
Abstract
Public attitudes toward people with mental disorders determine their life chances and potential integration in society. In this article, we present results from a large representative study that aims to understand whether and how Bulgarian society stigmatizes people with mental disorder, and how demographic characteristics relate to certain types of attitudes. The CAMI III instrument was the basis for the specific research design. The article presents two types of analysis of the data. Firstly, Factor analysis revealed three factors which partially coincide with original categories of the CAMI III Scale – Factor 1 ‘Authoritarianism and Social Restrictiveness’, Factor 2 ‘Benevolence and Community Mental Health Ideology’, and Factor 3 ‘Liberalism’. Secondly, a one-way ANOVA test was carried out, taking the assigned factor scores as dependent variable, on one hand, and demographic and social-economic characteristics as independent variables, on the other. Results reveal that people between 18–24 and over 75 years old are the most authoritarian and socially restrictive, while those between 24–75 years old are the most benevolent. Our analysis show an influence of religion and ethnicity on authoritarianism and social restrictiveness, but on benevolence as well. Education, occupation, and profession is related to the scores of the factors. The results correspond to findings from studies form other contexts but reveal underrepresented aspects such as 1. socio-economic characteristics – ethnicity and religion; 2. the socializing role of the institutions in the formation of the image of the mentally ill among different age groups.
Introduction
Mental disorders are widespread in all societies and stigma against people with mental disorders is considered a universal phenomenon. However, attitudes vary in different contexts, societies, and social groups (see Koschorke et al., 2017, p. 77; Papadopoulos et al., 2013, p. 271), as they depend on the social construction of the disorders (Sévigny et al., 1999, p. 42) in terms of existing characteristics, images and stereotypes. Culture is the background for the formation of notions of mental disorders, yet mental health institutions also imply certain framing of attitudes toward people with mental disorders and provide the basis for structural discrimination (Link et al., 2004, p. 530) ‒ a problem which is underrepresented in most studies. For example, the practice of certification for work still exists in Bulgaria; and it is structural discrimination by definition. This practice nourishes the view that people with mental disorders cannot work and others should take care for them. Generally speaking, the images of people with mental disorders are formed by a complex mixture of factors, such as cultural contexts, demographic specifics, and institutional notions regarding those people.
Stigma is one of the main topics of research on public perceptions, as far as stigma and the resulting discriminatory attitudes predetermine the life chances of people with mental disorders. If we use Erving Goffman’s (2009) classical concept of stigma, it designates the difference based on possession of a negative characteristic, which has the ability to reduce the social identity only to this characteristic and thus discredit the individual (p. 3). However, Goffman (2009) notes that the language of relationship is more important than that of attribute (p. 3), pointing out the fact that stigma is a label. Stigma arises in the process of social interaction – between professionals and people with mental disorders, between people with mental disorders and members of the society, and so on. Therefore, we can assume that public sentiment and everyday interactions are essential for the integration of people with mental disorders in the larger society. This makes the study of the public perceptions of mental disorders relevant.
Research on the public perceptions of mental disorders focuses on public stigma – stereotypes, internalized prejudices, and declared discriminatory behavior toward people with mental disorders (see Corrigan et al., 2003, p. 163, 2011, pp. 25–27). Stigmatizing images of people with mental disorders, the notion that they are dangerous and unpredictable, or incompetent (Seehan et al., 2017, pp. 43–44), for instance, evoke different societal reactions – social exclusion and restriction, or paternalism (supporting greater control or coercion in treatment) (p. 46). This article presents the results from a descriptive study that seeks to understand whether and how the Bulgarian society stigmatizes people with mental disorders and how demographic characteristics relate to certain types of attitudes.
Measures
Selection of the instrument of analysis
The approaches to the study of public attitudes toward mental disorders are extremely diverse, cover different types of issues, and utilize a multitude of frameworks. They can be divided into analyzing the stigma on a collective and on an individual level. In short, the former deal with the perception and declared behavior toward the group of people with mental disorders (referred to as ‘mentally ill’) and ex-psychiatric patients. These methodologies register common stereotypes about the group at the collective level, beliefs about those labeled with an undesirable characteristic, expectations from them and the degree of separation; the studies rarely comment on different diagnoses. This type of approach is useful in the Bulgarian context insofar as the media-produced images contain primarily the most general qualifications – ‘mentally ill’, ‘ex-psychiatric patient’, and so on, and as it captures what researchers call public stigma (Martinova & Dimitrova, 2020). The individual-level stigma studies focus on vignettes that depict individuals whose characteristics include either a description of a diagnosis, or the diagnosis itself, or mention a previous history of treatment. Researchers of stigma suggest that this type of tool is closer to interactive situations and is a better predictor of individual behavior. The focus is on the extent to which respondents evaluate the described characteristics as mental illness – that is to say, the extent to which they label diagnostic descriptions and behavior as ‘mental illness’ (Link & Stuart, 2017, p. 9; Rabkin, 1974, p. 11). However, these questionnaires are more sensitive to diagnoses and probably work better among populations that have more knowledge about mental disorders, and the knowledge on the subject is limited in the Bulgarian society. There are some advantages of the collective level stigma questionnaires for the purposes of the present study (national representative survey): they are shorter, allow comparisons with studies of different contexts, test labels that are broadly used by the common public, and capture the attitudes toward the institutional care. These are the reasons for choosing the CAMI III (Community Attitudes Toward the Mentally Ill) instrument.
The CAMI III questionnaire is widely used in countries around the world (Angermeyer et al., 2003; Högberg et al., 2008; Jee et al., 2006) and among different populations: the general population (Ewalds-Kvist et al., 2013; Ingram et al., 2019; Letovancová et al., 2017; Mehta et al., 2009; Winkler et al., 2016) and different segments of the population, such as medical professionals (nurses, physicians, psychiatrist, etc.) (Al-Awadhi et al., 2017; Sathyanath et al., 2016; Sévigny et al., 1999; Winkler et al., 2016), medical students (Alaqeel el al., 2020; Telles-Correia, 2015; Tong et al., 2020), cultural groups within a given society (Papadopoulos et al., 2013), or populations of particular cities or neighborhoods/areas in the cities (Brockington et al., 1993; Taylor & Dear, 1981; Taylor et al., 1979; Wolff et al., 1996).
This instrument allows making a distinction between those who accept and reject people with mental disorders, and has a strong predictive value for accepting or rejecting community-based care reforms (Taylor & Dear, 1981, p. 225; Taylor et al., 1979, p. 286). The scale does not cover all dimensions of the attitudes toward the mentally ill, but tries to ‘focus on those dimensions that are the most strongly evaluative and hence best discriminate between those positively and negatively disposed toward the mentally ill and mental health facilities’ (Taylor & Dear, 1981, p. 228). The original scale consists of 40 statements, each 10 of them presenting one of four different ideologies – authoritarianism, benevolence, social restrictiveness, community mental health. The personal level of agreement with each statement is evaluated on a 5-point Likert scale. The separate ideologies can be summarized, as follows: 1. The authoritarianism scale represents the perception of the mentally ill as a stigmatized category (different from normal people), which need to be coercively institutionalized; 2. The benevolence scale represents a more tolerant and humanistic anti-custodial attitude, but supports the paternalistic role of the institutions; 3. The social restrictiveness scale represents the perception of the mentally ill as dangerous and supports social distance; and 4. The community mental health scale represents acceptance of the deinstitutionalization and its principles, such as: therapeutic value of the community and locating mental health facilities in the community (Taylor & Dear, 1981, p. 228; see also Papadopoulos et al., 2013, p. 272).
Context of use of the CAMI III instrument
Studies of the public attitudes toward people with mental disorders began in the 1950s (Rabkin, 1974, p. 10). The deinstitutionalization movement made visible the problem of rejection of former psychiatric patients and its consequences such as restriction of work opportunities, education, and social contacts (Rabkin, 1974, p. 15). As everyday interactions are a possible source for changes of publicly accepted stereotypes, they are the basis for reintegration of people with mental disorders in the society. However, an unprepared society and its reactions, as Taylor and Dear note, may increase fear and resistance to community mental healthcare reforms, and reject people with mental disorders (Taylor & Dear, 1981, p. 225; Taylor et al., 1979, p. 283). Research demonstrates that the society’s negative attitudes grew along with the intensification of the deinstitutionalization processes. The image of the dangerous and unpredictable mentally ill person started to dominate, and so discriminatory behavior determined the fate of people with mental disorders and lead to a social response that is well summed up by the phrase ‘not in my backyard’ (Link et al., 1999, p. 1328). While CAMI III is broadly used to assess the changes of public attitudes after the onset of deinstitutionalization in western context, in ex-communist countries, and more precisely in Central and Eastern Europe, fewer surveys of public attitudes toward people with mental disorders have been conducted (Letovancová et al., 2017; Winkler et al., 2016). For example, a study in the Czech Republic shows a more stigmatizing attitude than that in Catalonia and England (Winkler et al., 2016, p. 1272), and a higher level of acceptance of hospital-based mental healthcare by medical doctors (Winkler et al., 2016, p. 1272). A Serbian survey shows that stigma is greater in a hospital-based institutional system, and a Croatian one reveals a generally positive attitude, but with a paternalistic view of the patient and emphasized social distance (Totic et al., 2012; Vučić Peitl et al., 2011, p. 143). Research on the former communist countries rarely links and discusses the institutional type of care inherited from the communist regime and the image of people with mental disorders (Sévigny et al., 1999).
In Bulgaria, mental health institutions have never been a priority for public authorities. The initiated reforms of the healthcare system in the 2000s have not affected the psychiatric practices, institutions and care significantly (Hinkov & Nakov, 2015, p. 1). The Bulgarian psychiatric system is criticized strongly by international organizations. The legacy of the socialist system still exists. The socialist institutional psychiatry was influenced by the main trends in the Soviet Union and was built primarily on the principles of segregation and paternalism, despite the declared and formal attempts to create dispensaries (Nakov & Dimitrova, 2022, pp. 70–71). The community type of care has never been the organizing principle in Bulgaria, and it has never been fully accepted (Nakov & Dimitrova, 2022, p. 74). As a result of the continuity of the socialist-era practices and the specifics of the healthcare reform (relying mainly on financial instruments), mental healthcare is fragmented, organized around institutionalization in hospitals and quasi-hospitals, there is a lack of social services or desire to integrate and provide rehabilitation for people with mental disorders (Hinkov & Nakov, 2015, pp. 11, 32–33).
Adaptation of the CAMI III instrument in Bulgaria
As already mentioned, the chosen public opinion research instrument has been applied primarily in countries where a psychiatric care reform has been implemented. This requires the introduction of several reservations. Firstly, while the instrument is applied in societies where community mental health reforms have begun and originally measures resistance against mental health facilities, in Bulgaria it is used to study public attitudes toward future reforms and the readiness of the Bulgarian population to accept the mentally ill in the society. This requires the omission of some items from CAMI III. Secondly, the instrument was originally applied at the city level, but in the Bulgarian case, it was used to capture the attitudes of the general population. This makes it possible to compare attitudes in different types of settlement, but also requires the omission of some statements (the ones relating to community mental health ideology, for example). Thirdly, some of the statements are difficult to understand in the Bulgarian context – this necessitated a change in order to capture a more general meaning related to the specific ideologies. This is the practice in other contexts as well (Sévigny et al., 1999, pp. 44–45).
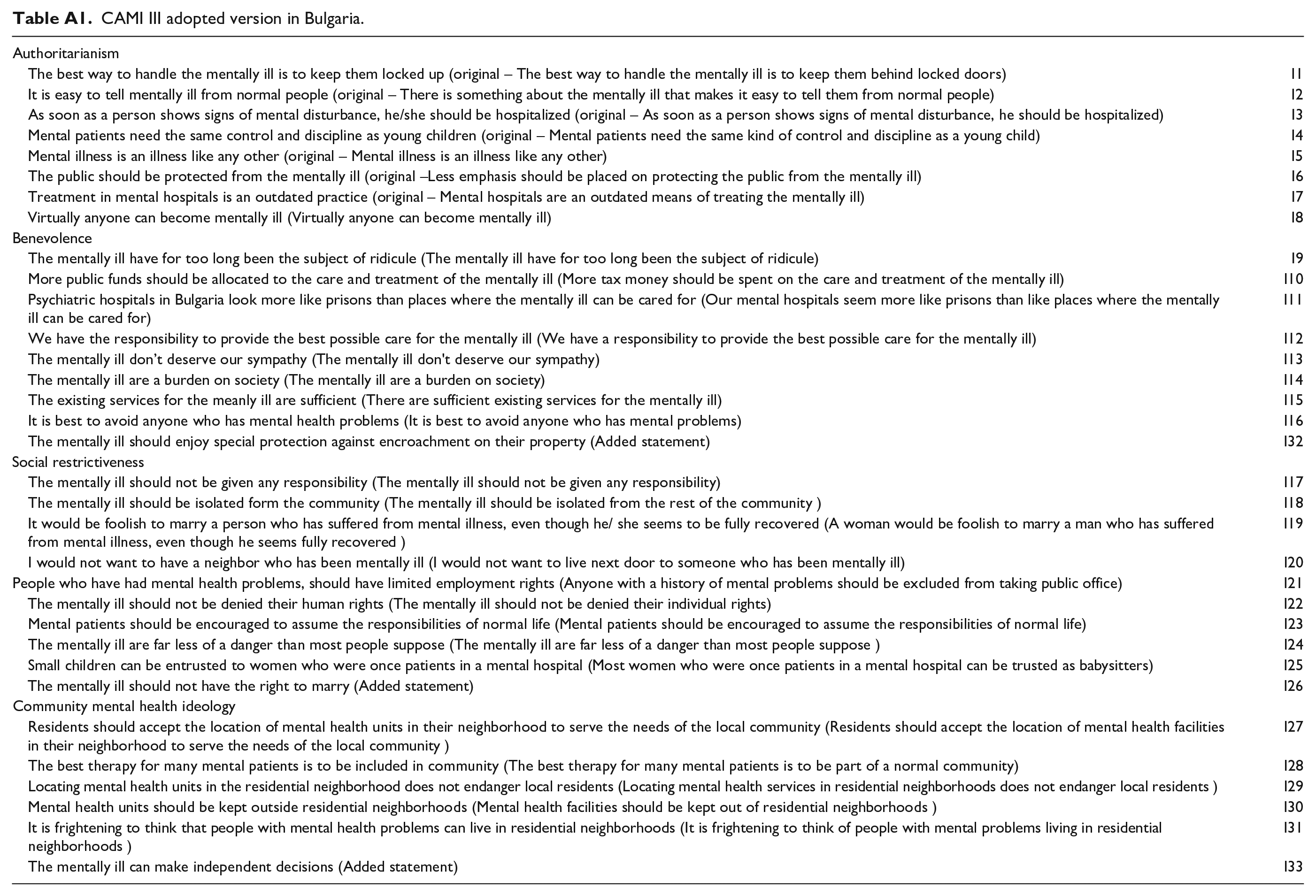
The questionnaire for Bulgaria includes 25 translated statements from the original version of CAMI III which comprises 40 statements. Five statements were adapted to indicate a more general notion and to correspond to the current global and Bulgarian context. For instance, ‘А woman would be foolish to marry a man who has suffered from mental illness, even though he seems fully recovered’ was substituted by ‘It would be foolish to marry a person who has suffered from mental illness, even though he or she seems to be fully recovered’, as same-sex marriages are recognized in some European societies. Similar modifications are made in the versions for China and Kuwait (Al-Awadhi et al., 2017, p. 33; Sévigny et al., 1999, p. 47). The statement ‘Anyone with a history of mental problems should be excluded from taking public office’ was modified to indicate a more general meaning – ‘People who have had mental health problems should have limited employment rights’. In the statement ‘The mentally ill should not be denied their individual rights’ ‘individual rights’ was substituted by ‘human rights’, because the term is more contemporary and universal. ‘Most women who were once patients in a mental hospital can be trusted as babysitters’ was adopted as ‘Small children can be entrusted to women who were once patients in a mental hospital’ because the role and the term ‘babysitter’ do not correspond to the Bulgarian reality (Sévigny et al., 1999, p. 47). ‘Less emphasis should be placed on protecting the public from the mentally ill’ was changed to have the opposite meaning – ‘The public should be protected from the mentally ill’, because the translated version was grammatically difficult to comprehend and because during the initial testing of the questionnaire, this statement was not understood by the respondents. Some words and expressions were also adapted in Bulgarian: ‘tax money’ was replaced by ‘public money’, ‘our mental hospitals’ by ‘mental hospitals in Bulgaria’, ‘live next door’ by ‘have a neighbor’, and ‘locked doors’ by ‘locked up’ (Table A1).
Three new statements were integrated in the questionnaire: ‘The mentally ill should not have the right to marry’, ‘The mentally ill should enjoy special protection against encroachment on their property’, and ‘The mentally ill can make independent decisions’. The first statement was added to measure stronger authoritarian views that we expected to encounter in the country due to institutional framework of mental health, some practices in the system and lack of informational campaigns. The second, because in Bulgaria the mentally ill are not sufficiently protected against embezzlement of their property by their relatives. The third, because a paternalistic model is sustained in Bulgarian psychiatric care and this statement corresponds to а more paternalistic attitude.
Some socio-demographic questions from the European Social Survey were added to the questionnaire – sex, age, education, occupation, working status, marital status, ethnicity, religion, type of settlement, number of household members, number of children under 18, income, subjective assessment of income, and so on. Questions about the social construction of mental disorders, familiarity with persons with mental disorders, personal experience with mental illness, were also added but they are not going to be discussed here.
The following procedure was applied for the translation of the questionnaire – it was translated into Bulgarian, the translation was discussed at a meeting with experts – sociologists, psychiatrists, economists, and others. Thus, a second, modified version of the questionnaire was produced. The second version was translated back by a professional translator. The back translation was discussed by the same experts to establish compliance with the original version. After the final phrasing was set, 10 pilot interviews with people from the general population were conducted to test the common understanding of the CAMI III statements and questions.
Sample
The sample is a multi-stage stratified random probability sample. The goal was to obtain a sample that is representative of the adult population living in Bulgaria. Two stratification criteria are applied: 1. National coverage at district level: 28 administrative districts that are consolidated in the six planning regions; 2. National coverage by type of settlement (capital, regional town, small town, and village). The basis for the sample is the official data of the National Statistical Institute on the structure of the population in Bulgaria from the last census in 2011 (with update corrections according to annual publications of the National Statistical Institute).
Steps of the sample
First step, in each region, settlements were selected randomly so that they are representative of the respective administrative area. The survey was conducted in all administrative districts (in proportion to their weight) and in all types of settlements in them – large cities, small towns and villages. Second step, according to the sample size (N = 1,000), the required number of nests (100) were selected, so as in each nest 10 respondents were interviewed in order to avoid intra-nesting correlation and minimize systematic deviations. Respectively, the larger the settlement, the greater the number of nests in it. The starting points for the survey in each nest were randomly selected. Third step, the adult member whose last birthday was the closest to the date of the interview was selected from each sampled household. The research was conducted by Alfa Research agency by face-to-face computer-assisted interviews. The interviewers were preliminary trained to work with the questionnaire.
Sample size
According to the last available census from 2011, the adult population (18 years of age and above) includes 6,177,660 people. The set volume of the sample was 1,000 effective interviews, providing for a standard deviation of ±3.1% at a confidence interval of 95%. Quality checks were carried out on 20% of the respondents. The response rate was 82%.
The study complies with all ethical principles and was approved by the Ethics Commission of Sofia University ‘St. Kliment Ohridski’.
Methods of analysis
We conducted an exploratory factor analysis using the CAMI-III scale as adapted for Bulgaria which measures attitudes toward the mentally ill. The initial inventory included 33 items, 27 of these remained in the final inventory and 6 were excluded because they did not load high enough into any of the factors. The factor analysis was carried out using STATA.
Finally, three factors were formed with the view of maximizing the scale reliability using Cronbach’s α. The cutoff point on communality coefficients is 0.4, but only 1 factor loads less than 0.45, and only 6 out of 27 factor loadings have a module below 0.5.
To perform the initial factor analysis, we used the principal-factor method and forced the creating of four factors corresponding to the original number of factors defined in the CAMI-III inventory. The other methods were found less appropriate because the data were not normally distributed and the factors displayed uniqueness significantly larger than 0. The lowest eigenvalue among the four factors was the last that just marginally exceeded 1. However, the resulting factors had lower scale reliability and were more difficult to interpret in the Bulgarian context than a model with only three factors, which are presented in Table 1.
Factors included in the model.
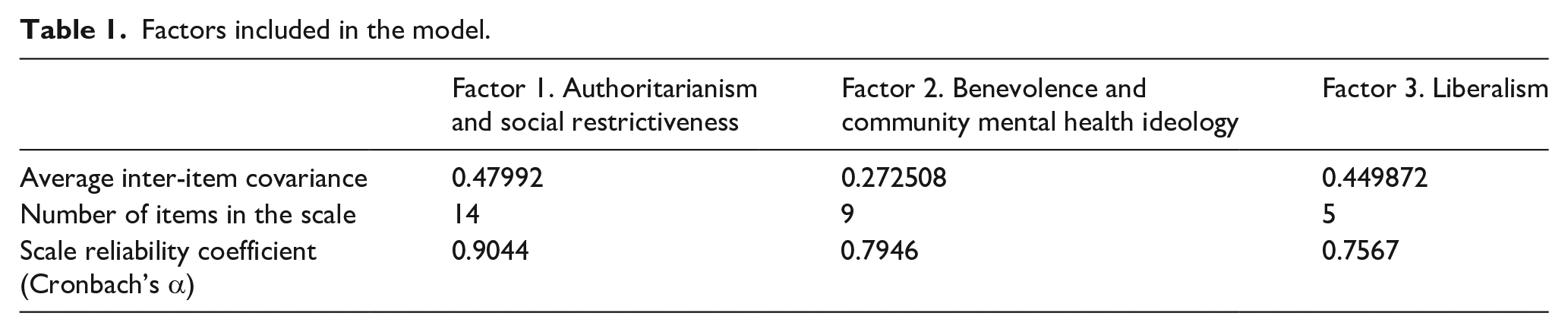
Factor scores for each individual were computed as averages of the corresponding variables from the inventory weighted by the factor loadings for each measured variable, that is, each of the 27 items in the scale with absolute factor loadings above 0.4. The mean was used as a cutoff point.
One-way ANOVA was carried out taking the assigned factor scores as a dependent variable and 12 independent variables representing various demographic and socio-economic characteristics of the respondents: type of settlement the respondent lives in, age group, marital status, sex, ethnicity, religion, occupation, profession, education and subjective well-being, size of the household, and whether the household includes children. The equal-variances hypothesis was tested using Bartlett’s test of homogeneity with a rejection cutoff point at p > .01. After that, the ANOVA descriptive comparison of between-group means was carried out to outline groups with distinctly higher and lower means.
Analysis
Our analysis reveals three factors (Table 2). Factor 1 is Authoritarianism and Social restrictiveness. The two original ideologies represent a single dimension. This is in line with the statement of the authors of the original scale: ‘Authoritarianism and social restrictiveness are approximately equally correlated with the first factor and to a lesser extent with the fourth factor. This provides some evidence that these two scales perhaps represent a single dimension’ (Taylor et al., 1979, p. 285). Other studies indicate the same (Brockington et al., 1993, pp. 94–95).
Statements included in the Factors.
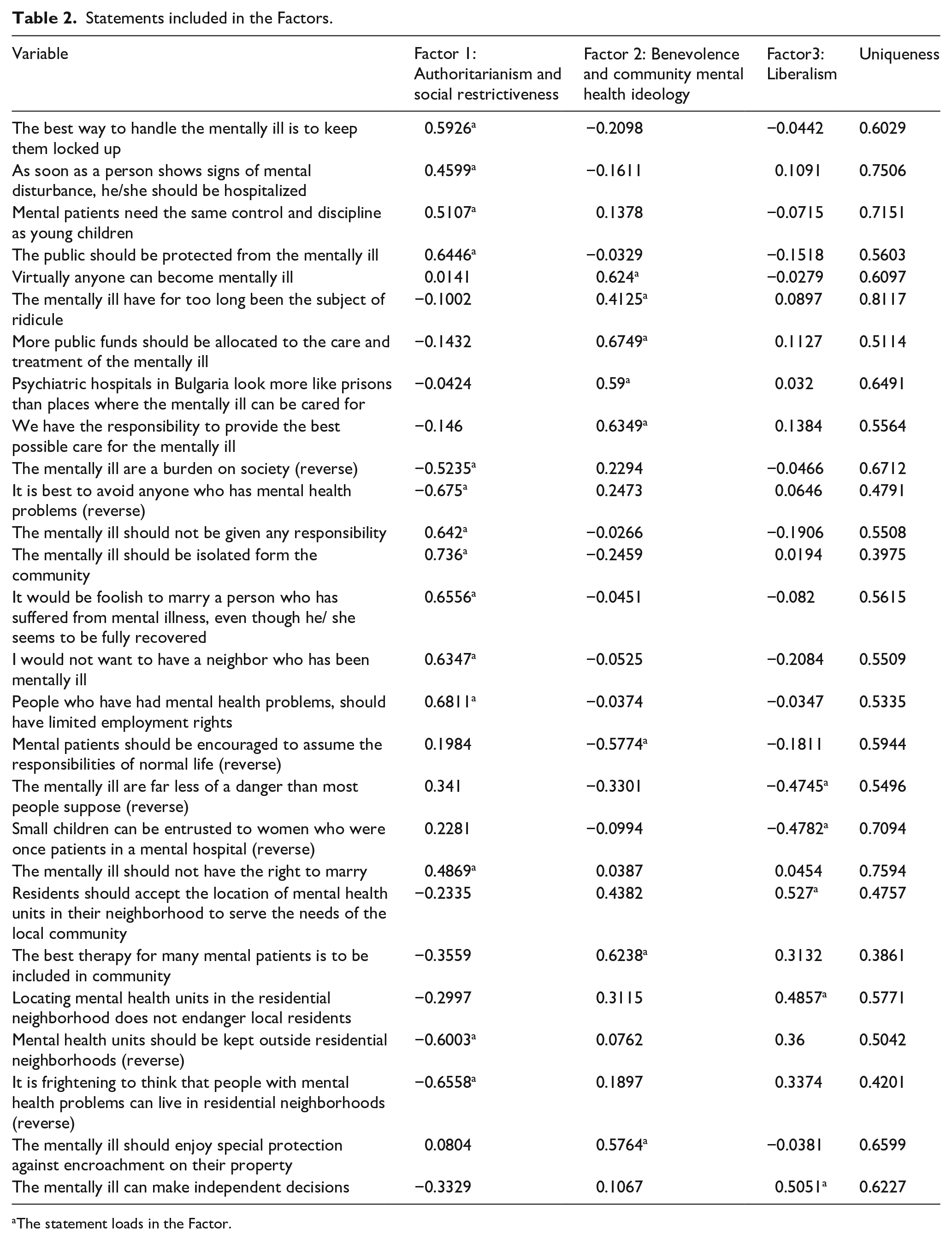
The statement loads in the Factor.
Factor 1 includes statements supporting the view that there is a big and lasting difference between mentally ill people and other people, which makes them unpredictable and dangerous, and fully justifies their separation from the society and reduces their ability to interact with others. Statements from the social restrictiveness scale dominate the formation of Factor 1 and authoritarianism is its aspect. Mental hospitals serve as a tool for social exclusion and paternalism. The main image of the mentally ill is that of a dangerous individual – danger triggers negative emotional reactions and declarations of action. This blocks future reform and the possibility of integration – as it is impossible to think of the mentally ill as independent members of the society and to reintegrate them into the society.
Factor 2 is Benevolence and community mental health ideology. It includes an attitude toward the mentally ill which recognizes their similarity to all other members of the society. In this ideology, the mentally ill have unjustly been separated from the society and deprived of protection for a long time. They should be encouraged to fully recover and integrate into the society and they should be cared for in the recovery process. The attitude is one of acceptance and support. In the Bulgarian case, Factor 2 includes Benevolence and some aspects of Community mental health ideology together. Here the image of the mentally ill is not radically different from that of all other members of the society (in contrast to the case with the thesis of danger). Factor 2 represents the more comprehensive notion of integration of people with mental disorders through their social inclusion, through locating mental health units in residential areas, as well as providing special protection to the category of people with mental disorders. This is probably due to the fact that no large-scale mental health reform has been undertaken in Bulgaria (in contrast to other countries where studies with the CAMI III questionnaire were conducted). Thus benevolence is the more general model from which the desire to integrate people with mental disorders into the society derives, yet here a paternalistic attitude toward people with mental disorders is maintained.
Factor 3 is Liberalism. The view presented here is that the mentally ill are self-sufficient and community mental health facilities should be accepted, because people with mental illness do not endanger the society and no social restriction is supported.
Demographic and socio-economic relationships with factor scores
The mean factor scores were calculated and ANOVA analysis was performed. The three factors revealed in the Factor analysis and their scores showed complex relations with demographic and social characteristics of the respondents (Table 3).
One-way ANOVA and Bartlett’s test.
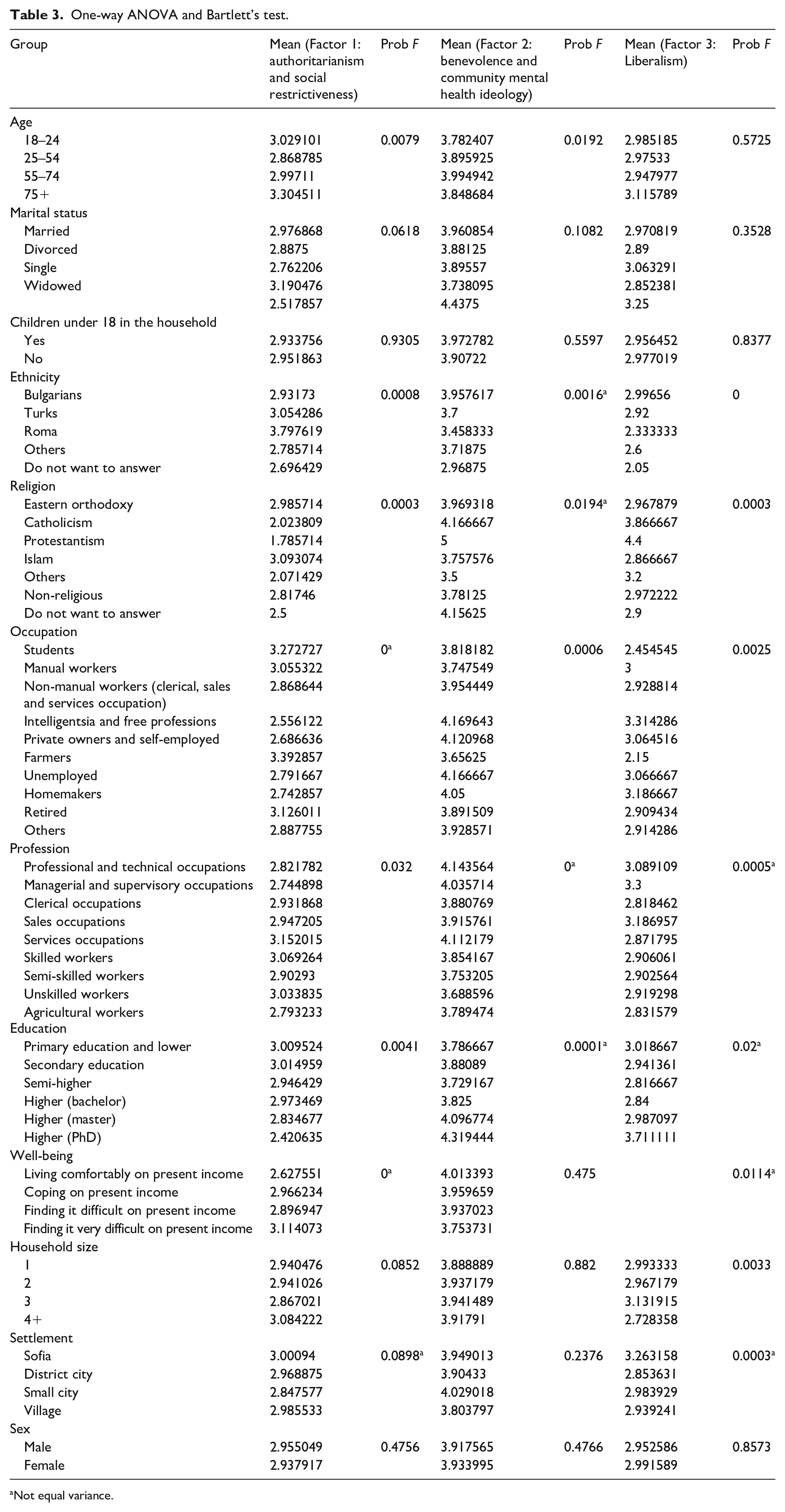
Not equal variance.
Authoritarianism and social restrictiveness
There is a relationship between Authoritarianism and age. Older age brings a higher score of the Factor. People belonging to age groups 25–54 and 55–74 years appear less authoritarian. Тhose in the age groups 18–24 and over 75 are the most authoritarian. Marital status also affects Factor 1. Single and married people are the most authoritarian and socially restrictive, compared to widowed ones. Ethnicity is related to Authoritarianism – it appears that authoritarian views on the mentally ill are somewhat more prevalent in the Roma community, Turks and Bulgarians follow them. Religion is also significant in relation to authoritarianism. The means of the score for Eastern Orthodoxy and Islam are much higher than for Protestantism, Catholicism, and other religions. Professional groups affect Factor 1 – some have higher values, for example, services occupations, skilled and unskilled workers. The lowest mean is among Managerial and supervisory occupations. Education also influences authoritarianism – the lower the educational level, the higher the value of authoritarianism. Household size also affects Factor 1 – people from bigger households (over 4) are more authoritarian.
Occupation affects the score for Authoritarianism – farmers, students, and retired are the most authoritarian. Bartlett’s test shows that the variances are likely different, so this result should be interpreted with a bit of caution. Variances appear different also for the categories ‘Well-being’ and ‘Settlement types’. The lowest the subjective income, the highest the scores of Factor 1. People ‘finding it very difficult on the present income’ have the highest result. People from bigger cities are more authoritarian. Having children under 18 in the household and the respondent’s sex do not affect the score of Factor 1.
Benevolence and community mental health ideology
Age group affects the mean score of Factor 2. The most benevolent ones are people aged 25–74, and the least benevolent are those aged 18–24 and over 75. Occupation affects Factor 2 – the most benevolent are the groups of intelligentsia and free professions, private owners and self-employed, unemployed and homemakers. Manual workers and farmers are the least benevolent.
There is no relationship between Benevolence and marital status, whether there are children under 18 in the household, subjective well-being, household size, settlement, and sex. Ethnicity (Bulgarian, Turks, and Others are more benevolent than Roma), religion, profession (people at higher professional positions being more benevolent than those at lower ones), education (higher level of education increases the mean score of Benevolence) showed relationship, but Bartlett’s test demonstrated different variances.
We can conclude that Benevolence is a more general and socially acceptable ideology and this is the reason why there are not a lot of differences between the different groups.
Liberalism
People with Bulgarian and Turkish ethnic origin display more often liberal attitudes toward the mentally ill; liberal attitudes are less widespread among the Roma. Religion affects the mean score of Factor 3 – Protestants and Catholics are more liberal than Orthodox Christians and the non-religious, who tend to have liberal attitudes less often. Occupation influences Factor 3 –people from intelligentsia and free professions are the most liberal while farmers and students are the least liberal occupational groups. Household size also affects Liberalism – people from bigger households (over 4 members) are less liberal than the others.
Liberalism showed no relationship with the age group (although the mean score of Factor ‘L’ in the age group over 75 is higher), sex, marital status, or children under 18 in the household. Education, well-being, settlement (with increased liberalism in the group from the capital Sofia), and profession correlate with the score of Factor 3, but Bartlett’s test demonstrated different variances.
Discussion
Two types of personal characteristics are discussed here in relation to the attitude toward the mentally ill – demographic and socio-economic variables in the Bulgarian version of the CAMI III questionnaire. Their relationship with the mean scores of the Factors revealed in this analysis was studied using one-way ANOVA.
Our results are consistent with previous studies which show that elderly people are: 1. more authoritarian and socially restrictive, 2. less benevolent and community mental health oriented (Brockington et al., 1993, p. 96; Ewalds-Kvist et al., 2013, p. 361; Letovancová et al., 2017, p. 3; Madianos et al., 1987, p. 161; Taylor & Dear, 1981, pp. 232–233; Wolff et al., 1996, p. 187). Some of the studies that we mentioned reveal that this attitude can also be found among younger population, and that populations are the most tolerant in their mature age (Brockington et al., 1993, p. 97; Ingram et al., 2019, p. 1380; Letovancová et al., 2017, p. 3; Winkler et al., 2016, p. 1268). This finding is similar to our results – it seems that elderly and young people in Bulgaria are almost equally intolerant.
There are not sufficient explanations why age is related to attitudes. The authors of the CAMI III scale suggest that the demographic relationships can be considered through the concept of ‘life-cycle status’ (Taylor & Dear, 1981, p. 233). Another suggested explanation is that elderly people ‘are more likely to be conventional and to reject odd behavior’ (Ewalds-Kvist et al., 2013, p. 361). It seems that this is a dominant, but limiting and essentializing approach in the interpretation of data. Although some of the demographic and socio-economic variables show similar results in different societies, we should take into account the cultural and institutional specificities. It seems pivotal to note another interpretation – that the respondents of the older generations were socialized in a different context of institutional care, which presupposes certain views on people with mental disorders. This does not imply essentialization of the age category, but thinking of it as culturally shaped. The finding that young people are also intolerant can be explained with insufficient education in the field of health-related topics in Bulgaria.
Although a large number of studies show a link between gender and attitudes – women are more tolerant toward people with mental disorders (Ewalds-Kvist et al., 2013, p. 366; Letovancová et al., 2017, p. 3; Taylor & Dear, 1981, p. 233), our study does not confirm this relationship and is consistent with Brockington et al. (1993, p. 98). Ewalds-Kvist et al. (2013) claim that women are more tolerant, but more afraid (p. 366). As Taylor and Dear mentioned ‘The direction of the effect shows more sympathetic attitudes among female respondents. This emerges on three of the four scales. No significant difference occurs for social restrictiveness’ (Taylor & Dear, 1981, p. 233). In Bulgaria, the strongest factor is Authoritarianism and Social Restrictiveness – this is probably the reason why gender shows no significant influence in our study.
Although some authors have found highly significant differences among marital status groups (Taylor & Dear, 1981, p. 233), our study is not consistent with them. As Brockington et al. (1993, p. 98), we did not confirm the importance of the marital status variable. It has some influence only on authoritarianism. Similarly, having children under 18 in the household does not have predictive value in Bulgaria, which is consistent with other studies (Brockington et al., 1993, p. 98). Probably this is due to the fact that the mental health reform has not started yet in Bulgaria and changes at local level cannot be felt.
The findings about socio-economic variables are similar to other studies – people with higher social status are more tolerant. The higher the education, the more benevolent and less authoritarian the attitude (Brockington et al., 1993, p. 96; p. 161; Letovancová et al., 2017, p. 3; Madianos, 1978; Wolff et al., 1996, p. 187). Low professional status is also related to negative attitudes toward the mentally ill (Brockington et al., 1993, p. 96; Letovancová et al., 2017, p. 3; Wolff et al., 1996, p. 187). However, there are inconsistencies that need to be explained – for example, populations from services occupations turn out to be more authoritarian in our study. Some of the conclusions concerning occupational groups overlap with those for age groups – students and the retired are more intolerant partially replicating similar conclusions for the young and the elderly.
In contrast to other studies, we cover more socio-economic variables: among those ethnicity and religion have proven to be essential. As outlined in other articles, ethnicity plays a significant role. In Bulgaria, it shapes the attitudes in several ways similarly to findings from studies in England (Papadopoulos et al., 2013, p. 275; Wolff et al., 1996, p. 187). Firstly, people from the Roma community more often display attitudes that are authoritarian and socially restrictive, less benevolent and less liberal. Secondly, people from groups with lower occupational status (manual workers, for example), with lower education and lower subjective assessment of income are less tolerant, and this coincides with the socio-economic situation of the Roma in Bulgaria. Thirdly, religion has a significant contribution to determining more authoritarian and socially restrictive attitudes. In our sample, 26% of Roma are Orthodox, 32% are Muslims, 29% are not religious, 13% do not want to answer. This is a clue for interpretation in two directions. Firstly, when ethnicity coincides with stigma, the process of discrimination and exclusion of ethnic minorities leads to deprivation that nourishes more negative attitudes (see also Ingram et al., 2019, p. 1383). Secondly, there is a clue that there are ‘different conceptual models’ about mental illnesses, based on distinct knowledge among ethnic and religious groups (see also Wolff et al., 1996, p. 190). More research is needed in this direction.
The belief variable has also been underrepresented in current studies. Taylor and Dear outline the differences between ‘denominations’: Of groups distinguished in the survey, the Pentecostal and Greek Orthodox groups emerge as the most authoritarian in contrast to the Baptists and Salvation Army, who expressed the least authoritarian views. Correspondingly, the Baptist, together with United Church, adherents held the most benevolent attitudes, again in contrast to the least benevolent views of the Pentecostal and Greek Orthodox members. (Taylor & Dear, 1981, p. 234)
We can confirm that the Orthodox and Muslims express generally less tolerant attitudes compared to other groups (see also Reta et al., 2016). This suggests the need for a more in-depth study of cultural differences among these religious groups.
Conclusion
In this article, we studied factors formed on the basis of the CAMI III questionnaire and their relationship with demographic and socio-economic variables such as: sex, age, education, occupation, working status, marital status, ethnicity, religion, type of settlement, number of household members, number of children under 18 in the household, income, subjective assessment of income, and so on. One-way ANOVA was performed. The total predictiveness of the demographic and socio-economic variables was not particularly strong but it was not negligible either.
Our results show that populations in their mature age, with higher social status (with higher education and professional status) in Bulgaria are more tolerant. Our research did not find any link between gender, marital status, having children under 18, on one hand, and attitudes toward the people with mental disorders, on the other. In Bulgarian context, we found that ethnicity and religion are relevant variables when attitudes toward the mentally ill are concerned. People from the Roma community display attitudes that are less tolerant more frequently. Representatives of different religious groups also differ significantly in their attitudes toward people with mental disorders ‒ the Orthodox and the Muslims express generally less tolerant attitudes compared to other groups.
The groups that the analysis reveals could be considered in the context of future policies aiming at the de-stigmatization of people with mental disorders in Bulgaria. Our results are important insofar as they shed light on group characteristics and contextual factors that are insufficiently considered such as the specific attitudes toward the mentally ill within various ethnic groups and religious communities, and so on, and Bulgaria’s profile as a post-socialist country that has not initiated a deep mental health reform.
Footnotes
Appendix
CAMI III adopted version in Bulgaria.
| Authoritarianism | |
| The best way to handle the mentally ill is to keep them locked up (original – The best way to handle the mentally ill is to keep them behind locked doors) | I1 |
| It is easy to tell mentally ill from normal people (original – There is something about the mentally ill that makes it easy to tell them from normal people) | I2 |
| As soon as a person shows signs of mental disturbance, he/she should be hospitalized (original – As soon as a person shows signs of mental disturbance, he should be hospitalized) | I3 |
| Mental patients need the same control and discipline as young children (original – Mental patients need the same kind of control and discipline as a young child) | I4 |
| Mental illness is an illness like any other (original – Mental illness is an illness like any other) | I5 |
| The public should be protected from the mentally ill (original –Less emphasis should be placed on protecting the public from the mentally ill) | I6 |
| Treatment in mental hospitals is an outdated practice (original – Mental hospitals are an outdated means of treating the mentally ill) | I7 |
| Virtually anyone can become mentally ill (Virtually anyone can become mentally ill) | I8 |
| Benevolence | |
| The mentally ill have for too long been the subject of ridicule (The mentally ill have for too long been the subject of ridicule) | I9 |
| More public funds should be allocated to the care and treatment of the mentally ill (More tax money should be spent on the care and treatment of the mentally ill) | I10 |
| Psychiatric hospitals in Bulgaria look more like prisons than places where the mentally ill can be cared for (Our mental hospitals seem more like prisons than like places where the mentally ill can be cared for) | I11 |
| We have the responsibility to provide the best possible care for the mentally ill (We have a responsibility to provide the best possible care for the mentally ill) | I12 |
| The mentally ill don’t deserve our sympathy (The mentally ill don’t deserve our sympathy) | I13 |
| The mentally ill are a burden on society (The mentally ill are a burden on society) | I14 |
| The existing services for the meanly ill are sufficient (There are sufficient existing services for the mentally ill) | I15 |
| It is best to avoid anyone who has mental health problems (It is best to avoid anyone who has mental problems) | I16 |
| The mentally ill should enjoy special protection against encroachment on their property (Added statement) | I32 |
| Social restrictiveness | |
| The mentally ill should not be given any responsibility (The mentally ill should not be given any responsibility) | I17 |
| The mentally ill should be isolated form the community (The mentally ill should be isolated from the rest of the community ) | I18 |
| It would be foolish to marry a person who has suffered from mental illness, even though he/ she seems to be fully recovered (A woman would be foolish to marry a man who has suffered from mental illness, even though he seems fully recovered ) | I19 |
| I would not want to have a neighbor who has been mentally ill (I would not want to live next door to someone who has been mentally ill) | I20 |
| People who have had mental health problems, should have limited employment rights (Anyone with a history of mental problems should be excluded from taking public office) | I21 |
| The mentally ill should not be denied their human rights (The mentally ill should not be denied their individual rights) | I22 |
| Mental patients should be encouraged to assume the responsibilities of normal life (Mental patients should be encouraged to assume the responsibilities of normal life) | I23 |
| The mentally ill are far less of a danger than most people suppose (The mentally ill are far less of a danger than most people suppose ) | I24 |
| Small children can be entrusted to women who were once patients in a mental hospital (Most women who were once patients in a mental hospital can be trusted as babysitters) | I25 |
| The mentally ill should not have the right to marry (Added statement) | I26 |
| Community mental health ideology | |
| Residents should accept the location of mental health units in their neighborhood to serve the needs of the local community (Residents should accept the location of mental health facilities in their neighborhood to serve the needs of the local community ) | I27 |
| The best therapy for many mental patients is to be included in community (The best therapy for many mental patients is to be part of a normal community) | I28 |
| Locating mental health units in the residential neighborhood does not endanger local residents (Locating mental health services in residential neighborhoods does not endanger local residents ) | I29 |
| Mental health units should be kept outside residential neighborhoods (Mental health facilities should be kept out of residential neighborhoods ) | I30 |
| It is frightening to think that people with mental health problems can live in residential neighborhoods (It is frightening to think of people with mental problems living in residential neighborhoods ) | I31 |
| The mentally ill can make independent decisions (Added statement) | I33 |
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research is funded by the Bulgarian National Scientific Fund – by the competition program of BNSF – 2018 for fundamental scientific research, under the project “Mental Health and Social Inequalities” (№КП-06-Н25/1 – 13.12.2018 г).