
Abstract
Background:
Suicidal attempt is a significant risk factor for future attempts, with the highest risk during the first-year post-suicide. Telepsychiatry has shown promise by providing easy access to evidence-based interventions during mental health crises.
Aims:
investigation the effectiveness of telehealth interventions in suicide prevention
Methods:
Four electronic databases (PubMed, Scopus, Web of Science, and Ovid) were systematically searched for studies on patients undergoing telepsychiatry intervention (TPI) up to June 2022. Following PRISMA guidelines, a systematic review and meta-analysis were conducted to investigate the effectiveness of telehealth interventions in suicide prevention. Continuous data were pooled as standardised mean difference (SMD), and dichotomous data were pooled as risk ratio using the random effects model with the corresponding 95% confidence intervals (CI).
Results:
Sixteen studies were included in the review. Most studies were case-control and randomised controlled trials conducted in Europe and North America. The findings of the studies generally showed that TPIs are effective in reducing suicide rates (odds ratio = 0.68; 95% CI [−0.47, 0.98], p = .04) and suicidal reattempts. The interventions were also found to be well-accepted, with high retention rates.
Conclusion:
Our results suggest that TPIs are well-accepted and effective in reducing suicide rates and reattempts. It is recommended to maintain telephone follow-ups for at least 12 months. Further research is needed to understand the potential of telepsychiatry in suicide prevention fully.
Introduction
Suicide is a major global health issue, with an annual mortality rate of 703,000. It is the fourth leading cause of death in people aged 15 to 29 years (World Health Organization, 2023). Nearly half of suicides are committed by people under 45, according to World Health Organization (WHO) (World Health Organization, n.d). Suicidal behaviour includes (World Health Organization, 2023) suicidal attempts, defined as self-injuries and/or self-poisoning behaviours with clear suicidal intent associated with suicidal ideation, persistent self-harm, and completed suicides (Stefanopoulou et al., 2020 This behaviour strongly predisposes individuals to further suicidal attempts (12%–30%), especially during the first year after the index attempt (Monnier et al., 2003). Other risk factors include worsening depressive symptoms, psychosis, substance abuse and the impact of life events (Pfender, 2020).
The increased risk of suicidal behaviours and the high rate of psychiatric morbidity in suicidal attempters emphasise the need for continuing follow-up. Conventional follow-up treatments are currently delivered through face-to-face psychosocial interventions such as Dialectical Behavioral Therapy (DBT), Cognitive Behavioral Therapy (CBT) and Problem-Solving Therapy (PST) (Klonsky et al., 2016). People with suicidal ideation or self-harm face many barriers to seeking immediate assistance, including limited geographical access, fear of hospitalisation, ignorance of suicidality, treatment costs, social stigma, and past negative experiences with healthcare, all of which may reduce the effectiveness of these interventions. To prevent the aggregation of suicidal thoughts into complete suicide, a person needs immediate help during mental health crises (Cedereke et al., 2002; Stanley et al., 2020).
Recent digital technologies have advanced digital interventions. Telepsychiatry interventions (TPIs) which include telephone, Internet, or video meetings, are easy-access and cost-effective methods (de Beurs et al., 2015; Monnier et al., 2003) that have shown promising outcomes in patients with psychological disorders such as depression, schizophrenia, and anxiety (Palylyk-Colwell & Argáez, 2018). Therefore, TPIs not only provide immediate access to evidence-based treatment during a crisis (Kruse et al., 2017; Lin & Yue, 2022), but they also can help manage other psychiatric disorders that most suicidal attempters also have (Nock et al., 2008). TPI can increase help-seeking by providing anonymity and confidentiality (Kruse et al., 2017; Obisike, 2018), lower cost (Butler & Yellowlees, 2012; Elford et al., 2001; Fortney et al., 2011; Hubley et al., 2016; Modai et al., 2006), and acceptable efficacy to reduce suicidal risk (Cedereke et al., 2002; Hubley et al., 2016). On the other hand, the growing use of technologies since the COVID-19 pandemic showed a promising future use of telehealth, especially for reaching rural communities with limited access to mental health care (Lin & Yue, 2022; Pfender, 2020). (Hubley et al., 2016; Modai et al., 2006; Stefanopoulou et al., 2020; World Health Organization, n.d)This systematic review and meta-analysis aimed to evaluate the effectiveness of TPIs in decreasing the incidence of suicidal attempts.
Methods
When reporting this systematic review and meta-analysis, we followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline (Page et al., 2021). All steps were conducted according to the Cochrane Handbook of Systematic Reviews and Meta-analysis of Interventions (Higgins et al., 2021). The protocol for this systematic review and meta-analysis study was registered on PROSPERO.
Search strategy
We systematically searched four electronic databases (Ovid, PubMed, Scopus, and Web of Science) for peer-reviewed English articles published until June 2022 from the beginning reports using different combinations of the following MeSH terms: ‘suicide prevention’, and ‘telemedicine’, ‘telepsychiatry’, or ‘telehealth’. Further, the references of the included studies were manually searched for any potentially eligible studies. The detailed search strategy and results for each database are reported in Supplemental 1.
Eligibility criteria
Studies were included in our review if they satisfied the following criteria (PICO), population: a patient at risk of suicide (i.e. recent suicidal ideation or attempt) and a therapist engaged in a real-time dialogue (i.e. without using avatars or internet-based self-help sites) through an entirely remote (not in-person) intervention; intervention: suicide-specific clinical interventions through telehealth; comparison: none, or standard conventional treatments; outcomes: suicide-specific outcomes, including depression scores, suicidality scores, and the number of suicidal attempts afterwards.
Selection process
Using Endnote (Clarivate Analytics, PA, USA), duplicates were removed. The obtained references were imported into Rayyan Software (Ouzzani et al., 2016) and screened in two steps: first, the titles and abstracts of all identified articles were reviewed independently by two authors to determine their relevance; second, the full-text versions of the identified records were reviewed by two authors to determine final eligibility to enter the meta-analysis. All authors involved in this process are consultant psychiatrists and mental health researchers.
Data extraction
Two authors extracted the data, including sample characteristics, methodology, suicide-related assessments, and outcomes, into tables revised by an additional reviewer (MC) after the extracted data were double-checked.
Risk of bias assessment
We systematically assessed the risk of bias for the included studies using the Newcastle-Ottawa Scale (Lo et al., 2014), which estimates the risk of bias in observational studies based on reporting three essential domains: selection of the study subjects, comparability of groups regarding demographic characteristics and important potential confounders and ascertaining the prespecified outcome. Two independent reviewers assessed the risk of bias. In disagreement, a third reviewer evaluated the data and made the final decision.
Synthesis method
We performed the meta-analysis using the Review Manager (RevMan) software version 5.3, using odds ratio (OR) for categorical variables and mean difference (MD) for continuous variables, with 95% confidence intervals. We calculated the pooled effect size for all outcomes according to the DerSimonian Liard (DerSimonian & Laird, 1986)random effects model (DerSimonian & Laird, 1986), which accommodates a larger standard error in the pooled estimate, making it suitable for inconsistent or controversial estimates.
Heterogeneity among studies was assessed using the Cochrane Q test; the I-squared (I2) and χ² p-value were used as indicators of heterogeneity, where χ² p < .1 indicates significant heterogeneity and I2 ⩾50% indicates high heterogeneity.
Publication bias assessment
In the present study, assessment of publication bias was not possible using Egger’s test, as according to Egger and colleagues (Egger et al., 1997; Terrin et al., 2003), publication bias assessment is unreliable when the number of studies is limited.
Certainty assessment
To test the robustness of the evidence, we conducted a certainty assessment through sensitivity analysis in multiple scenarios for every outcome in the meta-analysis, excluding one study in each scenario to ensure the overall effect size was not dependent on any single study.
Results
As outlined in the PRISMA flow diagram (Figure 1), 4,991 studies were initially identified through database searches and additional sources. After removing duplicates,4,886 studies were screened for eligibility, of which 16 were included in the systematic review. Most studies had a moderate risk of bias (Supplemental Table 2).
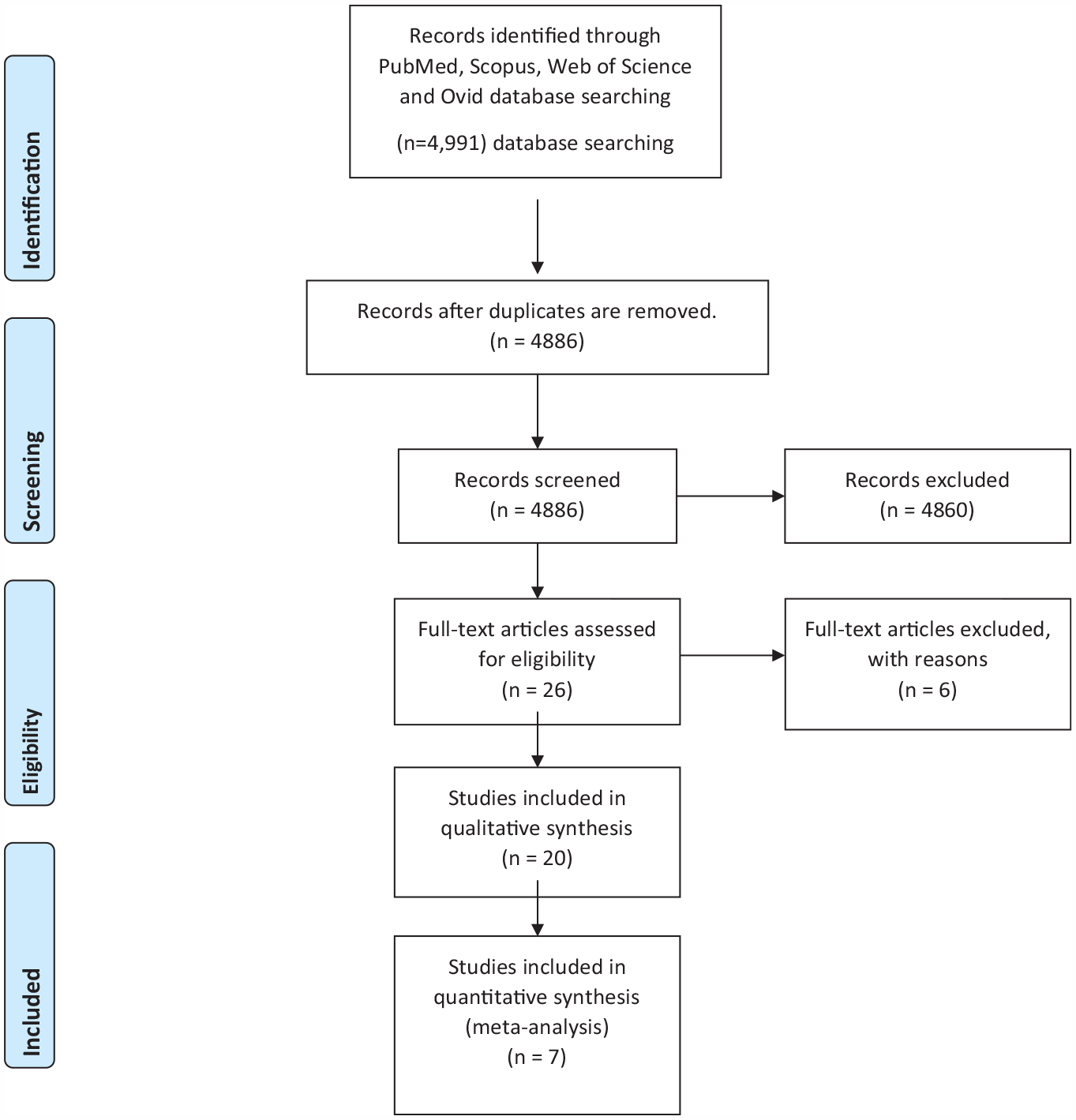
PRISMA flow diagram.
Findings of the systematic review
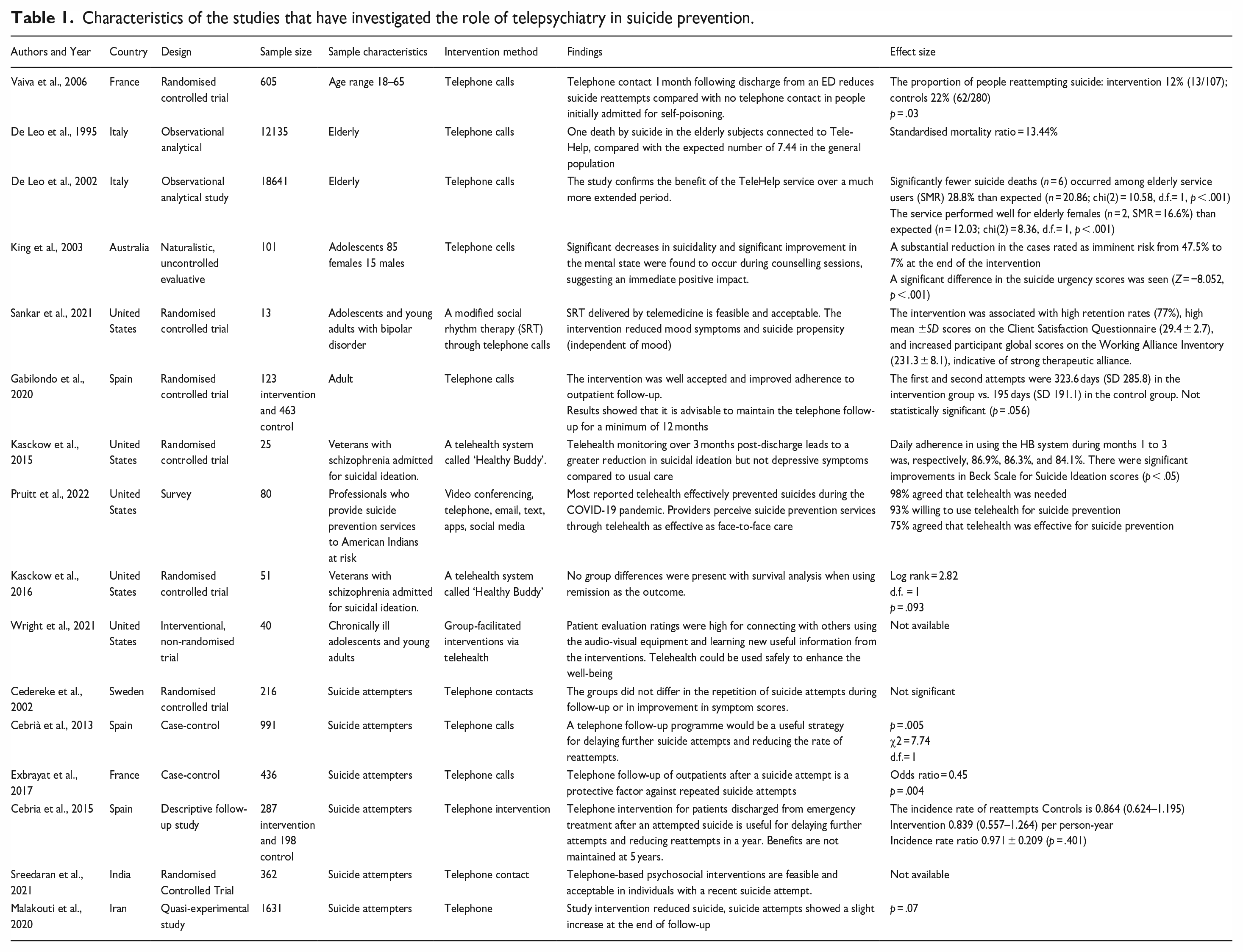
Table 1 summarises the 16 studies investigating the role of TPI in suicide prevention. Most studies were case-control studies or clinical trials from Europe and North America, with the samples varying from 13 to 18,641 patients. The TPIs were mainly delivered via telephone calls and proved effective in reducing suicide rates, suicide reattempts, and suicidal ideation while being well-accepted and having high retention rates (Table 1). The studies also recommended maintaining the telephone follow-up for a minimum of 12 months.
Characteristics of the studies that have investigated the role of telepsychiatry in suicide prevention.
Baseline characteristics of the studies in the meta-analysis
Seven of the 16 studies in the review entered the meta-analysis, with interventions varying from 3 months to 1 year. The studies were conducted between the years 2001 and 2022.
Comparison of the depression score outcome
The analysis showed no statistically significant difference in the depression score between the telehealth and standard treatment groups (MD = 1.15, 95% CI [[−7.14, 4.52], p = .66). Significant heterogeneity was among the studies (p < .05, I2 = 76%; Figure 2).

Forest plot for the comparison of depression scores.
Comparison of the suicide score outcome
The initial analysis showed no statistically significant difference in the suicide score between the two groups (MD = −0.58, 95% CI [−5.35, 4.19], p = .81). We observed a significant heterogeneity among studies (p < .05, I2 = 81%; Figure 3). We performed sensitivity analysis by removing the study by Cedereke et al. (2002), which significantly reduced the heterogeneity (p = .19, I2 = 43%), while the difference remained non-significant (MD = 1–2.78, 95% CI [−7.05, 1.48], p-value = .20; Figure 3).
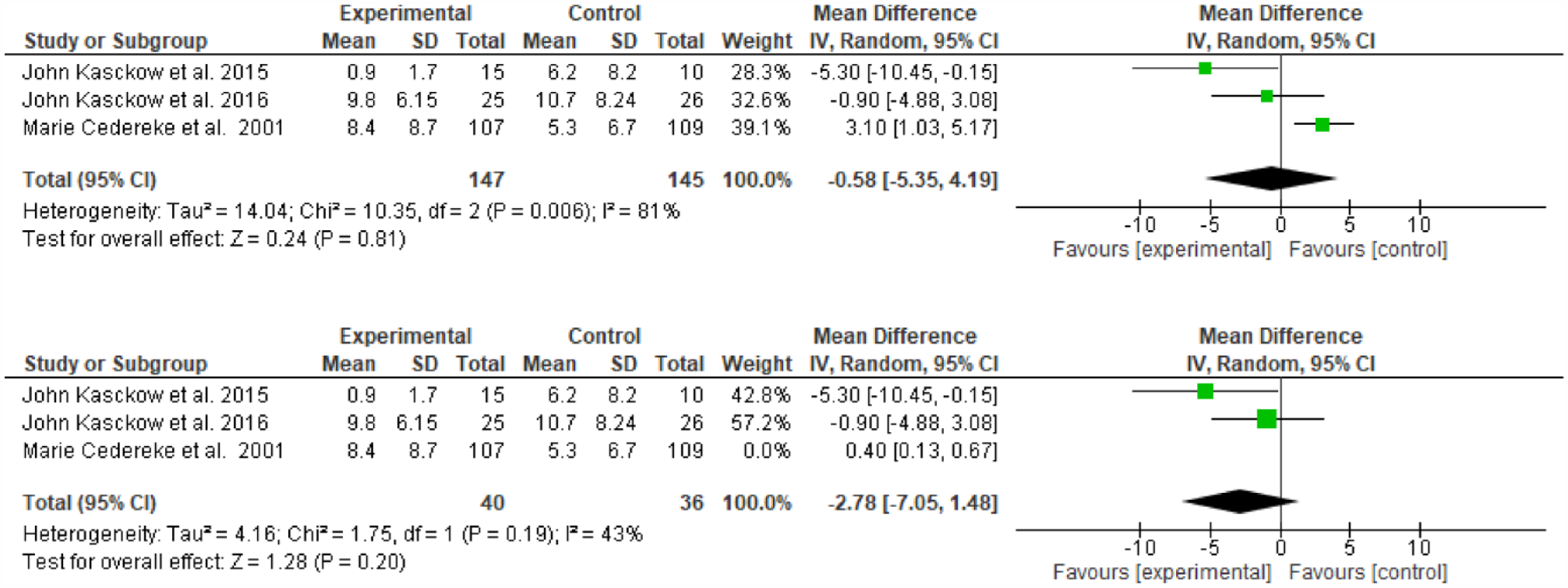
Forest plot for comparison of suicide scores.
Comparison of the frequency of suicides
The analysis showed a significant difference in the number of suicides between the two groups (OR = 0.68, 95% CI [[−0.47, 0.98], p = .04), indicating that TPIs significantly decreased the incidence of suicide in depressed patients. The observed heterogeneity among the studies was insignificant (p > .05, I2 = 48%; Figure 4).
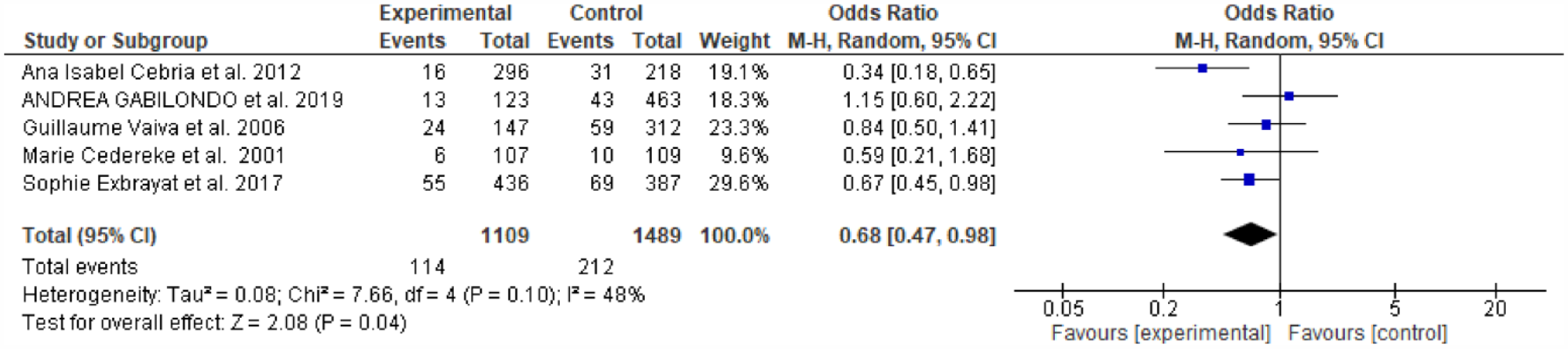
Forest plot for the comparison of suicide frequency.
Discussion
Suicide prevention is an ongoing public health concern, and there is a need for easy access and effective interventions to reduce suicide rates. Telepsychiatry, as a branch of telemedicine, has gained growing interest in suicide prevention recently. This scoping review aimed to summarise the current literature on the role of TPIs in suicide prevention.
The findings of the studies generally showed that TPIs are effective in reducing suicide rates, suicide reattempts, and suicidal ideation. For example, De Leo et al. (2002) conducted a case-control study in Italy and found that significantly fewer suicide deaths occurred among elderly service users who received TPIs than those who did not (De Leo et al., 2002). Similarly, Vaiva et al. (2006), in a randomised controlled trial in France, found that telephone contact 1 month following discharge from the emergency department reduces the rate of suicide reattempt compared with no telephone contact in people initially admitted for attempted suicide by self-poisoning (Vaiva et al., 2006).
Literature also shows that TPIs are well-accepted and have high retention rates. Sankar et al. (2021) found that the intervention had high retention rates (77%), high scores on the client satisfaction questionnaire, and increased participant global scores on the working alliance inventory, which indicates a strong therapeutic alliance (Sankar et al., 2021). Similarly, Gabilondo et al. (2020) found that the intervention was well-accepted and showed improved adherence to outpatient follow-up. However, it is important to note that some studies found worse results in preventing suicidality when programmes do not last 12 months or more. As Gabilondo suggested maintaining the telephone follow-up for a minimum of 12 months would be more effective in reducing suicide rates.
The review also highlights the need for more studies in this area, particularly in regions with diverse populations. With the increasing availability of technology and the growing demand for mental health services, telepsychiatry can potentially increase the accessibility and efficacy of psychiatry interventions for patients at high risk of suicide.
The meta-analysis
The meta-analysis showed insignificant results in terms of the effectiveness of TPIs in reducing depression and suicide scores. However, the analysis did show significant heterogeneity among the studies, which could indicate that the results may vary depending on the specific intervention and population being studied. The number of suicide attempts, on the other hand, was significantly associated with TPIs, indicating a significant decrease in the number of suicides among those who received these interventions compared to those who did not. Overall, these results suggest that TPIs may effectively decrease the number of suicides among depressed patients. However, more research is needed to understand the specific factors contributing to the observed heterogeneity among the studies and determine the most effective telehealth interventions for reducing suicide risk.
Strengths of the study
The strengths of this study include the use of a comprehensive search strategy to identify relevant studies reducing the risk of bias and increasing the external validity of the results, and the rigorous selection criteria used to include only high-quality studies. Additionally, the use of meta-analysis allows for combining data from multiple studies to provide a more robust estimate of the overall effect of telehealth treatment on depression and suicide outcomes. Another strength of this meta-analysis is that it also used subgroup analysis and sensitivity analysis, which allowed for the examination of potential sources of heterogeneity among the studies, which improved the overall generalisability of the findings.
Limitations
One limitation of this scoping review is that the studies included in the review have varying sample sizes and sample characteristics, which may affect the generalisability of the findings. Additionally, the type of TPIs used in the studies and the method of support varied, making it difficult to compare the results of the studies and make definitive conclusions about the effectiveness of TPIs in suicide prevention. Another limitation is that most of the studies were conducted in Europe and North America, which may not represent other regions and countries with different cultural and societal factors that may affect suicide rates and access to mental health services. Furthermore, many of the studies did not assess the long-term impact of TPIs on suicide rates, which would be essential to consider when evaluating the effectiveness of these interventions. Lastly, the studies included in the review were limited to telephone calls and other forms of TPIs, such as video conferencing and online support, were not included, which may also affect the generalisability of the findings.
Recommendations
Based on the results of this study, it is recommended that future research focus on developing and implementing TPIs tailored to the specific needs of individuals with depression. This approach may include incorporating cognitive-behavioural therapy, mindfulness-based interventions, and other evidence-based treatments into telehealth programmes. Future studies should also have larger sample sizes and more extended follow-up periods to understand better the long-term effects of telehealth interventions on suicide rates.
It is also recommended to focus on specific subpopulations such as veterans, senior citizens, and individuals with specific disorders such as bipolar disorder, post-traumatic stress disorder, and schizophrenia. It will allow for a more comprehensive understanding of how telehealth interventions may be used to effectively prevent suicide among individuals with depression in these specific populations.
Furthermore, future research can explore other telehealth modalities, such as video conferencing, text messaging, and mobile apps, to determine their effectiveness in reducing suicide rates. This approach will help to identify which telehealth modalities are most effective and best suited to different populations and will help to guide the development of future telehealth interventions for suicide prevention.
Conclusion
In conclusion, TPIs are effective in reducing suicide rates, suicide reattempts, and suicidal ideation, with high acceptance rates and lasting efficacy, especially if maintained over 12 months. TPIs can significantly reduce the number of suicides among depressed patients, suggesting them as effective methods for suicide prevention. Our results support the continued use of telepsychiatry in suicide prevention programmes. However, more studies are needed to determine the optimal TPIs duration and identify the most effective delivery methods.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231206059 – Supplemental material for The effectiveness of telehealth interventions in suicide prevention: A systematic review and meta-analysis
Supplemental material, sj-docx-1-isp-10.1177_00207640231206059 for The effectiveness of telehealth interventions in suicide prevention: A systematic review and meta-analysis by Sheikh Shoib, Nour Shaheen, Almoatazbellah Anwar, Abdelrahman M. Saad, Laila Mohamed Akr, Alaa I Saud, Mrinmoy Kundu, Mahsa Nahidi, Miyuru Chandradasa, Sarya Swed and Fahimeh Saeed in International Journal of Social Psychiatry
Footnotes
Acknowledgements
No.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.