
Abstract
Background:
Home treatment (HT) is a patient-centred and cost-effective alternative to acute psychiatric inpatient care. However, the progress of its implementation and utilisation in routine care is slow.
Aims:
The aim of this study was to examine the knowledge and attitude towards HT among healthcare professionals.
Method:
This observational study included telephone-based semi-structured interviews of 140 referring healthcare professionals including 35 self-referring patients to a large psychiatric hospital in Switzerland during 6 months in 2020. We assessed their knowledge, attitude and experience with HT along with sociodemographic characteristics, professional background and the intention for the referral. We completed the interviews with routine medical data of the referred patients such as diagnoses or symptom severity.
Results:
Regarding referrals for inpatient treatment (involuntary and voluntary), half of the referring healthcare professionals and 80% of the self-referring patients had no prior experience or knowledge of HT. Knowledge of HT differed in the order of the participants’ working places. We found that most participants were uncertain about the inclusion/exclusion criteria for HT. Despite the low levels of knowledge, attitudes towards HT were overall positive.
Conclusions:
Our results indicate that a proportion of the patients referred for inpatient treatment might have been eligible for HT too. The referring healthcare professionals’ and patients’ unfamiliarity and uncertainty with HT seems to be an important reason that home-based treatment approaches are still underused, although they are viewed very positively. Besides providing more information to potential referring health professionals, psychiatric hospitals should always carry out a standardized evaluation if HT is an option in patients who are referred for inpatient treatment.
Keywords
Introduction
Most industrial countries have committed to develop and implement community-based mental health services as a preferable alternative to large psychiatric institutions (Semrau et al., 2011). In the course of this deinstitutionalisation process, home treatment (HT) has been proposed as a patient-centred alternative to inpatient treatment for adults with episodes of acute mental disorders (Johnson et al., 2008; Perkins & Burns, 2001; Smyth et al., 2000). The mobile and multi-professional HT teams provide intensive care in the patients’ homes including up to several visits a day with 24/7 accessibility. HT has been proven to be an effective treatment option (Murphy et al., 2015; Stulz et al., 2019) with high treatment satisfaction (Morant et al., 2017; Mötteli et al., 2020). Furthermore, during the spread of the COVID-19 pandemic, home-based treatment approaches were particularly helpful for psychiatric patients when inpatient treatment was limited due to various reasons (Garriga et al., 2020). While HT services have become an indispensable component in different mental healthcare systems (Hasselberg et al., 2011; Hubbeling & Bertram, 2014; Wheeler et al., 2015) they are still not fully established in German-speaking countries (Schwarz et al., 2019; Sjølie et al., 2010). For instance, in Switzerland, although clinical and cost effectiveness was demonstrated for HT services (Mötteli et al., 2018; Stulz et al., 2019) their implementation in routine care is only slowly progressing due to a lack of financial coverage of some healthcare providers (Stocker et al., 2018). This results in an underutilisation of HT services despite of the high satisfaction in patients (Mötteli et al., 2020). For a better utilisation of HT as a routine in mental healthcare, it is important to know how it is accepted and known among potential referring healthcare professionals. However, their views have been widely neglected in the evaluation of HT services to date. Results of a previous study (Morant et al., 2017) suggest that there are misunderstandings and a lack of knowledge of home-based treatment approaches similar as it has also been shown for consultation-liaison psychiatry (Chen et al., 2016).
The aim of this study was to examine the knowledge and attitude towards HT among potential referring healthcare professionals and self-referring patients. For this purpose, we compared the referrers of four groups of admissions to a large psychiatric hospital in Switzerland: HT, involuntary admission (IA), voluntary inpatient treatment and self-referrals to inpatient treatment. We assumed that referring healthcare professionals in general have little knowledge and some preconceptions towards HT and that referring psychiatrists are better informed compared to non-psychiatric physicians such as hospital and emergency physicians. We further assumed that a substantial part of the voluntary referrals for inpatient treatment would have also been eligible for HT based on patient characteristics.
Materials and methods
This observational study included telephone-based semi-structured interviews with referring healthcare professionals and self-referring patients to a psychiatric hospital as described below. The interview data were completed with routine medical data of the admitted patients. The use of a case identification number allowed for an anonymized dataset for data analyses.
Setting
The University Hospital of Psychiatry Zurich implemented HT in 2016 as one of the eight wards at the Center for Acute Psychiatric Disorders. It allows the acute treatment of up to 30 patients at the same time. This service provides an equivalent alternative to inpatient treatment for patients with acute mental disorders (Mötteli et al., 2018, 2020). Patients should be between 18 and 65 years old, capable to make agreements, and with a permanent residence in the municipality of Zurich or adjacent districts. Written consent for HT must be given by patients and their housemates. Exclusion criteria are IA, acute intoxications, substance dependence as main diagnosis and being at risk of self-harm or harm to others.
Sample and procedure
The study participants were n = 105 professionals such as psychiatrists, physicians with another specialisation, psychologists or other mental healthcare professionals who referred their patients to the Centre for Acute Psychiatric Disorders at the University Hospital of Psychiatry Zurich. Of those, n = 35 referred patients to HT, n = 35 referred patients to IA and n = 35 referred patients to voluntary inpatient treatment. Furthermore, we included n = 35 patients who referred themselves to inpatient care in the same unit. We did not include self-referring patients to HT because almost all of these patients had prior experiences with HT. The sample size for the four admission groups was determined by an a priori power analysis with alpha = .05, beta = .80 and a medium effect size (dz) of 0.30 resulted in n = 32 participants per group (Faul et al., 2007).
The participants were consecutively recruited between February and July 2020 using an anonymised list of the weekly admissions of the Centre for Acute Psychiatric Disorders (later referred to as ‘admission list’) including the date and time of admission, group (HT, IA or voluntary inpatient treatment), the name of the referring person and associated institution (or labelled as self-referral), the name of the treating hospital psychiatrist or psychologist, and a case identification number. Two students completed the list by adding the contact data of the referring healthcare professionals. They consecutively contacted the referring persons by telephone or email and asked them to participate in the interview. Regarding self-referrals, treating psychologists were instructed to ask the patients within 5 days after admission whether they would like to participate in the study. The number of admissions to the different groups varied as well as the availability of the referring persons, which resulted in different response rates (see Figure 1). The referring persons were contacted up to three times. Those listed more than once were excluded subsequently after the one completed interview. In total, n = 127 interviews were successfully conducted by telephone and n = 13 were completed by emails due to time constraints. The referring health professionals’ professional backgrounds and working places varied according to the different groups (see Table 1).
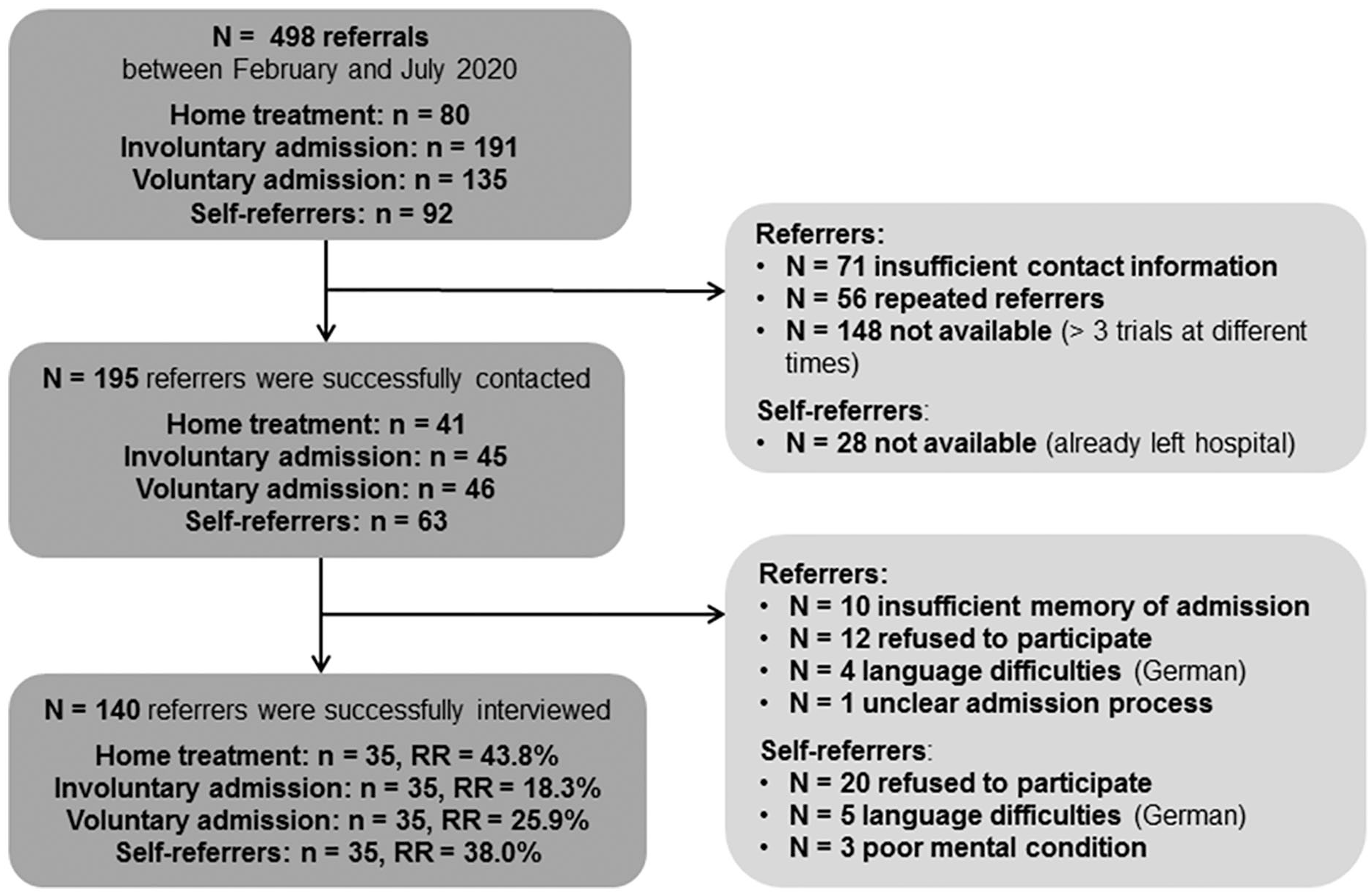
Flowchart of the participants’ inclusion process (RR = response rate).
Characteristics of the referring health professionals (n = 35 for each admission group).

Note. Missing data on age (n = 3), working experience (n = 1), working place (n = 1).
Interviews
Procedure
Between February and July 2020, we surveyed n = 105 referring healthcare professionals and between May and July 2020 additional n = 35 self-referring patients. The interviews lasted about 5 to 7 minutes. The mean duration between the patients’ admissions and the participants’ interviews was Md = 8 days. The questionnaire included, among others, closed and open questions about knowledge, attitude and experience with HT and other treatment settings. The questions have been specifically created for the study’s purpose and have been pretested with a handful volunteers for comprehensibility and duration. Where necessary, questions were slightly adapted for self-referrals. Open answers were noted as short sentences or keywords.
Measures
Knowledge of HT: We asked the participants how well they are informed about the HT of the University Hospital of Psychiatry Zurich. Answers could be given on a 5-point Likert-type scale ranging from 1 to 5 (1 = don’t know HT to 5 = very well informed). If the participants’ answers were 2 = slightly informed or higher, we further asked the participants to indicate the relevant inclusion/exclusion criteria for HT in their opinion (open question).
Attitude towards HT: If the participants stated to know HT (2 = slightly informed or higher), we asked the participants whether HT is, in their opinion, a good (equivalent) alternative to acute inpatient care (psychiatric treatment at home instead of a hospital stay). Answers could be given on a 5-point Likert-type scale ranging from 1 to 5 (1 = not at all to 5 = very good alternative). Answers ranging from 4 to 5 indicated positive attitude towards HT.
Previous experience with different treatment settings: Participants were asked whether they previously referred patients to inpatient treatment, HT, day-care hospital or outpatient treatment.
Case-related questions: We asked the participants about the reasons for the current admission, to describe the treatment aims of the hospitalisation in open-question formats, to state if risk of self-harm or harm to others was a reason for admission, whether they reflected about other treatment options, and for how long they have known the referred patient before admission.
We also assessed the following personal characteristics of the participants: Gender, age, professional background, years of working experience and working place (see Table 1). Working place was categorized as follows: Psychiatric clinics and private practices versus other working places including somatic hospitals, GP’s, emergency physicians and others.
Selected routine medical data
We used the following variables from the routine medical data records of the referred patients: Gender, age at admission, primary psychiatric diagnosis according to the ICD-10, severity of symptoms based on the Health of the Nation Outcome Scales (HoNOS) upon admission (Wing et al., 1998) with higher scores denoting worse health (ranging from 1 to 48), and number of previous hospital stays (see Table 2).
Characteristics of the referred treatment cases (n = 35 for each admission group).

Note. Missing data on HoNOS (n = 7) and main diagnosis (n = 12), routine data assessed by the responsible hospital psychiatrist/psychologist.
Qualitative and quantitative data analyses
Based on the recommendations of Braun and Clarke (2006) we conducted thematic analysis of the qualitative data from the open questions. The two students independently coded the open answers, compared and discussed the codes to achieve a consensual coding structure, supervised by the first author. They independently examined the coded data to identify common categories, which were again compared and discussed.
For descriptive analysis of the quantitative data, we calculated frequencies (n, %), means and standard deviations. Differences in HoNOS were calculated using one-way ANOVA and differences in knowledge and attitude were calculated using t-tests for independent samples. Statistical analyses were performed using IBM SPSS (version 26 for Windows, IBM Corp. 2019). The p-value for statistical significance testing was set at alpha ⩽ .05 for general questions and ⩽.025 for directed questions.
Results
Characteristics of referrals between HT and inpatient treatment
Regarding HT, the majority of the referring healthcare professionals were psychiatrists (60%) or psychologists (17%) who worked in a psychiatric practice or clinic (see Table 1). In line with the inclusion/exclusion criteria for HT, the participants stated that the patients were having a low risk for self-harm or harm to others. Besides ‘crisis intervention and stabilisation’, they named a variety of other treatment aims such as ‘support in daily routine’, ‘medical treatment’ or ‘avoidance of inpatient treatment’ (see Table 2). Two third of the participants had known their patients >4 weeks (Md = 36 weeks).
More than half of the patients referred for HT were female and had an affective disorder as main psychiatric diagnosis. Their HoNOS score was M = 20.82 (SD = 6.28) and did not differ among the other groups (F = 1.27, df = 3, p = .286).
Regarding inpatient treatment (IA and voluntary), most referring healthcare professionals were non-psychiatric physicians working in a somatic hospital (see Table 1). A substantial part of them referred their patients for inpatient treatment because they found the patients to be at acute risk for self-harm or harm to others. The treatment aim was mostly crisis intervention and stabilization (see Table 2). Most participants had known their patients <4 weeks. Patients referred for inpatient treatment were more likely male with a broader range of main ICD-10 psychiatric diagnoses compared to HT.
Knowledge of HT
Regarding referrals to HT, most of the n = 35 participants stated to be good or very well informed (68.6%) about this treatment option. Nevertheless, 10 participants responded to be little to medium (28.6%) informed and one participant (2.9%) had no prior knowledge of HT. In contrast, and in line with our expectations, half of the participants who referred their patients to inpatient treatment (IA: 45.7%, voluntary: 57.1%) and 80.0% of the self-referring patients were not at all informed about HT (see Figure 2). In addition, knowledge of HT differed in the order of the participants’ working places: Psychiatrists affiliated with the University Hospital of Psychiatry Zurich (M = 4.07, SD = 1.16, n = 15), psychiatrists in private practices (M = 3.64, SD = 1.22, n = 25), or in psychiatric clinics (M = 3.25, SD = 1.22, n = 12), physicians from other working places (M = 2.43, SD = 1.62, n = 7), from somatic hospitals (M = 1.91, SD = 1.41, n = 23), GP’s (M = 1.85, SD = 1.35, n = 13), and emergency physicians (M = 1.22, SD = 0.44, n = 9). Concerning only referrals for inpatient treatment, referring healthcare professionals who worked in psychiatric clinics or in private practices were significantly better informed about HT than those with other working places (M = 3.39, SD = 1.40 vs. M = 1.43, SD = 1.40, t = 7.12, df = 68, p < .001).
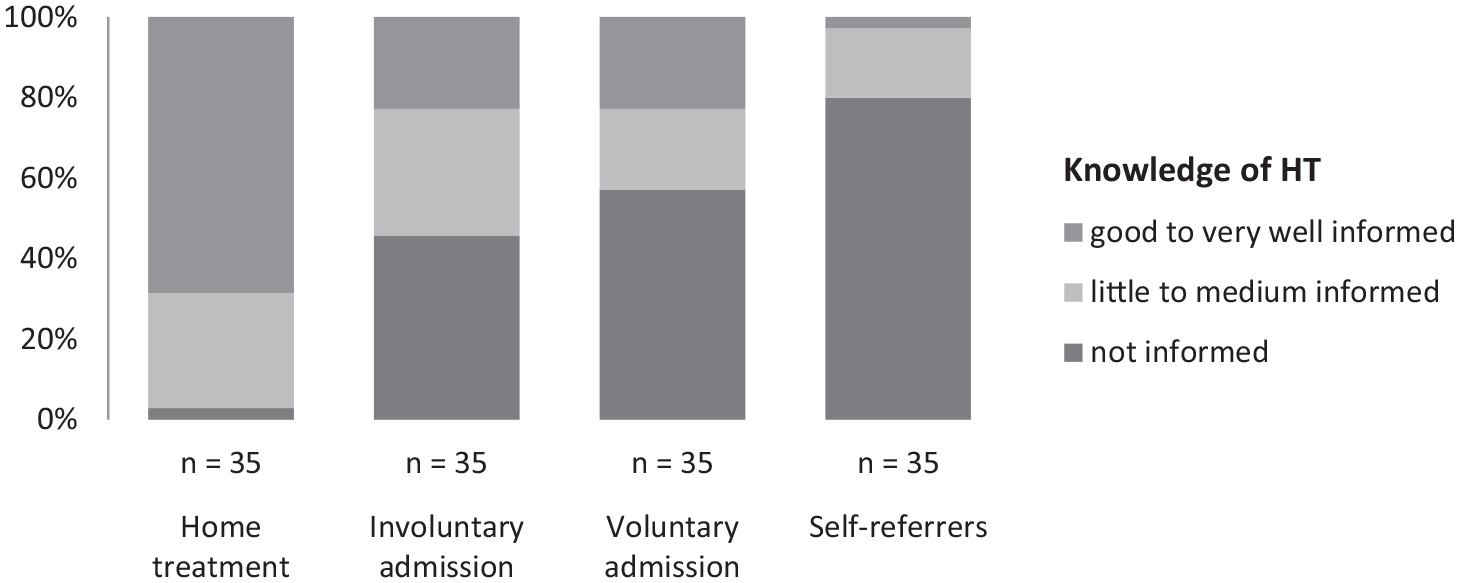
Knowledge of HT as an alternative to inpatient treatment among referring health professionals of the different admission groups.
Participants (n = 74) who indicated to be informed about HT named on average two criteria, which were, in their opinion, relevant inclusion/exclusion criteria for HT. Based on the participants’ open answers (p = participant), the criteria were summarized into the following categories: ‘Compatible psychiatric symptoms’ (n = 58, 78.4%, e.g. ‘no suicidal intention’, p 547), ‘independence/level of functioning’ (n = 38, 51.4%, e.g. ‘ability to keep agreements’, p 419), ‘housing preconditions’ (n = 18, 24.3%, e.g. ‘suitable living conditions’, p 572), ‘insufficient outpatient treatment’ (n = 17, 23%, e.g. ‘inpatient treatment is not necessary, but outpatient treatment is not enough’, p 40), ‘patient’s wish’ (n = 15, 20.3%, e.g. ‘wants to stay at home because of children, pets or work’, p 142), ‘legal preconditions’ (n = 9, 12.2%, e.g. ‘health insurance covers the costs’, p 139) and other not specified criteria (n = 11, 14.9%, e.g. ‘knows how to check the criteria online’, p 313).
Attitude towards HT
Attitude towards HT (only assessed for participants with knowledge of HT) varied among the examined groups in the following order: HT (M = 4.50, SD = 0.71, n = 34), IA (M = 4.17, SD = 1.04, n = 18), voluntary inpatient treatment (M = 3.62, SD = 1.12, n = 13) and self-referrals (M = 3.0, SD = 1.63, n = 4). Participants who referred their patients to HT had a significant more positive attitude towards HT compared to those who referred their patients to inpatient treatment (M = 4.50, SD = 0.71, n = 34 versus M = 3.83, SD = 1.18, n = 35, t = 2.87, df = 67, p = .006). However, there were no significant differences related to the participants’ working places.
Previous experience with HT
Half of the participants who referred their patients to HT (51.4%) stated to have previous experience with HT admissions. In contrast, a fifth (20%) of the referring persons to IA, a fifth (20%) of the referring persons to voluntary inpatient treatment, and only 8.6% of the self-referring patients indicated such experience. On the other hand, >80% of all referring healthcare professionals and 65.7% of the self-referring patients reported to have previous experience with admissions for psychiatric inpatient treatment.
Discussion
The implementation of HT as a patient-centred and cost-effective alternative to inpatient treatment for people in acute psychiatric crisis is only slowly progressing in German-speaking countries, although its benefits were demonstrated (Schwarz et al., 2019; Sjølie et al., 2010; Stulz et al., 2020). In this study, we examined the knowledge and attitude towards HT in referring healthcare professionals and self-referring patients of a large psychiatric hospital. By comparing different admission groups such as HT, IA and voluntary inpatient treatment, we showed that more than half of the referring persons to IA and voluntary inpatient treatment including self-referring patients had no or little knowledge of HT. In addition, referring healthcare professionals working in psychiatric clinics or psychiatric practices were significantly better informed than those with other professional backgrounds. Similarly, the majority of the referring persons had no prior experience with HT. Although only referring persons to HT had high knowledge levels, attitudes towards HT were positive in all groups. As a consequence, it seems to be necessary to better inform and educate potential referring healthcare professionals about HT services in the future. Especially general physicians, those working in somatic hospitals and emergency physicians who made up half of the referrals to inpatient treatment might benefit from information about HT. Sufficient information of non-psychiatric physicians about psychiatric treatment options, their indication, inclusion- and exclusion criteria seems to be important because a substantial part of the patients in the non-psychiatric fields of medicine have psychiatric problems (Downey et al., 2012; Fulbrook & Lawrence, 2015). Hospital physicians might further benefit from services of consultation- liaison psychiatry in their hospital who have a valid overview on the mental healthcare structures in the region (Evans et al., 2019). Related to emergency physicians, knowledge of HT might be helpful as well to prevent IA in circumstances were outpatient treatment seems to be not sufficient and inpatient treatment is refused by the patient (Mötteli et al., 2021). In addition, patients should also be informed about the HT option (for instance at the beginning of their inpatient treatment through the clinics’ triage team) as most of them do not know the existence of HT services, but have a positive attitude towards this approach.
Based on the examined clinical data in this study (e.g. risk assessment, treatment aims, main psychiatric diagnosis and severity of symptoms) and in line with previous results (Mötteli et al., 2018), a substantial proportion of the patients referred to voluntary inpatient treatment might also have been eligible for HT. Furthermore, the variety of treatment aims for HT which were named for HT supports the broad spectrum of patients who might benefit from HT and the personalised treatment approach of this service (Perkins & Burns, 2001). However, HT cannot replace inpatient treatment in every situation and, besides the patient’s willingness, some eligibility criteria have to be taken into account. Interestingly, the participants who stated to be informed about HT named less often legal criteria (e.g. age, place of residence) and housing preconditions (e.g. permanent residence, consent of housemates for HT) as barriers. More often, they named illness-related factors such as psychiatric symptoms and impaired level of functioning as limiting factors, although, in reality these criteria are less problematic and might be well handled depending on the HT’s resources. These results indicate some misunderstandings and uncertainties of the HT’s capability, that might influence the patients’ (and professionals’) considerations for/against HT and were already assumed in a previous study (Morant et al., 2017).
Due to contacting difficulties (e.g. low availability of hospital and emergency physicians), the response rates for the referring health professionals to IA and voluntary inpatient treatment were rather low, which could have produced biased samples. However, the assessed patient characteristics are in line with those of the patients generally treated at the acute wards of the University Hospital of Psychiatry Zurich indicating representativeness (Mötteli et al., 2018). Also, the participants’ characteristics correspond to those of a previous study including a similar sample (Hotzy et al., 2019). In addition, the results might be limited in terms of generalisation, as we only surveyed referrals to one psychiatric hospital. A further limitation is the interview duration of only 5 to 7 minutes, which did not allow asking more comprehensive questions about knowledge, attitude and experience with HT. Nevertheless, the combination of survey data including closed and open questions with medical routine data is a strength of the current study which provides useful insights in the views of referring health professionals and patients.
In conclusion, the results of this study indicate that a proportion of the patients referred to inpatient treatment might have been eligible for HT. The referring health professionals’ and patients’ unfamiliarity and uncertainty with HT seems to be an important reason that home-based treatment approaches are still underused as an alternative to inpatient treatment for adults with acute mental illness. Attitudes are rather positive in those with and without experiences and knowledge of this approach. Broader information about HT seems needed, especially for non-psychiatric physicians such as GP, emergency physicians or somatic hospital physicians. In addition, psychiatric triage teams should clarify if inclusion criteria for HT are met and provide sufficient information about HT when a patient is referred or refers him-/herself for inpatient acute treatment.
Footnotes
Acknowledgements
We thank Jeannette Rappo and Marc Peterhans for their support in the data collection process.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Compliance with ethical standards
This study does not fall within the scope of the Swiss Human Research Act and, therefore, ethical authorisation was not required. The local ethics committee of the Canton of Zurich provided a declaration of non-competence for this study (req-2019-01291). All participants agreed to participate in the interview.
Availability of data and material
Due to data sensitivity, data cannot be shared publicly.