
Abstract
Objectives:
The current study aimed to detect the BOS prevalence and determinants among residents working during the second wave of the COVID-19 pandemic in an Egyptian tertiary university referral hospital.
Methods:
A cross-sectional study evaluating the working period from June to November 2020 during the COVID-19 pandemic second wave, through a five sections questionnaire evaluating: 1 − sociodemographic characteristics, 2 − job characteristics, 3 − negative thoughts related to their job, 4 − resident’s health problems, and 5 − evaluating BOS through Maslach Burnout Inventory (MBI) scale (including emotional exhaustion [EE], depersonalization [DP], and personal accomplishment [PA] as subscales).
Results:
We included 230 residents with a median age of 27 years. The median MBI sub-scales (IQ Range) values were 30.0 (20, 39), 21.0 (15, 30), and 29.5 (22, 36) for EE, DP, and PA, respectively. About 51.0% and 83.0% of the residents were high in EE and DP, while 8.7% were low in PA. The median EE and DP were higher in younger age (⩽27 years; p = .002 and .024), males (p = .001 and <.001), working >90 hours weekly (p = .016 and <.001), exposure to harassment (p < .001), and having COVID-19 infection (p = .002 and .001). Residents working in surgical departments reported higher DP scores than those in non-surgical departments (p = .03). There was a mild positive correlation between working hours per week and the total scores in EE and DP, r = .24 (p < .001) and r = .23 (p = .001) respectively, while it was found to have a negative correlation with the PA (r = −.133 and p = .044).
Conclusions:
The BOS is evident and considerably high among the residents working during the COVID-19 pandemic. Younger age, males, working in surgical departments, and those who got COVID-19 infection were most vulnerable.
Introduction
Herbert Freudenberger (a psychologist) in 1974 was the first to describe burnout syndrome (BOS); through analyzed work dissatisfaction resulting from work-related stresses (Freudenberger, 1974). Three main elements characterize BOS: emotional exhaustion, depersonalization (presented as detachment and negative attitude toward others), and the feeling of diminished personal accomplishment (sense of incompetence and lack of advancement at work; Maslach, 1993).
From a healthcare worker’s perspective, BOS could be described as physical and mental exhaustion resulting from stresses related to providing medical care for others (Dimitriu et al., 2020), which appears to be prevalent in both developing and developed countries, with consequent economic, social, and psychological overloads to individual physicians, their institutions, and the healthcare system (Aljuhayman et al., 2021; Alsheikh et al., 2019; Al Subhi et al., 2020; Ben et al., 2018; Galaiya et al., 2020). In recent years, the prevalence of BOS among healthcare professionals was studied thoroughly and was shown to affect between 40% and 75% of healthcare professionals among various specialties (Chemali et al., 2019; Dubale et al., 2019; Galaiya et al., 2020).
The coronavirus disease or the COVID-19 pandemic is considered one of the most significant and thoroughly studied health crises in the present era (Rothan & Byrareddy, 2020), affecting most world countries regardless of their location or socioeconomic status, including Egypt (Bulut & Kato, 2020; Lai et al., 2020). Healthcare professionals are considered one of the major groups exposed and affected by the pandemic, as while the general population was advised to stay at home and practice social distancing, healthcare professionals had to continue their work necessitating direct contact with suspected and confirmed cases of COVID-19, added to that the deficiency of the personal protective equipment (PPE) and the uncertainty of management protocols led to a higher possibility of infection (The, 2020). The previously mentioned factors led to the imposition of further stresses on healthcare professionals with a further possible increase in BOS prevalence during the COVID-19 pandemic, which was confirmed in many recent reports (Abdessater et al., 2020; Alawad et al., 2022; Bradley & Chahar, 2020; Chen et al., 2020; Dewey et al., 2020; Elghazally et al., 2021; Lai et al., 2020).
In a survey conducted by Civantos et al. (2020) assessing BOS and anxiety among 349 otolaryngologists working during the COVID-19 pandemic, they reported a high prevalence of BOS, anxiety, and distress. In another study by Abdessater et al. (2020) evaluating the stress resulting from working during the COVID-19 pandemic and its negative impact on work and training quality among 275 urologists in France, they concluded that the pandemic has a negative psychological impact, especially on young urologists in training which affected their quality of life. Furthermore, Dimitriu et al. (2020) evaluated BOS among 100 Romanian medical residents working at the time of the COVID-19 pandemic; they reported that about 76% of the surveyed residents suffered from BOS measured using the Maslach Burnout Inventory (MBI) questionnaire.
Resident doctors act as the intermediate communication interface between attending physicians and patients; therefore, they are spending more time with patients, which became even more stressful during the COVID-19 pandemic, owing to the possibility of infection after contacting a suspected COVID-19 positive patient, which put most of the residents under mental stress till the results appear (Dimitriu et al., 2020). Furthermore, prolonged wearing of PPE, lack of sleep, and prolonged working hours aggravated the mental and physical fatigue among medical residents, especially those working at the frontlines (Abdelhafiz, Ali, et al., 2020; Al Sulais et al., 2020; Dimitriu et al., 2020).
Two recent studies were reported from Egypt evaluating the prevalence of BOS among Egyptian physicians working during the COVID-19 pandemic (regardless of their age or working place); interestingly, both studies revealed that the younger, less experienced physicians (mostly resident doctors) are more vulnerable and affected by BOS compared to older more experienced peers (Abdelhafiz, Ali, et al., 2020; Elghazally et al., 2021). As we believe that resident doctors were on the frontlines during the COVID-19 pandemic, we aimed in this study primarily to detect the prevalence of BOS among resident doctors working at Assiut University Hospital (Egyptian tertiary referral center) in different departments during the COVID-19 pandemic. The secondary objective was to determine the possible correlates affecting BOS incidence.
Methods
After obtaining an institutional Review Board approval (Approval no.: 17300514), a cross sectional study through an online questionnaire using Google forms in the period between December 2020 to March 2021 to evaluate the working period of the previous 6 months (June–November 2020) during COVID-19 pandemic where Assiut University Hospital (including nine branches) were among the centers receiving and taking care of suspected and established COVID-19 cases besides receiving other emergency and trauma cases.
Sample size calculation
The sample size was calculated using Epi-Info, version 2002. According to the prevalence of doctors’ BOS in different studies ranging from 22.2% to 85.1% (Abdo et al., 2016; Salles et al., 2019; Zheng et al., 2018), we expected a prevalence of 50% during the COVID-19 pandemic. Based on a level of significance of 95%, 80% power of the study, estimated prevalence of BOS of 50%, and error of 5%, on a population of 500 residents, the sample size was estimated to be 218 resident doctors.
Study participants and sampling
We included resident doctors from different clinical departments at Assiut University Hospital (nine branches), who were working for more than 6 months after the start of their residency, and were willing to participate in the study. We excluded residents refusing to be involved in the study, those on vacation during the study period, incomplete forms, and those who were residents for <6 months. Of 500 working residents at the time of the study, 350 responded to the questionnaire, and 230 of the questionnaires were available and valid for analysis.
Study tools
The study participants were asked to fill in a pre-designed self-administered questionnaire delivered through Google forms; a link was sent to the participants either by e-mail or WhatsApp application messages. The questionnaire included five sections to get information regarding the past 6 months: The first section included sociodemographic characteristics (age, sex, residence, and marital status). The second section related to job characteristics and experiences (job type, department or ward type, years of experience, a working zone during COVID-19 cases, working hours per week, and if the resident was taking shifts in private institutions outside the university hospitals to calculate the total working hours per week accurately). The third section evaluated the negative thoughts or attitudes related to their job (as thoughts of leaving the residency or being subjected to verbal or physical harassment). The fourth section included questions about the resident’s health problems (COVID-19 infection, other diseases he/she suffered from as attacks of depression, visits to a physician, or admission to a hospital). The last section included the BOS assessment through the Maslach Burnout Inventory (MBI) scale (Maslach et al., 1996; Maslach & Jackson, 1981). The interpretation of the score is confidential and was performed by one of the authors by assessing the three components (sub-scales) of the MBI: emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA). It is a 22-item questionnaire on a seven-point Likert-scale (ranging from 0 = never to 6 = every day). Scores for each section were obtained by adding the numeric responses of the items, which corresponded to each scale. High scores for the first two dimensions (EE and DP) and low scores for the third dimension (PA) indicated BOS (Salles et al., 2019). MBI scores were further used to classify participants as having low (⩽17 points), moderate (18–29 points), and high (⩾30 points) levels of EE, low (<6 points), moderate (6–11 points), and high (⩾12 points) levels of DP and For PA low (⩾40 points), moderate (39–34 points), and high (⩽33 points).
Data collection
Prior to the study, a pilot test on about 10% of the sample (whose results will not be included in the study) was carried out before starting data collection to determine potential obstacles and to estimate the time needed to complete it, and if there is a need to improve the quality of the questionnaire. We designed a distribution schedule for all hospitals to ease following up on responding to the questionnaire. Personal communication with residents and contacting their departments’ heads was performed to encourage responding to the questionnaires to decrease the dropout.
Data management and statistical analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS), version 26.0 for Windows. Quantitative data were expressed as median and interquartile range (IQ range), while frequencies and percentages summarized qualitative data. The Chi-square test was used to compare the difference between two proportions. Based on testing normality for quantitative data, Mann–Whitney U test and the Kruskal–Wallis test were used to compare the difference of means and Spearman correlation between two groups and test variables’ correlation. To identify predictors for MBI subscales and job satisfaction, a p-value of less than .05 was considered a significant cut-off point for all applied statistical tests. All participants were asked to sign an online informed-consent document, which was clearly stated and indicated the purpose of the study. All collected data were confidential, and all were anonymous during data analysis.
Results
For the total 230 participant resident doctors with a median age of 27 years, details of the study group’s sociodemographic, working conditions, and health characteristics are shown in (Table 1). During the study period, 44.8% of the participant residents worked in a red zone, and about half (47.4%) reported having COVID-19 infection. Physical or verbal harassment incidents were reported by 58.3% of the participants, 71.7% reported experiencing depression-like symptoms, and 73.0% were thinking about quitting their residency. According to the MBI sub-scales, the median (IQ Range) values were 30.0 (20, 39), 21.0 (15, 30), and 29.5 (22, 36) for EE, DP, and PA, respectively. Furthermore, 51.0% and 83.0% of the residents were categorized as high in EE and DP scales, while 8.7% were categorized as low in the PA scale (Figure 1).
Sociodemographic, working conditions, and health characteristics of the study group, a total of 230 resident doctors working in Assiut University Hospital.
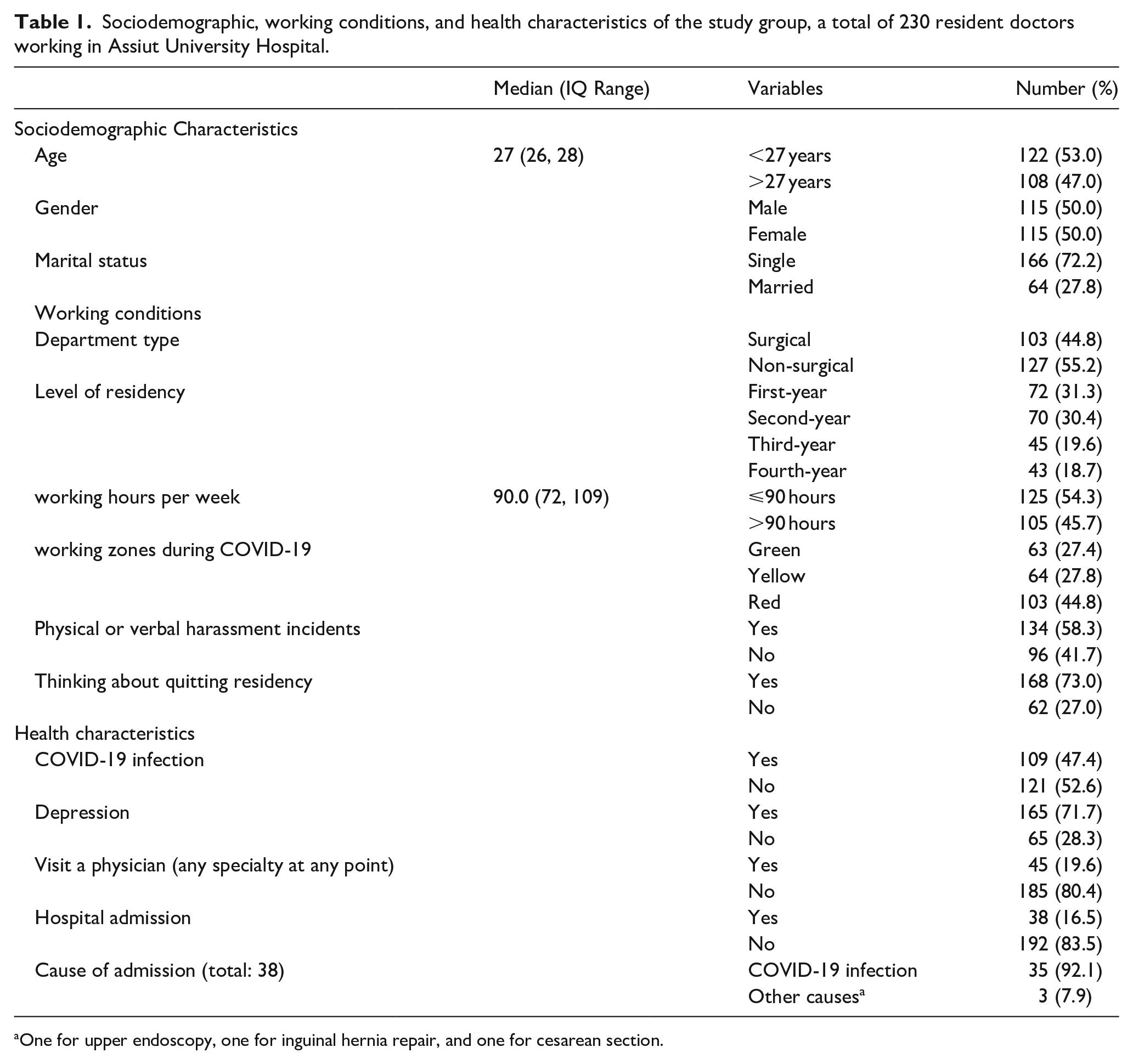
One for upper endoscopy, one for inguinal hernia repair, and one for cesarean section.
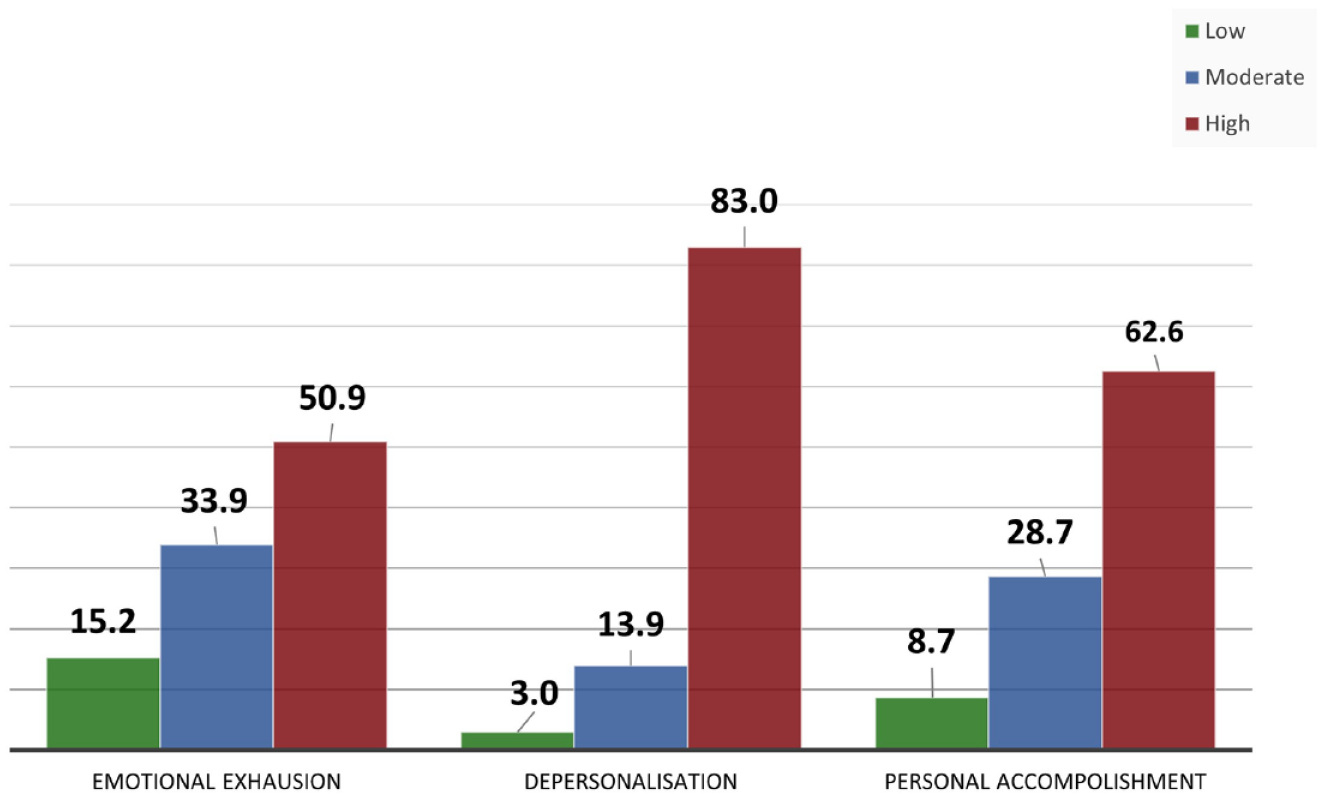
The distribution of participant physicians by burnout according to the total three categories of the Maslach Burnout Inventory scale.
The effect of sociodemographic characteristics and working conditions as determinants on residents’ BOS according to MBI median scores are shown in (Table 2), where the median EE and DP scales were significantly higher in the younger age (⩽27 years; p = .002 and .024, respectively), male residents scored significantly higher scores in EE and DP scales than females (p = .001 and <.001, respectively). The surgical departments’ residents reported significantly higher scores in the DP sub-scale than those in non-surgical departments (p = .03). As regards the years of residency, there is a significantly higher difference in median EE sub-scale scores between the fourth and the first year of residency (p < .001), the fourth and the second year (p = .03), and the fourth and the third year (p = .005). Those who had worked >90 hours weekly scored higher median scores in EE and DP sub-scales (p = .016 and <.001, respectively), and significantly lower median scores in the PA sub-scale (p = .03); however, there were no significant differences in all sub-scales related to working in different zones during COVID-19 pandemic. On the other hand, those who reported exposure to physical or verbal harassment had higher scores in EE and DP sub-scales than those who were not (p < .001) and significantly lower median scores in PA (p = .001).
Sociodemographic characteristics and work conditions determinants of BOS according to Maslach Burnout Inventory median scores (total = 230).
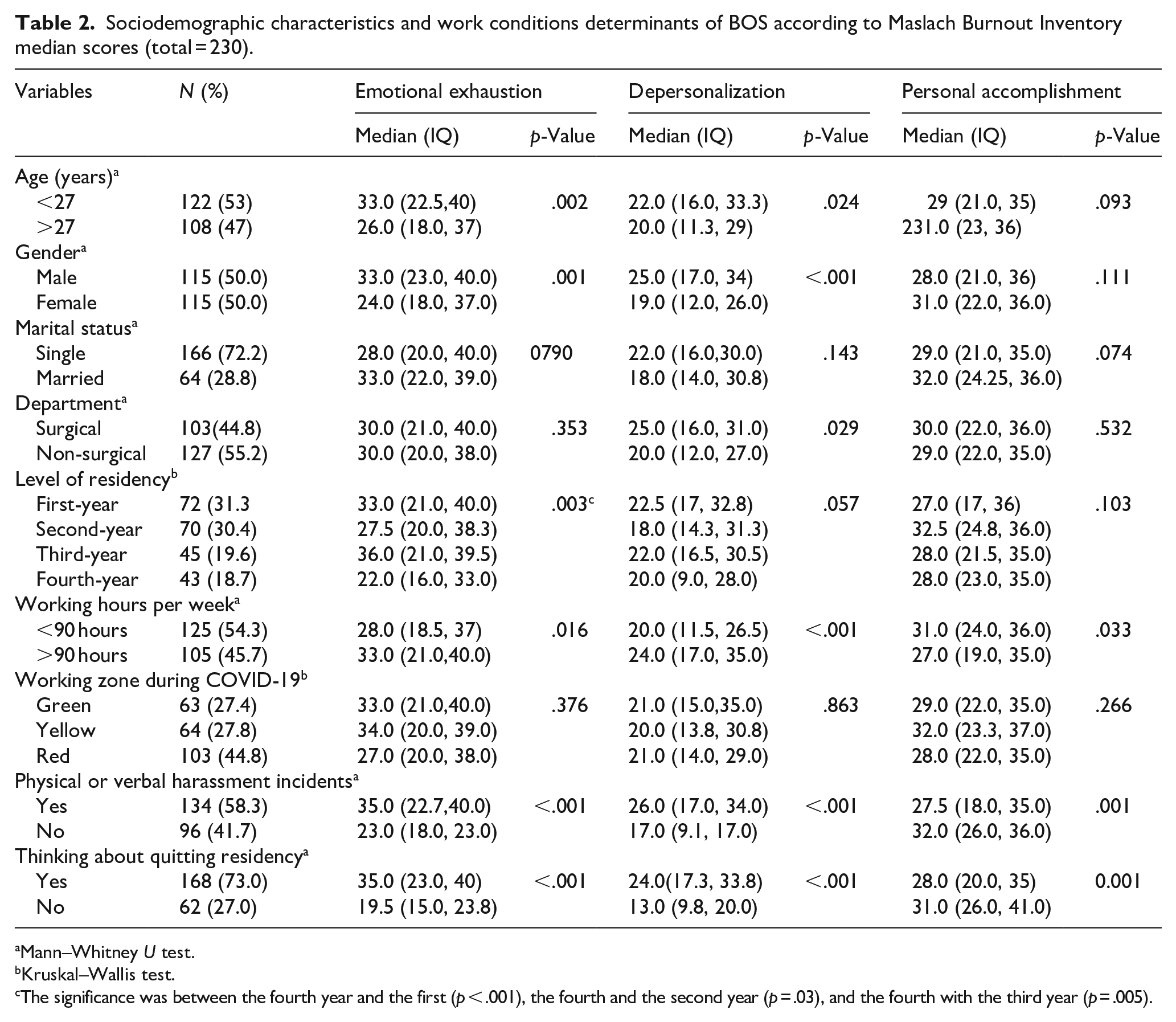
Mann–Whitney U test.
Kruskal–Wallis test.
The significance was between the fourth year and the first (p < .001), the fourth and the second year (p = .03), and the fourth with the third year (p = .005).
The effect of health characteristics as determinants of residents’ BOS according to MBI sub-scales median scores is shown in (Table 3); participants who got COVID-19 infection reported significantly higher EE and DP sub-scales scores than those who did not get an infection (p = .002 and 0.001, respectively). In addition, those who reported depression-like symptoms had higher scores in EE and DP sub-scales (p < .001 and .002, respectively). Those admitted to the hospital reported significantly higher EE and DP sub-scales (p = .034 and .005, respectively). There was a significantly mild positive correlation between working hours per week and the total scores in EE and DP sub-scales, r = .0.24 (p < .001) and r = .23 (p = .001) respectively, while it was found to have a significant negative correlation with the PA total scale (r = −.133 and p = .044; Figure 2).
Health characteristics determinants of BOS according to Maslach Burnout Inventory median scores (total = 230).
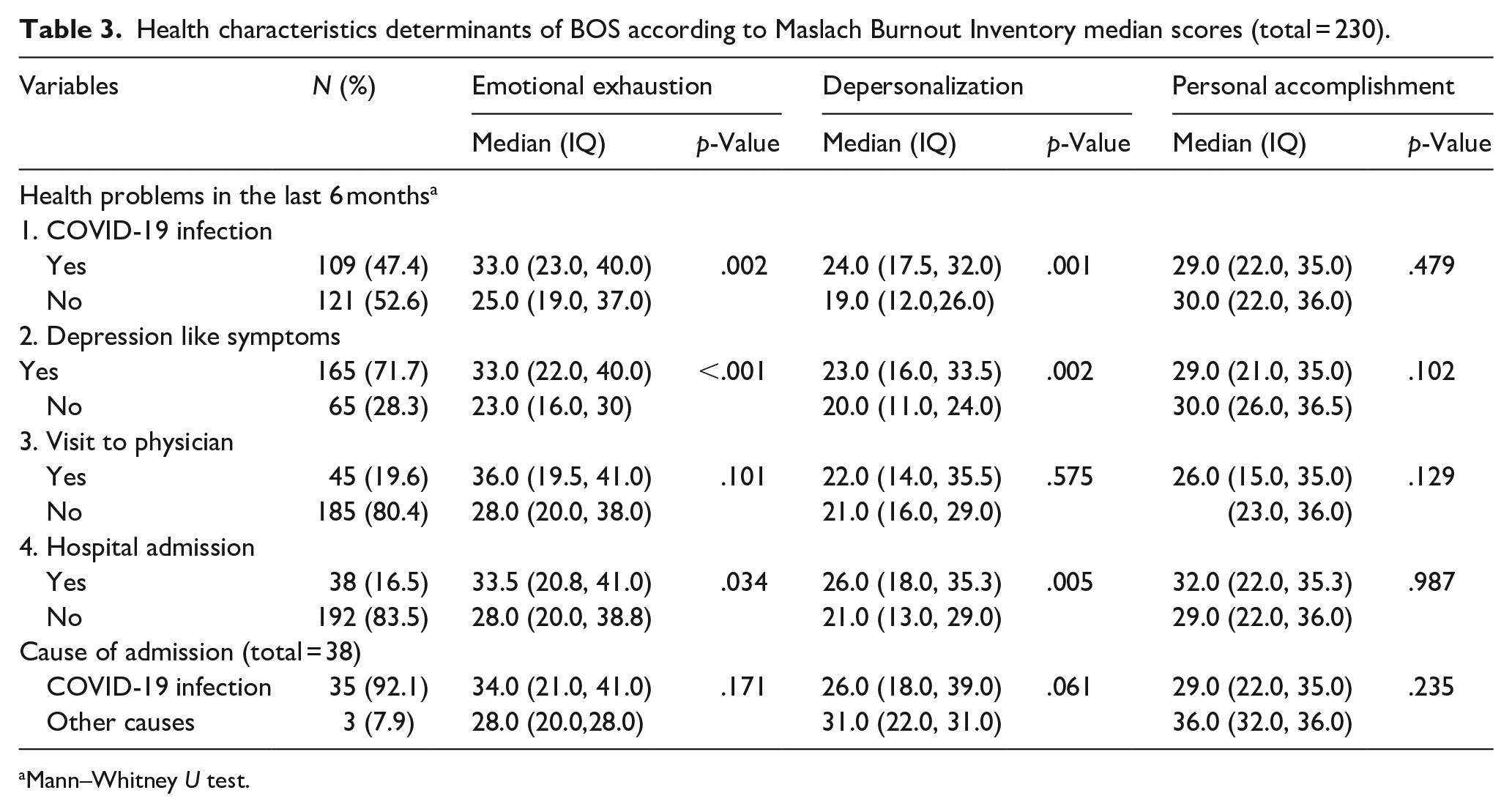
Mann–Whitney U test.
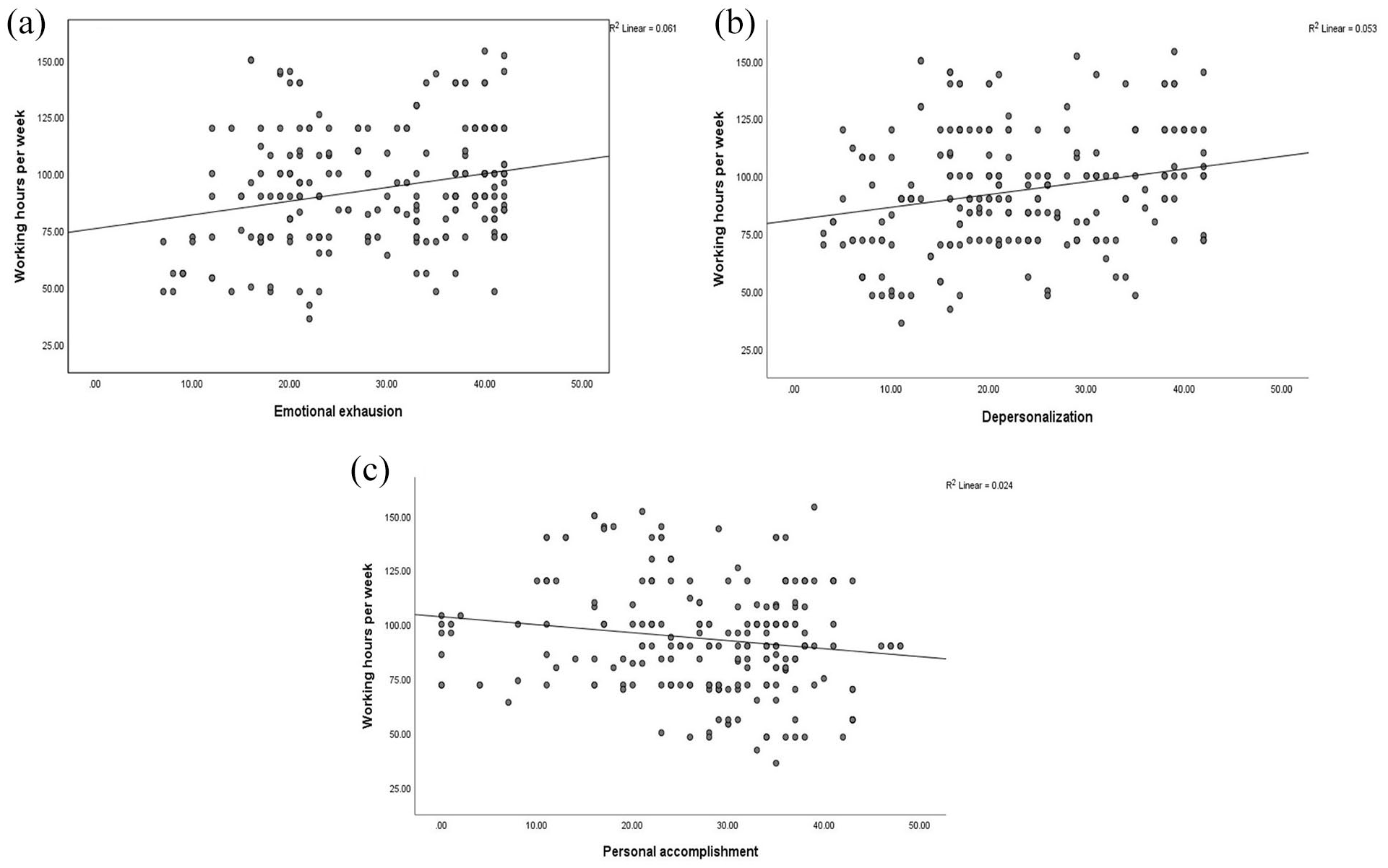
Correlation between MBI subscales and working hours per week: (a) Emotional exhaustion, (b) Depersonalization, and (c) Personal accomplishment.
Discussion
Egypt, like other countries, was hit by the COVID-19 pandemic with estimated positive cases of 104 thousand and about 6,000 deaths by the first week of October 2020 (Abdelhafiz, Ali, et al., 2020). This created a burden over the shoulders of healthcare professionals owing to the considerable novelty of such situations they had to face, combined with the uncertainty about the disease, ignorance of the definitive management, the severity of the clinical presentation, the fear of the higher possibility of patients mortality and the obligation to make the appropriate and ethical decisions regarding diagnosing and managing patients, which put even greater physical and mental stresses on the healthcare workers, especially if they are working in an overwhelmed healthcare system (Brooks et al., 2020; Health Workforce Burn-Out, 2019; Tsamakis et al., 2020; Xiang et al., 2020). Furthermore, trying to balance between patients’ care, their own needs, and caring for their families, healthcare professionals experienced more stress (Greenberg et al., 2020). This eventually resulted in increased physical and mental fatigue among healthcare workers, with a series of symptoms such as fear, anxiety, insecurity, and thoughts about quitting their career, which could be described as healthcare workers’ BOS (Chen et al., 2020; Shanafelt et al., 2020; Xiang et al., 2020).
In the current study, we identified a higher incidence of BOS measured using the MBI scale, where over 80% and about 50% of the participated resident doctors reported high scores in the DP and EE subscales, respectively. Regrettably, about half of the residents reported being subjected to incidents of perceived verbal or physical harassment and having COVID-19 infection during the study period. BOS subscales scores were higher in younger age, male residents, surgical departments, and showed a positive correlation with working hours per week.
Two studies were reported from Egypt by Abdelhafiz, Ali, et al. (2020) and Elghazally et al. (2021) on the effect of working during COVID-19 on BOS incidence among 220 and 201 healthcare professionals, respectively. In both studies, the authors included physicians regardless of their age or position; wherein one study, the mean age was 33.4 years, and in the other study, only 44% of the participants were below 30 years old; in both studies, resident doctors represented around 33% of the whole participants. While in the current study, we concentrated on evaluating the incidence in younger physicians (resident doctors), where all participants were resident doctors with a median age of 27 years.
In a study by Martini et al. (2004) evaluating BOS among 110 residents working in different medical specialties, the authors identified the first year of residency as one of the possible risk factors for BOS development; the same finding was found in the current study where the median EE and DP subscales were significantly higher in the younger age (⩽27 years); additionally, we found higher differences between MBI subscales median score when comparing fourth year residents with their relatively younger peers. Furthermore, Abdelhafiz, Ali, et al. (2020) reported that younger age was a predictor of BOS development, especially DP. Elghazally et al. (2021) detected a downward linear trend in the mean EE and DP for the age where younger physicians had the highest mean EE (28.3) and DP (22.9) compared to older groups. The increased BOS subscales scores in younger residents compared to their older colleagues could be explained by the fact that they are less experienced in handling stressful conditions (especially with the introduction of a new disease), having less knowledge increases their anxiety, and usually they are forced to work more hours.
The gender of the health professional has a variable effect on BOS development; in the current study where the number of male and female participants were equal, males reported significantly higher scores in DP and EE subscales than their female counterparts. At the same time, no difference was detected in PA subscale. On the contrary, Elghazally et al. (2021) found that males had significantly higher PA scores (32.7) compared to their female peers (28.9), p = .01, while the EE and DP subscales showed no difference between males and females. Moreover, Abdelhafiz, Ali, et al. (2020) identified the male gender as a predictor of DP while the female gender was a predictor of EE. The controversy among various reports indicates the complexity of the predicting factors on BOS development. Among the factors contributing to a higher incidence of BOS among females were working overnight shifts with prolonged working hours, which could negatively affect their social and family life, especially if they are married, which could eventually lead to a sense of fear and guilt (Abdelhafiz, Ali, et al., 2020).
We found that working in a surgical department led to higher DP subscales scores compared to the non-surgical department; this could be partially attributed to the fact that most of the surgical departments, although they held receiving elective surgical cases, they still have to deal with emergency cases, with extra precautions added to the usual procedures for fear of COVID-19 positive patients spreading the infection to their treating surgeons. The effect of medical specialties on the incidence of BOS was reported in previous studies wherein a study by Martini et al. (2004) where the incidence of BOS was about 50% among the participants, the highest incidence was reported among residents working in the obstetrics and gynecology department. In a metanalysis by Rodrigues et al. (2018), evaluating BOS incidence among 4,664 medical residents, the overall incidence was 35.7%, where surgical specialties and anesthesiology represented the highest incidence by 40.8%; followed by internal medicine and pediatrics, where the incidence was 30.0%. In the study by Elghazally et al. (2021) the authors showed that subspeciality did not affect EE and DP subscales. In contrast, PA showed higher scores among physicians working in anesthesia and surgical departments (p < .001; Elghazally et al., 2021).
Regarding being subjected to physical or verbal harassment, 58.3% of the residents participating in the current study reported being subjected at least once to these incidents from the patients or their relatives; those residents reported significantly higher DP and EE with lower PA compared to residents who were not subjected to any harassment. Abdelhafiz, Ali, et al. (2020) reported that about 41% of the participant in their study reported an incident of harassment during their study period; furthermore, they found that the BOS incidence nearly doubled when the healthcare professional was subjected to harassment by the patients’ families.
In the current study, we reported that 47.4% of the residents had COVID-19 infection, which could be related to PPE deficiency, as reported by Abdelhafiz, Ali, et al. (2020), and also could be attributed to longer working hours (with possible longer contact with COVID-19 patients) where 45.7% of the participants in the current study reported working more than 90 hours per week; we found both factors related to higher MBI subscale scores. It is noted that the reported working weekly hours for residents reported from western countries (United States, Canada, New Zealand, and Australia) ranged from 48 to 90 hours per week (Pattani et al., 2014).
In a cross-sectional study by Al Sulais et al. (2020) evaluating the psychological impact of COVID-19 on 529 physicians working in Saudi Arabia, they reported that most of the participants experienced negative psychological experiences in the form of a sense of worry (67.5%), sense of isolation (56.9%), and fear (49.7%). These feelings of fear and worry were more reported in female physicians, while more isolation was felt in physicians above 60 years. The authors concluded that COVID-19 possessed a profound negative psychological effect on physicians working in Saudi Arabia during the pandemic, which was affected by the physician’s age and gender (Al Sulais et al., 2020). In accordance with the previous study, we found that 71.7% of the residents experienced depression-like symptoms where they reported significantly higher scores in DP and EE subscales compared to residents who did not experience depression-like symptoms; furthermore, 73% of the residents thought about quitting their residency.
Although in the current study, we did not thoroughly investigate the exact reasons behind depression-like feelings (apart from other factors leading to BOS among the participants), however, Abdelhafiz, Ali, et al. (2020) alluded to some of the possible reasons where 38% of the participants in their study reported feeling less appreciated by the general population; they also mentioned that most of the participants complained of the disproportion between the effort they made and the salaries, to be noted that Egyptian physicians working in public hospitals (including governmental and university hospitals) are having lower salaries when compared with physicians working in the western or Gulf area countries (Abdelhafiz, Mohammed, et al., 2020; Schumann et al., 2019), which disproportionate with the effort and hazards related to their profession. Added to the burden, the stigma related to the COVID-19 patients and the healthcare workers taking care of such cases, wherein Al Sulais et al. (2020) study, the authors reported that about one-third of the participants showed concerns related to being stigmatized by being healthcare workers offering service to COVID-19 patients. Furthermore, in a study originating from Egypt, the authors reported that taxi drivers and restaurants refused to serve some Egyptian physicians working in COVID-19 isolation hospitals (Abdelhafiz & Alorabi, 2020); all previously mentioned factors could aggravate negative psychological impact among physicians.
A Cross-sectional online survey by Ruiz-Fernandez et al. (2020) was performed to determine the impact of the working area during the COVID 19 pandemic on healthcare professionals in Spain through evaluating the incidence of BOS among 506 physicians and nurses with an average age of 46.7 years; they showed higher BOS scores among personnel working in specific COVID-19 units and emergency departments. On the contrary, in the current study, we found that the zone where the residents were working did not affect any of the BOS subscales.
Limitations of the study
Firstly, we could not get a response from all residents working at the time of the study, which could add to the robustness of the results; however, the participants are still over the estimated sample size. Secondly, we did not report on the salaries and financial compensation the residents are gaining while working in the COVID-19 period and whether they are satisfied. Thirdly, we did not investigate the deaths due to COVID-19 infection among resident colleagues and families or relatives, which could significantly affect the BOS development.
Maslach (2003) phrased a compelling fight to compete against burnout as the following ‘If all of the knowledge and advice about how to beat burnout could be summed up in one word, that word would be “balance”: balance between giving and getting, a balance between stress and calm, a balance between work and home’.
Conclusions
The burnout syndrome is evident and considerably high among the residents working during the COVID-19 pandemic. Younger age, males, working in surgical departments, and those who got COVID-19 infection were most vulnerable. In addition, half of the residents were subjected to various kinds of harassment. Further strategies should be carried out to prevent and detect BOS development among healthcare professionals, especially residents, such as improving communication between coworkers and colleagues, creating support groups, and educating the general population about the effort paid by the healthcare workers to increase the sense of appreciation. Financial compensation and salaries for young physicians need reevaluation.
Footnotes
Author contributions
A.A.K. and A.A.F. carried out the study conception and design. A.A.F. and S.S.K. carried out data acquisition and assessment. D.G.M. carried out analysis and interpretation of data. O.F., A.A.K., A.A.F., S.S.K., and H.G.S. drafted the manuscript and designed the figures and tables, O.F., D.G.M., and H.G.S. did the critical revision. All authors discussed the results and commented on the manuscript. All authors read and approved the final manuscript. The first and the second authors contributed equally to the manuscript.
Availability of data and material
All the data related to the study are mentioned within the manuscript, however, the raw data are available with the corresponding author and will be provided upon a written request.
Ethical approval
This article does not contain any experimental studies with human participants or animals performed by any of the authors, and the ethical committee of our institution approved it: Faculty of Medicine, Assiut University, Egypt (IRB no.: 17300514; Telephone, Fax: +20882332278, ethics-committee12@yahoo.com, IRB-Asyut@aun.Edu.eg, ![]() ), Study setting: Assiut University Hospital, Assiut, Egypt.
), Study setting: Assiut University Hospital, Assiut, Egypt.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.