
Abstract
Background:
Cannabis is associated with the onset and persistence of psychotic disorders. Evidence suggests that accessibility of substances is associated with an increased risk of use-related harms. We sought to examine the effect of residing in proximity to non-medical cannabis retailers on the prevalence of health service use for psychosis.
Methods:
We conducted a cross-sectional study using linked health administrative data, and used geospatial analyses to determine whether people in Ontario, Canada (aged 14–60 years) resided within walking (1.6 km) or driving (5.0 km) distance of non-medical cannabis retailers (open as of February-2020). We identified outpatient visits, emergency department (ED) visits, and hospitalizations for psychotic disorders between 01-April-2019 and 17-March-2020. We used zero-inflated Poisson regression models and gamma generalized linear models to estimate the association between cannabis retailer proximity and indicators of health service use.
Results:
Non-medical cannabis retailers were differentially located in areas with high levels of marginalization and pre-existing health service use for psychosis. People residing within walking or driving distance of a cannabis retailer had a higher rate of psychosis-related outpatient visits, ED visits, and hospitalizations, compared to people living outside these areas. This effect was stronger among those with no prior service use for psychosis.
Conclusions:
Proximity to a non-medical cannabis retailer was associated with higher health service use for psychosis, even after adjustment for prior health service use. These findings suggest that opening of non-medical cannabis retailers could worsen the burden of psychosis on mental health services in areas with high-risk populations.
Keywords
Background
Cannabis use is associated with the earlier onset of schizophrenia (Donoghue et al., 2014), acute episodes of psychosis (Sideli et al., 2020), and a higher risk of relapse for people with existing psychotic disorders (Schoeler et al., 2016). Prior research has established a dose-response relationship between cannabis and psychosis, whereby frequent consumption and use of high potency products are associated with a greater odds of developing schizophrenia or other psychoses (Marconi et al., 2016). Meta-analyses suggest that cannabis users have twice the odds of developing a psychotic disorder, compared to non-users, and frequent users have four-times greater odds (Marconi et al., 2016). Cannabis use is considered a preventable risk factor for psychosis, with sufficient evidence to justify harm reduction through public health interventions (Arseneault et al., 2004).
In October 2018, Canada legalized the production and sale of cannabis for non-medical purposes, leaving the regulation of cannabis sales to the provinces (Myran, Brown & Tanuseputro, 2019). Ontario used a phased approach, beginning with online purchase of cannabis flower and seeds, followed by the opening of 25 physical retail locations in April 2019 (Myran, Staykov et al., 2022).
Analyses have not found any significant immediate changes in health service use for psychosis or incident cases of psychotic disorders associated with legalization or the opening of cannabis retailers (Anderson et al., 2023; Myran, Pugliese et al., 2022). However, the retail cannabis market in Ontario was very limited during the observation periods of these studies, with limited supply, a cap on retail licenses, and restrictions on high potency products (Myran, Brown & Tanuseputro, 2019). In our prior study, there was a marked increasing trend health service use for psychotic disorders, particularly substance-induced psychosis, prior to legalization (Anderson et al., 2023).
These studies of the short-term effects of cannabis legalization did not consider whether accessibility to cannabis retail stores has affected health service use for psychosis in the surrounding communities. Studies in Washington state and California found that proximity to cannabis retailers was associated with a higher frequency of cannabis use, particularly among youth and young adults (Pedersen et al., 2021; Rhew et al., 2022). There is strong evidence to suggest that increased physical availability of alcohol correspondingly increases the rates of alcohol-related emergency department visits, traffic injuries, crash fatalities, and suicide (Myran, Chen et al., 2019; Popova et al., 2009). Exploring whether this holds true for cannabis will help quantify the impacts of legalization on the healthcare system and provide crucial information for health policy and mental health service planning.
The goal of this study was to explore how geographic proximity to non-medical cannabis retailers impacts health service use for psychosis. Specifically, we sought to compare the prevalence of outpatient visits, ED visits, hospitalizations, and hospital length of stay (LOS) for psychotic disorders among people living within walking or driving distances to non-medical cannabis retail locations, compared to those living outside those distances. Our secondary objective was to explore heterogeneity of this effect by age, sex, and prior health service use for psychosis.
Methods
Study design and data sources
We conducted a cross-sectional study using linked, population-based, health administrative data from Ontario, Canada held by ICES. ICES is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. Databases were linked at the patient level using unique, encoded identifiers, and analyzed onsite at ICES. A detailed description of databases can be found in Online Supplemental 1. This manuscript followed the REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines (Benchimol et al., 2015), Online Supplemental 2.
Study population
We identified all Ontario residents aged 14 to 60 years who were eligible for the Ontario Health Insurance Program (OHIP) on 01-April-2019 from the Registered Persons Database (RPDB). We included people below the legal age to purchase cannabis (19+ years in Ontario) based on prior research which found that proximity to cannabis retailers was associated with higher cannabis use in adolescents (Firth et al., 2022). We excluded people under 14 due to a low incidence of psychotic disorders and people over the age of 60 to avoid misclassified cases of dementia. The observation period began on 01-April-2019 when retail outlets first opened in Ontario, and ended on 17-March-2020 when Ontario declared a state of emergency due to the COVID-19 pandemic, which led to significant changes in mental health service use (Myran, Staykov et al., 2022).
People who were ineligible for OHIP or non-residents at the start of the observation period, people with invalid or missing age or sex (<1%), and rural residents were excluded. Cannabis retailers were restricted to urban areas for the initial licenses, and only opened outside of cities in December 2019. Rurality of residence was determined using the Rurality Index of Ontario. We did not impose any exclusions based on co-morbid medical or psychiatric illnesses.
Variable definitions
A detailed description of the variables in this study can be found in Online Supplemental 1.
Cannabis retailer proximity
Our exposures of interest were residing within 1.6 km or 5.0 km of a non-medical cannabis retail outlet. We obtained data on the location of non-medical cannabis retailers that were open as of 29-February-2020 from the Alcohol and Gaming Commission of Ontario (AGCO), which oversees cannabis retailer regulation (Myran, Brown & Tanuseputro, 2019). The number of non-medical cannabis retailers increased substantially from the first opening date of April-2019 to February-2020.
ArcGIS Pro (Version 2.3, Esri Canada Ltd) was used to geocode and map the 291,070 postal code centroids in Ontario. Using the Network Analyst tool, we identified postal codes within a standard walking distance (1.6 km, <15 min) and driving distance (5 km, <10 min) of a cannabis retail outlet along street networks (Gilliland et al., 2019; Healy & Gilliland, 2012; Song et al., 2013; Spielman & Yoo, 2009). We created binary variables to indicate whether each person resided within either distance of a retailer, using the best available postal code provided when accessing health services (Myran, Chen et al., 2019).
Outcomes
The outcome of interest was health service use for psychotic disorders, including outpatient visits, ED visits, hospitalizations, and LOS among those who had an inpatient admission. Psychotic disorders included schizophrenia, schizoaffective disorder, schizophreniform disorder, psychosis not otherwise specified, brief psychotic disorders, delusional disorder, bipolar disorder with psychotic features, depression with psychotic features, and substance-induced psychosis. Of note, affective psychoses were included in ED visit and hospitalization definitions, but not in outpatient visits, as we are unable to identify these in the outpatient data. We also conducted a subgroup analysis to examine service use specific to non-affective psychotic disorders using a validated algorithm (Kurdyak et al., 2015).
Outpatient and ED visits were accessed through the OHIP and NACRS databases, respectively. Data on hospitalizations and LOS were obtained from the Ontario Mental Health Reporting System (OMHRS) and the Discharge Abstract Database (DAD).
Covariates
Several confounding variables were selected based on their associations with service use for psychotic disorders (Carr et al., 2003; Durbin et al., 2015; van der Ven et al., 2020). Age and sex were obtained from the RPDB. Age was categorized into 5-year increments from 14 to 60 years. Sex assigned at birth was used as a binary variable. Migrant status (immigrant or refugee) was obtained from the Immigration, Refugees, and Citizenship Canada Permanent Resident (IRCC-PR) Database, which does not include non-migrants, second-generation migrants, and people who migrated prior to 1985. The Ontario Marginalization Index (ON-MARG) uses census-based indicators to quantify marginalization by dissemination area (a well-used proxy for neighborhood) across the following domains: dependency, material deprivation, ethnic diversity, and residential instability (Matheson et al, 2018). Each ON-MARG variable was dichotomized into ‘low marginalization’ (quintiles 1–3) versus ‘high marginalization’ (quintiles 4, 5), due to small numbers in some of the quintiles. We created a binary variable to indicate whether people had any health service use for psychotic disorders in the year prior to the observation window.
Analysis
We summarized descriptive characteristics of the cohort using frequencies, proportions, and standardized differences. Standardized differences >0.10 indicate a meaningful imbalance between groups (Austin, 2009). We calculated rates of service use for psychotic disorders per 100,000 population in the 1-year periods prior to and following 01-April-2019.
Multivariable zero-inflated Poisson (ZIP) regression models were used to estimate the effect of cannabis-retailer proximity (i.e. residing within 1.6 km or 5.0 km of a cannabis retailer) on the rate of outpatient visits, ED visits, and hospitalizations for psychotic disorders. ZIP models were selected to handle excess zeros in the observed data (Li et al., 2012). Gamma generalized linear models (GGLM) were used to estimate the effect of cannabis-retailer proximity on hospital LOS, and were selected to handle the right-skew of hospitalization data (Faddy et al., 2009). All models were adjusted for age group, sex, migrant status, dependency, deprivation, ethnic concentration, residential instability, and prior service use for psychotic disorders. There were minimal missing data in ONMARG variables, only (⩽1%), and people with missing data were classified as ‘low marginalization’.
Our descriptive analyses suggested that cannabis retailers were differentially located in areas with high baseline service use for psychotic disorders; therefore, we conducted a post-hoc analysis to test for interaction between proximity to cannabis retailers and prior service use for psychotic disorders by adding an interaction term to fully adjusted models. We found a significant interaction effect for outpatient visits only, so we stratified these models by prior health service use for psychotic disorders in the year prior to the index date. We also performed stratified analyses by sex and age group to identify sex differences in the impact of cannabis availability on psychosis-related service utilization, as well as the impacts on people above and below the legal age to purchase cannabis in Ontario (19+ years). Logistic regression models were used for the stratified analyses, due to outcome sparsity in the subgroups which violated count model assumptions. The odds ratios from the stratified analyses were assumed to approximate the risk ratio because the outcome was rare in our cohort (Davies et al., 1998).
All analyses were performed at ICES using SAS Version 9.4 (SAS Institute, Cary North Carolina), and results are presented as incidence rate ratios (IRR) and risk ratios (RR) with corresponding 95% confidence intervals (CI). Our description of the findings focuses on the fully adjusted models, as these largely aligned with the unadjusted models.
Results
Sample
The study sample characteristics can be found in Table 1. We identified 8,584,530 people who met the inclusion criteria on 01-April-2019. The sample was 50.1% female with a mean age of 37.9 years (SD = 13.9). There were 43 cannabis retailers in operation in Ontario on 29-February-2020, and 7.9% of the sample resided within 1.6 km of a retail outlet and 32.1% within 5.0 km. A larger proportion of people residing within 1.6 km of a cannabis retailer were aged 14 to 19 years, 25 to 29 years, and 30 to 34 years. Cannabis retailers were also more likely to open in areas with high levels of marginalization (Table 1).
Sample characteristics.

Note. SD = standard deviation; IQR = interquartile range; Std diff = standardized difference.
Indicates standardized differences >0.10, considered to be a meaningful imbalance between groups.
Health service use for psychotic disorders
Table 2 contains the rates of health service use for psychotic disorders per 100,000 in the 1-year period prior to and following cannabis retailer opening. There were higher rates of all types of health service use for psychotic disorders among people residing within 1.6 and 5.0 km of cannabis retail outlets in both pre- and post-retailer periods, compared to people who resided outside of these distances.
Health service use for psychotic disorders by proximity to cannabis retailers, in the 1-year period prior to cannabis retailer opening and 1-year period after cannabis retailer opening.
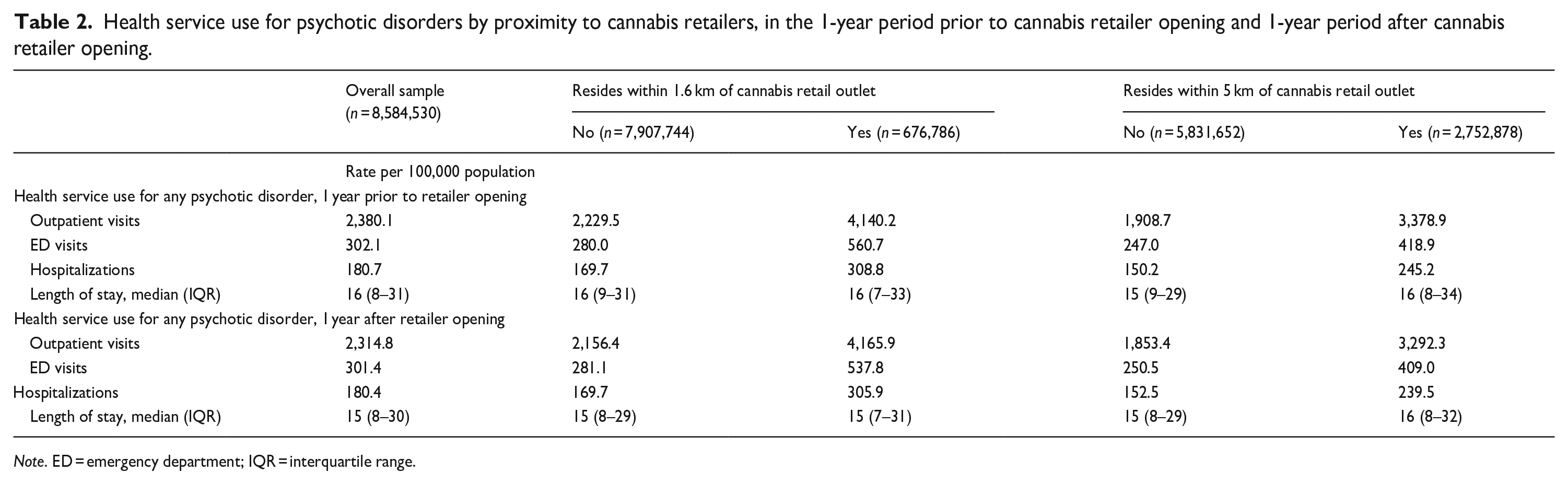
Note. ED = emergency department; IQR = interquartile range.
The results for the association between proximity to retailers and service use for psychotic disorders can be found in Table 3. People who resided <1.6 km of a cannabis retail outlet were more likely to have an outpatient visit (IRR = 1.23, 95% CI [1.19, 1.28]) and ED visit (IRR = 1.10, 95% CI [1.03, 1.16]) for psychotic disorder, but were not more likely to have a psychosis-related hospitalization (IRR = 1.05, 95% CI [0.96, 1.15]), relative to people residing >1.6 km from a retailer. Among those who had each type of visit, residing <1.6 km of a cannabis retail outlet was associated with a greater number of outpatient visits (IRR = 1.16, 95% CI [1.14, 1.17]), ED visits (IRR = 1.27, 95% CI [1.21, 1.33]), and hospitalizations (IRR = 1.30, 95% CI [1.19, 1.41]) for psychotic disorders, relative to those residing >1.6 km from a retailer.
Association between residing within proximity of a cannabis retail outlet and health service use for psychotic disorders.
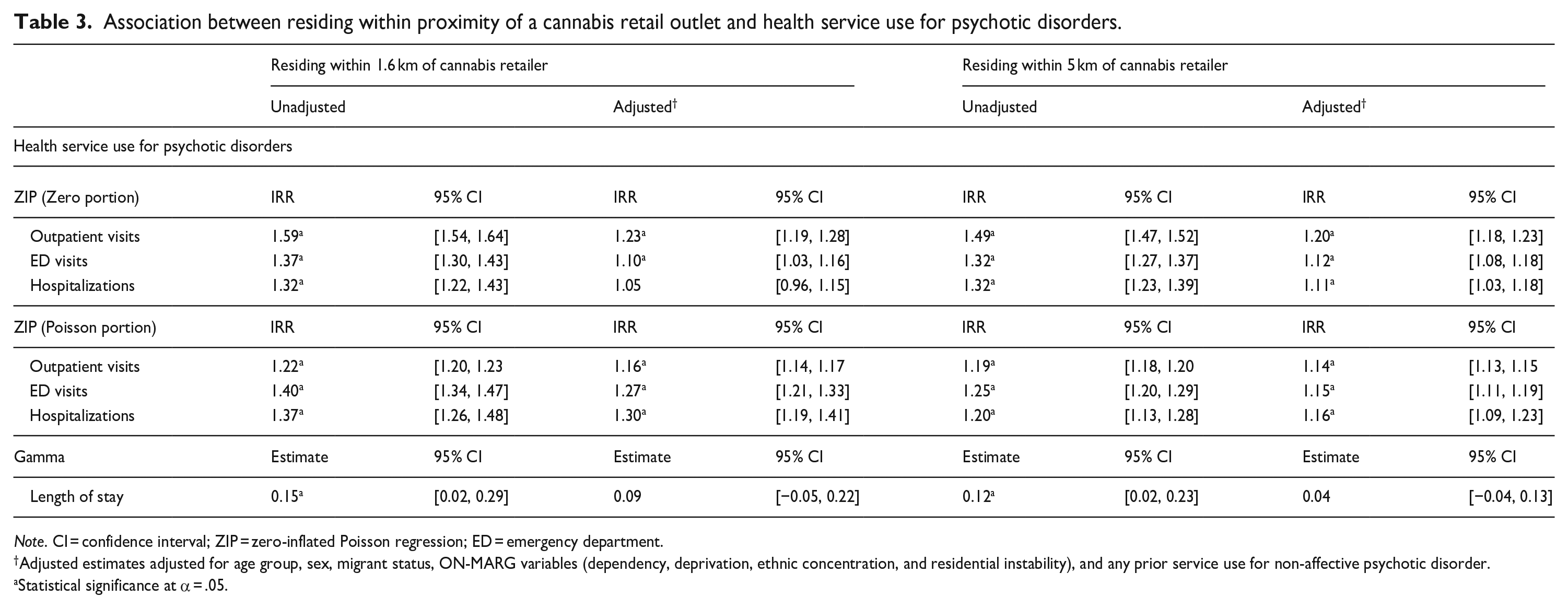
Note. CI = confidence interval; ZIP = zero-inflated Poisson regression; ED = emergency department.
Adjusted estimates adjusted for age group, sex, migrant status, ON-MARG variables (dependency, deprivation, ethnic concentration, and residential instability), and any prior service use for non-affective psychotic disorder.
Statistical significance at α = .05.
Similarly, people who resided <5.0 km of a cannabis retail outlet were more likely to have an outpatient visit (IRR = 1.20, 95% CI [1.18, 1.23]), ED visit (IRR = 1.12, 95% CI [1.08, 1.18]), or hospitalization (IRR = 1.11, 95% CI [1.03, 1.18]) for psychotic disorder, relative to people resided >5.0 km from a retailer. Among those who had each type of visit, residing <5.0 km of a cannabis retailer was associated with a greater number of outpatient visits (IRR = 1.14, 95% CI [1.13, 1.15]), ED visits (IRR = 1.15, 95% CI [1.11, 1.19]), and hospitalizations (IRR = 1.16, 95% CI [1.09, 1.23]) for psychotic disorders, compared to those who resided >5.0 km from a retailer. Proximity to a cannabis retailer was not associated with differences in length of hospital stay for psychosis-related hospitalizations.
The results of the subgroup analyses specific to non-affective psychotic disorders were consistent with our main analyses (Online Supplemental 3).
Stratified analyses
The results for the analysis of the association between cannabis retailer proximity and outpatient visits for psychosis, stratified by prior health service use for psychosis, are displayed in Table 4. The effects of proximity to retailers on the rate of outpatient visits were significantly greater among those with no prior health service use for psychotic disorders, compared to those with prior health service use. Among those with prior health service use for psychosis, residing <1.6 km of a retailer was associated with a 16% higher risk of outpatient visits for psychosis, compared to those residing >1.6 km (IRR = 1.16, 95% CI [1.10, 1.23]). Among those without prior service use, residing <1.6 km of a retailer was associated with a 33% higher rate of outpatient visits for psychosis, compared to those residing >1.6 km (IRR = 1.33, 95% CI [1.27, 1.40]).
Effect modification of the association between proximity to cannabis retailers and outpatient visits for psychotic disorders, by prior health service use for psychotic disorders.
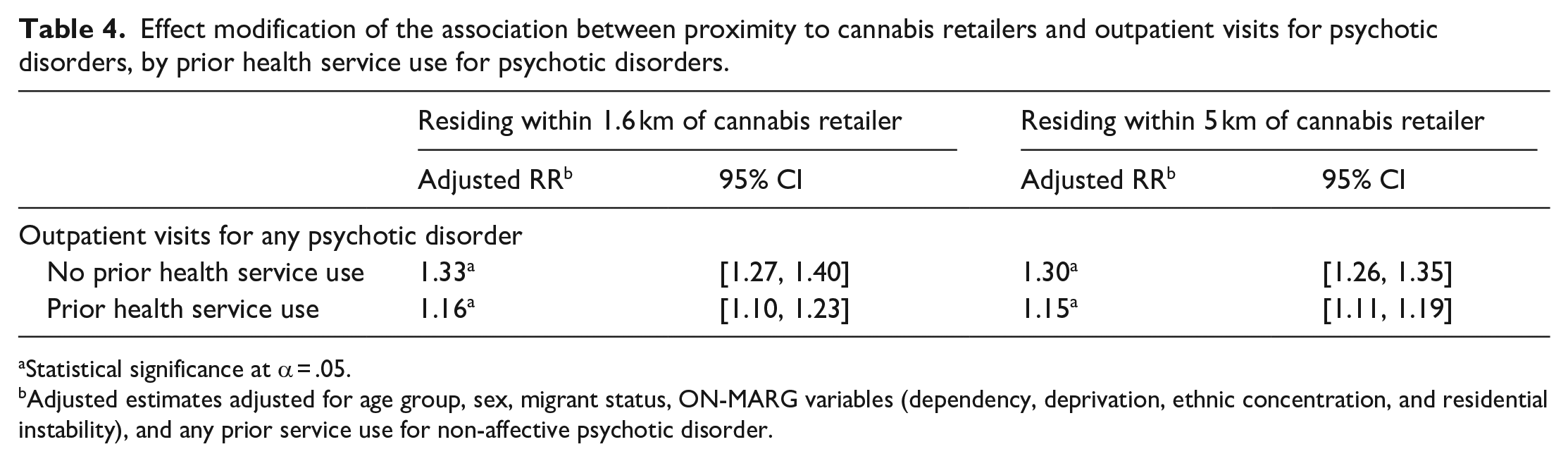
Statistical significance at α = .05.
Adjusted estimates adjusted for age group, sex, migrant status, ON-MARG variables (dependency, deprivation, ethnic concentration, and residential instability), and any prior service use for non-affective psychotic disorder.
The results of the stratified analyses by age and sex can be found in Online Supplemental 4. There were no differences in the effects of proximity to cannabis retailers on the rate of ED visits, hospitalizations, and outpatient visits among those under the age of 19, versus those over 19. For the sex-stratified analyses, the magnitude of effect for residing <1.6 km of a cannabis retailer on the number of outpatient visits for psychotic disorders was greater among females (IRR = 1.25, 95% CI [1.22, 1.27]) than males (IRR = 1.12, 95% CI [1.10, 1.14]). This heterogeneity of effect was not observed for the effect of residing <5 km of retailers, for other types of service use, or for the likelihood of any health service use for psychotic disorders.
Discussion
Living in proximity to cannabis retail outlets was associated with higher rates of outpatient visits, ED visits, and hospitalizations for psychotic disorders. There was no significant association between proximity to cannabis retailers and length of hospital stay. To our knowledge, this is the first study to examine the association between proximity to a cannabis retailer and psychosis-related health service use. Our findings are consistent with studies examining alcohol and tobacco retailers, which found that accessibility of substances is associated with use-related harms (Myran, Chen et al., 2019). Our findings are strengthened by the use of population-based health administrative data and the examination of multiple levels of exposure across several types of service use.
Prior analyses of the short-term impacts of cannabis legalization in Canada during the early period of market restriction found no evidence of an increase in health service use for psychosis or incident cases of psychotic disorders(Anderson et al., 2023; Myran, Pugliese et al., 2022). The current study examined the effects of local cannabis availability in terms of physical proximity to retailers. In terms of quantifying the impacts of legalization, measuring proximity to retailers may be advantageous for periods when retail locations were sparse, and the online retailers faced distribution issues (Cheung, 2018). Furthermore, the removal of restrictions on retail licenses and increased availability of high potency products in 2020 coincides with the COVID-19 pandemic – which carried implications for the healthcare system, the economy, substance use, and society at large. Therefore, these effects may be difficult to parse from one another. We hypothesize that the effect of proximity to cannabis retailers would be more pronounced in the period following March of 2020, with greater accessibility of cannabis and high potency products. Taken together, these findings suggest that while exposure to the heavily-regulated legal cannabis market did not result in short term changes in health service use for psychosis, the increasing availability of cannabis may lead to long-term changes, and strain the mental health system where retailers are located.
The effect of proximity to cannabis retailers on the number of outpatient visits for psychosis was stronger among females than males. A recent study using data from a survey in Ontario found that there was no interaction between cannabis legalization and sex on cannabis use or daily cannabis use. However, we speculate that females may be more likely to obtain cannabis from the legal market (Imtiaz et al., 2023). Therefore, greater availability of legal cannabis may differentially affect cannabis use patterns among females, and translate into differences in effects on health service use for psychosis. A prior study found larger increases in cannabis-related ED visits among women than men in Ontario (Kim et al., 2022). Furthermore, females are more likely to access outpatient services for mental health than males (Hansen & Høye, 2015), which may explain why we only found effect modification for this type of service use. Future research should focus on the interactions of sex and gender with cannabis use on the risk of psychosis.
Interestingly, the effect of proximity to cannabis retailers on outpatient visits for psychosis was greater among those without psychosis-related service contact in the past year. This is counterintuitive assuming that those with prior service use for psychosis are already connected with outpatient services. It is possible that people without a prior history of psychotic disorder are more likely to be first-time users of cannabis, who might be more likely to obtain cannabis from the legal market.
Cannabis retail outlets were also differentially located in more marginalized areas with a greater prevalence of prior health service use for psychosis. This finding is consistent with that of Myran and colleagues (Myran, Brown & Tanuseputro, 2019; Myran, Staykov et al., 2022), who found that cannabis retailers across Canada were more likely to open in neighborhoods in the lowest income quintile. Similar patterns were observed in California and Washington State (Pedersen et al., 2021; Rhew et al., 2022; Unger et al., 2020). Unger and colleagues found that neighborhoods with cannabis retailers had higher proportions of Black and Hispanic residents, lower proportions of non-Hispanic whites, and higher proportions of people living below the poverty line (Unger et al., 2020). Retailers may be located in areas of high urban density to conform with zoning for commercial land use and increase foot traffic (Yoshimura et al., 2021). However, retailers are likely targeting areas with higher expected rates of cannabis use, such as those with higher urban density, lower socioeconomic status, and greater marginalization (Rhew et al., 2022), each of which are also associated with risk of psychotic illness (Heinz et al., 2013; Kwok, 2014; Rotenberg et al., 2023). Urbanicity is associated with an increased risk of non-affective psychosis through social drift of people with psychosis to urban areas, as well as being associated with the development of psychosis (Heinz et al., 2013). Furthermore, areas with the highest levels of residential instability, material deprivation, and ethnic diversity have higher rates of psychotic disorders (Rotenberg et al., 2022). The availability of cannabis retailers in these areas could exacerbate the demand on mental health services. Future research is required to examine the long-term effects of cannabis accessibility, availability of high potency products, and cannabis sales on the rates of mental health service use for psychosis. Determining these long-term effects are crucial for targeting and funding of mental health services and informing future rollout of cannabis policies.
Limitations
The present analysis is unable to establish causality, as we are unable to determine whether stores caused an increase in rates of service use in these areas, or whether retail locations opened in areas with high cannabis demand and higher pre-existing rates of service use for psychosis. We have attempted to account for this by adjusting for prior service use for psychotic disorders, but residual confounding may remain. The distance to cannabis retailers was calculated from the postal code centroid, rather than the residential address, which may have led to misclassification for postal codes with a large geographic area. We also do not have individual-level data on cannabis purchasing and consumption patterns. Therefore, we are unable to determine whether the people buying and using cannabis from these retailers were the ones using health services for psychosis. Instead, we are limited to inferences regarding residential proximity to cannabis retailers, which are valid for informing public health policy. We used a dichotomous measure of rurality, which may fail to capture the full granularity of urban density. Our accessibility measure for cannabis retailers was based on outlets that were open on 29-February-2020, whereas the number of retailers was increasing over the observation period, from 16 in April-2019 to 43 in February-2020, and we do not have information on exact opening dates. Therefore, there is likely some misclassification in our accessibility measure with the opening and closing of cannabis retailers. We lack data on the illicit sales of cannabis, and we do not have access to information on unlicensed retail locations and other illegal sources which supplied the majority of cannabis users in Ontario during the observation period (Ontario Cannabis Store, 2020). The proportion of cannabis users who report obtaining cannabis from the legal market has been increasing over time (Government of Canada, 2022), meaning that we may see stronger effects if we were to repeat the analysis based on the current market. Online retail of cannabis was also available in Ontario during our study period via the Ontario Cannabis Store, and people farther from cannabis retailers may have accessed cannabis online. We did not include information on proximity to mental health services, which included physician offices, walk-in clinics, and hospitals. It is likely that cannabis retailers and health care providers are differentially located in areas of high population density, which could result in higher use of mental health services for psychosis. We have excluded rural areas in an effort to control this, but residual confounding may remain. Furthermore, we do not have information on the location of tobacco or alcohol retailers, which may have confounded the associations observed if they are located in proximity to cannabis retailers. Finally, our definition of health service use for psychotic disorders included substance-induced psychosis, which may be attributable to other substances, such as methamphetamine or alcohol.
Conclusions
We found evidence that cannabis retailers were differentially located in areas with high pre-existing service use for psychotic disorders, and proximity to cannabis retail outlets was associated with higher rates of health service use for psychotic disorders, even after adjusting for pre-existing service use. This effect was stronger for the use of outpatient services among those without prior service use for psychosis. Taken together, this suggests a need for careful consideration when issuing retail licenses in vulnerable areas, and a cap on the total number of licenses granted. It is important to mitigate the harms associated with cannabis legalization, despite potentially slowing the dissolution of the illicit market, which was a stated goal of legalization in Canada (Government of Canada, 2020). These findings can inform future policy directives regarding cannabis and the issuance of retail licenses, and the planning of mental health services in areas with cannabis retailers.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231206053 – Supplemental material for The effect of non-medical cannabis retailer proximity on use of mental health services for psychotic disorders in Ontario, Canada
Supplemental material, sj-docx-1-isp-10.1177_00207640231206053 for The effect of non-medical cannabis retailer proximity on use of mental health services for psychotic disorders in Ontario, Canada by Jared C Wootten, Rebecca Rodrigues, Jason Gilliland, Brooke Carter, Salimah Z Shariff, Shiran Zhong, Suzanne Archie, Jordan Edwards, Tara Elton-Marshall, Daniel Thomas Myran, Lena Palaniyappan, Christopher M Perlman, Jamie A Seabrook, Robin M Murray and Kelly K Anderson in International Journal of Social Psychiatry
Footnotes
Acknowledgements
We gratefully acknowledge the contributions of Jennifer Reid and Britney Le at ICES Western, who provided methodological and statistical oversight to this project. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and information compiled and provided by: Ontario Ministry of Health, and the Canadian Institute of Health Information (CIHI). The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. Parts or whole of this material are based on data and/or information compiled and provided by Immigration, Refugees and Citizenship Canada (IRCC) current to March 17, 2020. However, the analyses, conclusions, opinions and statements expressed in the material are those of the author(s), and not necessarily those of IRCC. We thank the Toronto Community Health Profiles Partnership for providing access to the Ontario Marginalization Index.
Disclosures
Lena Palaniyappan reports personal fees for serving as chief editor from the Canadian Medical Association Journals, speaker/consultant fees from Janssen Canada and Otsuka Canada (2019), SPMM Course Limited, UK, Canadian Psychiatric Association; book royalties from Oxford University Press; investigator-initiated educational grants from Janssen Canada, Sunovion and Otsuka Canada outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study also received funding from the Canadian Institutes of Health Research (CIHR) and the Mental Health Commission of Canada (MHCC). Kelly Anderson is supported by a Tier 2 Canada Research Chair in Public Mental Health Research. Lena Palaniyappan is supported by the Monique H. Bourgeois Chair in Developmental Disorders and Graham Boeckh Foundation (Douglas Research Centre, McGill University) and a salary award from the Fonds de recherche du Quebec-Sante ́ (FRQS).
Data availability statement
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g. healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at https://www.ices.on.ca/DAS (email: ![]() ).
).
Supplemental material
Supplemental material for this article is available online.
References
{kind=link}
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.