
Abstract
Background:
COVID-19 pandemic has affected all crucial aspects of daily life, including; food security, education, gender relation, mental health, and environmental air pollution, in addition to the impact of the lockdown that had far-reaching effects in different strata of life.
Aims:
To study the impact of COVID-19 on people with respect to their mental and social suffering and consequences.
Methods:
This cross sectional study was conducted during the period from November 2020 through August 2021. A sample of 1,000 attendants to four teaching hospitals and eight PHCCs, was collected. The mental and social sequels of COVID-19 were assessed for all participants whether previously infected or not.
Results:
Out of the total sample (1,000), 389 had a history of infection with COVID-19. The main mental symptoms reported were depression (67.8%), and anxiety (46.9%), males and females equally reported symptoms of anxiety, while depressive symptoms were reported more among females (59.9%), Fear and worries of the participants about their health and their families’ was the main reason for mental symptoms (94.7%).
Conclusions:
Symptoms of depression and anxiety in time of COVID-19 are prevalent. Suspending educational activities was the most social burden that affect people while increase the price of food and cessation of work were the main causes of economic burden.
Introduction
Coronavirus disease (COVID-19), which is a contagious viral infection mainly of the respiratory system, and can infect the intestine, has flared up progressively, and was declared by WHO in March 11, 2020 as a pandemic (WHO, 2020a) that represents an unprecedented challenge to global health, never experienced before (Khan et al., 2021). It has increasingly spread across the world due to its high transmissibility, high population mobility and no herd immunity, creating a real dilemma for global health (Ibrahim et al., 2021).
The pandemic affected all crucial aspects of daily life, including; food security, global economy, education, tourism, gender relation, and mental health. However, the impact of the lockdown has had far-reaching effects in different aspects of life, including; changes in the accessibility of education delivery to students, food insecurity (as a result of unavailability and fluctuation in prices), increase in mental health challenges, wellbeing and quality of life (Bhowmik et al., 2021; Onyeaka et al., 2021), in addition to many other massive adverse impacts on the whole globe (Hu et al., 2021).
COVID-19 infects people of all ages, however, recent studies showed that older people (over 60 years), and those with underlying medical conditions such as cardiovascular disease, diabetes, chronic respiratory disease, hepatic dysfunction and cancer, are at a higher risk of getting severe disease (WHO, 2020a, 2020b). Children might be less likely to become infected, even though, they may show milder symptoms or asymptomatic infections (Velavan & Meyer, 2020). The most common clinical symptoms are fever, dry cough, shortness of breath, loss of smell and taste, in addition to other nonspecific symptoms, including headache, fatigue, and myalgia (Chen et al., 2021; Ibrahim et al., 2021).
The psychological impact of COVID-19 pandemic must be recognized for all those affected or even those not affected. Mental symptoms have already been observed on a population level including anxiety and paranoia about attending social events. Students, workers, and tourists who have been prevented from accessing their training institutions, workplaces, and homes, are expected to develop mental symptoms due to stress and reduced self-sufficiency and concerns about job, and security (Lai et al., 2020). On the other hand, high levels of anxiety are mostly among adolescents, making them an especially vulnerable group to develop mental health problems like worries about becoming infected, fear of dying, and fear of the unknown (Saddik et al., 2021), they may also have changes in their mood and become more aggressive (Lafta et al., 2021).
More than 2,110,000 Iraqis have contracted the novel coronavirus till mid-January 2022, with two peaks; August to October 2020, and March to July 2021, and 24,250 deaths (Reuters Staff, 2021; COVID-19 Map-Johns Hopkins). The actual number of cases and deaths is definitely more than the official figures, which are based on limited testing and poor data systems (Al-Saiedi & Haddad, 2021).
This survey was set to study the impact of COVID-19 on people with respect to their mental and social suffering and consequences.
Methods
This cross sectional study has been implemented during the period from November 2020 through August 2021, the sample was collected from the attendants of four teaching hospitals and eight PHCCs, on both sides of Baghdad city. These facilities were randomly selected through a simple random sampling technique. We could not do a general population (house to house) survey because of the strict curfew that was imposed by the authorities. A sample of 1,000 attendant to the outpatient clinics of the targeted health facilities was collected, they were not patients, but-mostly-companions of the patients, or visitors seeking other services like vaccination of their children. A systematic random sampling technique was adopted by standing at the main gate of the clinic and taking every other attendant, which means that the denominator was double the sample size or a bit more. Only those who were willing to participate were included in the study.
- Compliance with health authority instructions like adherence to curfew, avoid crowding, compliance with personal hygiene, wearing personal protective tools, and history of contact and quarantine.
- The mental sequels of COVID-19 like anxiety, depression, fear and insomnia, mainly related to the disease or to the lockdown, this was for all participants whether previously infected or not. The questionnaire was borrowed from the ‘Patient Health Questionnaire Anxiety and Depression Scale (PHQ-ADS)’ (Kroenke et al., 2016). Anxiety among adults was measured using the Generalized Anxiety Disorder Scale (GAD-7), which is a self-reported 7-item validated Likert-scale. Participants indicated how often they were bothered during the previous 2 weeks by symptoms of feeling nervous, not being able to stop worrying, worrying about different things, trouble relaxing, restless, irritable and afraid that something awful might happen. Response options were: ‘not at all’ scored (0), several days (1), more than half the days (2), and nearly every day, scored (3), and was interpreted as follows: normal (0–4), mild (5–9), moderate (10–14), and severe (15–21). A cut-off score of 8 was used, indicating a diagnosis of anxiety (on symptomatic basis).
The Brief Patient Health Questionnaire (PHQ-9) depression scale assesses depressive symptoms’ severity over the past 2 weeks on a 4-point severity Likert-scale: 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). Total scores range between 0 and 27. The total score was calculated for each patient and interpreted as: minimal (1–4), mild (5–9), moderate (10–14), moderately severe (15–21), and severe (20–27). A standard cutoff score of 10 was used, indicating a diagnosis of depression (on symptomatic basis).
- The socioeconomic effect of COVID-19 pandemic on people such as social isolation or loss of family income (also for all participants).
After taking the verbal consent of the participants for the anonymous interview, they were assured that all information they give will be kept strictly confidential in a safe storeroom and would not be used by anyone other than the researcher and for any purpose other than research work.
Results
A total number of 1,000 respondents was collected with a response rate of 95%. Table 1 shows the distribution according to age groups, gender, employment, and residence. More than half of the sample (50.2%) were among the age group (30–49) years, 59.4% were females, and 22% governmental employees. The history of infection was significantly associated with respondent’s age, adherence to curfew, constraining social isolation, and avoiding crowding and social contact especially during holidays.
Association between age, gender and compliance to health authority’s instruction and history of infection with COVID 19.
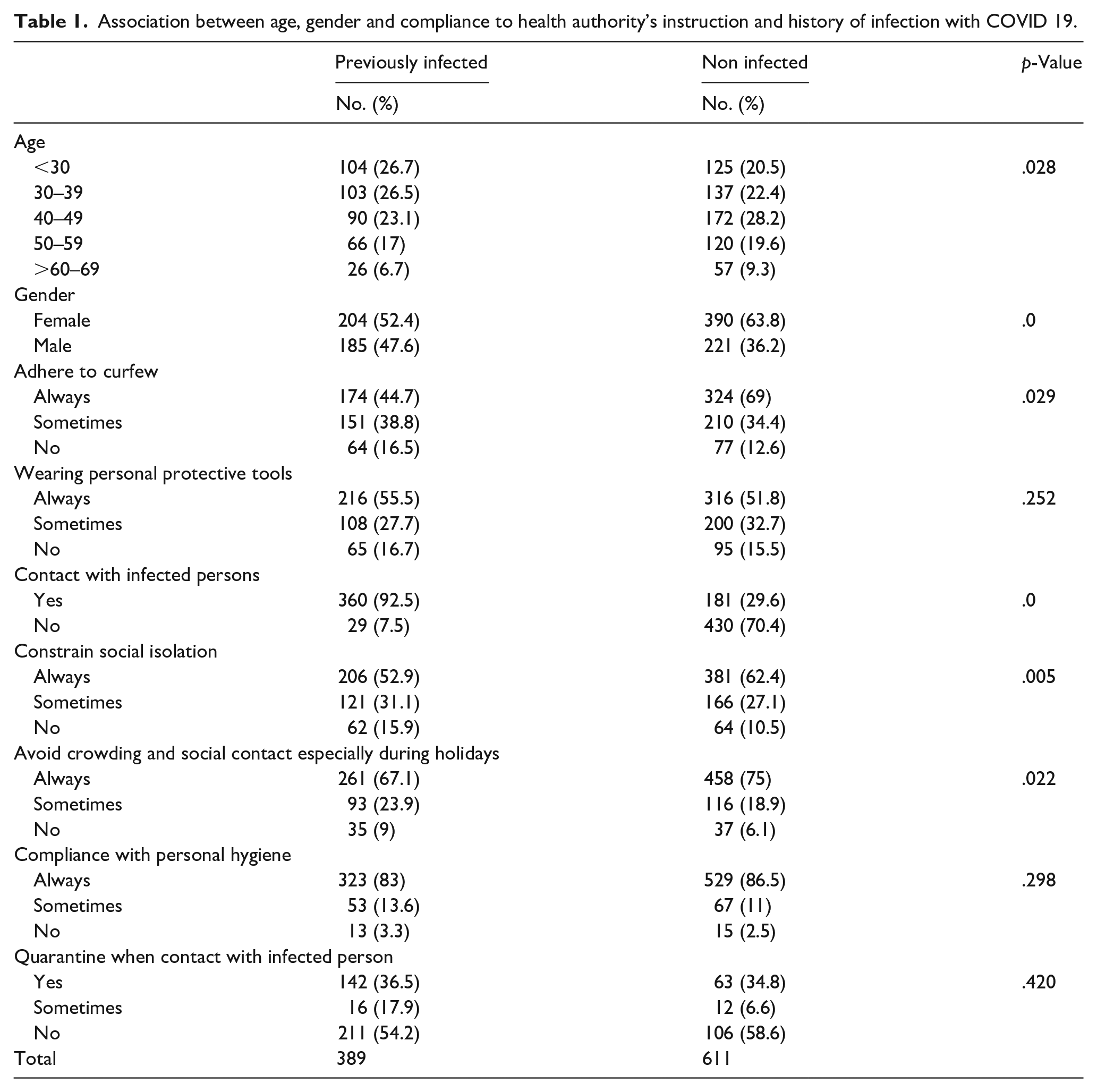
Figure 1 demonstrates the types of mental symptoms reported by the respondents during the pandemic, 40% had anxiety, 34% fear, and 27% reported having depression. Moderate type of anxiety symptoms (49%) and of depression symptoms (45.6%) were the most common (Figure 2).

Mental symptoms reported by the respondents attributed to COVID 19 pandemic (there is an overlapping).
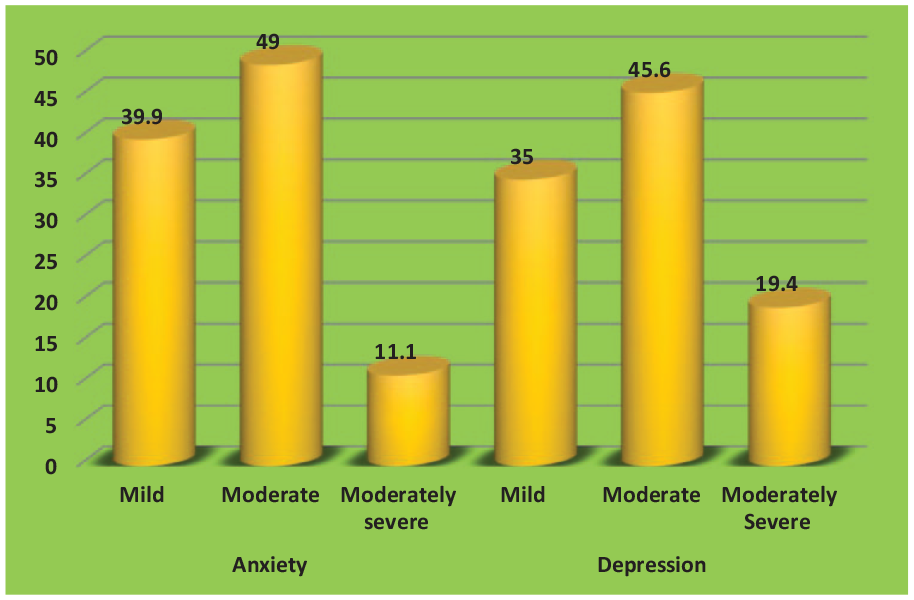
Anxiety and depression by severity.
Table 2 illustrates that males and females equally reported symptoms of anxiety, mainly among the age group (30–49) years (51%), while depressive symptoms were reported more among females (59.9%), in the same age group, 53.5% of those reported having fear were females, mostly in the age group (40–49) years, and 51.3% of those reported insomnia were females, mostly under 30 years of age. Fear and worries of the participants about their health and their families’ was the main reason for their mental symptoms (94.7%) (Table 3).
Distribution of mental symptoms by age and gender.
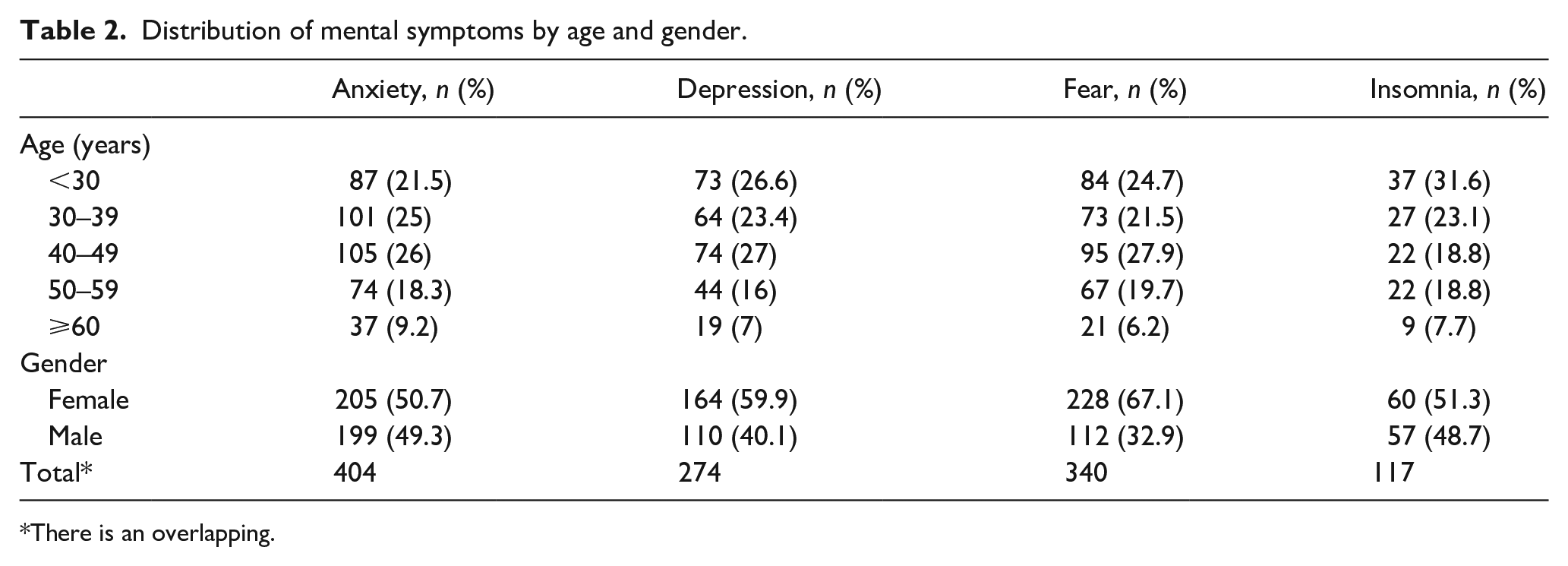
There is an overlapping.
Reasons behind mental symptoms-reported by respondents (n = 850).
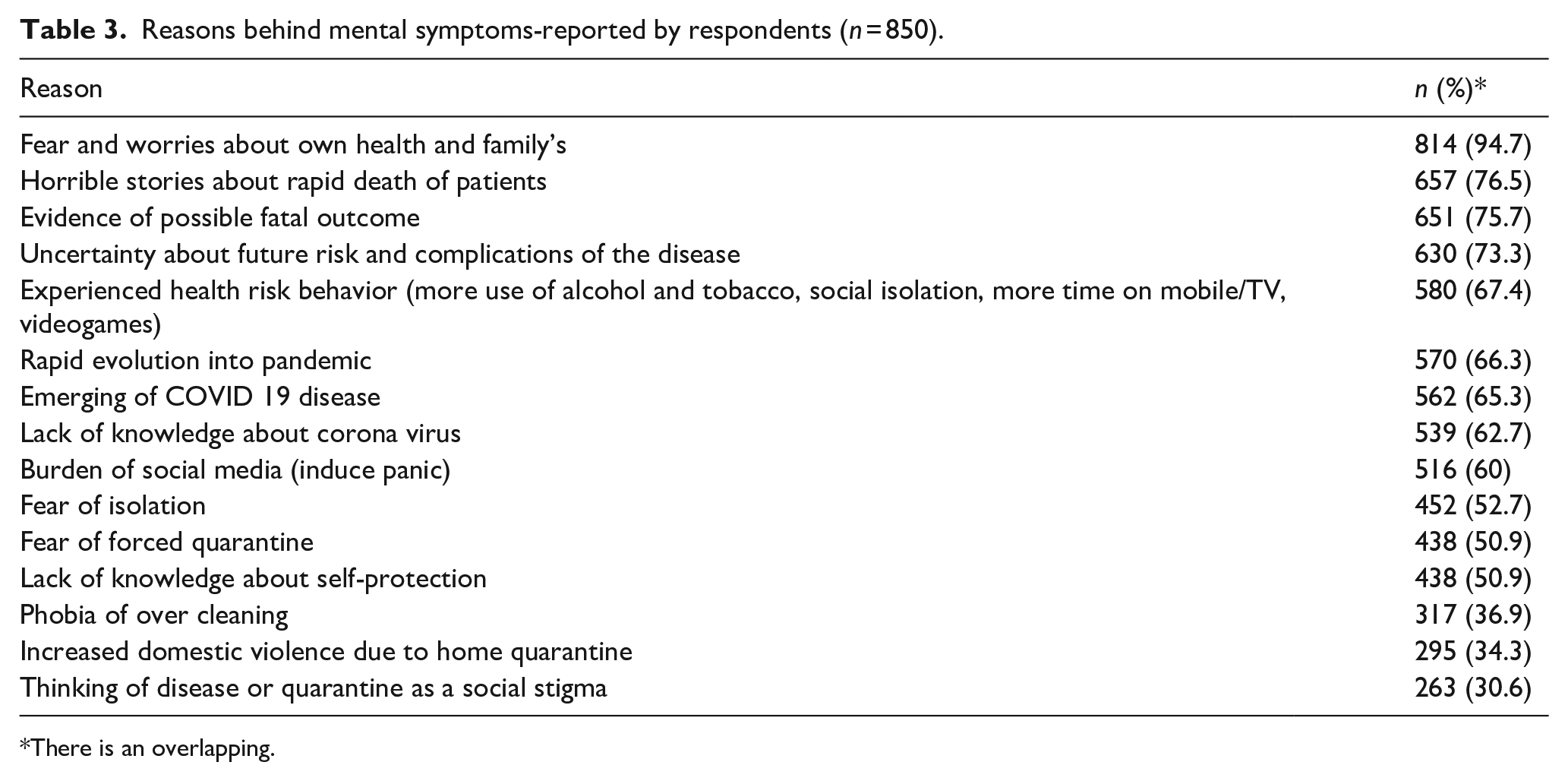
There is an overlapping.
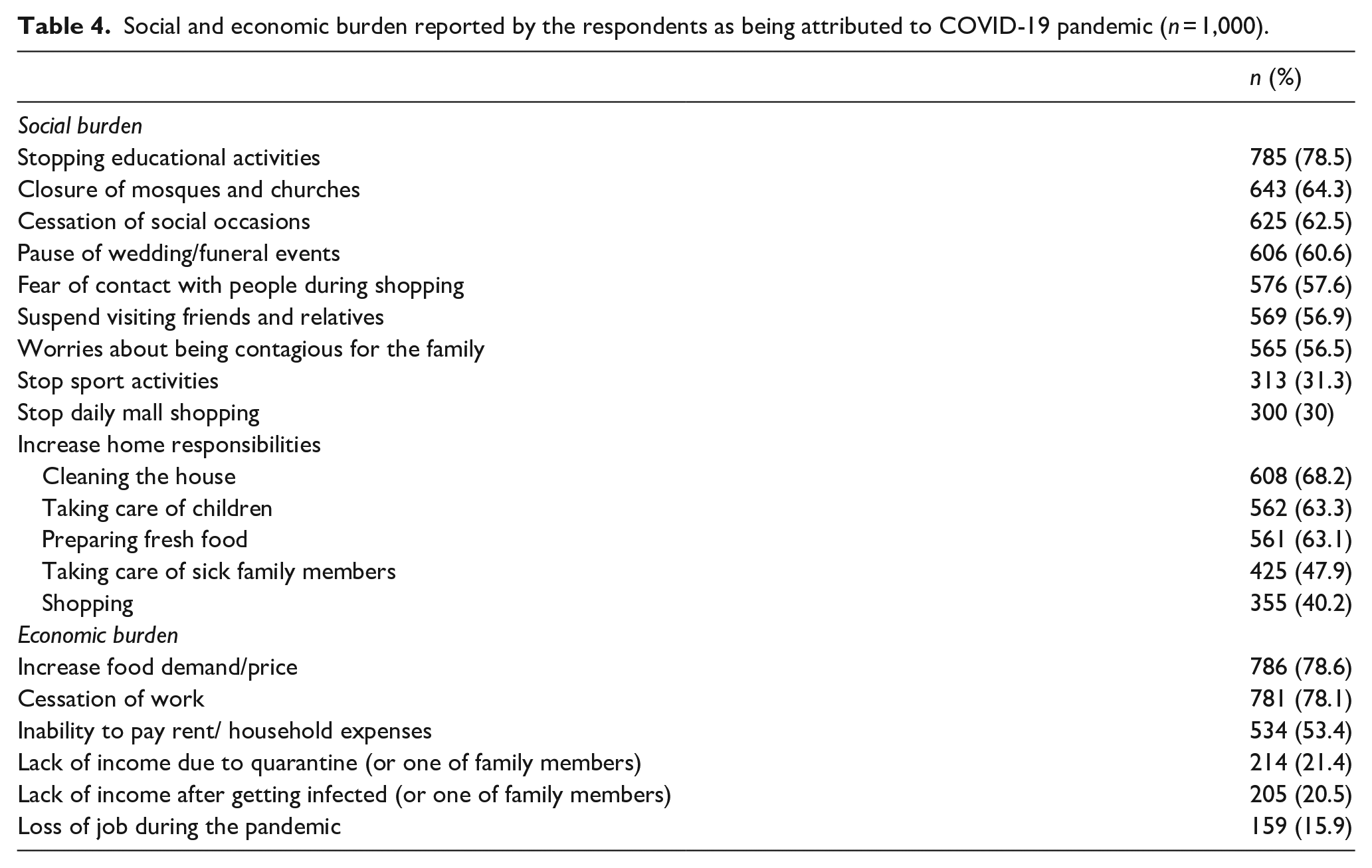
Table 4 reveals that stopping educational activities was the most social burden (78.5%), while cleaning the house was the main burden among increased home responsibilities (68.2%). The participants complained of increase food demand/price (78.6%) and cessation of work (78%), while 53.4% reported inability to pay the rent of the house.
Social and economic burden reported by the respondents as being attributed to COVID-19 pandemic (n = 1,000).
Discussion
The results revealed that about two third of the participants were females, in the age group (30–49) years, and more than one third were housewives; this could be explained by that most of the hospitals and PHCCs visitors are females as males are mostly at work in the morning.
Nearly half of the participants follow the health authority’s instructions regarding curfew and wearing masks to lessen the risk of infection. This goes with a previous study in Greece (Eleni et al., 2020). Personal protective equipment have become an important and emotive tool during the pandemic as it is a respiratory tract infection, predominantly transmitted by contact or droplets (Cook, 2020).
Testing the association between variables revealed that getting infection was significantly associated with respondent’s age, adherence to curfew, constraining social isolation, and avoiding crowding and social contact especially during holidays. A study in U.S (Canning et al., 2020), concluded that old age was one of the risk factors for disease severity and mortality in viral infection studies. SARS, MERS, and COVID-19 are all more severe in aged patients (Channappanavar & Perlman, 2020). However, in this study, there was no significant association between age or gender with the degree of anxiety or depression, this disagrees with other studies (in Ireland and China) where anxiety and depression were significantly associated with being younger, female, and experiencing a loss of income due to the pandemic (Huang & Zhao, 2020; Hyland et al., 2020).
More than 400 of the respondents reported having anxiety, more than one third developed fear, and one third developed depressive symptoms; these relatively high levels are expected in terms of pandemic psychological effects. There is evidence that the severity of COVID-19 pandemic and the high mortality rate aggravated the mental health of individuals (Le & Nguyen, 2021). The prevalence of depression was comparable to that reported in other countries such as Kuwait (30.13%) (Burhamah et al., 2020), and Turkey (23.6%) (Özdin & Özdin, 2020) The prevalence of anxiety also goes in line with both studies.
The percentage of fear in the current study was similar to Parlapani study in Greece (35.7%) (Parlapani et al., 2020). People’s fear of the unknown nature of the virus can lead to mental disorders. Emotional responses during massive infectious disease outbreaks are likely to include feelings of extreme fear and uncertainty that, along with the separation from loved ones and the limitations on movement, may eventually lead to dramatic mental health burden (Moccia et al., 2020). Furthermore, the moderate type of anxiety and depression were the commonest among those developed psychological symptoms, which is higher than that reported in other studies, such as in Saudi Arabia (10.1%, 11.9%) (AlKhamees et al., 2020), and in China (7.1%, 12%), respectively (Ren et al., 2020). Anxiety and depression, when abnormally increase, weaken body’s immune system and consequently increase the risk of contracting the virus (Salari et al., 2020).
In this study, both genders were almost equally affected by anxiety, while depressive symptoms was more in females than in males, this is comparable to most of other studies in which females were affected more than males, probably because they are more vulnerable to stress and post-traumatic stress disorder than men (Moccia et al., 2020; Parlapani et al., 2020; Ren et al., 2020; Özdin & Özdin, 2020).
The results of the existing study show that during the pandemic, the levels of anxiety, depression and stress are significantly higher in the age group 21 to 40 years, that is especially concerned over the future consequences and economic challenges caused by the pandemic for they are the key active working forces in a society, so, are more affected by redundancies and business closures. Some researchers thought that a greater anxiety among young people may be due to their greater access to information through social media, which can also cause stress (Salari et al., 2020).
Two third of the females (with mental symptoms) had fear, with an excess in the age group 40 to 49 years, this is consistent with a study in Bangladesh (Siddique et al., 2021). Fear is known as one of the most primitive feelings that come up in the face of a real or perceived threat.
Studies suggested that sleep (sleep quality and latency) can be susceptible to alterations due to irrepressible or random stressors (Siddique et al., 2021). Insomnia in our sample was reported more in females and in age group <30 years, this is in line with a meta-analytic study for 39 different countries (including Iraq) (Alimoradi et al., 2021). Some studies found a positive correlation between the level of fear and practicing some protective behaviors (Iorga et al., 2021).
Many reasons are behind the appearance of mental symptoms such as the sudden emergence of the disease, horrible stories about rapid death of patients, or uncertainty of future risk and complications. The commonest reason in the current study was fear of respondents to get infected with coronavirus and transmit it to their families (94.7%), this percentage is higher than that of another study in Berlin where the fear of the consequences for the health of their relatives was the commonest (78.3%) (Petzold et al., 2020).
With introduction of the long-term home quarantine, most university students had to study or work at home while living together in a confined space with their families. This led to an increase in family conflict and, thereby, more individual anxiety levels (Jiang, 2021). The quarantine, in turn, has been associated with unhealthy behaviors, such as physical inactivity, sedentary behavior and poor dietary habits (Werneck et al., 2020). The current study showed some of risk health behaviors among half of the participants, the most common of which was overuse of mobile, this seems to be higher than the findings (66.3%) of a study on 184 Italian children and adolescents (Serra et al., 2021). Adults who put more efforts and time into mobile social media had poorer sleep quality, lower self-esteem, and higher levels of anxiety and depression (Jiang, 2021).
In the current study, stopping educational activities was the most social burden that affected two third of the participants; closing all places of daily social activities as a precautionary measure for containing COVID-19 had an impact on students’ lives in relation to being inactive physically and created the feeling of a lack of space for movement. Moreover, feelings of isolation and being away from their community members were confirmed as negative impacts (Rapanta et al., 2020).
The Middle East Region faces the dual threats of potential mass virus outbreaks in conflict zones and impending socioeconomic trouble. Each crisis might have severe humanitarian consequences (Taha, 2021). Daily workers have suffered many kinds of impacts resulting from the pandemic, the main consequences of which has been a reduction of working hours and, in some cases, a loss of job, resulting from fear and restricted mobility associated with confinement measures. This impact is on both male and female domestic workers, as well as those in formal and informal employment (ILO, 2020). Cessation of work was one of the main economic problems that the participants complained of, large numbers of workers around the world have been made redundant or have been placed on temporary, unpaid leave of absence. Inevitably this will have a significant impact on individuals’ abilities to pay rent, mortgages and various household expenditures (Nicola et al., 2020).
Conclusions
The findings of this study indicate that symptoms of depression and anxiety in time of COVID-19 are relatively prevalent. Suspending educational activities was the most social burden that affected people, while increase the price of food and cessation of work were the main causes of economic burden. Implementation of mental health assessment and supporting programs can make a difference in lessening the burden of the pandemic on people.