
Abstract
Objective:
This study looked at the bright and dark-side personality profile of distressed and potentially derailing doctors (82% male). The derailing doctors were on average 48.75 years old, and from many specialities, in particular, general practice and surgery.
Method:
In all, a group of 77 derailing British doctors, and a control group of 357 doctors completed a valid multi-dimensional test of bright-side (normal) personality (NEO-PI-R) and one of dysfunctional interpersonal themes (sub-clinical personality disorders) (HDS: Hogan Development Survey).
Results:
Controlling for sex and age, the derailing doctors were more Neurotic (less resilient), and less Agreeable, Conscientious, Extraverted and Open-to- Experience. They were also more Excitable (Borderline), Sceptical (Paranoid), Cautious (Avoidant), Reserved (Schizoid), Leisurely (Passive Aggressive) and Bold (Narcissistic). Discriminant analysis showed age, Neuroticism, Extraversion, Leisurely and Excitable were, in that order, the greatest personality discriminators between those who did and did not derail.
Conclusion:
More research needs to be done on doctor derailment to inform the selection and training of doctors.
Introduction
There is a growing literature on the mental and physical health of doctors (Kay et al., 2008). There is also a research literature on doctors with mental health problems (Bogacheva et al., 2019; Gerada, 2017; Hohaus & Berah, 1985; Miller & Surtees, 1991; Myers & Gabbard, 2008). Numerous studies on doctors have shown they have distinct personality profiles. Thus, Lovejoy and Nashef (2018) reviewed many studies that consistently showed that surgeons have lower Neuroticism as well as higher trait Conscientiousness, Openness and Extraversion scores compared to the general population norms. This is important research for both the selection, education and management of doctors (Bisset et al., 2020).
The behaviour of doctors in the workplace has resulted in various research studies (Cox et al., 2006). Many of the studies are based on survey work such as that of Weber (2004) who had over 1,600 members of the American College of Physician Executive report on doctors’ disruptive behaviours. They noted that the problems were often caused by the same doctor with repeating bad behaviour and that it was only reported when they were ‘completely out of line and a serious violation occurs’ (p. 12). The question is whether these disruptive behaviours are a function of health, mental health or moral issues.
There are also several papers on the selection of medical students including systematic reviews (Nei et al., 2017; Patterson et al., 2016). A few are directly relevant to this paper which was concerned with both normal personality, but also subclinical personality disorder traits, of distressed doctors. Knights and Kennedy (2006) used the Hogan Development Survey (HDS), a measure of dysfunctional personality characteristics, to see if it could detect relevant traits. They found that many students had elevated scores on the dysfunctional patterns that were not detected by interviews. They found 10.7% of students reported an extreme tendency towards aggressive, self-promoting behaviour which they suggest might lead them to engage in abuse of other students or patients, or to engage in cheating or other unethical conduct. Also, around a third had scores which indicated that they were picky, critical and stubborn, as well as unwilling to delegate due to obsessional perfectionistic tendencies. This study used this measure to understand derailing doctors.
Pegrum and Pearce (2015) argued that most medical jobs are highly stressful and that, as a consequence it is not ‘surprising that some traits associated with a psychopathic personality (preternatural calmness under pressure, or apparent indifference to human suffering when making life-or-death decisions) are perhaps selected out in those who rise to the top of our profession’ (p. 322). In a paper subtitled ‘Are surgeons psychpaths?’ they demonstrated surgeons and paediatricians had significantly higher than population norms on psychopathic traits, particularly stress immunity. They suggest that these traits may be self-protective for many in the medical profession.
Whilst there is an increasing number of studies on business managers and leaders who derail there are relatively few concerning doctors (Furnham, 2008, 2018, 2021, 2022). The results suggest that fairly consistently two traits relate most to work success: low Neuroticism and high Conscientiousness. Neurotics (those less resilient) are prone to stress, illness and often poor decision making; Conscientious people are well organised, planful and hardworking. Equally those high on Neuroticism and low on Conscientiousness are associated with failure and derailment.
For the other three Big Five personality factors much depends on the nature of the job. Thus, in some jobs Agreeableness is positively correlated with work success (counselling) whereas in others it is negatively correlated (negotiations). Given the nature of medicine, particularly in relation to how doctors relate to patients and how they work in multi-disciplinary teams, it may be expected that derailment is associated with low Agreeableness. The same is true of Extraversion, which is usually correlated with work success, because of the optimism and social skills associated with relationship building, though it is obvious that in some jobs (pilot, air traffic controller) it may be Introversion which is a best predictor. For doctors the benefits of Extraversion may well depend on speciality: for example in General Practice (although not exclusively) where the ability to put the patient at ease and create a trusting relationship quickly is likely to be important in the effectiveness of the consultation.
Openness is usually correlated with job success as is intellectual curiosity and adaptability. Clearly with a great amount of change and progress in medicine, it may be assumed that Openness would predict success in medicine. Given the results in this area it was predicted that, compared to the control group, the derailing doctors would be more Neurotic (H1), but less Extraverted (H2), Open (H3) Agreeable (H4) and Conscientious (H5).
There is a large and growing literature on what psychologists have called the dark-side traits and psychiatrists the personality disorders. The measurement of the former have been pioneered by the measure used in this study: the HDS (Hogan & Hogan, 1997). The relationship between the classic psychiatric nomenclature and the HDS is shown in Table 1
The DSM IV and the HDS.
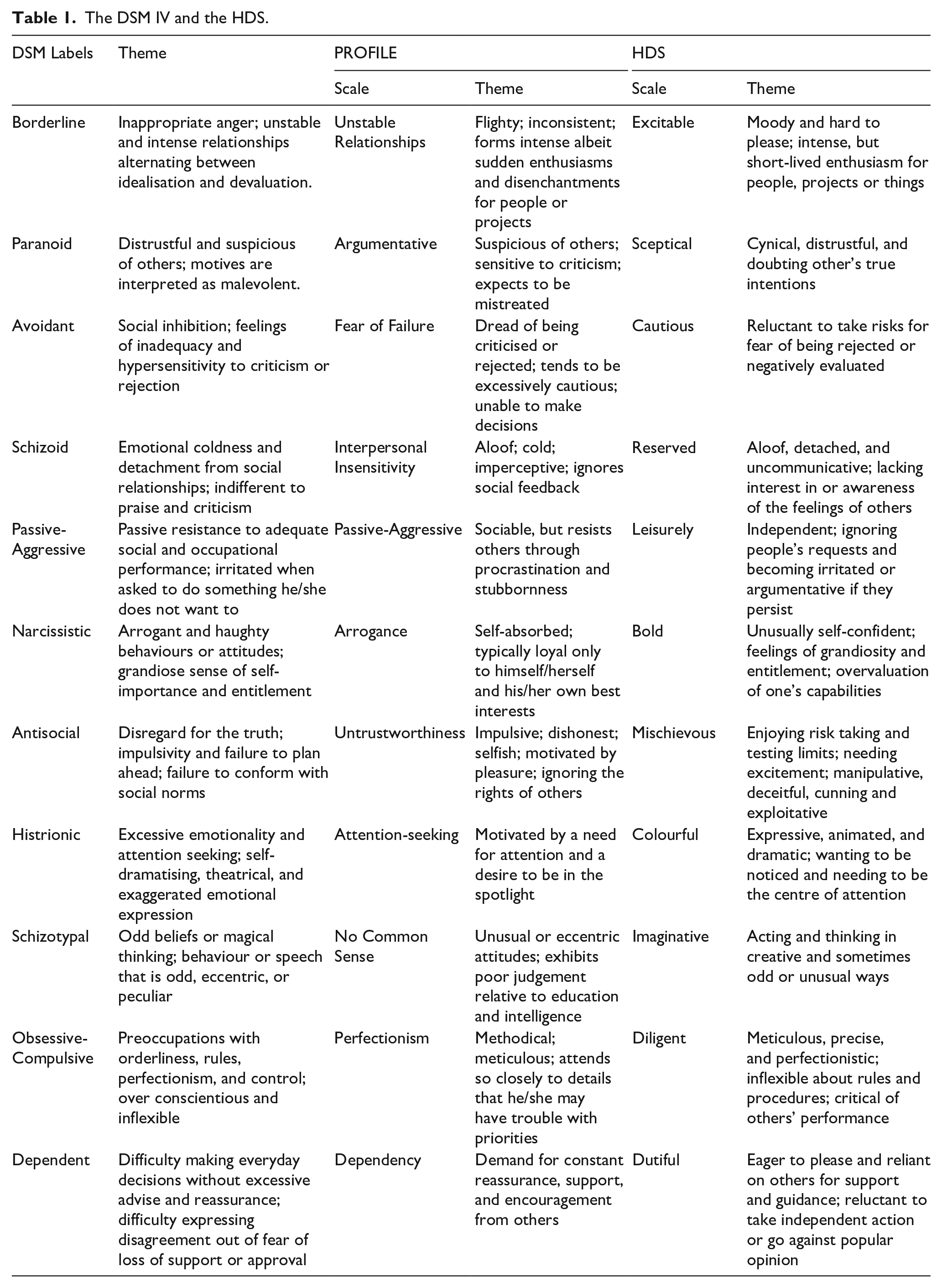
There are fewer, but yet still a growing number of studies on the Dark-Side (sub-clinical personality disorders) correlates of failure at work (Furnham & Sherman, 2021). Many have pointed out the paradox that dark-side personality traits appear to be associated with short term success but long-term failure in the workplace (Furnham, 2022). For instance, Davies (2004) found that transformational leadership had a negative relation with Excitable, Sceptical, Cautious, Reserved, Leisurely and Dutiful but a positive relation with Colourful and Imaginative traits. Benson and Campbell (2007) found that leader performance was negatively related with high scores on Excitable, Sceptical, Cautious, Leisurely, Mischievous and Imaginative.
Traditionally the personality disorders have been classified into three clusters: A (Odd and Eccentric); B (Dramatic, Emotional and Erratic) and C (Anxious and fearful). Similarly the eleven HDS dark-side traits can be both theoretically grouped or factored into Karen Horney’s theory which proposed three ways of managing interpersonal anxiety: Moving Away (Cluster A) (i.e. detaching and withdrawing from others), Moving Against (Cluster B) (i.e. influencing and charming others) and Moving Towards (Cluster C) (i.e. obeying and getting close to others).
The literature on leadership derailment is dominated by the HDS which is used to explain and predict it. There are now probably 50 studies that have showed how these dark traits, particularly those from the Moving Against cluster (Anti-Social, Narcissistic, Histrionic, Schizotypal) are clearly and logically related to various markers of failure (Furnham, 2022).
Doctors are expected to exercise clinical and medical leadership defined in a competence framework (https://www.leadershipacademy.nhs.uk/wpcontent/uploads/2012/11/NHSLeadership-Leadership-Framework-Medical-Leadership-Competency-Framework3rded.pdf/ https://www.leadershipacademy.nhs.uk/resources/healthcare-leadership-model/structure-healthcare-leadership-model/).
The aim of this study was to identify bright-side (normal) and dark-side (dysfunctional) characteristics of qualified doctors who had been identified over time by a number of different sources as derailing. The same has been done for business leaders but much less work has been done on doctors (Furnham, 2021). Given the previous literature our hypothesis is that derailed doctors would score highly on all Cluster A, but lower on Cluster B traits (H6).
Method
Participants
There were two groups of doctors:
The derailed group who were referred by their Chief Medical Officer/Medical Director as someone who is in difficulty and might benefit from a behavioural assessment and/or coaching. They were referred to the first and third author, certified psychologists and undertook a number of sessions. The individuals complete a set of psychometric tests as a result of the referral and as part of the process. In this group there were 72 males and 16 females with an average age of 48.75.
The control group were medical consultants applying for jobs in hospitals – they apply for a job advertised and as part of the selection process are required to complete the same three tests. They were classified into successful and unsuccessful: those who are successful were offered a job. In this group there were 216 males and 141 females with an average age of 41.32.
Both groups did the tests on-line and received full feedback. This was done over a number of years and collected before the Covid-19 crisis. This study was given ethical approval by the appropriate ethics committee: CEHP/2017/514. Participants gave consent for their anonymised data to be used in academic research.
Tests
Bright Side, ‘Normal’ Personality. The NEO Personality Inventory-Revised (NEO-PI-R; Costa & McCrae, 1992 ). This 240-item, non-timed questionnaire measures 30 primary personality traits (facets) and the underlying ‘Big Five’ personality factors (domains), that is, Neuroticism, Extraversion, Openness-to-Experience, Agreeableness and Conscientiousness. Items involve questions about typical behaviours or reactions, which are answered on a five-point Likert scale, ranging from ‘strongly disagree’ to ‘strongly agree’. The manual shows impressive indices of reliability and validity.
Dark Side Traits. Hogan Development Survey (HDS; Hogan & Hogan, 1997) is a measure of the personality disorders expressed in non-clinical language. The survey includes 154 items, scored for 11 scales, each grouping 14 items. Respondents are requested to ‘agree’ or ‘disagree’ with the items. The HDS has been cross-validated with the MMPI personality disorder scales. It has considerable evidence of satisfactory reliability and validity (Hogan & Hogan, 2001). Furnham (2022) show the overlap of the HDS and DSM-IV disorder terminology. The HDS assesses dysfunctional interpersonal themes. It is argued that these dysfunctional dispositions reflect distorted beliefs about others that emerge when people encounter stress or stop considering how their actions affect others. Over time, these dispositions may become associated with a person’s reputation and can impede job performance and career success. The HDS assesses self-defeating expressions of normal personality.
Results
Table 2 shows the correlations between all the variables. The size and directions of the correlations is very similar to those in other studies using these tests.
Bivariate correlations across all study variables with both groups combined.

The next analysis concerned examining bright and dark-side personality differences between the two groups. A MANCOVA controlling for age and sex was first done on the Bright Side (Table 2) and then the Dark-Side (Table 3) variables.
Big Five means and standard deviations for experimental and control group.
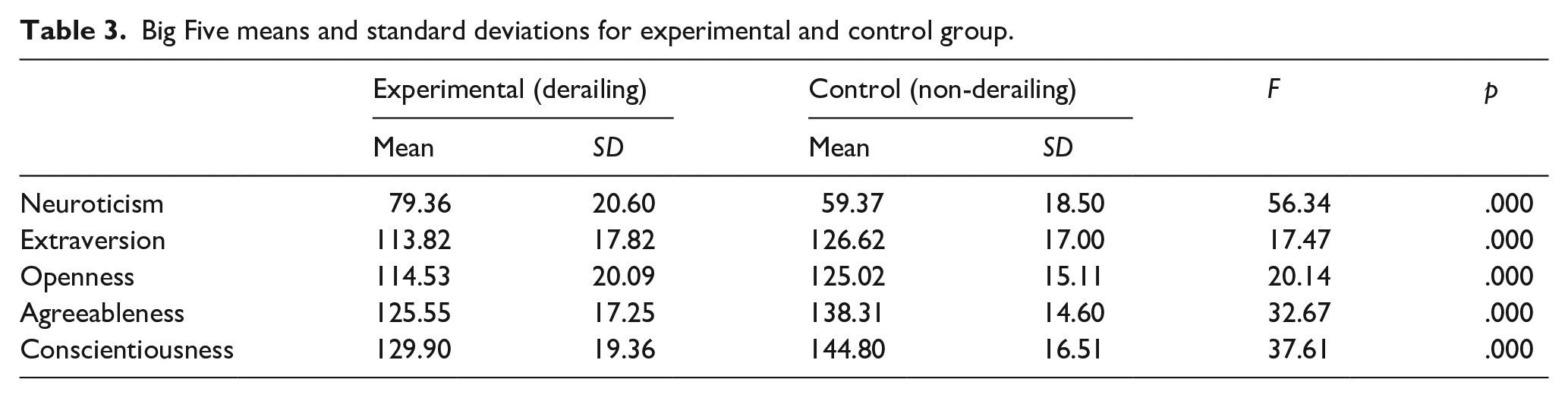
Table 3 shows the results for the analysis of the Bright-Side traits which was significant: Wilks’ Lambda = .831, p = .000, Partial Eta squared = .169. The Derailed doctors were higher on Neuroticism but lower on the other four traits, particularly Conscientiousness and Agreeableness. This is the typical profile of managerial failure and derailment. This confirms H1 to H5.
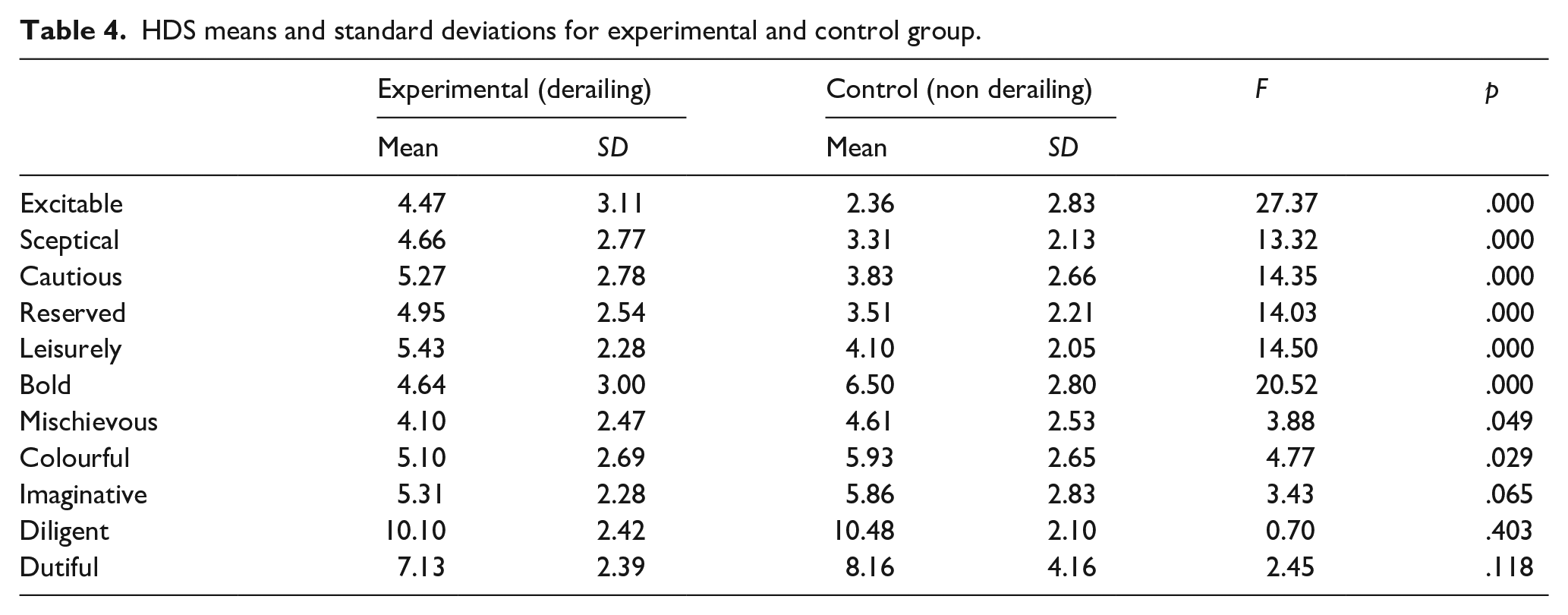
Table 4 shows the results for the analysis of the Dark-Side traits which was also significant: Wilks’ Lambda = .851, p = .000, Partial Eta squared = .149. With one exception, all the Cluster A (Moving Away) and Cluster B (Moving Against) disorders, but not Cluster C (Moving Towards) disorders, showed significant differences. As predicted the derailed doctors scored higher on Cluster A but lower on Cluster B traits. This confirms H6.
HDS means and standard deviations for experimental and control group.
Finally, a discriminant analysis was performed (see Table 5). The objective of discriminant analysis is to develop discriminant functions that are the linear combination of independent variables that will discriminate between the categories of the dependent variable in a perfect manner. This was significant. In all 89.4% of original grouped cases correctly classified: 96.4% of the control group and 57.1% of the experimental group were correctly classified. There was one single factor shown in Table 5. Discriminant analysis revealed the items which showed most differences in the response between the two groups.
Rank ordered factors that discriminate between derailed group and control group.
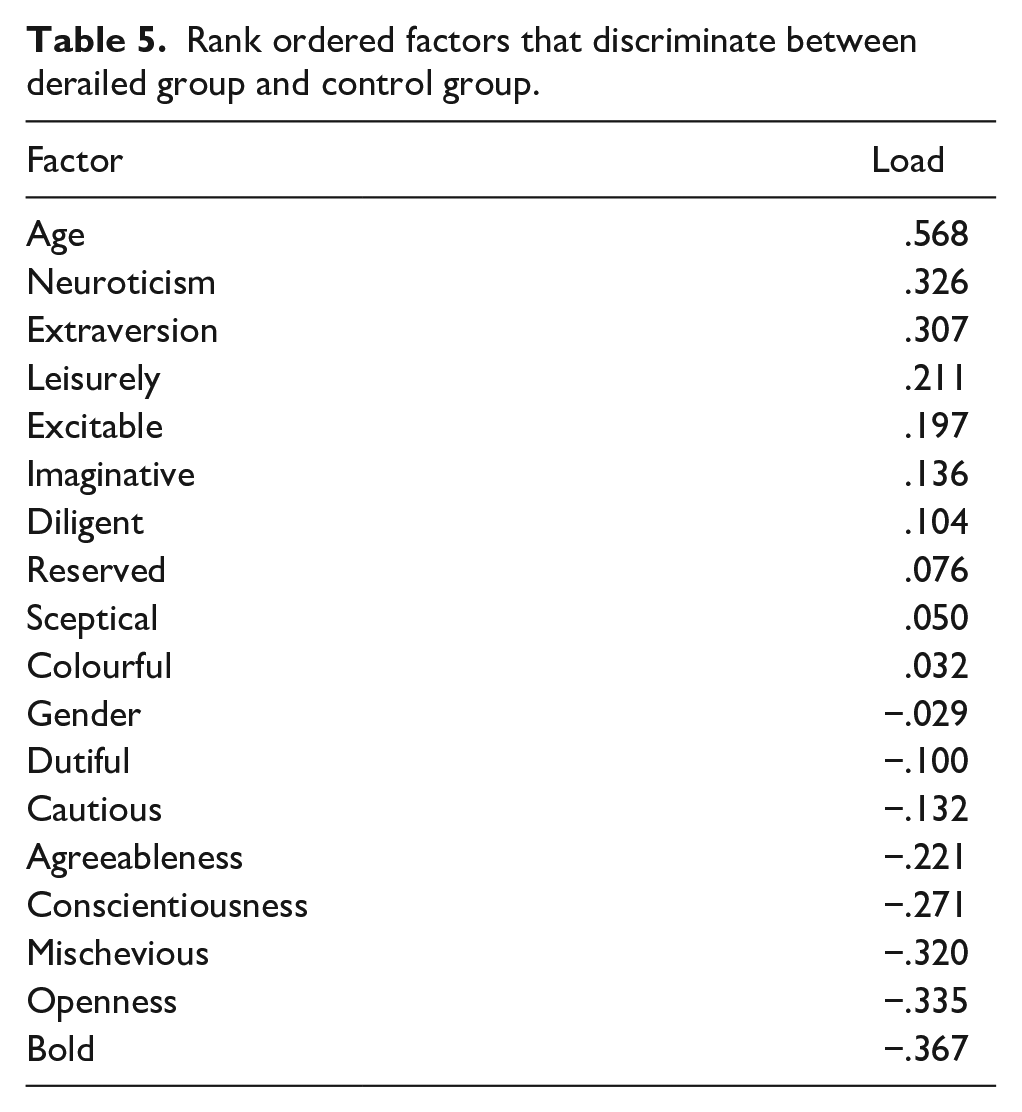
The results of the discriminant analysis showed that after age, two bright-side and two dark-side personality factors clearly differentiated between the two groups. The derailing doctors were more likely to be Melancholic, namely Unstable Intraverts. They were also likely to be Passive Aggressive (i.e. Leisurely) and Borderline (Excitable).
Discussion
This study confirms the extensive literature in personality and work psychology on the profile of derailing and failed leaders. The growing literature on the Big Five suggests that successful people are low on Neuroticism but high on the other traits, particularly Conscientiousness. The results from this study (see Table 4) show that derailing doctors demonstrate the opposite personality profile, compared to a large group of functioning doctors.
The bright-side, personality results of the current study suggest that the derailing doctors are more Neurotic, that is less resilient and proficient at coping with pressure, and more socially reserved than others (low Extraversion) and therefore not as naturally inclined to engage or relate easily with their colleagues as they need to in a multi-disciplinary context. The high Neuroticism result suggests that derailing doctors are more vulnerable to experiencing pressure and stress reactions. They have lower resilience and are prone to anxiety, depression and psychosomatic disorders. This may manifest in the workplace as anxiety about decisions and frustration with others or the system and a propensity to resistance to critical feedback.
As the results show them to have a stronger propensity for introversion than extraversion it may be that their feelings of stress (i.e. anxiety, hostility, depression) are internalised perhaps affecting their health and wellbeing. The low Extraversion may be evident in them not readily explaining their thought processes and decision-making to other team members or to patients; and their discomfort in engaging easily in team conversation which could result in them being personally and professionally isolated. It is also possible that such individuals prefer a slower pace of working, sometimes leading to frustration on the part of other colleagues in a busy work setting.
Similarly, the data on the dark-side traits indicates that derailing managers tend to be higher on Clusters A and B (Moving Away from and Against others) and lower on Cluster C (Moving Towards) others. This study showed the derailing doctors were, compared to the control group, higher on Cluster A (Moving Away) but lower on Cluster B (Moving Against). Moving Away (Cluster A) behaviours play out in workplace difficulties associated with team working, and, seeking and accepting feedback and help, all of which are at the core of providing safe and effective patient care. Lower Moving Against (Cluster B) behaviours have similar implications but they also suggest that these individuals may be less socially skilled. Being Bold (Narcissistic) or confident is helpful and, arguably, necessary, for a surgeon, for example, ‘to put knife to skin’. When this confidence is manifested as overconfidence or arrogance, entitlement and fantasised talent it is counterproductive. It may mean that they take on tasks/activities that push the boundaries of innovation but which may simultaneously be highly risky to patients, or that they don’t listen to challenge and that they have unrealistic expectations of others in terms of expected deference and compliance. The results also reflect a dilemma for doctors who in relation to clinical leadership might need to be more Colourful (Histrionic) and Imaginative (Schizotypal) (both Moving Against behaviours) to create alignment in their team but in contrast need to be Cautious (Avoidant), Leisurely (Passive Aggressive) Moving Away behaviours) in relation to patient care.
Other bright-side factor results, that is less Agreeable, Conscientious, and Open to Experience have further implications for how easy the derailing population are to get along with, their work ethic and their willingness to consider difference and diversity of opinion and perspective. Less Agreeable doctors may be seen to be less emotionally intelligent and less caring. Further, it may be difficult to deal with doctors low on Conscientiousness because of their lower work ethic, and organisational skills
Additionally, their inclinations, under pressure, towards volatility (Excitable), cynicism and lack of trust in others (Scepticism), independence (Leisurely) may make it still more difficult for them to work comfortably with others and to seek and receive help and support, and to adapt to changing organisational contexts and demands. The Excitable (Borderline) domain (unpredictable/volatile) may result in others becoming wary of them and can negatively affect their willingness to challenge the derailing doctor, with potentially serious implications for both patient care and clinical leadership.
A question, and oft encountered challenge, is whether the distressed doctors are ‘melancholic’ (i.e. high Neuroticism) as a result of their referral; how they perceive themselves to have been treated (i.e. typically perceived to be unfairly), and the implications of their referral for their future career, or whether this is, indeed, a natural disposition (Pendleton et al., 2021). Very few doctors in the experimental/derailing group willingly volunteer to be assessed, although in the case of the control group the assessment is increasingly accepted as part of the recruitment process. In the case of the experimental group a fairly regular outcome of the assessment (of which the psychometric profiles only form a part) is that the doctor lacks insight which may be associated with low Openness especially, Openness to ideas, and Openness to values as many tend to attribute their problems to others (the team), to over-use of authority by medical management, and to unfairness; and they tend to show little, if any, curiosity about their own contribution to the concerns raised about them.
Many organisations concerned with the possibility of management and leadership failure and derailment have used ‘screen out’ measures like the HDS to ‘flag up’ the possibility of later problems (Furnham, 2018). This is because there is a growing literature on the topic and calls for attempting to address problems of derailment at the selection phase or in the developmental processes, for the sake of colleagues and clients of those prone to stress-related dysfunctional responses (Furnham, 2022). The emotional and financial cost to the organisation (hospital, practice) as well as to colleagues and patients means that investment on sensitive and successful screening is thought to be very important and a good investment.
Like all others this study had limitations. Some might argue the possibility of test scores being influenced by circumstance (i.e. the participants are likely to be feeling depressed or anxious etc, because they are in difficulty, rather than vice versa). The extensive data on test-retest reliability as well as the stability of personality over time suggests this is very unlikely or at best a very minor effect. There is also the ever-present concern about faking, dissimulation and impression management. Whilst this does occur and may in this instance be thought to occur more with the derailing doctors it would mean that the difference between the groups would be reduced, rather than enhanced by faking. In other words, any differences found may in fact indicate important and fundamental indicators of derailing doctors.
Finally, the experimental/derailing group was a small population, and the results may not generalise to the wider medical profession, but they nevertheless offer lines of inquiry for further research for example, researching speciality specific data.