
Abstract
Background:
Refugee youth often face numerous adversities before and during forced migration. Although experiences vary across settings and subpopulations, common mental disorders are prevalent among refugee youth who are displaced in low- and middle-income countries. It is important to examine how risk factors are intricately linked and contribute to common mental health issues to inform clinical practice and social policy.
Aims:
This study aims to test the pathways from risk factors previously identified as determinants of Somali refugee youth mental health (i.e. trauma exposure, substance use, social functioning, aggression) to symptoms of PTSD, depression, anxiety, and somatic pains.
Method:
We collected survey data in 2013, using snowball sampling to recruit Somali refugee youth (15–35 years old) living in Eastleigh, Kenya. We ran three structural equation models to assess paths from trauma exposure to mental health symptoms, through psychosocial factors including substance use, aggression, and functional impairment. We first conducted this analysis with a mixed-gender sample (N = 305) and then assessed gender differences by running one model for male participants (n = 124) and another for female participants (n = 181).
Results:
In the mixed-gender sample, trauma exposure directly predicted substance use and both directly and indirectly predicted aggression, functional impairment, and mental health symptoms. Substance use directly predicted aggression and functional impairment, and substance use both directly and indirectly predicted mental health symptoms. The split-gender models revealed gender differences, with only functional impairment directly predicting mental health symptoms in the male sample and with many significant direct and indirect pathways in the female sample.
Conclusions:
This study shows the role of trauma exposure, substance use, aggression, and social functioning in determining mental health outcomes among refugee youth and how CMD symptoms are differently manifested across genders in this population.
Keywords
Refugee youth comprise the majority of refugee populations globally, including an estimated 30 to 34 million minors below the age of 18 (United Nations High Commissioner for Refugees [UNHCR], 2020a). Given the challenges throughout forced migration, refugee youth are exposed to cumulative and prolonged traumas that can worsen social functioning and health and mental health outcomes (Frounfelker et al., 2020; Newnham et al., 2018; Reed et al., 2012). Although experiences vary across settings and subpopulations (Blackmore et al., 2020; Fazel et al., 2005; Hinton & Lewis-Fernández, 2011), common mental disorders (CMDs), such as depression, anxiety, post-traumatic stress disorder (PTSD), and somatization, are prevalent among refugee youth and particularly those in low- or middle-income countries (LMICs; Frounfelker et al., 2020; Reed et al., 2012). For example, up to 87% of refugee youth in camp settings report trauma-related CMD symptoms (Vossoughi et al., 2018). Precarious living in low-resource settings likely adds multi-layered challenges that exacerbate mental health issues in refugee children and youth (Patel et al., 2008; Scharpf et al., 2020).
Various risk and resilient factors impacting mental health at individual, family, and school and community levels have been identified and explored in previous research (Patel et al., 2008; Pieloch et al., 2016; Roberts & Browne, 2011; Tol et al., 2010). Some of these factors include demographic characteristics (e.g. gender, age, education, socio-economic factors), the type and chronicity of trauma exposure (e.g. cumulative or prolonged trauma vs. acute trauma, complex trauma, recency of trauma events), coping styles and resources, social functioning, and family and community support (de Anstiss & Ziaian, 2010; Giacco et al., 2018; McGregor et al., 2015). Refugee youth, for example, appear to have greater resilience and less mental health susceptibility than older refugees following stress and trauma related to migration (Ahmad et al., 2020; Jensen et al., 2015; Porter & Haslam, 2005). Among others, gender is a significant predictor of CMDs as well as refugee traumas. Numerous studies have shown that women are at higher risk of mental health issues, especially PTSD and depression, than men (Olff et al., 2007; Schubert & Punamäki, 2011; Sherin & Nemeroff, 2011; Young & Chan, 2015). This increased risk is often attributed to the types of trauma events commonly experienced by women (e.g. sexual and gender-based violence), which are likely to occur at a younger age and have more devastating physical and mental health effects on women with stronger perceptions of threat and loss of control due to insufficient social support resources during social conflicts or displacement (Olff et al., 2007; Renner & Salem, 2009). The type and chronicity of refugee trauma experiences are also well-known factors associated with mental health outcomes (Bielas et al., 2016; Reed et al., 2012) along with substance use as self-medication in response to trauma (Ertl et al., 2016; Horyniak et al., 2016; Lockwood & Forbes, 2014; Posselt et al., 2015). Both trauma exposure and malfunctioning coping, such as substance use, have devastating effects on social functioning, which likely exacerbate mental health symptoms in refugee populations (Lockwood & Forbes, 2014; Miró et al., 2020; Norman et al., 2018; Rodriguez et al., 2012).
Mental health among Somali refugee youth
Somali refugee communities have experienced prolonged conflict for decades, since the civil war in 1991, which caused the forced migration and protracted displacement of millions of Somalis (UNHCR, 2020b). Due to the cumulative effects of individual and collective traumas and life challenges faced before and during displacement, high levels of CMDs, substance use, and psychiatric problems have been reported in Somali refugees, including youth (de Jong et al., 2011; Ellis et al., 2010; Feyera et al., 2015; Onyut et al., 2009). Research has suggested gender differences in terms of how Somalis experience, process, and respond to traumatic stress (Kroll et al., 2010). For example, female Somali refugees are more likely to report mental health problems than male Somali refugees (Feyera et al., 2015; Mölsä et al., 2014) in part due to cultural, social, and gender norms associated with emotional expressions and self-presentation (Kroll et al., 2010). Somali refugee youth have reported using various substances, such as alcohol, drugs, tobacco, and khat (a plant commonly used as a stimulant drug in East Africa), as a coping mechanism; however, research indicates that such substance use can lead to worsened traumatic pain, diminished social functioning, and psychotic symptoms for Somali refugee youth (Im & George, 2021; Odenwald et al., 2005). Dysregulation of destructive emotions, such as anger and aggression, also interferes with refugee youth mental health (Nickerson, 2018; Nickerson et al., 2015; Spiller et al., 2016; Tuomisto & Roche, 2018). In Somali youth, research has indicated that negative emotions, such as anger and aggressive behaviors, following trauma exposure tend to contribute to interpersonal and community violence and fuel the cycle between trauma and violence (Im et al., 2016).
Associations among multiple factors
A substantial body of empirical studies has identified risk factors in refugee youth in general and in Somali refugee youth specifically, but the associations between multiple risk factors are complex and incongruent across studies. For example, several studies have explored acculturative stress, gender discrimination, cultural orientation, and coping style as mediators between refugee trauma exposure and CMDs (Kartal et al., 2018; Kira et al., 2010; Matheson et al., 2008). Another study showed how different types of traumas (e.g. interpersonal- and non-interpersonal-trauma) are associated with CMDs among refugee youth in resettlement (Kim, 2016). A study with young people in South Africa examined how childhood trauma contributes to drug use and the perpetration of interpersonal violence and how such trauma and subsequent life challenges (e.g. food insecurity, disrupted education) directly and indirectly affect depression (Gibbs et al., 2018). One recent study with Somali refugees in the U.S. revealed how acculturation factors may mediate the relationship between refugee trauma and mental health issues (Jorgenson & Nilsson, 2021). These studies suggest pathways and associations among trauma exposure, risk factors, and CMDs, although few have focused specifically on Somali refugee youth in the context of displacement in marginalized communities or LMICs.
Given the magnitude of adversities that refugee youth face during displacement, it is important to untangle how multiple risk factors are intricately linked and contribute to common mental health issues. This study aims to test the pathways from risk factors previously identified as determinants of Somali refugee youth mental health (i.e. trauma exposure, substance use, social functioning, aggression) to symptoms of PTSD, depression, anxiety, and somatic pains. This model examines how substance use as a way of coping with traumatic experiences may affect aggression and social functioning, ultimately influencing mental health in this population. Since there are highly divergent effects of trauma and distinct, gender-based patterns of mental health in the Somali community, we also tested the model with a split-gender sample.
Methods
Participants and procedure
In collaboration with a community-based organization and local clinic in Eastleigh, an urban area in Nairobi, Kenya where many Somali refugees have resettled, we used snowball sampling to recruit Somali refugee youth living in Eastleigh for study participation. This sampling strategy was deemed necessary due to the challenges associated with mobilizing and recruiting refugee participants in urban settings. We included participants aged 15 to 35 years old according to the African Union Commission’s (2006) definition of youth. A local community advisory board and the Institutional Review Board at the authors’ institution approved this research. We collected data in two phases, with the first producing 250 participants in 2013 and the second producing 86 participants later in 2013. After comparing data from the two phases on key study variables revealed adequate phi and Pearson’s correlations, we combined the two phases for a total sample size of 336. After removing 31 cases with missing data, our final sample size was 305.
Measurement
Participants completed a survey, available in both English and Somali, assessing trauma exposure, psychosocial factors, mental health symptoms, and demographic characteristics.
Trauma exposure
In consultation with community partners, the authors compiled a list of 12 trauma experiences that are common in this population (experiencing war, experiencing loss of family members, experiencing domestic violence, living in a refugee camp, experiencing forced migration, experiencing injury from community violence, observation of community violence, being arrested, being kidnapped, experiencing child abuse, experiencing sexual abuse, experiencing a serious accident). For each trauma category, participants indicated whether they had (=1) or had not (=0) experienced that type of trauma. These items were then summed for a theoretical range of 0 to 12. Cronbach’s alpha (α = .780) indicated that this measure had adequate internal reliability.
Psychosocial factors
We assessed substance use with a single item asking participants about their use of substances (i.e. drugs or alcohol) over the past month to reduce stress and bad feelings. We also assessed aggression with a single item asking participants about becoming angry and yelling, hitting, threatening, or destroying things in the past month. We assessed functional impairment by summing two items (α = .735) asking participants about avoiding socialization and feeling unable to fulfill family or community roles. Response options for each of these items ranged from “not at all” (=0) to “almost always” (=4). As adapted from Terheggen et al. (2001), we aimed to help participants understand this Likert-type scale by providing a visual scale showing glasses filled with various amounts of water and images of a monthly calendar with increasing numbers of days marked.
Mental health symptoms
Symptoms of PTSD, depression, and anxiety were assessed using established measures previously used with Somali and refugee populations (Jakobsen et al., 2017; Wind et al., 2017; Yeomans et al., 2010). We used the 17-item PTSD Check List–Civilian Version (PCL-C) to assess symptoms of PTSD and the 25-item Hopkins Symptom Checklist-25 (HSCL-25) to assess symptoms of depression and anxiety. Since there is no established somatization measure validated with this population, through consultation with our community partners, we developed a seven-item measure assessing the presence of the following culturally-relevant somatic symptoms: (1) heavy feelings in the legs and arms, (2) having diarrhea due to stress and bad feelings, (3) having an upset stomach, nausea or bloating, (4) feeling pain in the lower back, (5) having a dry mouth, (6) having cold hands and feet, and (7) being unable to move and becoming like a stone or being frozen.
Response options for each PCL-C, HSCL-25, and somatization item included response options ranging from “not at all” (=0) to “almost always” (=4). As described above, this Likert-type scale was accompanied by a visual scale. Cronbach’s alpha indicated that these measures of PTSD (α = .909), depression (α = .917), anxiety (α = .890), and somatic symptoms (α = .860) had high internal reliability for this sample.
Demographic variables
We also included two demographic control variables. We assessed gender as a dichotomous variable (0 = female, 1 = male) and age as an open-ended continuous variable.
Analytic strategy
We conducted descriptive and bivariate tests followed by three structural equation models estimated using maximum likelihood and 10,000 bootstrapping replications. Each structural equation model assessed paths from trauma exposure to mental health symptoms, through substance use, aggression, and functional impairment (see Supplementary Resource 1). We first conducted this analysis with the full, mixed-gender study sample, while controlling for the effects of age and gender. Then, we assessed gender differences by running one model for male refugee participants and another for female refugee participants, while controlling for the effects of age. Data analyses were conducted in SPSS version 26 and Mplus version 8. With the full, mixed-gender sample (standardized factor loadings ranging from 0.457 to 0.849) and with the female-only sample (standardized factor loadings ranging from 0.360 to 0.909), all factor loadings were significant. With the male-only sample (standardized factor loadings ranging from 0.372 to 0.734), all factor loadings were significant except for the two functional impairment items (see Supplementary Resource 2).
Results
Demographic characteristics
Table 1 shows participant characteristics by gender. The mean age of the sample was 20.04 (SD = 3.01), and there were more female participants (n = 181, 59.3%) than male (n = 124, 40.7%). Male and female participants did not significantly differ on age, trauma exposure, substance use, or aggression, but female participants reported significantly higher functional impairment and more symptoms on all mental health measures.
Participant characteristics.
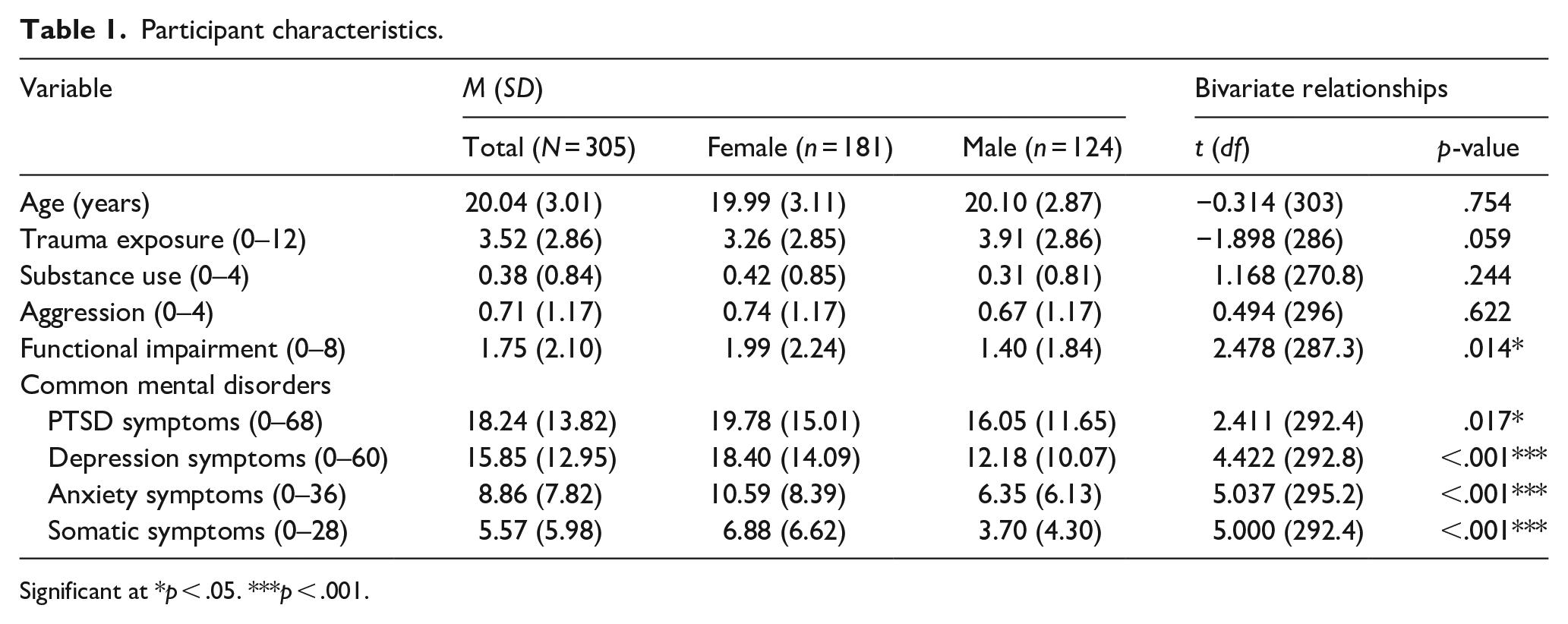
Significant at *p < .05. ***p < .001.
Mixed-gender model
The first, mixed-gender model (N = 305) had good fit for the data (χ2 = 2035.520, df = 4059, p = 1.000). As shown in Table 2, the model indicated statistically significant direct effects of trauma exposure on substance use (β = .256, p = .003), aggression (β = .272, p = .001), functional impairment (β = .303, p = .002), and symptoms of PTSD (β = .148, p = .036), and anxiety (β = .194, p = .007). Substance use had a direct and positive effect on aggression (β = .315, p < 0.001), functional impairment (β = .294, p < .001), and symptoms of depression (β = .147, p = .013) and somatization (β = .161, p = .021). Aggression and functional impairment had direct and positive effects on symptoms of PTSD (aggression: β = .169, p = .003; functional impairment: β = .549, p < .001), depression (aggression: β = .206, p = .001; functional impairment: β = .522, p < .001), and somatization (aggression: β = .232, p = .001; functional impairment: β = .450, p < .001), while increased functional impairment (β = .501, p < .001) but not aggression (β = .098, p = .146) directly predicted anxiety symptoms.
Structural equation model direct effects.
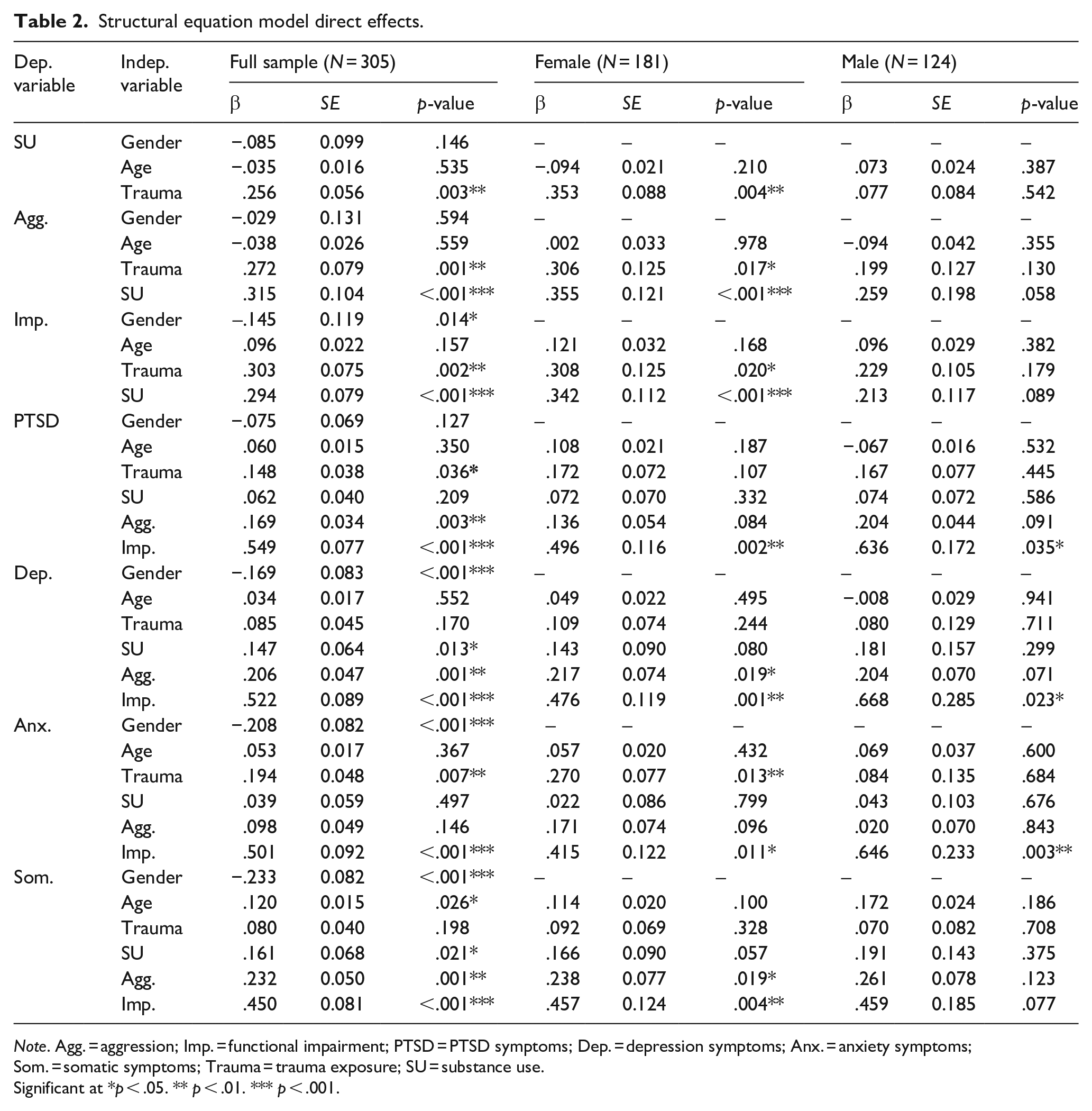
Note. Agg. = aggression; Imp. = functional impairment; PTSD = PTSD symptoms; Dep. = depression symptoms; Anx. = anxiety symptoms; Som. = somatic symptoms; Trauma = trauma exposure; SU = substance use.
Significant at *p < .05. ** p < .01. *** p < .001.
Table 3 presents the specific indirect effects of this first model, indicating that substance use, aggression, and functional impairment were significant mediators in this model, indirectly affecting relationships between trauma exposure and mental health symptoms. While all hypothesized mediation effects were present for depression and somatic symptom outcomes, substance use did not mediate the relationship between trauma exposure and PTSD symptoms, and several indirect predictors of anxiety symptoms were non-significant.
Structural equation model specific indirect effects (N = 305).
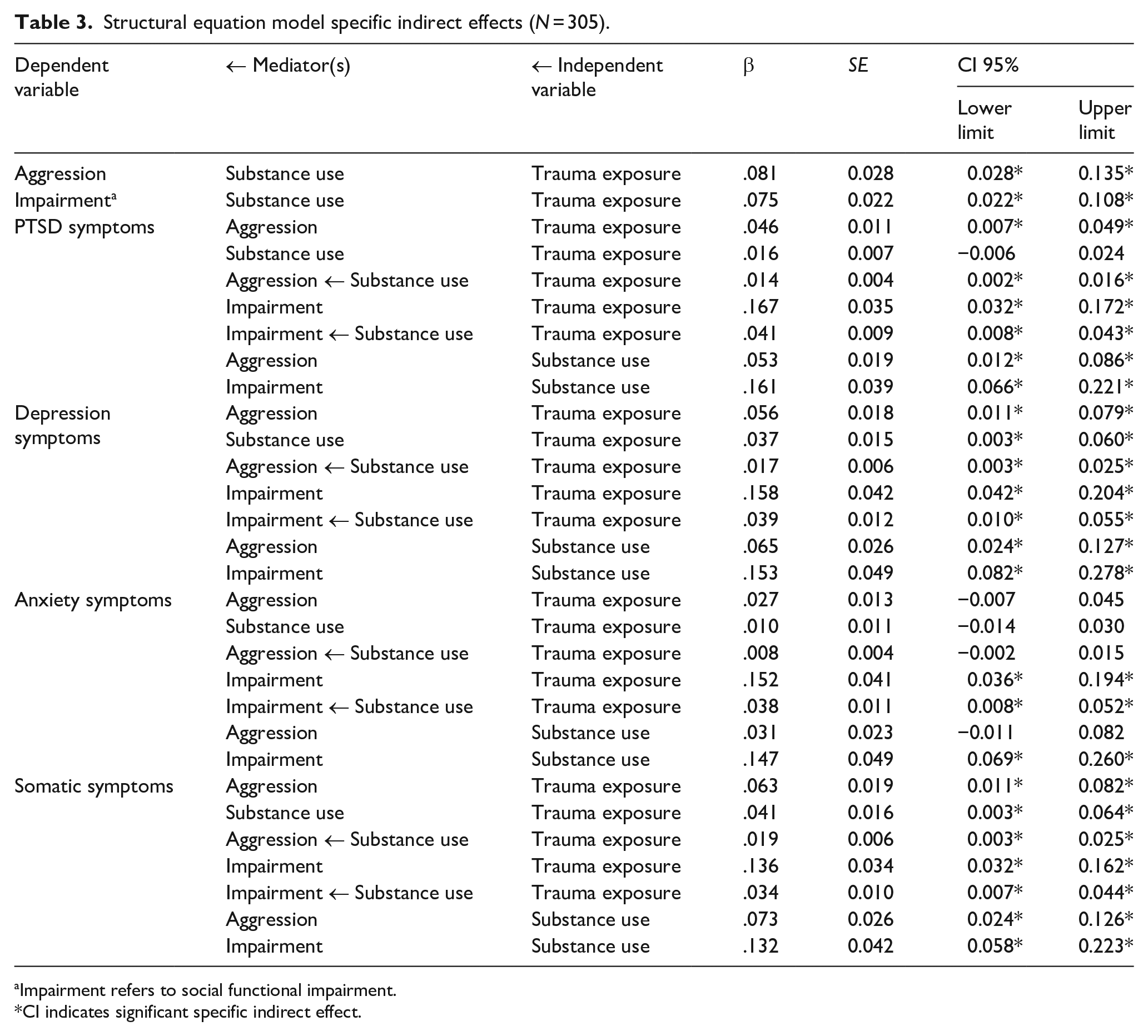
Impairment refers to social functional impairment.
CI indicates significant specific indirect effect.
Modeling gender differences
Table 2 also presents the direct effects of the two split-gender structural equation models. Both the female-only (χ2 = 132.049, df = 7463, p = 1.000) and male-only (χ2 = 1504.583, df = 4062, p = 1.000) models had good fit for the data. Results showed that in the male sample, only functional impairment had a direct effect on mental health symptoms (PTSD: β = .636, p = .035; depression: β = .668, p = .023; anxiety: β = .646, p = .003; somatic: β = .459, p = .077). However, in the female sample, trauma had a direct and positive effect on substance use (β = .353, p = .004), aggression (β = .306, p = .017), functional impairment (β = .308, p = .020), and anxiety symptoms (β = .270, p = .013). Additionally, in this female sample, substance use had a direct and positive effect on aggression (β = .355, p < .001) and functional impairment (β = .342, p < .001). In the female sample, aggression had a direct and positive effect on symptoms of depression (β = .217, p = .019) and somatization (β = .238, p = .019). Figure 1 shows these significant direct effects from the split-sample models compared to the significant direct effects in the full, mixed-gender sample.

Significant direct effects in full and split-sample structural equation models.
Table 4 presents the specific indirect effects of the two split-gender models. Results showed substantial gender differences in these indirect effects, with no significant mediation effects in the male sample and many significant mediation effects in the female sample.
Structural equation model specific indirect effects for split-gender samples.

Note. Agg. = aggression; Imp. = functional impairment; PTSD = PTSD symptoms; Dep. = depression symptoms; Anx. = anxiety symptoms; Som. = somatic symptoms; Trauma = trauma exposure; SU = substance use.
CI indicates significant specific indirect effect.
Discussion
This study tested structural equation models to examine the relationships among trauma, substance use, functioning, and CMD symptoms among male and female Somali refugee youth in urban Kenya. Functional impairment directly predicted CMD symptoms in both the mixed-gender and split-gender samples. This is consistent with previous studies that emphasize the role of functional impairment in PTSD symptom manifestation (Miró et al., 2020; Norman et al., 2018; Rodriguez et al., 2012). This study extends this finding to other CMD symptoms, revealing that functional impairment also predicts symptoms of depression and anxiety among Somali refugee youth in urban displacement. Aligned with the previous research on gendered patterns in experiencing and communicating mental health issues (Marshall et al., 2016; Young & Chan, 2015), our findings present differential effects of functional impairment on somatization, showing that the significant effect of functional impairment on somatic symptoms is only found among female participants. This may indicate that reporting somatic symptoms is a culturally acceptable way to express trauma-related pains among women (Lehti et al., 2009; Rometsch et al., 2020; Ventevogel & de Jong, 2020), while women and girls likely face a higher vulnerability to mental as well as physical health risks during forced migration (Hollander et al., 2011; Mohwinkel et al., 2018).
Results indicated that trauma exposure had a direct, global impact on Somali refugee youth and yet disproportionately affected functioning as well as CMD symptoms across genders. Trauma exposure directly and indirectly affected CMD symptoms among female participants but neither directly nor indirectly impacted CMD symptoms among males. This may imply a higher vulnerability among female refugees who likely experience greater trauma exposure and gender-specific reactions to trauma and have access to fewer resources for coping, corroborating previous studies on gendered mental health patterns (Kroll et al., 2010; Olff et al., 2007; Renner & Salem, 2009). Female refugees may also be more likely to self-report mental health symptoms than male refugees (Hollander et al., 2011; Mohwinkel et al., 2018; Pottie et al., 2005). Gender differences were notable in the relationship between functional impairment and somatization, which may be explained by the disproportionate pervasiveness of somatoform pains among women (Hessel et al., 2002; Hiller et al., 2006; Jacobi et al., 2004). Additionally, Somali girls commonly face female genital mutilation or cutting (United Nations International Children’s Emergency Fund, 2016), which is believed to contribute to somatic symptoms that likely reflect aggregated physical and mental health risks (Im et al., 2020; Mulongo et al., 2014; Pereda et al., 2012).
As hypothesized, substance use was a key predictor of functional impairment, aggression, and CMDs, although there were differences in these relationships based on gender. Female Somali youth who reported substance use presented with higher levels of aggression and functional impairment that led to negative mental health outcomes. Previous research has shown mixed results regarding the effect of gender on pathways from substance use to mental health. Some research (Schwinn et al., 2010) has shown little effects of gender on the relationship between substance use and mental health, while our findings corroborate other studies showing the effect of gender on this relationship (Saban et al., 2010; Schiff & Fang, 2014). Given the cultural and social norms in the Somali community, where substance use is often considered more socially acceptable for men but highly stigmatized for women (Osman & Söderbäck, 2011; Salama et al., 2018), Somali men may use substances more recreationally and casually, while tabooed use of substances among Somali women may be associated with an increased risk of substance use as self-medication, deviant behaviors and delinquency, and social marginalization (Authors, 2021; Gunn et al., 2018; Neupane & Bramness, 2014). The current study adds to this growing body of literature, implying that substance use is an indicator of higher risk for CMDs and other associated functional issues for Somali refugee women. A more nuanced approach is necessary for Somali refugee men despite the overall harmful effects of substances on mental health.
Implications
This study highlights the role of social functioning in addressing trauma-related mental health symptoms in refugee youth displaced in urban, low-resource settings. Recent studies have focused on the improvement of individual functioning through transdiagnostic psychological interventions (e.g. Problem Management Plus, Self-Help Plus). Although these scaleable interventions have made significant contributions, many are designed as gender-neutral or are aimed at women or victims of gender-based violence but are not necessarily informed by different patterns of social functioning and their mental health consequences for both genders (Akhtar et al., 2020; Dawson et al., 2015; Heim et al., 2019; Tol et al., 2020). To effectively intervene to address reduced social functioning, this study points to the need for future interventions to be informed by the divergent effects of cumulative traumas and substance use across genders in order to take a culturally nuanced and gender-sensitive approach to mental health care. Given the inequitable access to services and community resources among refugee women in low-income countries (Kohrt et al., 2018), Somali refugee women are likely more vulnerable to harmful effects of substances as well as trauma exposure, and therefore, trauma-informed prevention that incorporates social protection is necessary. For male Somali refugee youth, experiences of trauma and substance use alone may not significantly predict CMD symptoms via functional impairment or aggression, which implies that other psychosocial factors may buffer or exacerbate mental health issues as well as social functioning. Future studies could test pathways through variables such as employment, social discrimination, and other sources of distress to better understand risk and protection from mental health issues. Given the impeded social support systems during displacement, interventions that strengthen family and community support systems, as well as social and economic empowerment and protection, are critical to the mental health of urban refugee youth (Lahiri et al., 2017; Logie et al., 2020; Reed et al., 2012; Torre, 2020). Given the differential pathways to CMD symptoms, future research may consider more gender-responsive and locally grounded questions that consider sociocultural and structural challenges faced by urban refugees (Freedman, 2010). In order to further understand mental health issues in both genders, daily challenges and structural issues commonly faced by urban refugees in LMICs need to be considered in future studies, such as legal protection or documentation, livelihoods and poverty, education, social discrimination, community infrastructures, and basic social services and healthcare access (Im et al., 2017).
Limitations
These findings must be interpreted with the consideration of several study limitations. First, participants were recruited using snowball sampling since the target population is hard to reach due to their highly mobile and unstable status as urban refugees (Pavanello et al., 2010). Although this sampling strategy was unavoidable due to the lack of a complete or known sampling frame (Kim et al., 2019; Spring et al., 2003), it limits the representativeness of the study sample and the generalizability of these findings. Second, this study used a self-report survey design, in which some variables relied on single items or measures that have yet to be culturally validated (e.g. substance use, aggression, and social functioning). The questions adopted in this study allowed us to capture important information on constructs that currently lack culturally validated measures; however, it also decreases confidence in the accuracy of these findings. This study provides important information about relationships between study variables, but its cross-sectional design precludes causal inferences. Future longitudinal studies could provide causal evidence about these study variables by investigating their time order. Finally, this model does not involve sociocultural and structural factors, such as poverty, documentation or refugee status, social discrimination, and acculturative stress during displacement, which might contribute significantly to mental health outcomes as well as social functioning. In fact, several studies have revealed the mediating role of discrimination in the relationships between refugee trauma and mental health (Kira et al., 2010; Oppedal & Idsoe, 2015), while others have emphasized the importance of food security and community insecurity, as well as social support, in depressive symptoms among displaced refugees (Logie et al., 2020; Mugisha et al., 2015).
Conclusion
Female Somali refugee youth are likely more susceptible to direct harmful effects of trauma exposures and substance use, whereas male Somali refugee youth are afflicted by impeded social functioning. This is the first study examining how common adverse factors relate to low social functioning and mental health outcomes among Somali refugee youth displaced in urban, low-resource settings. Specifically, this study highlights how trauma-related CMD symptoms are differently manifested through substance use and social functioning based on gender. It sheds light on the need for gender-sensitive and culturally nuanced approaches to mental health care for this population.
Supplemental Material
sj-pdf-1-isp-10.1177_00207640211037726 – Supplemental material for Trauma exposure, social functioning, and common mental health disorders in Somali refugee male and female youth: An SEM analysis
Supplemental material, sj-pdf-1-isp-10.1177_00207640211037726 for Trauma exposure, social functioning, and common mental health disorders in Somali refugee male and female youth: An SEM analysis by Hyojin Im and Laura ET Swan in International Journal of Social Psychiatry
Footnotes
Acknowledgements
The authors wish to thank Somali refugee community leaders and study participants in Eastleigh, Kenya. This study is indebted to Tawakal Medical Centre (TMC).
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This study was approved by IRB approval from the authors’ institution. In addition, the research protocol and materials were reviewed and approved by a locally formed community ethics committee that comprises of Somali community leaders and medical professionals. All procedures performed in this study were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first half of the data collection was supported by the Kenya Transitional Initiative, USAID (CHXEAS053).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.