especially in the context of feeling depressed (Pilowsky, 1979). Such over reliance on others could worsen feelings of external entrapment. Additional novel DOC findings were bivariate patterns in which DOC Leadership and Destiny Control were associated with healthier levels of defeat and entrapment, and DOC Destiny control related to lower suicidal thinking. Desires to engage in leadership and possess control over your future are worthy targets of future research as they may precede or be impacted by positive processes such as leadership training and personal and professional successes. Such pursuits, when exercised well, may help reduce entrapment, defeat, and suicidal thinking.
The present study possesses several important implications for the study and prevention of suicide. The IMV model (O’Connor, 2011; O’Connor & Kirtley, 2018) is quickly becoming an international lens through which suicide is being studied and intervention work is being developed (e.g. De Beurs et al., 2020; Cramer et al., 2019; Tucker et al., 2016). While the primary defeat-entrapment-suicidal behavior pathway is fairly well-supported, much more work is needed to identify threat-to-self and motivational moderators. The present study identified Decisional Avoidance as one such motivational moderator. Moreover, an understudied aspect of the IMV is the pre-motivational phase. Present bivariate findings point to DOC Leadership and Destiny Control are possible avenues of further inquiry as background factors in the IMV. The present study also did not test volitional moderation, or DOC as a factor influence suicidal ideation to behavior. Future prospective research should include such assessment of DOC within the IMV.
Moderation findings hold clinical implications for suicide intervention. Mental health service providers may need to attend specifically to decisional avoidance where feelings of entrapment are observed in working with persons experiencing suicidal thinking. Depending on the nature of one’s unique presentation of entrapment and Decision Avoidance, the preference to avoid decisions may become a specific target of treatment through suicide-specific intervention (e.g. Collaborative Assessment and Management of Suicide; CAMS, Jobes, 2012) or general psychotherapeutic techniques like cognitive-behavioral therapy.
The present study possesses several limitations. The sample possessed restricted demographic diversity. Any conclusions regarding the role of DOC within the IMV model should be interpreted with caution. Next steps in sampling DOC-IMV research can include examination of vulnerable populations such as sexual and gender minority, immigrant, or youth samples. Additionally, to assess DOC’s clinical relevance, the construct can be integrated into clinical studies of suicide in hospitalized settings. Two primary methodological limitations were the cross-sectional online survey procedure and the low internal consistency of DOC subscales. These issues may be intertwined, as responses to the DOC scale may suffer when administered online. The DOC scale factor structure may also need to be examined; indeed, there is very little factor analytic work on the DOC scale to date. A next logical stage in this line of research would be to conduct a large-scale, multi-administration method DOC scale study to investigate the robustness and measurement variance of its single- and three-factor structures.