
Abstract
Aim:
to assess the efficacy of psychosocial interventions delivered through task-sharing approaches for preventing perinatal common mental disorders among women in low- and middle-income countries.
Methods:
We conducted a systematic review of randomized controlled trials following a prespecified protocol registered in the Open Science Framework (osf.io/qt4y3). We searched MEDLINE, Web of Science, PsycINFO, and Cochrane Central Register of Controlled Trials (CENTRAL) through June 2022. Two reviewers independently extracted the data and evaluated the risk of bias of included studies using the Cochrane risk of bias tool. We performed random-effects meta-analyses and rated the certainty of evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.
Results:
We included 23 studies with 24,442 participants. At post-intervention, task-shared psychosocial interventions, were effective in preventing the development of mental disorders in general (RR 0.57, 95% CI [0.35, 0.91]), and specifically depression (RR 0.51, 95% CI [0.35, 0.75]), but not anxiety disorders (RR 0.46, 95% CI [0.06, 3.33]). Similarly, psychosocial interventions reduced psychological distress (SMD −1.32, 95% CI [−2.28, −0.35]), and depressive symptoms (SMD −0.50, 95% CI [−0.80, −0.16]), and increased parenting self-efficacy (SMD −0.76, 95% CI [−1.13, −0.38]) and social support (SMD −0.72, 95% CI [−1.22, −0.22]). No effect was detected for anxiety symptoms at post-intervention. At follow-up the beneficial effects of interventions progressively decreased.
Conclusions:
Psychosocial interventions delivered through the task-sharing modality are effective in preventing perinatal common mental disorders and fostering positive mental health among women in low- and middle-income countries. However, our findings are tentative, due to the low number of preventative intervention strategies considering outcomes as the incidence of mental disorders, especially in the long-term. This evidence supports calls to implement and scale up psychosocial prevention interventions for perinatal common mental disorders in low- and middle-income countries.
Keywords
Introduction
Mental health promotion, prevention, and treatment of perinatal common mental disorders (PCMDs) is considered a global priority for achieving the United Nations Sustainable Development Goals (SDG) related to health, well-being and gender equality (Lule et al., 2005; Miranda & Patel, 2005; Patel et al., 2018).
PCMDs, which include depression and anxiety disorders, are prevalent conditions in both high income countries (HICs) and low- and middle- income countries (LMICs), and represent a significant public health concern (GBD 2019 Mental Disorders Collaborators, 2022). These disorders often begin during the perinatal period, which is frequently accompanied by significant psychological, social, financial, and physical changes (Howard et al., 2014). A review of studies in LMIC studies identified socioeconomic disadvantage, a lack of intimate partner empathy, and insufficient emotional support, as risk factors for PCMDs (Fisher et al., 2012). Despite this, maternal mental health is still a globally neglected issue. Evidence-based mental health and psychosocial support interventions (MHPSS) for preventing and treating common mental disorders in the perinatal period exist (Tol et al., 2020), nevertheless their access remains a challenge in LMICs. There persists a severe gap between individuals in need of mental health support and those who actually receive it (WHO, 2018a), mainly because of the paucity of resources in terms of skilled staff and inequitable access to mental health services (WHO, 2020). A strategy developed to overcome this challenge is task-sharing which entails the employment of trained and supervised non-specialized providers for the delivery of evidence based psychosocial interventions (Baron et al., 2016; Rahman et al., 2013).
A growing body of evidence on MHPSS interventions delivered through task-sharing approaches in the perinatal period has emerged in the past few years, but most studies focused on treatment rather than prevention (Clarke et al., 2013; Rahman et al., 2013; Tol et al., 2020). Prevention aims at reducing the likelihood of future mental disorders with the general population or with people who are identified as being at risk of disorder (e.g. women victims of intimate partner violence or with some level of maternal distress) addressing risk and protective factors that are predictive of mental health conditions (Eaton, 2019; Institute of Medicine, 1994). Prevention is further subdivided on the basis of the population targeted, into universal (i.e. strategies that can be offered to the general public or a whole population group), selective (i.e. strategies that are targeted at subpopulations whose risk of developing a mental disorder is significantly higher than that of the rest of the population) and indicated (i.e. strategies that are targeted at smaller groups of the population at high-risk for mental disorders and that might already show some signs of disorder without meeting criteria of a formal diagnosis) (Purgato et al., 2020; Tol et al., 2015).
Against this background, the aim of the present systematic review and meta-analysis was to assess the efficacy of psychosocial interventions delivered through task-sharing approaches for preventing common mental disorders among women in the perinatal period living in LMICs.
Methods
The present systematic review was conducted following the Cochrane Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) 2020 guidelines for data reporting (J. Higgins et al., 2022; Page et al., 2021). The protocol for this review was registered in the Open Science Framework (osf.io/qt4y3).
Randomized Controlled Trials (RCTs) were eligible for inclusion if they met the following criteria: (1) they were conducted in LMICs, defined according to the World Bank criteria (World Bank Country and Lending Groups, 2022); (2) included women without any formal diagnosis of any mental disorders at the time the trial was conducted; (3) interventions were delivered during the perinatal period, defined as ‘the time frame from 1 year before to 18 to 24 months after the birth of the child’ (Helfer, 1987); (4) interventions incorporated any type of prevention interventions (universal, selective, indicated) (Institute of Medicine, 1994; Tol et al., 2015) with a psychosocial component (Carll, 2008) delivered by non-specialized providers through the task-sharing approach (i.e. trained and supervised by mental health specialists) (WHO, 2018b); (5) trials adopted any type of control group (i.e. no intervention, waiting list [WL], usual care, active controls).
Primary outcomes of this review were (a) proportion of participants with a diagnosis (or a proxy thereof, as assessed by scoring above a cut off for a screening tool) of any mental disorder at any timepoint post intervention, (i.e. 0–1 month after the intervention, 1–6 months post-intervention, 7–24 months post-intervention), depression, and anxiety disorders at post-intervention, determined according to the Diagnostic and Statistical Manual of Mental Disorders (DSM), International Classification of Diseases (ICD), or any other standardized criteria; (b) depressive symptoms, (c) anxiety symptoms and (d) generically assessed psychological distress assessed on rating scales. As promotive factors for mental health, we will also consider (e) parenting self-efficacy, and (f) social support at any timepoint as primary outcomes. Secondary outcomes included adverse events, psychological functioning and impairment, quality of life, and dropouts for any reason at any timepoint.
Search strategy and data collection
We searched MEDLINE, Web of Science, PsycINFO, and Cochrane Central Register of Controlled Trials (CENTRAL) from database inception to June 2022, without publication type or language restrictions. The searches were conducted combining terms indicative of the perinatal period, mental health, common mental disorders, psychosocial intervention, primary health care, community health workers, and LMICs, with filters for RCTs and research involving human participants. Electronic database searches were supplemented by a manual search of reference lists from relevant systematic review and meta-analyses related to this topic. For this review, we also cross-checked the search strategy of two systematic reviews recently published by Cochrane (Papola et al., 2020; van Ginneken et al., 2021). The full search string for all databases is provided in the Appendix B of the Supplemental Materials.
All records were screened by two independent authors (EP, CCa) using online software (Rayyan QCRI) (Ouzzani et al., 2016). In case of disagreement, a third author (MP, DP) resolved conflicts. Records that met initial inclusion criteria were retrieved as full text and carefully appraised by two authors (EP, CCa), independently. From each included study, two authors (EP, CCe) independently extracted information of interest using an electronic spreadsheet. Disagreements were resolved by consensus or with a third author (MP, CB). For continuous outcomes, we extracted the mean score, the standard deviation (SD), and the number of participants included in the analyses for each trial arm at following timepoints: post intervention, 1 to 6 months post-intervention, 7 to 24 months post-intervention. For dichotomous outcomes, we recorded the number of randomized participants and the number of events of interest for each trial arm at the same timepoints. Trial authors were contacted to provide missing data when necessary. Two authors (EP, CCe) conducted the risk of bias assessment using the revised Cochrane risk-of-bias tool (RoB 2.0) for RCT (Sterne et al., 2019). We employed the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach (Guyatt et al., 2008) to assess the overall certainty of evidence and to interpret findings for the following outcomes at post-intervention: diagnosis of any common mental disorders, depressive symptoms, anxiety symptoms, psychological distress, psychological functioning and impairment, quality of life, adverse events, parenting self-efficacy, and social support.
Data synthesis
Given the potential heterogeneity of preventive psychosocial interventions, we applied the random-effects model in all analyses, using the software Cochrane Review Manager 5.4 (Nordic Cochrane Centre, The Cochrane Collaboration Review Manager (RevMan), 2020).
For dichotomous data, we estimated the effect of the intervention by using risk ratio (RR), together with the appropriate associated 95% confidence interval (CI); for continuous data, we used standardized mean difference (SMD), together with the 95% appropriate associated confidence interval (J. Higgins et al., 2022). Data from cluster RCTs was adjusted with an intra-cluster correlation coefficient (ICC). If the ICC was not available, we assumed it to be 0.05 (J. Higgins et al., 2022). Graphical tools (forest plots) and I2 statistic were used to investigate statistical heterogeneity among studies. We interpreted I2 estimates according to Cochrane ranges: 0%–40% might not be important; 30%–60% may represent moderate heterogeneity; 50%–90% may represent substantial heterogeneity; 75%–100% considerable heterogeneity (J. P. T. Higgins & Thompson, 2002; J. Higgins et al., 2022; Purgato & Adams, 2012).
In meta-analyses including 10 studies or more, we performed the following subgroups analyses: type of perinatal period (postpartum period, pregnancy, pre- and post-partum period), setting (community, primary health care services), delivery format (individual, pairs, family, group, mixed (group + individual), type of prevention (universal, selective, indicated), provider (primary health workers, community health workers), and comparisons (active control group, no treatment, wait-list, usual care). We furthermore planned a sensitivity analysis restricting analysis to studies with low risk of bias.
In case of missing information on outcomes, we contacted investigators when possible. For cluster-RCTs, we contacted study authors for an ICC value when data were not adjusted and could not be identified from the trial report. In case of studies not reporting the proportion of participants with depression or anxiety disorders, if study authors did not provide this information, we applied commonly employed cut-off scores of continuous measures of depressive and anxiety symptoms to impute proportions of participants with a diagnosis of depression or anxiety disorders at post-intervention (Supplemental Appendix K), using an established methodology (Furukawa et al., 2005). Publication bias was examined through funnel plots as per Cochrane standards (J. Higgins et al., 2022).
Results
Characteristics of included studies
The search strategy yielded 7,182 records. After removal of duplicates (n = 2,298), a total of 4,884 titles and abstracts were assessed for eligibility, 296 of which fulfilled the eligibility criteria. After inspection of full-texts, a total of 23 studies (Abhari et al., 2021; Asnani et al., 2021; Baumgartner et al., 2021; Chaharrahifard et al., 2021; Dayhimi et al., 2020; Gao et al., 2010, 2015; George et al., 2020; Guo et al., 2021; Koçak et al., 2021; Li et al., 2019; Mao et al., 2012; Ozcan & Eryilmaz, 2021; Özçoban et al., 2022; Rajeswari & SanjeevaReddy, 2020; Ramezani et al., 2017; Rong et al., 2021; Rotheram-Borus, Richter et al., 2014; Rotheram-Borus, Tomlinson et al., 2014; Sanfilippo et al., 2020; Sapkota et al., 2022; Tripathy et al., 2010; Vargas-Porras et al., 2021) from 28 publications (Supplemental Appendix D) with 24,442 participants were included in the systematic review. Of these, 22 provided data suitable for the meta-analysis (Figure 1 and Supplemental Appendix D, E).
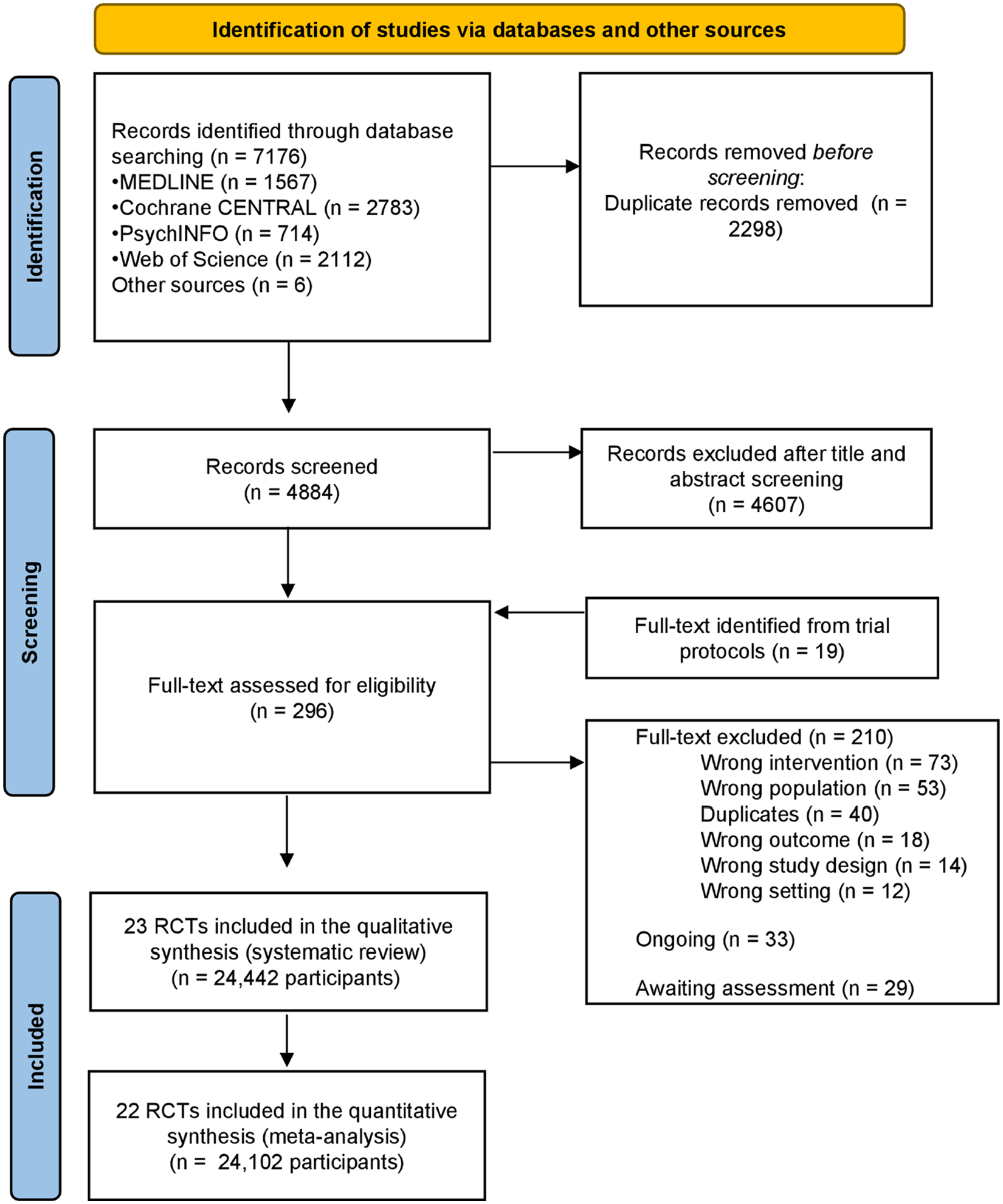
PRISMA flow-chart diagram.
Included RCTs were conducted in 10 LMICs (China, Iran, India, Turkey, South Africa, Colombia, Gambia, Ghana, Jamaica, and Nepal) (Table 1). Included trials enrolled mainly pregnant women (n = 12), six included women in their whole perinatal period (from pregnancy to post-natal period), and five enrolled women during their post-partum period (Table 1).
Characteristics of included RCTs.
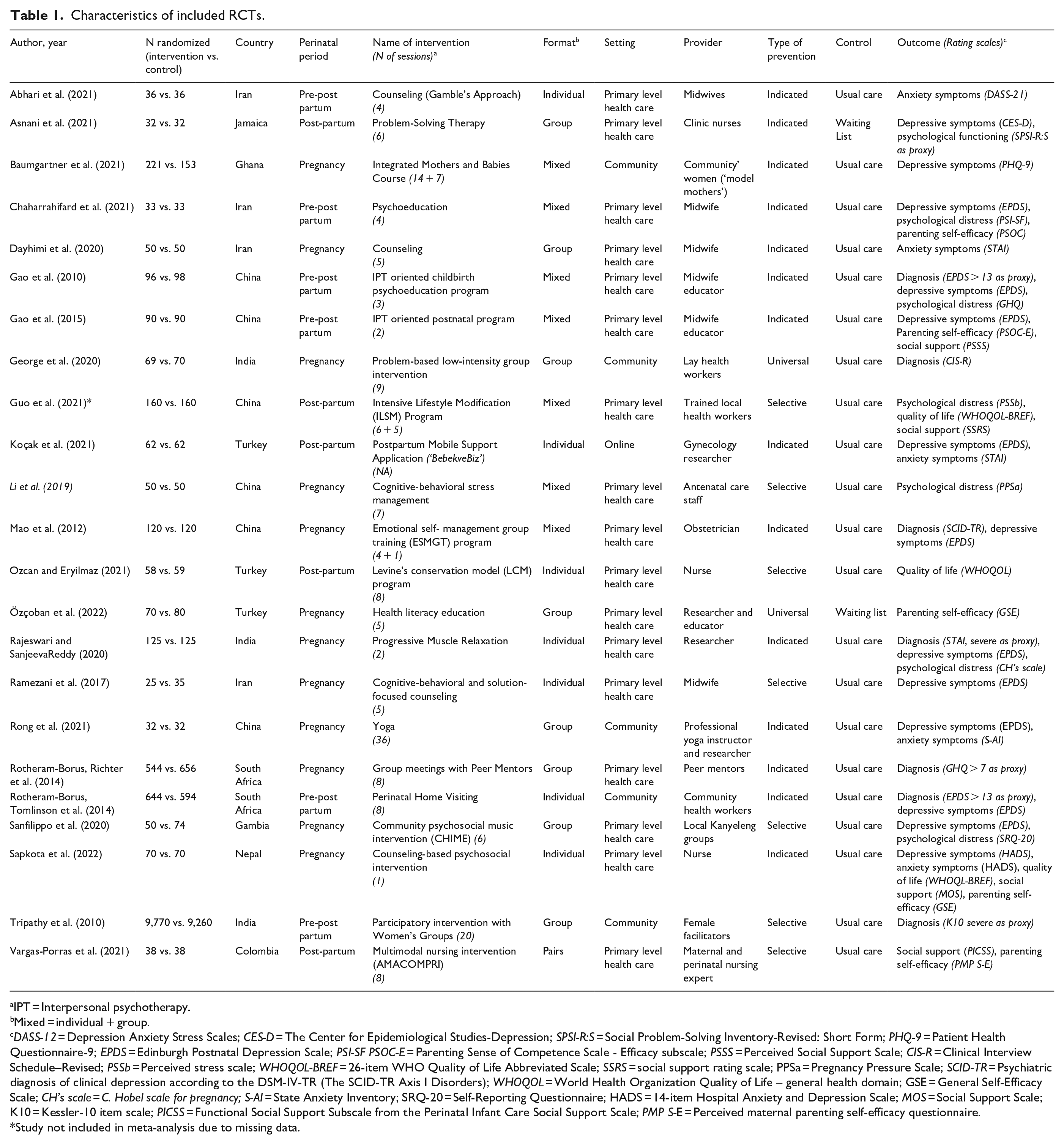
IPT = Interpersonal psychotherapy.
Mixed = individual + group.
DASS-12 = Depression Anxiety Stress Scales; CES-D = The Center for Epidemiological Studies-Depression; SPSI-R:S = Social Problem-Solving Inventory-Revised: Short Form; PHQ-9 = Patient Health Questionnaire-9; EPDS = Edinburgh Postnatal Depression Scale; PSI-SF PSOC-E = Parenting Sense of Competence Scale - Efficacy subscale; PSSS = Perceived Social Support Scale; CIS-R = Clinical Interview Schedule–Revised; PSSb = Perceived stress scale; WHOQOL-BREF = 26-item WHO Quality of Life Abbreviated Scale; SSRS = social support rating scale; PPSa = Pregnancy Pressure Scale; SCID-TR = Psychiatric diagnosis of clinical depression according to the DSM-IV-TR (The SCID-TR Axis I Disorders); WHOQOL = World Health Organization Quality of Life – general health domain; GSE = General Self-Efficacy Scale; CH’s scale = C. Hobel scale for pregnancy; S-AI = State Anxiety Inventory; SRQ-20 = Self-Reporting Questionnaire; HADS = 14-item Hospital Anxiety and Depression Scale; MOS = Social Support Scale; K10 = Kessler-10 item scale; PICSS = Functional Social Support Subscale from the Perinatal Infant Care Social Support Scale; PMP S-E = Perceived maternal parenting self-efficacy questionnaire.
Study not included in meta-analysis due to missing data.
Most psychosocial interventions (n = 17) were delivered in primary care settings, such as prenatal clinics, urban health care centers, family health centers, while in five RCTs interventions were delivered in the community, such as the participants’ homes, community centers, municipality facilities, and one intervention was delivered online (Table 1). Psychosocial interventions were provided by primary-level health care workers (e.g. midwives, nurses, obstetricians) in 16 studies (Abhari et al., 2021; Asnani et al., 2021; Chaharrahifard et al., 2021; Dayhimi et al., 2020; Gao et al., 2010, 2015; Guo et al., 2021; Koçak et al., 2021; Li et al., 2019; Mao et al., 2012; Ozcan & Eryilmaz, 2021; Özçoban et al., 2022; Rajeswari & SanjeevaReddy, 2020; Ramezani et al., 2017; Sapkota et al., 2022). Community workers (e.g. lay health workers, facilitators, women groups leaders) were responsible for the delivery of the intervention in five trials (Baumgartner et al., 2021; George et al., 2020; Rotheram-Borus, Richter et al., 2014; Rotheram-Borus, Tomlinson et al., 2014; Sanfilippo et al., 2020; Tripathy et al., 2010), and one study employed a yoga instructor (Rong et al., 2021) (Table 1). In terms of active ingredients, most interventions (n = 7) included techniques derived from cognitive behavior therapy (CBT)(Abhari et al., 2021; Baumgartner et al., 2021; Koçak et al., 2021; Li et al., 2019; Mao et al., 2012; Ramezani et al., 2017; Sanfilippo et al., 2020), followed by problem-solving techniques in four studies (Asnani et al., 2021; George et al., 2020; Sapkota et al., 2022; Tripathy et al., 2010), and interpersonal theory techniques in two trials (Gao et al., 2010, 2015). Psychoeducation was implemented in four RCTs (Chaharrahifard et al., 2021; Özçoban et al., 2022; Rotheram-Borus, Tomlinson et al., 2014; Vargas-Porras et al., 2021). Three trials employed psychoeducation alongside relaxation techniques (Dayhimi et al., 2020; Guo et al., 2021; Ozcan & Eryilmaz, 2021), and one study adopted psychoeducation alongside CBT (Rotheram-Borus, Richter et al., 2014). Relaxation techniques (including yoga and mindfulness) were adopted in five studies (Li et al., 2019; Mao et al., 2012; Özçoban et al., 2022; Rajeswari & SanjeevaReddy, 2020; Ramezani et al., 2017), while a music component was implemented in one study (Sanfilippo et al., 2020) (Table 1).
Risk of bias of included studies
Two RCTs (Ozcan & Eryilmaz, 2021; Rotheram-Borus, Richter et al., 2014) showed high risk of bias in one or two of the five domains, for example related to reporting (domain 5) or because missingness in the outcome could be potentially related to its true value (domain 3). All the others (20 RCTs) showed an overall judgment of ‘some concerns’. Major issues in the risk of bias evaluation emerged for domain 2 (risk of bias due to deviations from the intended interventions) and domain 4 (risk of bias in measurement of the outcome). Risk of bias summary and the full tables are provided in the Supplemental Appendix F.
Effects of preventive psychosocial interventions compared to control conditions
At post-intervention, preventive psychosocial interventions decreased the frequency of any diagnosed mental disorders (4 RCTs, 621 participants, RR 0.57, 95% CI [0.35, 0.91], I2 = 0%, GRADE: low certainty), and depression (12 RCTs,1,442 participants, RR 0.51, 95% CI [0.35, 0.75], I2 = 42%) but not of anxiety (4 RCTs, 376 participants, RR 0.46, 95% CI [0.06, 3.33], I2 = 99%) (Figure 2). Moreover, interventions decreased depressive symptoms (10 RCTs,1,236 participants, SMD −0.50, 95% CI [−0.80, −0.16], I2 = 88%, GRADE: moderate certainty), but had no effect on anxiety symptoms (4 RCTs, 376 participants, SMD −0.12, 95% CI [−0.95, 0.69], I2 = 93%, GRADE: low certainty) (Table 2). Meta-analysis showed significant beneficial effect of preventive psychosocial interventions for psychological distress, however, the certainty of evidence was very low (4 RCTs, 387 participants, SMD −1.32, 95% CI [−2.28, −0.35], I2 = 93%, GRADE: very low certainty). Additionally, preventive psychosocial interventions increased both social support (3 RCTs, 368 participants, SMD −0.72, 95% CI [−1.22, −0.22], I2 = 80%, GRADE: low certainty) and parenting self-efficacy (5 RCTs, 552 participants, SMD −0.76, 95% CI [−1.13, −0.38], I2 = 77%, GRADE: moderate certainty).
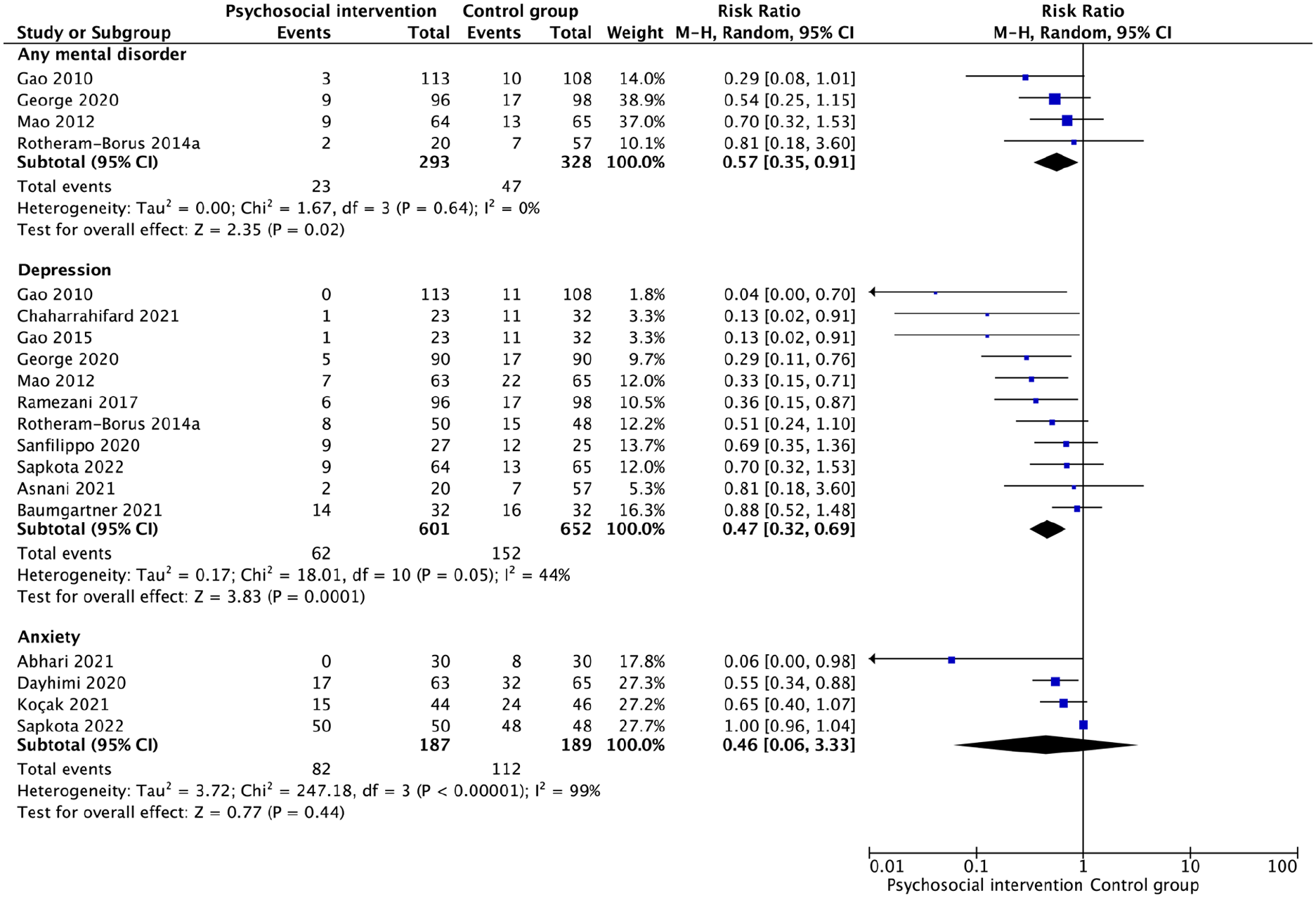
Efficacy of psychosocial interventions in preventing the development of any mental disorders, depression, and anxiety at post-intervention.
Random-effects meta-analyses of psychosocial interventions compared to control groups at different timepoints in the perinatal period in low- and middle-income countries.

Note. SMD = Standardized Mean Difference; SMD < 0 favors psychosocial interventions.
RR = Risk Ratio; RR < 1 favors psychosocial interventions.
MD = Mean Difference; MD < 0 favors psychosocial interventions.
At 1 to 6 months post-intervention, no effect was found for the outcome diagnosis of mental disorder, anxiety symptoms, and psychological distress (Table 2). A beneficial effect of interventions on depressive symptoms and parenting self-efficacy was observed (Table 2). No data on social support was available (Table 2). At 7 to 24 months of follow-up, no beneficial effects of psychosocial interventions were observed (Table 2).
For secondary outcomes, one study found that psychosocial interventions improved quality of life (1 RCT, 128 participants, SMD −2.56, 95% CI [−3.40, −1.72], GRADE: moderate certainty due to serious imprecision) but not psychological functioning at post-intervention (1 RCT, 64 participants, MD −2.00, 95% CI [−7.00, 3.00], GRADE: low certainty due to serious indirectness, imprecision). No differences were identified for dropouts, and no RCTs provided data on adverse events (Supplemental Appendix G, H, I).
Subgroup and sensitivity analyses
As at least 10 studies were available only for depressive symptoms, this outcome was used for subgroup and sensitivity analyses. Meta-analysis of studies of interventions delivered in primary health care services showed a positive effect in decreasing depressive symptoms at post-intervention (9 RCTs,1,032 participants, SMD −0.61, 95% CI [−088, −0.33]), while in community settings only one study contributed to the analysis and showed no effect (1 RCT, 204 participants, MD 0.36, 95% CI [0.08, 0.64]) (Supplemental Appendix J). Subgroup analysis considering RCTs in the whole perinatal period versus RCTs during pregnancy only and women during the post-partum period showed no difference across subgroups (p = .45). Similarly, subgroup analysis accounting for type of prevention strategies showed that selective and indicated prevention were similarly effective in preventing depressive symptoms at post-intervention (p = .04). For universal prevention no data were available. Subgroup analysis accounting for the type of control group showed beneficial effect of preventive psychosocial interventions over usual care, while no difference was observed between interventions and waiting list (p = .21). For active control group and no treatment no data was available. Regarding the type of provider, subgroup analysis accounting for primary health workers showed beneficial effect of preventive psychosocial interventions, whereas no difference was showed between intervention and control in terms of community workers (p = .58).
Regarding the delivery format, individual interventions suggested beneficial effect, while intervention in group and mixed format showed no difference (p = .81). For family and pairs format no data were available. Sensitivity analysis by trial risk of bias was not performed due to the lack of RCTs with low risk of bias as overall judgment (Supplemental Appendix F).
Discussion
This systematic review and meta-analysis suggests beneficial effects of psychosocial interventions delivered through the task-sharing modality in preventing the development of common mental disorders and in decreasing mental health symptoms. Psychosocial interventions nearly halved the frequency of mental disorders at post intervention; at follow-up, however, fewer, and more heterogeneous studies contributing to the analyses did not allow us to ascertain if the effect can be maintained in the long-term. Additionally, a beneficial effect on positive mental health, and more specifically on parenting self-efficacy and quality of life, was observed. Surprisingly, only a few studies reported on the effects of these interventions on social support. This is despite the fact that meaningful intimate partner relationships and sufficient social support networks have been identified as two of the main protective factors for CPMDs in this population group (Bedaso et al., 2021; Fisher et al., 2012).
The finding of the efficacy of task-sharing interventions are consistent with those of a recent Cochrane review by van Ginneken et al. (2021). This work included 95 RCTs from 30 LMICs reporting on the efficacy of primary-level worker interventions for the treatment of a variety of mental health conditions in LMICs. Among the included studies, only five specifically focused on women during the perinatal period (N = 1,989), and results suggested a beneficial effect of task-sharing treatment interventions in improving depressive symptoms at 1 to 6 months post-intervention (van Ginneken et al., 2021). The present review adds to this, highlighting how preventive interventions delivered through task-sharing approaches may be similarly beneficial for women living in LMICs. Another Cochrane review, which analyzed preventive interventions delivered by both professionals and paraprofessionals in LMIC humanitarian settings (Papola et al., 2020), collected data from seven trials with 2,398 adult and child participants. Even though this work was not limited to task-sharing interventions, and it was restricted to humanitarian settings, it represents one of the few reviews synthesizing evidence of preventive interventions in LMICs. Findings on the specific subpopulation of women indicated that psychosocial counseling with a preventive aim was effective in decreasing symptoms of depression at post-intervention, as well as at 3 months of follow-up (Papola et al., 2020). Altogether these reviews go in the same direction and reinforce each other in showing the benefit of preventive approaches delivered through task-sharing approaches in LMICs.
Another important finding of the present review relates to the role of the delivery setting. Psychosocial interventions were effective in decreasing depressive and anxiety symptoms when delivered in primary-level health care, as for example maternal-child health care centers, local antenatal wards, or family health care clinics as opposed to community settings, like municipality facilities or participants’ homes. This could be explained by the fact in these settings most women received psychosocial interventions in addition to perinatal routine care and health education. The combined nature of this approach may better address the entirety of maternal needs with a stronger integration of mental health in maternal-child health approaches. Such integrated programs are relevant public health strategies. For many women in LMICs antenatal care is typically the first and only time of interaction with the health-care system, and this interaction is promoted by the WHO Guide for integration of perinatal mental health in maternal and child health services (WHO, 2022a). This Guide, designed to support health workers and peers in mental health promotion and prevention, recommended the integration of psychoeducation across perinatal services. In the present review we found that psychoeducation techniques were implemented in more than a third of the included studies. These techniques included sharing information on maternal mental health, and reducing stigma, in line with the WHO recommendations (WHO, 2022a).
Notably, maternal mental health interventions can also improve child-related outcomes. As synthetised by a recent systematic review and meta-analysis by Tol et al. (2020), maternal mental health interventions along the continuum ill-health (promotion, prevention, treatment) for women living in LMICs have shown promising results for the improvement of child health, nutrition and development outcomes (e.g. exclusive breastfeeding). Our finding that parenting self-efficacy increased adds to this literature. Taken together, these elements highlight that psychosocial interventions for women in the perinatal period may play a role not only in reducing the treatment gap for CPMDs in LMICs, but also for wider public health purposes, in line with current WHO guidelines (Gelaye et al., 2016; Lancet Global Mental Health Group, 2007; WHO, 2018a).
Results from this review should be considered in light of some limitations. First, relatively few studies and participants contributed to some of the meta-analysis, especially in the analyses that explored the long-term outcomes. For the outcome prevention of any mental disorders, only four studies were included, with a sample size of less than 700 participants. Clearly, this lack of data accounts for a low confidence in the estimates, as detected by the GRADE approach. In addition, evidence on perinatal mental health in LMICs is limited. Considering a broad area as South Asia as an example, only four studies were conducted in this region, three in India and one in Nepal. The majority of studies included in this review were conducted in East Asia and Pacific Area Countries, and in the Middle East. Consistently with the recent literature (Chalise et al., 2022; Prom et al., 2022; Simkhada & van Teijlingen, 2018), our results highlight an imbalance in the geographical distribution of research outputs. The identified gap may help to orient the research agenda for the next years, in order to prioritize critical geographical areas that are still neglected. A second limitation is that no data were available on the preventive effect of psychosocial interventions on depression and anxiety disorders. Therefore, proportions of participants with depression and anxiety were imputed from continuous measures of depression and anxiety symptoms. Although an established method were used for these imputations, aiming to make the best use of available data, it should be acknowledged that this approach is based on a number of assumptions, and therefore it should only be considered an approximation of true frequencies (Altman & Royston, 2006). We note, however, that the overall preventive effect calculated with imputation techniques for depression and anxiety is similar in magnitude as compared with the preventive effect observed for the outcome prevention of any mental disorders. Third, we did not identify any trial with a low risk of bias according to the Cochrane RoB2. This result might be related to multiple factors. Some poor-resource regions where the included studies were conducted may have lower research capacity compared to HIC settings. Most of these settings do not have experienced research infrastructures. This could be related to a wide range of historical, financial, human resource and policy reasons. For example, insufficient research funding (WHO, 2022b), scarcity of material and human capacity with adequate research skills, and limited networking (Franzen et al., 2017) might be relevant factors. Clearly, the Cochrane approach requires the same standard irrespective of the country income level, and highlighting the lack of studies with a low risk of bias calls for policy actions oriented to increase the research capacity of researchers in LMICs. Overall, we found high levels of heterogeneity across studies that could indicate the complexity of conducting research with preventive purposes, which has been attributed to wide differences in modes or contents of psychosocial interventions delivery and differences in types of outcomes (Singla et al., 2021).
In terms of implications for research, this review showed that the current evidence base is mostly focused on CBT-based psychologically-oriented interventions delivered by health workers in primary care settings. The evidence base needs to be expand to encompass a wider range of prevention approaches, for example, with more studies assessing prevention interventions delivered in a range of settings, also addressing the social determinants of mental health (as opposed to targeting psychological processes) (Lund et al., 2018). This is particularly urgent given the widespread exposure to gender-based violence and poverty as risk factors for maternal mental health (Ankerstjerne et al., 2022; Wang et al., 2021). As social determinants and maternal mental health may be mutually reinforcing, it is important to understand whether intervening on structural social determinants outside of the health care system (e.g. through integrated social and mental health interventions) may provide sustainable benefits for maternal wellbeing (Greene et al., 2019, 2021). Moreover, more studies that assess medium- and long-term effects of preventive interventions are needed. In addition, studies should be designed to investigate and report results for specific subgroups of women, for example nulliparous women, to support the process of becoming a mother, or women having experienced risky conditions during gestation or delivery. With more investigations specifically thought to assess these questions, it would be possible to study whether different conditions (e.g. women with a history of intimate partner violence, mothers with HIV, pregnant women with maternal distress) and different sub-groups of women (e.g. first-time mothers, not married women, pregnant adolescents) play a role as moderators of preventative effect.
In terms of implication for policy, our results provide initial background evidence in support to the principles of the WHO Global Action Plan, the WHO Mental Health Report 2022 (WHO, 2022b), and the Sustainable Development Agenda2,030 (UN General Assembly, 2015). In these policy documents, task-sharing approaches are mentioned as a strategy to provide sustainable mental health care, and to promote a preventative culture, in line with a public health approach. Our findings, by showing that task-sharing psychosocial interventions are associated with preventive benefits with returns in terms of improvements in depressive symptoms and enhancements of quality of life and parenting self-efficacy, go in the same direction by corroborating these policy recommendations with evidence. As part of the global call to action to prioritize perinatal mental health (McNab et al., 2022), evidence-based preventive psychosocial interventions may be effectively implemented and integrated into existing mental and child health programs, aiming to improve the quality and coverage of prevention of PCMDs in women living in LMICs.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231174451 – Supplemental material for Task-sharing psychosocial interventions for the prevention of common mental disorders in the perinatal period in low- and middle-income countries: A systematic review and meta-analysis
Supplemental material, sj-docx-1-isp-10.1177_00207640231174451 for Task-sharing psychosocial interventions for the prevention of common mental disorders in the perinatal period in low- and middle-income countries: A systematic review and meta-analysis by Eleonora Prina, Caterina Ceccarelli, Jibril O Abdulmalik, Francesco Amaddeo, Camilla Cadorin, Davide Papola, Wietse A Tol, Crick Lund, Corrado Barbui and Marianna Purgato in International Journal of Social Psychiatry
Footnotes
Acknowledgements
We acknowledge all the researchers and authors whom we consulted to assess the inclusion of their studies in this review: Azam Maleki, Diksha Sapkota, and Zohreh Mahmoodi.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data of the present review will be made available upon motivated request to the authors. The protocol for this review is available online via OSF (osf.io/qt4y3).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.