
Abstract
Background:
Different stages of a physician’s career may be associated with different types of mental health impairment.
Aims:
This study aimed to compare symptoms of anxiety, depression, and stress and their associated factors among medical students, medical residents, and physicians.
Methods:
A cross-sectional study was conducted. Data collection included sociodemographic data, religiosity (Duke University Religion Index), and mental health (21-item Depression, Anxiety and Stress Scale – DASS-21) data. The comparison between the groups was performed using ANOVA, and the associated factors were evaluated via linear regression models.
Results:
The sample consisted of 1,417 participants: 778 medical students, 190 medical residents, and 468 established physicians. Medical students had significantly higher depression, anxiety, and stress scores as compared to medical residents and established physicians. However, regarding DASS 21 scores, no significant differences were found between established physicians and medical residents. The factors associated with mental health in the different groups showed that being married and male were associated with better mental health among physicians and medical residents, while the factors of male gender, being in later years of the course, and lower religious attendance were associated with better mental health in students.
Conclusion:
Medical students had worse mental health outcomes when compared to residents and established physicians. Interventions are needed to minimize suffering during medical education and career.
Introduction
Several studies have shown that depression and anxiety symptoms are observed in medical students, medical residents, and established physicians, generally with greater intensity than in the general population (Moutinho et al., 2019). However, every phase in a medical student and physician’s life has distinct characteristics, which allow a better understanding of the problem.
In medical students, for example, there is a worsening in mental health soon after joining the course (Dyrbye et al., 2005, 2006). This is related to several factors, such as distance from family and friends, less time for leisure, the need to cope with suffering, grades, and tests, and a poor learning environment (Dyrbye et al., 2005, 2006; Paro et al., 2010). These factors have multiple consequences for students, including a drop in academic performance, substance abuse, increased cynicism, reduced empathy, low self-esteem, suicide attempts, and future professional impacts (Dyrbye et al., 2005, 2006; Paro et al., 2010).
Medical residents are exposed to an environment where there is a high demand for results, the need to develop many skills in a short period of time, great responsibility regarding their work with patients, exhausting workload, and the moment of transition from student to physician (Pereira-Lima & Loureiro, 2015; Schwenk, 2015) resulting in high levels of stress, sleep deprivation, and decreased quality of life (McManus et al., 2002; Schwenk, 2015; Toral-Villanueva et al., 2009). Consequently, greater emotional and physical exhaustion, increased cynicism, substance abuse, and a worsening in patient care and attendance can occur (McManus et al., 2002; Pereira-Lima et al., 2019; Schwenk, 2015).
Finally, established physicians are also exposed to several factors that impact their mental health, such as long shifts and night shifts, a high workload, daily medical failures, the patients’ suffering, a high demand for technical skill, the pressure of making swift decisions, financial concerns, and institutional bureaucracy (Gong et al., 2014; Wallace et al., 2009). Due to these factors, established physicians also suffer from great emotional burden, which leads to high rates of depression, burnout, substance abuse, and suicide, in addition to a higher risk of suffering work-related and automobile accidents (Wallace et al., 2009).
Different stages of a physician’s career may be associated with different types of mental health impairment. However, although numerous studies have been conducted considering medical students (Dyrbye et al., 2005; Moutinho et al., 2017; Paro et al., 2010), medical residents (Toral-Villanueva et al., 2009) and physicians (Gong et al., 2014; Wallace et al., 2009), these groups have usually been studied separately, without being compared to each other.
The present study aims to compare symptoms of anxiety, depression, and stress and their associated factors among medical students, medical residents, and established physicians who were trained at the same medical school in Brazil.
Material and methods
Study design and participants
A cross-sectional and comparative study was conducted during the period from July 2017 to March 2020. Data were collected from three distinct populations (medical students, medical residents, and established physicians), as approved by the Research Ethics Committee of the University Hospital of the Federal University of Juiz de Fora (HU-UFJF), Brazil, under opinion numbers 790.822, 57905716.4.1001.5133, and 94348818.5.0000.5133.
Eligibility criteria
The eligibility criteria were adopted with respect to the characteristics of each group evaluated, as shown below:
(a)
(b)
(c)
In all the groups, the participants who did not fill out the informed consent form or who filled out the questionnaires incompletely were excluded (in other words, only complete questionnaires without missing values in the depression, stress and anxiety scales were considered eligible).
Procedures
For the present study, the approach to the different type of participants was different for each group, because each group of participants had specific characteristics due to being in different contexts and locations. The details of the data collection process are as follows:
During the application of the questionnaires, whether face-to-face or virtual, all participants were guaranteed the confidentiality of the collected data.
Instruments
The questionnaires used for the present study were completed by the participants in approximately 15 min and were composed of the following:
Statistical analysis
The statistical analysis was performed using SPSS software, version 21 (IBM Corporation, Armonk, NY, USA). First, a descriptive analysis of sociodemographic and religious data was conducted, in addition to analyzing the percentage of depression, anxiety, and stress symptoms, respecting the cutoffs suggested by Lovibond (Lovibond & Lovibond, 1995) (for depression, these cutoffs are: score 0–4, normal; 5–6, mild; 7–10, moderate; 11–13, severe; ⩾14, extremely severe; for anxiety: 0–3, normal; 4–5, mild; 6–7, moderate; 8–9, severe; ⩾10, extremely severe; and for stress: 0–7, normal; 8–9, mild; 10–12, moderate; 13–16, severe; ⩾17, extremely severe).
Second, the sociodemographic data and the depression, anxiety, and stress symptoms were compared in relation to the different groups (students, residents, and established physicians) through the chi-square test for categorical variables and an independent-measures analysis of variance (ANOVA) with Bonferroni’s post-hoc correction for continuous variables. A correlation between the scores of each group’s DASS-21 subscales was also performed, using Pearson’s correlation coefficient.
Finally, an evaluation of the factors associated with the participants’ mental health was conducted through multivariate stepwise linear regression models, using the DASS-21 subscales as dependent variables, and gender, age, years in medicine, religiosity, and marital status as independent variables. For the analyses, p < .05 was considered significant.
Results
The sample of the present study consisted of 1,417 participants: 778 medical students (77.1% of the medical school’s total student population), 190 medical residents (90% of the total residents registered at the hospital), and 468 established physicians who were UFJF alumni (35.9% of those who graduated from UFJF Medical School between 2001 and 2012).
Table 1 shows the comparison between the groups regarding sociodemographic data and religiosity. The sample included more women (51.5% among physicians, 59.6% among residents, and 52.7% among students), and the mean ages varied according to the group (37.3 for established physicians, 28.4 for residents, and 21.9 for students). There were significant differences between the groups regarding marital status (established physicians were more often married), age (established physicians were older), and years of medical practice (more years among established physicians). Regarding religiosity, residents had greater organizational and intrinsic religiosity than the other groups, while students had less non-organizational religiosity than the other groups.
Comparison between physicians, medical residents, and medical students regarding sociodemographic data and religiosity.
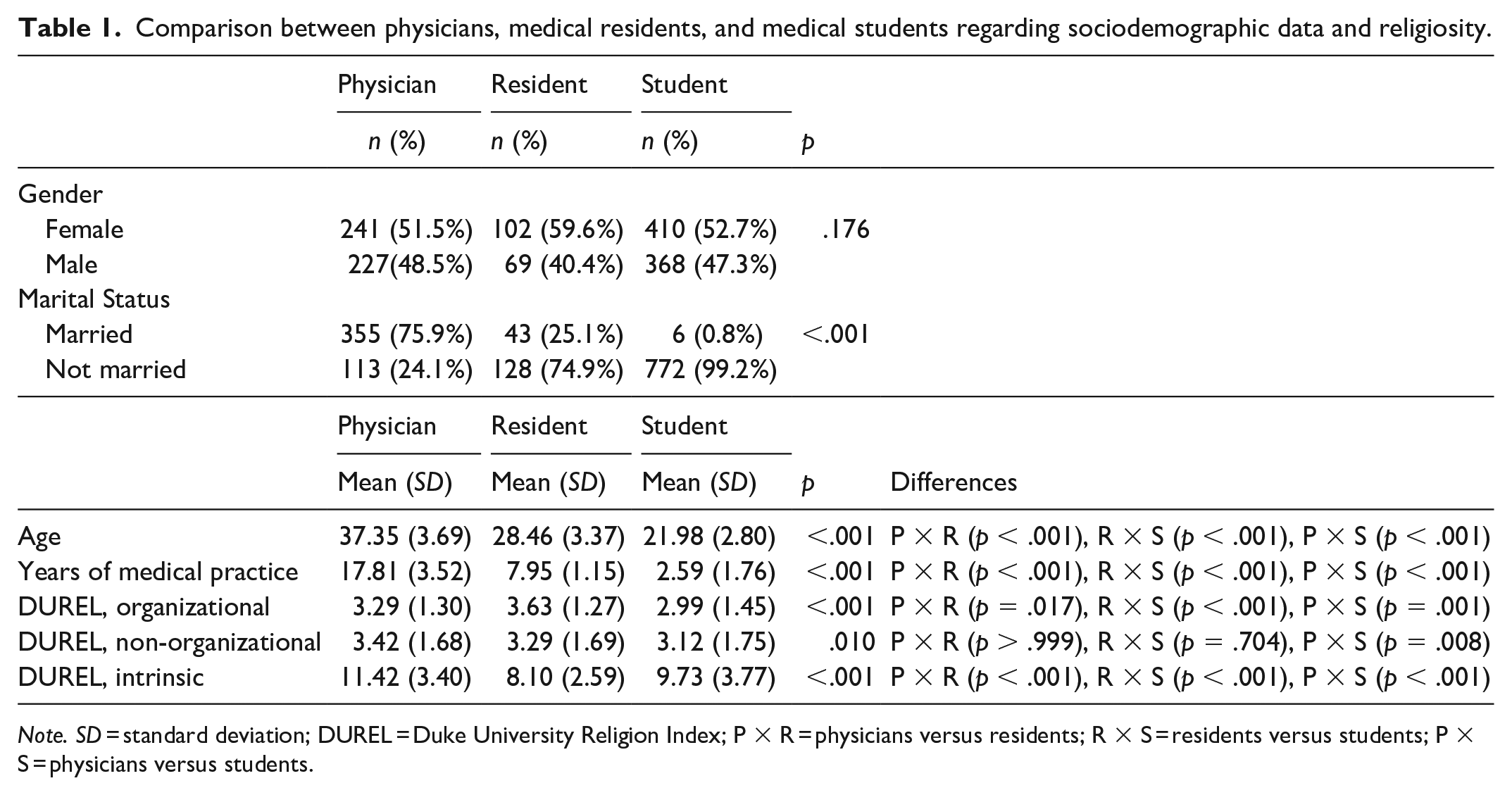
Note. SD = standard deviation; DUREL = Duke University Religion Index; P × R = physicians versus residents; R × S = residents versus students; P × S = physicians versus students.
The comparison between the groups regarding mental health symptoms and the different levels of symptoms is better described in Table 2. It can be observed that medical students had significantly higher scores of depression, anxiety, and stress as compared to residents and established physicians. However, no significant differences were found between established physicians and residents regarding DASS-21 scores. Regarding prevalence, it is important to note that more severe symptoms showed a higher association with students, while the absence of symptoms occurred more often in established physicians and medical residents.
Comparison between physicians, medical residents, and medical students regarding symptom levels of depression, anxiety, and stress.

Note. SD = standard deviation; DASS-21 = 21-item Depression, Anxiety, and Stress Scale; P × R = physicians versus residents; R × S = residents versus students; P × S = physicians versus students.
The correlations between the mental health symptoms are shown in Table 3. In all groups, there were significant correlations between the DASS-21 subscales, with Pearson correlations ranging from .635 to .741.
Correlation of DASS-21 subscales for established physicians, medical residents, and medical students.
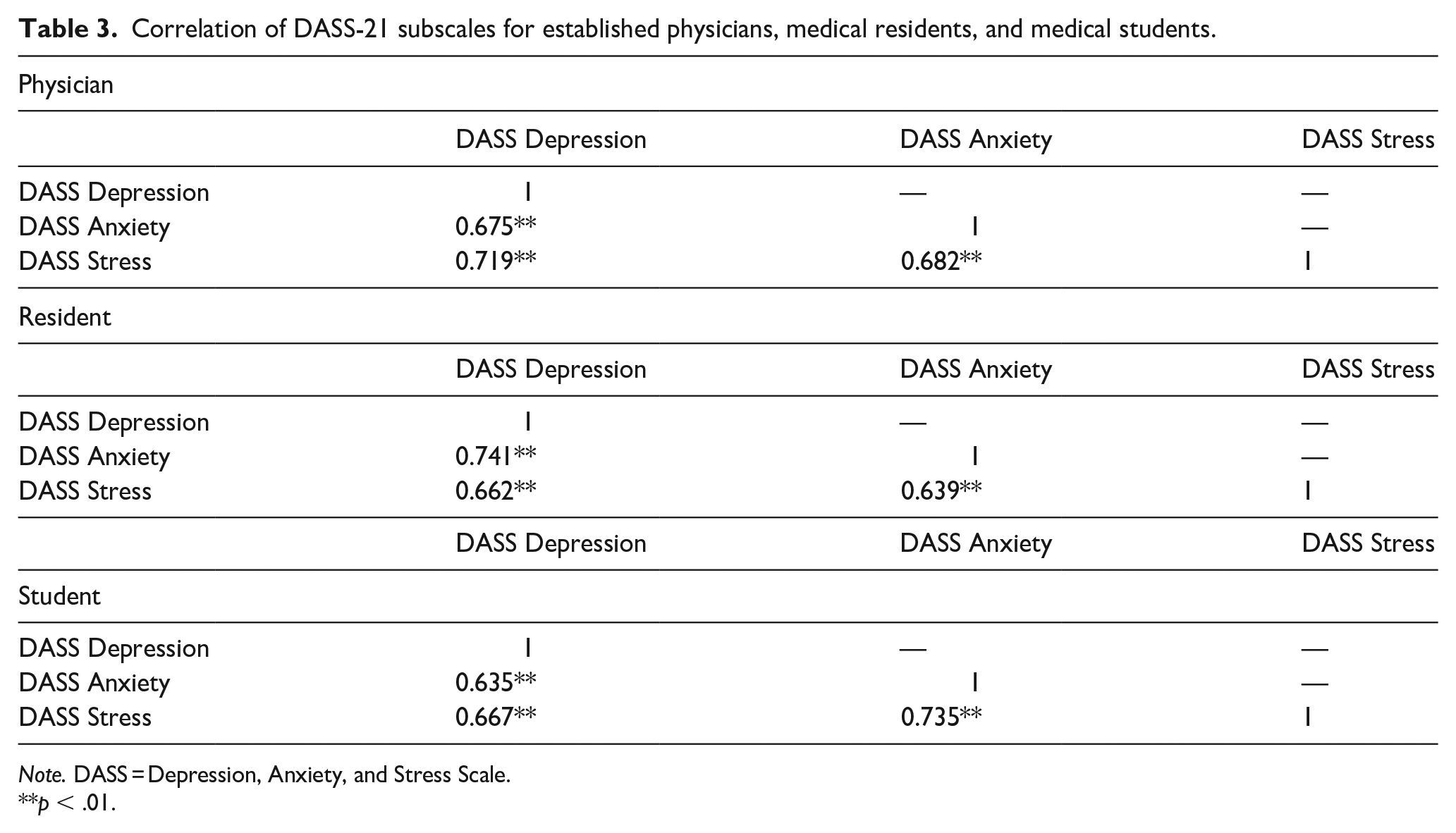
Note. DASS = Depression, Anxiety, and Stress Scale.
p < .01.
Finally, Table 4 presents the factors associated with mental health for each group according to the stepwise linear regression models. Among established physicians, being married was a protective factor for depression, anxiety, and stress; being male was also associated with lower stress levels in this population. Among residents, no factor was associated with depression symptoms, whereas being married was a protective factor against anxiety, and being male was a protective factor against stress. In the student population, there was no factor associated with depression symptoms, but being male and being in medical school for longer were associated with lower symptoms of stress and anxiety. Conversely, religious attendance was associated with higher stress among students.
Stepwise linear regression* of the factors associated with mental health issues for established physicians, medical residents, and medical students.

Note. DASS = Depression, Anxiety, and Stress Scale; SE = standard error
Variables analyzed in the stepwise model: gender, marital status, years of medical experience, Duke University Religion Index (DUREL) 1, DUREL 2, intrinsic DUREL, age.
Discussion
The results of this study showed greater symptoms of depression, anxiety, and stress in medical students as compared to medical residents and established physicians. However, when comparing the symptoms of depression, anxiety, and stress in residents and established physicians, no significant differences were found. These findings in the three populations that received training at the same institution and in the same geographic region can help in understanding their mental health issues suffered by medical students, residents, and established physicians and encourage strategies to minimize these problems.
Previous studies on this subject are very distinct, and the prevalence of mental health problems depends significantly on the instruments and the sample used. Recent systematic reviews on this subject have shown to be very heterogeneous, while lacking precise conclusions, because they evaluated participants from several different contexts and cultures, making an accurate comparison between the groups impossible and leading to conflicting results (Mata et al., 2015; Rotenstein et al., 2016).
Attempting to minimize these problems, some studies compared groups at different stages of medical education and career. A large North American study with approximately 13,000 participants observed that depression symptoms and suicidal ideation were significantly more frequent in students than in medical residents and early career physicians. Meanwhile, burnout was greater in residents and fatigue was greater in physicians (Dyrbye et al., 2014). Another similar North American study with approximately 2,000 participants (Goebert et al., 2009) found a higher prevalence of depression in medical students as compared to medical residents.
However, other studies have found different results. A study conducted in Nepal with 651 participants (Pokhrel et al., 2020)compared medical students and residents, and found that depression was more common in residents, while anxiety was more common in students. A Canadian study evaluating 1,681 participants (Toews et al., 1997) found that stress levels and other mental health issues were higher in graduate science students as compared to residents and medical students. However, when comparing mental health issues only among residents and medical students, students continued to have worse mental health outcomes. The results of these previous studies are largely congruent with the sample in the present study, showing that students tend to suffer from more depression, anxiety, and stress symptoms relative to other groups.
The justification for these findings is not yet fully understood. In the case of medical students, factors such as entering university, the transition to ‘adulthood’, the high demand for grades and results, the large amount of educational content, and the little time available for studying tend to result in anxiety and stress (Damiano et al., 2020; Dyrbye et al., 2005, 2006). In residents (i.e. student to physician transition), the excessive concern for grades and results starts to be replaced by the responsibilities inherent to medical care and the role of a physician who is responsible for a patient and has full ethical and legal attributions (Pereira-Lima & Loureiro, 2015; Schwenk, 2015). Finally, physicians who have already completed residency and are inserted in the labor market are in a more consolidated phase of their lives. Nevertheless, they have financial concerns, need to manage their families, and tend to work in multiple institutions at once (Gong et al., 2014; Wallace et al., 2009). This continuum of the medical career seems, at least according to the findings of this study, to generate less damage to mental health as the physician becomes more experienced and more distant from training periods, which tend to demand a lot from trainees.
The present study also evaluated factors associated with mental health in the three groups and found results comparable to the existing literature. The female gender was associated with worse mental health in all the three groups. These results are in agreement with the scientific literature (Dahlin et al., 2005; Mao, Zhang et al., 2019; Smith et al., 2007) and reveal a greater susceptibility of women with regard to suffering from mental health issues from the medical career as a whole.
Another factor closely associated with mental health for physicians and residents was marital status, as married people had better mental health outcomes (Yan et al., 2011). This may be related to the social and family support, the partner’s perception that the person needs help, the adherence to treatment of mental health issues, greater financial support, and the fact that people with worse mental health tend to have more difficulty in maintaining stable relationships (Wong et al., 2018).
In this study, among medical residents, being married acted as a protective factor only for anxiety, whereas among medical students, there was no significant difference. Marital status also did not affect the prevalence of depression, anxiety, or stress among students according to previous studies (Jadoon et al., 2010; Smith et al., 2007).
In medical students, the later years of the course were associated with better mental health. These results are congruent with the previous literature, in which most studies tended to find worse mental health in medical students at the beginning of the course (Moutinho et al., 2017; Radcliffe & Lester, 2003). This may be justified by the initial difficulties of joining medical school and the extensive syllabus with limited practice, a common occurrence in the context of medical courses in Brazil (Lucchetti et al., 2018).
Finally, religiosity was associated with worse mental health only in medical students, while in the other groups, there was no significance. Although this finding seems to be unusual as many studies in this field suggest better mental health outcomes in the more religious (Moreira-Almeida et al., 2014), other studies have found similar results (Lupo & Strous, 2011; Machado et al., 2018). In the present study, the probable justification for these findings is in the cross-sectional design, in which it is possible that students who are experiencing stress turn to supportive activities such as religious meetings as a way of coping with their mental health problems.
The present study has some limitations. First, this was a cross-sectional study, which precludes conclusions about causality. Second, the participants of the three groups were different and were not followed up to assess the changes in their mental health symptoms over time. Finally, despite the lower response rate of established physicians in relation to residents and students, this rate was similar to the only other study that, to the authors’ knowledge, evaluated these three groups (Dyrbye et al., 2014).
Conclusion
This study investigated the stage at which individuals are more vulnerable during medical education and career, finding that medical students had worse mental health outcomes when compared to residents and established physicians. Factors such as gender, marital status, years of study, and religious attendance were associated with mental health. Further research is needed to understand these differences and propose interventions to minimize suffering during medical education and career.
Footnotes
Acknowledgements
None.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.