
Abstract
Background:
Mother–infant bonding is an important factor that supports an infant’s socio-emotional development. Therefore, every family member should acknowledge these processes, especially in an extended family set-up like in Indonesia. The general study objective was to predict several socio-demographic factors associated with mother–infant bonding in Indonesian samples.
Method:
This is a cross-sectional study. The participants included 168 mothers who had infants aged 0 to 36 months and willingly joined the study by signing the informed consent form. The Indonesian version of mother–infant bonding scale and a socio-demographic questionnaire were administered to all mothers. Logistic regression was applied to identify the socio-demographic factors that had any association with the mother–infant bonding scale. The data were analyzed using the SPSS program version 21 for Mac.
Results:
The study showed that 13.1% of the participants were categorized as having a moderate-to-high level of impaired mother–infant bonding. Logistic regression analysis showed that vaginal or normal delivery mode was 4.07 (95% CI [1.27, 13.09]) times more likely to exhibit low levels of impaired mother–infant bonding compared to a cesarean section. The model explained 18.6% (Nagelkerke R2) of the variance in impaired mother–infant bonding and accurately classified 86.9% of cases.
Conclusion:
The findings support prior studies that have been conducted in several countries. Psychoeducation on supporting mother–infant bonding may consist of several topics, such as the advantages of vaginal delivery mode and the importance of family support. It may be delivered in the early adulthood period and, hopefully, basic knowledge during those periods may help strengthen the understanding of mother–infant dyad issues among all family members.
Background
The foundation of mother–infant dyads is usually described in terms of attachment and bonding (Stoodley et al., 2021; Taylor et al., 2005). Several studies have suggested that maternal–infant bonding involves a one-way association between the mother and her child, whereas infant mother–infant attachment involves the reciprocal association that develops over time between the mother and infant (Kinsey & Hupcey, 2013; Yoshida et al., 2020). Mother–infant bonding develops initially during pregnancy, subsequently up to the infant’s first year of life, and so on. These initial experiences that form an internal working model and object representation in the infant mind lays the foundation for future relationships across a lifetime (Stoodley et al., 2021). An optimal mother–infant bonding is important for infants’ future social, emotional, and cognitive development (Kinsey & Hupcey, 2013; Yoshida et al., 2020). Correspondingly, a low level of mother–infant bonding may potentially increase the risk of infant depression, anxiety, and low resilience skills, learning, and working memory difficulties (McNamara et al., 2019; Tsuchida et al., 2019).
Mother–infant bonding may be associated with maternal confidence after childbirth. Mothers gained confidence as their babies developed on a par with other infants, and they started to identify their baby’s needs, as part of a learning process by using environmental resources, trial-and-error, and their internal intuitive sense, especially in recognizing and dealing with their infant distress (Murdoch & Franck, 2012). Therefore, there were several elements that may possibly affect mother–infant bonding, consisting of maternal and infant factors. Maternal factors can be generated as working mothers, lack of social support, non-vaginal delivery mode, postpartum depression, and primiparity. Moreover, premature infants, infants with difficult temperament, emotional dysregulation, and excessive clinging were more likely to have difficulties in bonding with their mothers (Adama et al., 2018; McNamara et al., 2019). Guittier et al. (2014) explained that women subjectively preferred to have a vaginal delivery, related to their preference for natural childbirth with minimal intervention. Therefore, they may easily bond with their babies. Conversely, women who have undergone a cesarean section are more likely to report feelings of helplessness and loss of perceived control. Correspondingly, the mode of childbirth impacted a mother’s emotions and initial moments of contact with their newborns, and influenced mother–infant bonding processes, especially in first-time mothers (Guittier et al., 2014). The mode of delivery also had a significant impact on the infant itself. Babies born through a natural delivery mode had significantly higher cortisol levels and expressed enthusiasm to find direct emotional contact with their mothers after delivery, which created favorable conditions to form adequate mother–infant bonding (Pilch, 2015). Primiparity was also often associated with poor mother–infant bonding. A study in Japan found that primiparous mothers had worse mother–infant bonding than multiparous mothers. This may be associated with a lack of parenting experiences in primiparous mothers (Motegi et al., 2020). A study by Tsuchida et al. (2019) revealed that primiparous women may develop postpartum depression, which may also indirectly affect bonding.
In Indonesia, cultural values may have a significant impact on mothers’ feelings toward their infants, such as belief that using religious symbols or objects (knife, scissors, or other sharp objects) to drive away evil spirits. Therefore, family members may create a safe heaven environment that support mother’s feeling to develop a better mother-infant bonding. Currently, Indonesia represents more than 200 ethnic groups. However, in the last century the modern environment of globalization and rapid cultural changes has influenced Indonesia as a nation. Riany et al. (2017) demonstrated that theoretically, Indonesian parents regardless of their ethnicity, may possibly more culturally adhere to Westernized parenting norms, values, and orientations, compared to parents in other East Asian countries, but still conform the beliefs of local cultural values and norms. Another difference is the concept of the extended family in Indonesia. All family members play a significant role in an infant’s life, and spend time with the child whenever possible. The family-based parenting model in Indonesia consists of co-parenting by nuclear and extended families. In extended families, co-parenting is usually performed by grandparents or other family members (Fauzi et al., 2021). Members of extended families could have different backgrounds and knowledge about newborn care and parenting. An extended family structure could also affect the socio-economic status of the entire family. Therefore, it is also a very common issue for Indonesian families to be extremely cautious with infant development, and each family member has his/her own approach and style to enhance infant developmental milestones. Consequently, the existence of extended family members in parenting can either support or pressure the mother, affecting the mother’s mental well-being, and successively, the mother–infant bonding processes itself (Anifah et al., 2018). Nevertheless, in Indonesia, socio-economic factors may have a strong impact on the quality of parenting and indirectly influence mother–infant bonding (Hidayat et al., 2019; Zevalkink & Riksen-Walraven, 2001). Pregnancy and motherhood are considered a major responsibility by every woman in Indonesia, especially for continuing the bloodline, and the family usually places a higher value for having a male child in the next generation. Meanwhile, it is also considered a taboo for mothers to express feelings of dislike toward their babies, even though it could plausibly occur (Hidayat et al., 2019; Wiguna & Ismail, 2019).
There are limited studies on the factors associated with mother–infant bonding in Indonesia, compared to the birth rate of the country. Therefore, it is imperative to learn about the various factors associated with mother–infant bonding in Indonesia, especially from a socio-demographic perspective. The findings of this study may be used to guide and develop strategies to prepare and assist in understanding mother–infant bonding processes for every family member in the community based on their social context. Furthermore, it was also aimed at heightening the importance of early detection programs on mother–infant bonding risks on both nuclear and extended family members, which may reduce the possibility of impaired bonding processes.
Method
Participants
This cross-sectional study included mothers with infants aged 0 to 36 months, who agreed to participate in the research by completing the informed consent and questionnaire. The participants were originally from the Beji Volunteer-Staffed Integrated Health Service (Posyandu)-Depok/West Java and the pediatric outpatient clinic at Dr. Cipto Mangunkusumo General Hospital, Jakarta. The questionnaire included questions about demographic data like mother’s age during pregnancy (low risk pregnancy was set as <35 years old or high risk pregnancy ⩾35 years old), educational level (low educational level was set as less than secondary high school), employment status (employed or unemployed), family income (middle-to-low-level or high-level income based on the minimal standardized income in Jakarta and West-Java), and questions related to pregnancy – whether the pregnancy was intended or not, parity (multiparity or primiparity), and did the mother receive social support during pregnancy from her husband and family (‘Yes’ or ‘No’). There are also questions about the delivery modes (normal or cesarean), baby birth weight (<2,500 or ⩾2,500 g), and the age of the infant during the study (<12 or ⩾12 months).
Instruments
The Mother–Infant Bonding Scale–Indonesian Version (MIBS-I) was used to assess the quality of mother–infant bonding. MIBS-I consists of eight items on a 4-point Likert scale (from 0, ‘not at all’ to 3, ‘very much’). Several items were reversed scales. Wiguna and Ismail validated the Japanese version of MIBS into Indonesian language in 2018 (Wiguna & Ismail, 2019). A higher total score on MIBS indicates worse mother–infant bonding compared to a lower score. Since the Japanese version of MIBS-I has had no exact cut-off point yet (Yoshida et al., 2012), the study used data-driven cut-offs. MIBS-I scores of 3 and under (less than M + 1 SD) were categorized as low level of impaired mother–infant bonding and a score of 4 and above (>M + 1 SD) was categorized as moderate to high level of impaired mother–infant bonding. Each of these scales specifically addressed the mother’s emotions and feelings toward the infant, rather than her behavior or parenting confidence. The MIBS-I categorized all the eight items into three domains. The first domain was ‘desire to love and denial’, which contains items associated with the ambivalent attitude of the mother toward the infant (item numbers 8 and 9); the second domain was ‘hate and being closed’, which included items related to the ambivalent feelings in the form of emotions of ‘hate and being closed’ toward the baby (item numbers 3, 5, 6, and 10); the third domain was ‘feelings of rejection’ toward the infant (item numbers 4 and 7; Wiguna & Ismail, 2019).
Data analysis
Data analysis was performed using the SPSS version 21 for Mac. The data comprised numerical and categorical variables, and the authors further converted the data into categorical variables in order to identify the association between dependent and independent variables. Chi-square and Fisher’s exact tests were used to determine the association between the dependent variable (low level of impaired mother–infant bonding and moderate to high level of impaired mother–infant bonding) and independent variables. Binomial logistic regression analysis was applied to identify whether impaired mother–infant bonding can be predicted by several independent variables in Indonesian samples. In addition, Spearman’s correlation analysis was performed to determine the correlation between each variable and the MIBS-I domains. The p-value was set at <.05.
Results
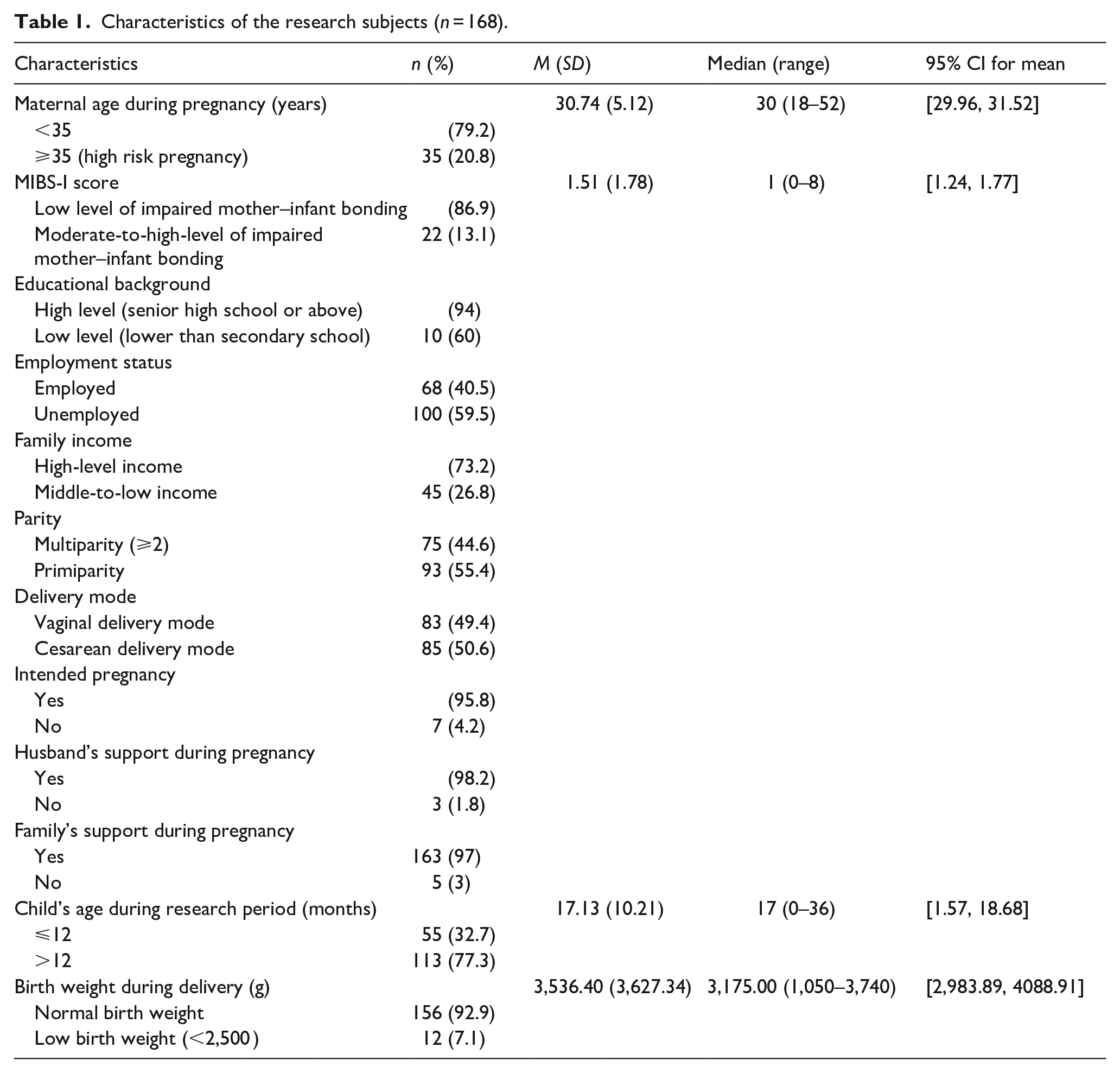
Overall, 168 participants completed the questionnaire. The average maternal age during pregnancy was 30.74 (5.12), with 20.8% aged ⩾35 or within the high-risk pregnancy category. The participants mostly had a high-level educational background (94%), and belonged to a high-income family (73.2%). Most of the mothers were unemployed (59.5%). All the participants had an extended family background. The study found that 13.1% of the participants were categorized as having a moderate-to-high level of impaired mother–infant bonding. Among the participants, 55.4% were primiparous, and 50.6% delivered their babies through cesarean mode (49.4% had vaginal delivery). Most of the pregnancies were intended pregnancies (95.8%). A majority of the participants acknowledged their husbands’ support during pregnancy (98.2%), and they also received support from their families (97%). The mean age of infants by the time the questionnaire was filled was 17.13 months. Approximately 7.1% of the participants had infants with low birth weights during delivery (Table 1).
Characteristics of the research subjects (n = 168).
The bivariate analysis showed that there was a significant association between impaired mother–infant bonding and employment status (OR = 3.51, 95% CI [1.13, 10.89]), family income (OR = 2.64, 95% CI [1.05, 6.64]), delivery mode (OR = 0.17, 95% CI [0.05, 0.55]), and infant age during the study period (OR = 3.50, 95% CI [0.99, 12.4]; Table 2).
Association between socio-demographic factors and MIBS (n = 168).
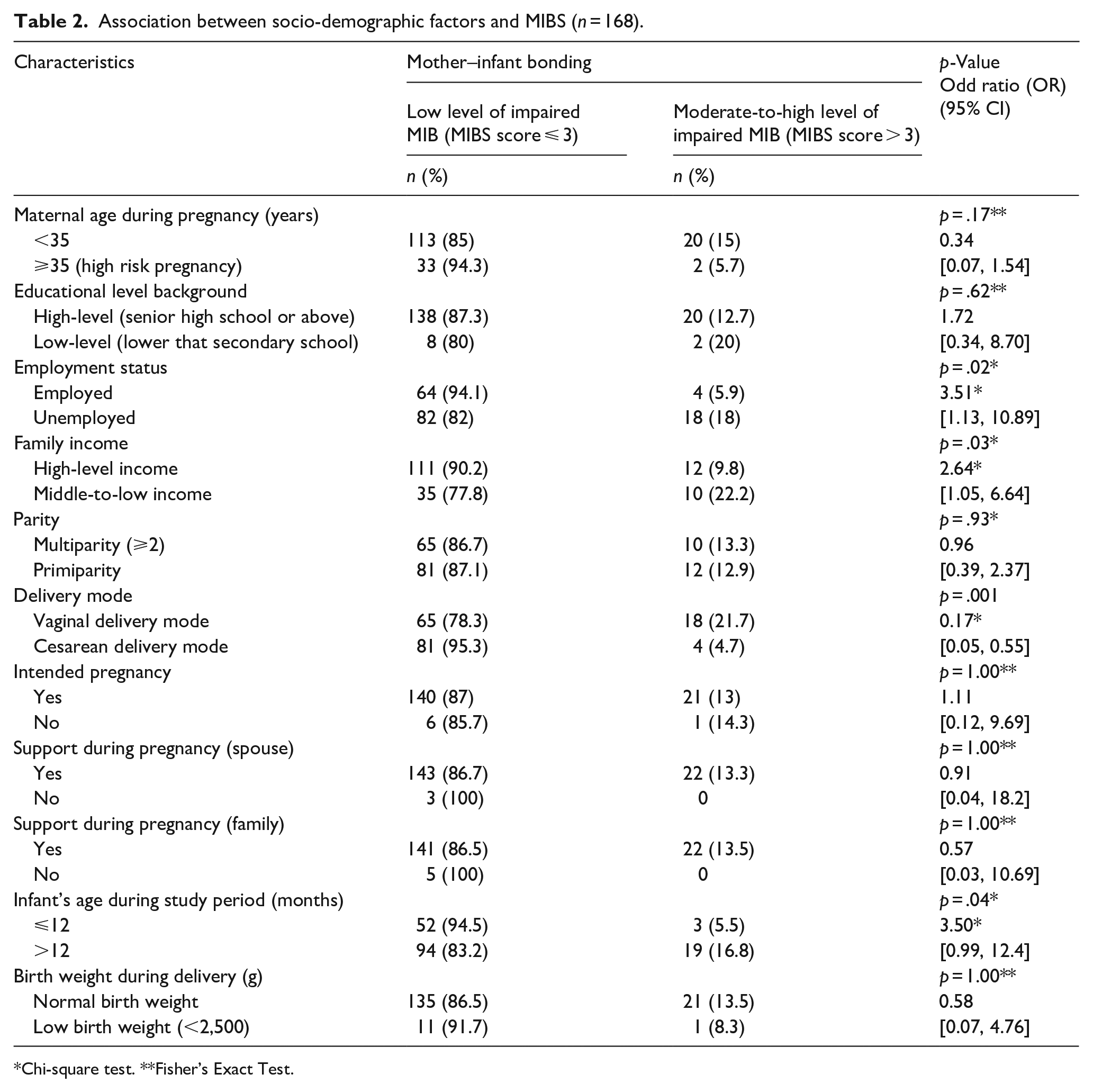
Chi-square test. **Fisher’s Exact Test.
Logistic regression analysis showed that the model was statistically significant, χ2(4) = 17.765, p = .001). The model explained 18.6% (Nagelkerke R2) of the variance in impaired mother–infant bonding and accurately classified 86.9% of cases. The Hosmer and Lameshow test of the goodness of fit suggested that the model was a good fit to the data (p = .957). Vaginal delivery mode was 4.07 (95% CI [1.27, 13.09]) times more likely to exhibit low levels of impaired mother–infant bonding compared to cesarean delivery mode (Table 3).
Logistic regression analysis between socio-demographic factors and MIBS-I (n = 168).

Note. χ2(4) = 17.765.
p = .001; Hosmer and Lameshow p = .957.
Meanwhile, Table 4 demonstrated several significant correlations between participants’ characteristics and the domains of MIBS. The first is that the mother within the high-risk pregnancy age group had a significant negative correlation with the second domain, which is ‘hate and being closed’ toward the infant (r = −.227, 95% CI [−0.35, 0.07]). Meanwhile, employment status had a significant positive correlation with the second domain (r = .193, 95% CI [0.04, 0.32]), as well as the child’s age (r = .240, 95% CI [0.08, 0.36]). Mode of delivery also had a significant negative correlation with the second domain (r = −.257, 95% CI [−0.39, 0.10]). The third domain, which concerns ‘feelings of rejection’ toward the infant, was significantly correlated with employment status (r = .272, 95% CI [0.13, 0.40]) and family income (r = .290, 95% CI [−0.12, 0.44]).
Correlation analysis between socio-demographic factors and MIBS domains.
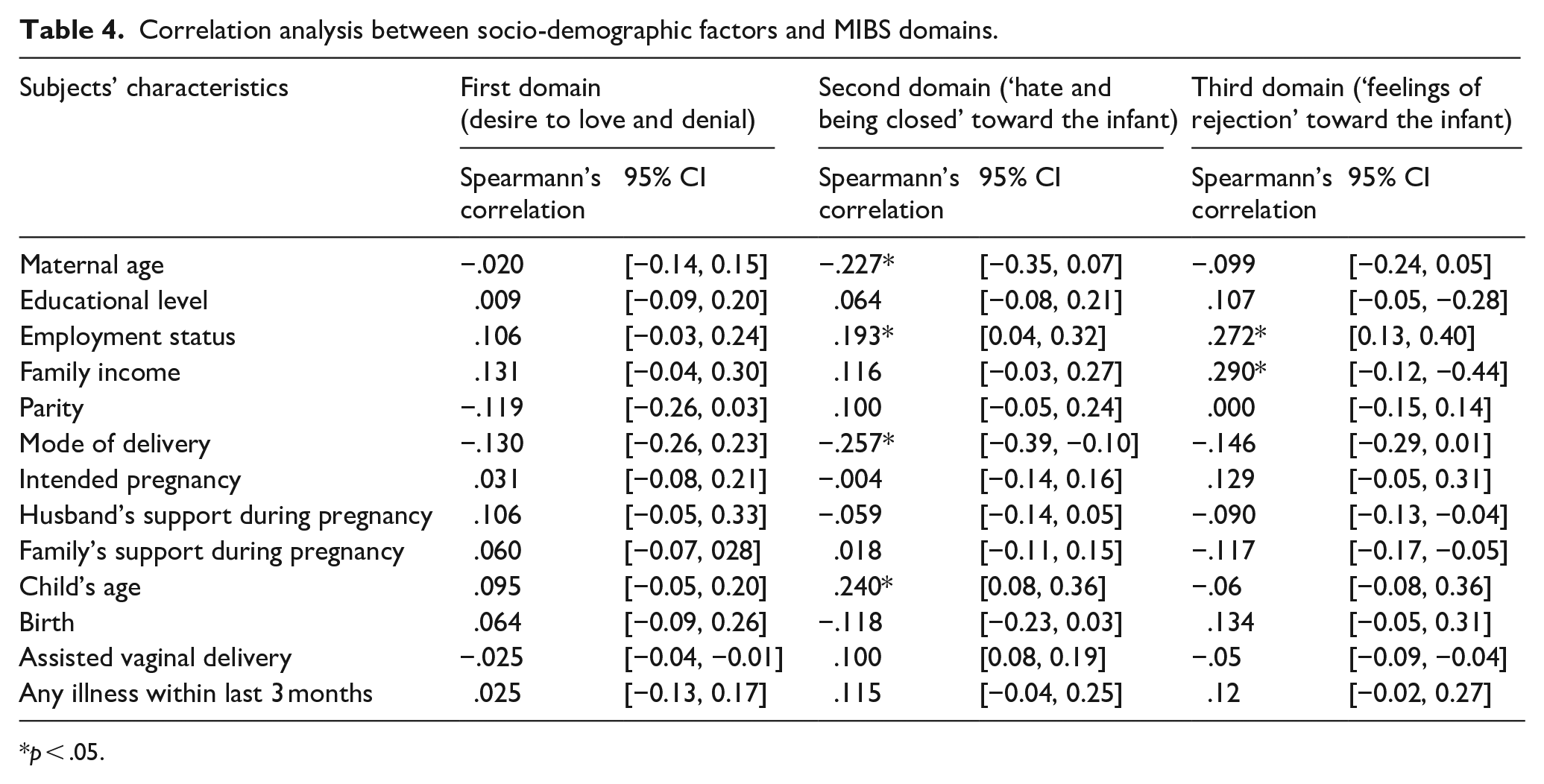
p < .05.
Discussion
The results of this study strengthened to the current knowledge regarding the perinatal risk factors and added new insight on the importance of psychosocial role that associated with mother–infant bonding. First, according to several studies, socio-economic factors such as income and employment status have a positive impact on the development of mother–infant bonding, and are important to develop secure mother–infant bonding and attachment (Abbas et al., 2018; Diener et al., 2003). Accordingly, this study showed that mothers with higher income and employed tend to develop a low risk of impaired bonding between the mother and the baby. Poor socio-economic status as well as low income and unemployment could lead to stress and anxiety, potentially resulting in postpartum depression, which consequently would affect the mother–infant bonding process in the early postpartum period (Lutkiewicz et al., 2020; Matsumura et al., 2019). Therefore, assessment of postpartum depression should be included in future studies. A study of mothers in Semarang in Central Java, Indonesia, showed that working mothers experienced difficulty in caring for their baby because of their brief maternity leaves and long working hours. Muslims account for a majority of the Indonesian population, and they have strong values which encourage every mother to directly care and breastfeed their babies, so that working mothers might experience ‘guilt’ toward their babies, and consequently they would put more efforts in caring for their babies in their limited time, which could improve the quality of the bonding process (Anggraeni et al., 2020). Employment correlated with the second domain (hate and being closed) and the third domain (feelings of rejection) of the MIBS, while family income was also interrelated to the third domain. This finding showed that even though mothers with a lower income and unemployed were physically still close to their babies, but it is assumed that it triggered the feeling of denial and resistance toward the baby respectively. This can be attributed to the fact that having a baby entails additional expenditure, and mothers from a low income family background and those who are unemployed might have limited financial resources for the baby and family needs, especially during the newborn phase (Goyal et al., 2010). Family with low economic status is also associated with increased depressive symptoms during pregnancy and postpartum period, so that mother–infant bonding is considered affected by those circumstances (Matsumura et al., 2019).
According to this study, the mode of delivery is one of the crucial factors associated with mother–infant bonding, with mothers who have had a vaginal delivery likely to have a lower risk of impaired mother–infant bonding than those who have undergone a cesarean section. This finding supports several previous studies on the mode of delivery and the MIB score. Ebrahimi et al. (2018) found that mothers who had normal childbirth had significantly more successful attachment with their babies than those who had a cesarean section. These mothers also showed more positive attachment behaviors like caressing and hugging the baby more often. Various studies also explained that mothers who delivered their babies by cesarean mode more likely experienced problems related to breastfeeding than those who had normal delivery, so that the formation of mother–infant bonding might be affected (Cetisli et al., 2018). Guittier et al. (2014) found that mothers usually had negative connotations for cesarean delivery, and those who delivered the baby via cesarean sections felt somehow deprived of the sensory discovery of the baby, thereby affecting the mother–infant bonding process.
Indonesian women who experienced problems during pregnancy and labor, such as cephalopelvic disproportion, preeclampsia, premature rupture of membranes, and fetal breech were 12 times more likely to have a cesarean delivery (Rahmawati et al., 2016). Conditions such as preterm birth and other pregnancy-related issues could also lead to maternal distress and decreased responsivity, thus leading to interactional problems and insecure attachment between the mother and the infant. Additionally, behaviors of preterm infants and other medically fragile infants might be difficult to read and require a high level of parental sensitivity in order to develop adequate mother–infant bonding (Poehlmann & Fiese, 2001). In several health services, following a cesarean section, babies are placed under observation in a nursery room, and separated from their mothers, sometimes even until a few days after delivery (Vääräsmäki & Raudaskoski, 2017). The separation of the mother and the baby during this crucial time could have impacted the mother–infant bonding process. The separation could prevent early skin-to-skin contact, because it influenced mother–infant interactions (Bystrova et al., 2009). This also explains the correlation between the mode of delivery and the second domain of the MIBS, which is ‘hate and being closed’, where mothers who had a cesarean section tend feel less ‘hate and being closed’ when compared to mothers who had a vaginal delivery.
There was also a significant association between infant age during the study and MIBS. It also had a significant positive correlation with the second domain of the MIBS, where mothers with older infants tend to develop feelings of ‘hate and being closed’ with their infants. During the first 1 or 2 years, Indonesian mothers preferred to remain with their infants whenever possible. If the mother works outside the home, she leaves the infant with someone she trusts, usually siblings, grandparents, or other family members. Therefore, maternal behavior that emphasizes soothing, holding, and overprotection with the infant is considered typical in Indonesia, especially in the early years (Anggraeni et al., 2020). Conversely, mothers with older infants have spent more time ‘being closed’ to the baby, thus explaining the ambivalent feelings of ‘hate and being closed’.
The co-parenting model by extended family members, which is commonly practiced in Indonesia, could be considered as factors associated with the mother–infant bonding process. Daily baby-care assistance by grandmothers or other family members can lower the interaction time for mothers and infants. That mother–infant interaction time might even decrease after the mother returns to work after maternity leave. Different opinions or ways to care for the baby between the mother and other family members can also affect mothers’ confidence in caring for their babies, especially a first-time mother (Fauzi et al., 2021). Responsibility shared in infant-care in Indonesia is mostly performed by grandparents, with age range in the early elderly. People in this age category be vulnerable to physical and psychological problems, so that the interaction between the mother and the infant to be affected (Fauziningtyas et al., 2019). Those considerations, an assessment of family structure, should be included in future studies as well.
The findings of this study showed that mother–infant bonding is a very complex process that is associated with several psychosocial factors such as family income, maternal age during pregnancy, infant’s age during the study, and mode of delivery. Skin to skin contact between mother and infant was an important factor that promoted mother-infant bonding. Therefore, psychoeducation on mother–infant bonding may commence at the end of puberty and during early pregnancy for every family member. Psychoeducation include topics such as the importance of vaginal delivery mode, the significance of family support, skin to skin contact in the earliest time after delivery, and the best age to get married and have children, understanding the meaning and importance of mother-infant bonding, etc. The basic knowledge on mother–infant bonding that was afforded during those periods strengthen the understanding of mother–infant dyad issues, especially for extended family members. Therefore, it can possibly enhance the mother–infant bonding process for expectant mothers. In addition, initial assessment and screening of mother–infant bonding can be made for every expectant mother since the beginning of pregnancy, specifically those who are at risk, so mental health promotion, prevention, and support can be provided during the early stages. Therefore, initial assessment and screening can be performed at the primary health care or maternity center, so that every expectant mother can directly access it.
This study has certain limitations. First, it only included several psychosocial factors and not any assessment of difficulties during pregnancy and the delivery process, postpartum depression, personality profiles of the mother, and other maternal psychopathological factors that effected on the mother–infant bonding processes. Therefore, future studies may consider these factors especially since it could provide more important details on the bonding process. The second limitation is that the characteristics of the participants in this research were originally come from one Posyandu (West Java) and general hospital (Jakarta) that may not represent the whole country. Furthermore, they mostly had high-education and high-income backgrounds, which may have affected the perception of bonding among mothers and also the data that showing a high rate of cesarean delivery. Further research with participants from other provinces in Indonesia, various educational and economic backgrounds might enrich the knowledge about mother–infant bonding especially in heterogeneous population likes Indonesia. In conclusion, this study is the first to elucidate the association between several psychosocial factors and mother–infant bonding in Indonesia. Therefore, it may be used to guide and assist the perinatal mental health research, prevention and promotion program in Indonesia and other developing countries that have similar geographical contexts.
Footnotes
Acknowledgements
We would like to thank you all parents and infants that participated in this study.
Author contributions
All authors contributed on: (1) made a substantial contribution to the concept or design of the work; or acquisition, analysis, or interpretation of data, (2) drafted the article or revised it critically for important intellectual content, (3) approved the version to be published, and (4) each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication was funded by the PUTI Grant Universitas Indonesia with contract number NKB-4091/UN2.RST/HKP.05.00/2020.