
Abstract
Objectives:
Hikikomori – an almost complete withdrawal from social interaction first seen in Japan – is becoming an emerging psychological syndrome worldwide. The mental health community in Japan has focused on hikikomori since the 1990s. Hikikomori was initially considered a culture-bound trait, unique to Japan; however, it has become an international concern, and cases have been reported even outside of Japan. While home visiting support for people with hikikomori has gained popularity, an effective solution remains elusive. This paper describes the process involved in effective home visiting support provided by experienced workers to help people with hikikomori.
Method:
Semi-structured interviews were conducted with 21 home-visiting support workers in Japan. Collected data were analysed using a constant comparative method based on Grounded Theory.
Results:
‘Supporting them in finding their own way to participate in society’ was identified as the core category. This core category was substantiated by following three interrelated stages: preparing the involved surroundings for reaching out to a person, maintaining constant communication and expanding the range of activities and relationships. The process encouraged people with hikikomori to enhance their social connections and improved their motivation for social participation. People with hikikomori experiencing despair and isolation began to find pleasure in social participation through the three stages of support provided by home-visiting workers.
Conclusion:
Our study suggests that Home visiting support for people with hikikomori can be enhanced by these three interrelated methods which can help individuals integrate into society and connect with others.
Introduction
A globally emerging psychiatric syndrome among youth, hikikomori, is characterised by an almost complete withdrawal from social interaction. It has received considerable attention from the Japanese mental health community since the 1990s. In 2010, the Japanese Ministry of Health, Labour and Welfare (2010) defined hikikomori as a psycho-sociological phenomenon characterised by withdrawal from social activities and being largely homebound for more than half a year. A community-based survey revealed hikikomori affects approximately 1.2% of the Japanese population (Koyama et al., 2010). Reports estimate the number of hikikomori cases among 15- to 39-year-old and 40- to 69-year-old people is 563,000 and 613,000, respectively, in Japan (Japan Cabinet office, 2016, 2019).
While hikikomori was considered a uniquely Japanese culture-bound trait, it has become an international concern; cases have been reported in several countries and every inhabited continent (Roza et al., 2020; Stip et al., 2016; Teo et al., 2015). One study reported hikikomori’s prevalence as 1.9% among people aged 12–29 years in Hong Kong (Wong et al., 2015). Furthermore, in three metropolitan cities in China, a cross-sectional open web report indicated that 6.6% of the population between the age of 10 and 39 years were classified as withdrawn and asocial for more than 3 months (Liu et al., 2018). Bowker et al. (2019) reported the self-reported prevalence of past hikikomori experiences among university students from Singapore, Nigeria and the United States to be 20.9%, 9.5% and 2.7%, respectively. Self-report survey results from Wu et al. (2020) identified hikikomori in Taiwan, and 9% of the valid responses indicated social withdrawal for at least 6 months.
Hikikomori is comorbid with various psychiatric conditions, including depression, social anxiety and suicidal behaviours (Kubo et al., 2020). Furthermore, Kato et al. (2020) suggested that the emergence of the internet is an important contributing factor in the occurrence of hikikomori. Hikikomori prevalence is higher among adolescents with internet gaming disorders (Stavropoulos et al., 2019) and heavy internet and media device use, which is also linked to obesity, distraction, addiction and cyberbullying (Bozzola et al., 2019). Japanese college and university students who have longer internet usage times and higher scores on internet and smartphone addiction scales are also at high risk for hikikomori (Tateno, Teo, Ukai et al., 2019). Among patients with major depressive disorder, social withdrawal may have subtle associations with clinical symptoms, social connection and personality traits (Teo et al., 2020). Additionally, people with hikikomori were more likely to have suicidal risk factors than people without hikikomori in a wide population study in Japan (Yong & Nomura, 2019).
We believe that even people with hikikomori with no comorbid psychiatric disorders require professional support, as they exhibit psychosocial maladjustment symptoms that hinder them from having a normal social life. Wong et al. (2019) reported that East Asian countries provide various interventions to address hikikomori, including internet addiction programs, pharmacotherapy, home visits and therapies involving psychodynamics, art, animal assistance and family participation. Japan has facilitated hikikomori-specific primary consultation services in each prefecture and 12 major cities, and an educational program based on ‘Mental Health First Aid’ and ‘Community Reinforcement and Family Training (CRAFT)’ for family members has been shown to improve behaviours and social participation in people with this disorder (Kubo et al., 2020). Meanwhile, interventions encouraging people with hikikomori to access treatments are also necessary, although Imai et al. (2020) reported that hikikomori corresponds with low clinic attendance. Malagón-Amor et al. (2015) emphasised the need for specialised domiciliary teams to detect and treat hikikomori, since affected individuals referred for treatment at the Crisis Resolution Home in Spain had serious symptoms, were socially impaired and were uncollaborative in treatment.
Previous studies have suggested that the home visiting approach is effective. Lee et al. (2013) reported several behavioural changes following visitation programs utilising a structured manual in Korea. These included increased outdoor activities, engaging more in family conversations, improved interpersonal contact, spending more time outside, increased participation in group activities, returning to school, acquiring part-time jobs and significant improvements in participants’ average GAF scores. Similarly, a study by Yuen et al. (2019) conducted in Hong Kong showed significant improvement in participants’ social, psychological and physical health. Furthermore, nearly half of the participants recovered from hikikomori by returning to the workforce after social workers provided social counselling and life planning in regular visits. In Japan, Shinohe et al. (2014) reported changes in the family’s attitudes or the hikikomori status after 2 months of home visit support.
While home visiting services for people with hikikomori have gained popularity worldwide, there are no specific details regarding how to provide home-visit support for hikikomori. Clarifying the support workers’ experiences, including their philosophy and intentions, may offer ways to resolve treatment difficulties and provide better practise, as suggested in a previous study about home-visiting services for people with mental disorders (Arriola-Vigo et al., 2019; Tanaka et al., 2018). Therefore, this paper reports the process of home visiting support for people with hikikomori by experienced and effective workers.
Method
A qualitative methodology based on the grounded theory approach (Strauss & Corbin, 1999) was considered most appropriate for describing home visiting support details, which is a developmental and interactive process between support workers and people with hikikomori.
Participants
The participants were home visiting workers who had over 2 years of experience working with people with hikikomori and are considered experts in their respective fields. We actively approached these experts once they were referred to us. We intentionally selected our study participants across various socio-demographic characteristics according to theoretical sampling. In accordance with the sampling technique of grounded theory, participants were selected based on an emerging core category and a conceptual framework. Saturation was reached after 21 interviews.
Data collection
We conducted face-to-face, in-depth, semi-structured interviews which were audio-taped and later transcribed in full. The interviews lasted between 27 and 190 minutes (M = 108.8 minutes, SD = 36.4). The interviews focused on the clinical episodes of services for people with hikikomori. The interview guide included their experiences with effective interventions, factors contributing to success, evaluations of outcomes and demographic data. The focus of the interviews and the topics to be pursued in subsequent interviews were identified. In accordance with theoretical sampling, after each interview, we intentionally selected participants across various socio-demographic characteristics for further interviewing.
Ethical considerations
The research protocol was approved by the ethics committee of the university. All participants were informed verbally and in writing about the purpose and methods of the study. Participants were assured that neither they nor their places of work would be identified. They were also informed that participation in the study was voluntary and that they could withdraw at any time. Written consent was obtained.
Data analysis
Data collection and analysis occurred simultaneously in a constant comparative manner (Strauss & Corbin, 1999). The transcripts were coded line-by-line using the workers’ actual words to analyse and describe the process of home visiting services for people with hikikomori. Codes were continually compared to identify similarities and differences, and similar codes were integrated. Categories were produced, and characteristics of concepts were identified by repeating the classification and the integration of codes.
The interviews were conducted until no new categories were identified. The relationships among the categories were examined by subsuming and abstracting categories, and the conceptual framework was modelled contingent on the process of effective interventions leading to an outcome and other related factors. The successive memos were created for initial category development and theoretical abstraction and synthesised the constant comparative analysis. Diagramming, including creating concept maps and matrices, helped define and refine the relationships between categories.
Rigour
Credibility and dependability were established using the following methods: (i) member checks: two study participants reviewed all emergent concepts and subcategories, and categories were deemed to be accurate representations of their experiences; (ii) theory triangulation (Denzin, 1978): we conducted interviews among three people who experienced hikikomori and recovered through home visiting services, and referred to their comments on the analysis; and (iii) peer debriefing: we discussed the interpretation of the data until consensus was reached.
All interviews and analyses were conducted in Japanese. For this report, interview data were translated into English. To ensure accurate translation, the translated text was proofread several times by native English speakers.
Results
Our study participants were 21 home visiting workers with 2 to 25 years of experience working with people with hikikomori. Participants comprised 13 men and 7 women, and their ages ranged from 31 to 75 years (M = 50.1, SD = 13.2). The sample included seven certified social workers or psychiatric social workers, three psychologists, a public health nurse and an advanced practice nurse. Four participants had no professional licences. Two participants had experienced hikikomori, and there were two fathers of people with hikikomori. The participants practiced at 18 agencies in 12 cities nationwide.
The core category was identified as ‘Supporting them in finding their own ways to participate in society’. This core category was substantiated by following three interrelated stages: preparing the involved surroundings for reaching out to a person, maintaining constant communication, and expanding the range of activities and relationships. Figure 1 shows the theoretical structure of the result. The process encouraged people with hikikomori to enhance their social connections and improved their motivation for social participation. People with hikikomori experiencing despair and isolation began to find pleasure in social participation through the three stages of support provided by home-visiting workers.
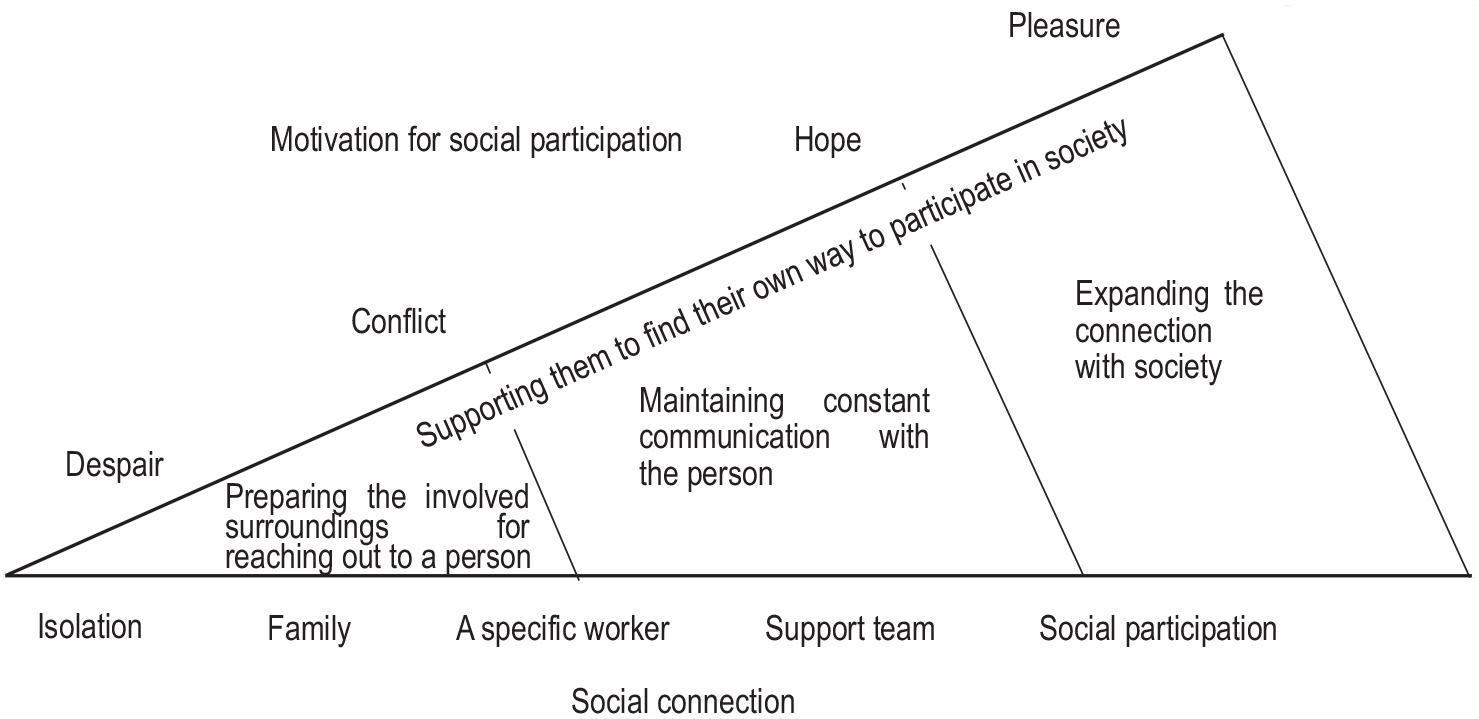
The three stages’ process of home visiting support for people with hikikomori.
Preparing the involved surroundings for reaching out to a person
Participants were provided with crisis interventions or family support to rebuild the relationship between the person with hikikomori and their family members. Such interventions helped individuals in despair and isolation realise their psychological conflict between their present state and their desired social participation.
Intervening in crises affecting those with hikikomori or family members
Specific crises included attempted suicides, violence against parents, deteriorating mental health and the sudden death of a parent. Participants informed the family of the crisis intervention response beforehand and cooperated with authorised organisations such as the police, public health centres, or hospitals to intervene efficiently in the affected individual’s home. After the crisis intervention, the person with hikikomori would be connected with appropriate support organisations and encouraged to build supportive relationships.
In a case that I oversaw, an adolescent with hikikomori assaulted his mother and brothers many times, leading to police visits. So, I went to visit the son after moving the mother and brothers to a nearby relative’s home. (19–8)
Supporting the family to rebuild a relationship with the person with hikikomori
For the person with hikikomori to re-establish independence in daily life and communication with their family, participants also provided support for family members such as advice for interacting with their dependent and listening closely to the family’s anxieties and frustrations. Support for the family usually occurred at the office, but home visits were conducted depending on the family’s situation.
I use actual conversations to advise parents about the best response to their withdrawn child. I looked at the notes in which parents wrote what they had said to their child and advised them, such as “This was not the best way to say. It would be better to say it like this next time”. (10–56).
Evoking feelings of conflict
As family members changed their attitudes towards those with hikikomori, feelings of conflict emerged between their reality and their ideal for social participation. Using information obtained from family members, participants sought to understand whether those with hikikomori realised that it was undesirable to continue in a withdrawn state and were motivated to change their behaviours.
When my advice helps family members to behave appropriately with the person with hikikomori, there is a change in the attitude of the person with hikikomori. Many families describe these changes as “we have more conversations with our child”, and “the atmosphere at home has become more pleasant”. The person with hikikomori starts to express their concern with their family: “Can I keep this withdrawn lifestyle?” They are conflicted between the desire to stop hikikomori and the fear that they are unable to do so. As I support the family, the suppressed conflicted feelings of the person with hikikomori begin to surface. (10–57)
Maintaining constant communication with the person
Sustained communication with specific home visiting workers offered hope to the afflicted individuals that solutions were available.
Sending a person messages expressing the desire to meet
Participants attempted to establish direct contact with the person with hikikomori by sending a message expressing their desire to meet face-to-face. Often, participants had the family propose the idea of home visit support to the person with hikikomori.
After approximately six months of consultations with parents, the person with hikikomori was still unable to talk to the mother but could speak to the father. So, I asked the father to “inquire about home visit support”. (1–4, 10)
Even when the person with hikikomori refused to be helped or to meet with the home visiting workers, participants made regular visits. They waited for the opportunity to offer support the moment the afflicted person changed their mind and prepared themselves to intervene when crises occurred. Participants knocked on the door to show that they were ready to help, and left quickly, leaving prompts such as information pamphlets, letters and notes: I visit the person refusing support three or four times a year to provide information that was written by people who used to have hikikomori and are now participating in the employment support programs. On rare occasions, when I saw the person with hikikomori, I explained employment support projects. (13–36, 37)
Creating a safe place
During home visits, participants did not discuss issues regarding work and school. Instead, they engaged in entertaining conversations about the person’s interests, hobbies and other general topics to make the person with hikikomori feel safe. Participants also shared hobbies and details of their personal lives to develop rapport with the affected individual.
I put all my energy into becoming friends with the person with hikikomori. I talk about myself a lot more than usual. Instead of “I came from XX clinic. My name is YY, and I am a psychologist. Can we talk about whatever is bothering you?” I make small talk like “You read that magazine? Me too”. “There seems to be no convenience store in the neighbourhood, isn’t that a pain?” and so on. Of course, I get the information about the person with hikikomori ahead of time and intentionally talk about things that would make me more acceptable to them. (14–29)
Accepting their life struggles
It was not unusual for the person with hikikomori to disclose their childhood trauma and difficult past experiences that led to the state of hikikomori. Participants did not pursue these negative thoughts or offer solutions; instead, they listened empathetically to the struggles of the person with hikikomori.
The person with hikikomori sometimes talked about their pain, calling him/herself “garbage”, but I didn’t take it too seriously. I think home visit support is different from psychotherapy, which aims to solve problems. Instead, I hope that spending time with me will allow them to slowly gain positivity to step out of their lonely hikikomori life (11–51).
Dealing with dissatisfaction and inconveniences in daily life
Participants helped the person with hikikomori to express their current dissatisfaction and inconveniences they faced in everyday life. They provided support, including making medical appointments, preparing paperwork for welfare services, accompanying them shopping, and advising them on how to communicate with their family members. By addressing these challenges, participants helped the person with hikikomori to naturally re-establish contact with society.
Since the person with hikikomori told me that ‘my computer broke down and I can’t play games’, I said, “Shall we go out to buy a new one together?” He responded with, “My mother wouldn’t approve, so I think we can’t”. I got permission from the mother, and we went to a computer shop together. (12–52, 53)
Expanding the connection with society
Participants made the person with hikikomori re-connect with society and experience the pleasure of social participation.
Increasing the number of people involved with the person with hikikomori
Participants tried to expand the relationships of the person with hikikomori by visiting with multiple staff who matched them in age, gender and interests.
For the person with hikikomori, it is important that the relationship grows gradually, and they become socialized. First, the same person makes all the visits, but by changing the staff or increasing the number of staff, we hope that the person with hikikomori will become able to talk to anyone who visits. However, we cannot make a sudden change, so we let the person with hikikomori set the pace. (15–98)
Helping the person with hikikomori to make their own decisions on how to connect with society
Participants provided the person with hikikomori positive feedback, role models and advice to ensure that they could make decisions about social participation at their own pace.
He said, “I have to find a job that is worth doing for a man’s whole life”, so I bluntly said, “you sound exactly like your father”. But his idea slowly changed, and he began compromising, saying, “I guess I will look for whatever job I can do”. I told him “I’ve changed jobs many times and I do not know if I’ll keep working at the present job, but I like this job anyway”. I do not know if I was somewhat of a role model for him, but he slowly let go of his father’s way of thinking, and he began accepting different ideas. (11–42, 43, 44)
Having the person with hikikomori experience the pleasure of social participation
After several visits, participants proposed going to self-help groups or job assistance. Participants helped the person with hikikomori to feel a sense of pleasure or fulfilment by visiting a social setting during the day.
We make efforts so that people with hikikomori can find joy in their social activities. For example, we sometimes enjoy cooking and having dinner together after field labour. (15–18-A)
Following the development of their social involvement
When the person with hikikomori was able to play a role in society, such as getting a job or enrolling in welfare services, the home visit support was terminated. Participants monitored the person with hikikomori and remained prepared to assist them if they encountered any problems in their ongoing journey.
Within the regional hikikomori support network, once the person with hikikomori has become connected to an appropriate support organization for social participation, the home visit team will take a step back and watch over them. If home visit support becomes necessary and the person is referred, they will step in again. (10–19)
Discussion
Our study suggests that home visiting support for people with hikikomori can be enhanced by three interrelated methods that help them to re-integrate into society and connect with others. The description of the specific details in home visiting support derived from the grounded theory approach indicates how to successfully connect withdrawn people with social services and treatments. Some studies have indicated that psychological status is related to attachment or childhood trauma and initial withdrawal episodes often begin in adolescence or early adulthood (Krieg et al., 2013; Li et al., 2015). Providing efficient early intervention would help those with hikikomori re-emerge into society without further delay.
The present study concretely described how to establish direct contact with people with hikikomori. Lee et al. (2013) indicated that the predominant problem in supporting people with hikikomori was therapeutic access, and that the home visit approach may be a good gateway to solve this problem. A French study showed nearly half of people with hikikomori had no professional assistance until they received home visit support (Chauliac et al., 2017). The first interview was conducted with the family or caregiver in over 70% of cases in a Spanish study (Malagón-Amor et al., 2020). However, the person with hikikomori who accepted and attended the initial visit had better outcomes, including decreasing problematic behaviours, and ensuring regular attendance/completed treatment, than those who refused the first visit (Imai et al., 2020; Kondo et al., 2008). In the present study, to establish constant communication with the person with hikikomori, participants carefully proposed home visit support in a personalised manner after considerable preparations, including family support, crisis intervention, assessments and evoking conflicting feelings.
The present study’s findings suggest that maintaining constant communication while solving dissatisfaction and addressing everyday life inconveniences is an effective way to build a trusting relationship with people with hikikomori. Kuroda (2018) indicated that to develop a relationship with people with hikikomori, it is essential to assess their state of mind that contributes to the support process towards social participation. Katsuki et al. (2019) reported that psychological tests revealed that persons with hikikomori were more likely to express emotions indirectly and expect others to presume their feelings and thoughts. It remains possible that these psychological statuses stem from difficulties in becoming emotionally independent from early attachments with significant others. Participants accepted the people with hikikomori, empathised with their life struggles, and provided a safe environment to build a relationship of trust while maintaining an appropriate psychological distance. Thus, it helped avoid dependency.
This study clarified that enabling autonomy in forming connections with society is crucial for people with hikikomori to expand their ranges of activities and relationships. People who feel lonely and isolated from society tend to evaluate themselves negatively and feel rejected by others (Jones, 1982). Hall-Lande et al. (2007) demonstrated that social isolation was associated with low self-esteem in youth. Masi et al. (2011) reported that the most successful interventions to reduce loneliness addressed maladaptive social cognitions. The results of our study indicate that participants believed the goal of home visit support was to find ways to participate in a society that allows the person to enhance their self-esteem, which was not limited to employment. This result suggests that people who were socially isolated and had low self-esteem developed positive views of themselves and trust in others via home visiting support.
The present study also suggested that workers require high levels of mental health knowledge, counselling skills and service planning in the home visit support process, which we confirmed. Previous studies have mentioned that home visit support for people with hikikomori requires professional skills. Lee et al. (2013) reported that due to difficulties in meeting clients, well-trained caseworkers visited each client’s home to interview both the client and their parents using a structured manual. There are reports in which the home visitation support team consisted of mental health personnel (Lee et al., 2013; Malagón-Amor et al., 2020). Further evidence is needed regarding the training of home visiting workers for people with hikikomori.
Limitations
The present study did not establish the effectiveness of home visiting methods since our results are contingent on the qualitative analysis of experts’ experiences or opinions. Further quantitative research is necessary to confirm the causal correlation between the implementation of such methods and its impact on people with hikikomori. Furthermore, the process of the actual practices may vary. Future participant-observer studies must validate such assessments. Additionally, this study did not examine the impact of the different demographic factors of workers and people with hikikomori, such as age or mental health status. Further research should evaluate how the process of home visit support varies according to such factors.
Conclusion
People with hikikomori who were experiencing despair and isolation found their own ways to participate in society through the three stages of support with home-visiting workers: preparing the involved surroundings for reaching out to a person, maintaining constant communication and expanding the range of activities and relationships. These findings are transferable to various settings of home visiting support for socially withdrawn people, including those outside of Japan. The nature of the comprehensive process of interaction between people with hikikomori and support workers is that it can work regardless of national health systems and cultural backgrounds. In future research, clarify training and qualifications for home visiting support is required to implement these methods effectively.