
Abstract
Background:
The concept of recovery for people with schizophrenia (PwS) is still a matter of debate. Growing numbers of PwS living to older age calls for examination of their disease trajectories with a focus on recovery.
Aim:
To compare two groups of PwS (good wellbeing; poor wellbeing) on several psychosocial variables associated with social wellbeing to identify interventions that support functional recovery.
Method:
Data was drawn from participants from across New Zealand (NZ), who had received a formal diagnosis of Schizophrenia; were living independently in the community, and who had undergone their first International Resident Assessment Instrument (interRAI) assessment from 2012 to 2022. We compared two groups of PwS (good social wellbeing; poor social wellbeing) examining associations with demographic and psychosocial variables.
Results:
We compared interRAI assessments for: ‘poor psychosocial wellbeing’ (n = 1,378; 67%; 56% female; 70.5% 65 years and over; 36.1% never married); and ‘good psychosocial wellbeing’ (n = 693; 33%; 61.1% female; 78.1% 65 years and over; 29.8% never married; n = 549 did not have sufficient social wellbeing data to be included). We found significant associations between social wellbeing and depression, disruptive behaviour, decision making, self-expression, understanding verbal information, activity level, self-reported health and medication adherence. Logistical regression showed depression (β = .84, p < .001, Wald = 51.01, Exp(B) = 2.31) and mild disruptive behaviour (β = .63, p = .002, Wald = 9.26, Exp(B) = 0.53) were the only predictors of poor social wellbeing. Those who reported some degree of depressive symptoms were 2.31 (CI [1.84, 2.91]) more likely to be in the poor social wellbeing group.
Conclusions:
A significant minority (33.5%) of older PwS enjoy positive social wellbeing. Several psychosocial variables are associated with wellbeing. By addressing the comorbidity of depressive symptoms, we may be able to improve wellbeing for older PwS.
Introduction
A report of spontaneous recovery in two cases of advanced ‘schizophrenic organismic stagnation’ in 1948 is probably the earliest published description of recovery in people living with schizophrenia (PwS; Boltz, 1948). In the 1950’s and 1960’s the term recovery in the context of PwS was used to describe recovery from acute psychotic episodes. However, our understanding of the potential for recovery has changed over time and numerous studies have now shown that a substantial proportion of PwS can experience significant degrees of recovery with good functional capacity (Bleuler et al., 1976; Ciompi & Müller, 1976; Harding et al., 1987; Strauss & Carpenter, 1972). The conceptualization of recovery from schizophrenia continues to evolve (Bellack et al., 2007; Valencia et al., 2015). Researchers conceptualize recovery as a long period of remission of psychotic symptoms, clinicians view recovery as an improved general functioning and patients perceive recovery as understanding the disorder, learning how to live with it and being able to have normal functioning in daily life (Bellack et al., 2007; Jose et al., 2015; Liberman & Kopelowicz, 2005).
Advances in the understanding of schizophrenia aetiology, natural history and treatment have increased interest in the development of consensus-defined standards for remission. The symptomatic remission scale in schizophrenia published by the American Psychiatric Association in 2005 became a standard measure of symptomatic remission used in more than 200 studies (Helldin et al., 2007). However, refinement, particularly in relation to psychosocial function and dysfunction, is greatly needed to capture patient-centred perceptions of recovery (Barak & Aizenberg, 2012; Valencia et al., 2015). While remission is conceptualized as improvement of psychotic symptoms – necessary but not sufficient for recovery – recovery reflects overall functioning in everyday life, that is, improved psychosocial wellbeing or ‘functional’ recovery. To date, several functional recovery models have been proposed acknowledging that ‘functional’ recovery is a multidimensional construct along a continuum (Davidson et al., 2005; Jacobson & Greenley, 2001; Liberman & Kopelowicz, 2005).
With an aging population the numbers of people suffering from schizophrenia who are 65 years or older are increasing, with the number of people suffering from schizophrenia over the age of 55 years predicted to double by 2050 (Cohen et al., 2015). This will present an increased demand for both healthcare and social services. However, less than 1% of scientific publications about schizophrenia are devoted to older adult patients (Cohen et al., 2018), and even fewer about recovery in older adult patients. Thus, there is a need to study older people suffering from schizophrenia especially as reports examining the trajectory of aging with schizophrenia are contradictory (Lyketsos & Peters, 2015; Mentzel et al., 2023). Studies taking a psychosocial approach to examine functional recovery for older people living with schizophrenia are needed to direct potentially helpful interventions for older adults.
Additionally, a fuller understanding of the progression of schizophrenia through the life cycle is required. The ongoing social course for those with schizophrenia comes about from an interplay between biological, developmental and environmental factors over time. Throughout the life course, pronounced age differences emerge in illness and socially negative behaviours (Häfner et al., 1998). An approach advocating for different interventions over a person’s lifetime was first publish 30 years ago (Adler et al., 1995). This approach focussed on providing access to a continuum of services in the context of a comprehensive mental healthcare programme and is still relevant today. Resiliency factors for those who survive into older age are diverse and include engaging with life, social connectedness, health and well-being and generalized positive attitudes (Smart et al., 2021). In their study on life course perspectives of adults with schizophrenia, Walker and Harrison (2023) suggest that aging adults are experts on their own care. Few studies ask PwS to reflect on their own needs throughout their life. Life course input from PwS would help inform a continuum of healthcare interventions relevant for the diverse population of PwS throughout their life course (Meester et al., 2019).
In the present study we use indicators of social functioning ‘social wellbeing’ as a proxy measure of functional recovery. That is, we defined social wellbeing based on measures of ‘loneliness’, ‘social engagement’ and ‘social adversity’. Using data from the International Resident Assessment Instrument (interRAI; Hogeveen et al., 2017) we compared two groups of PwS, those with poor social wellbeing and those with good social wellbeing. We examined multiple additional psychosocial factors and their association with social wellbeing amongst older people with schizophrenia. Specifically, we explored which psychosocial factors predicted good or poor social wellbeing to direct future research towards potentially helpful interventions to support functional recovery for PwS.
Method
The International Resident Assessment Instrument (interRAI) is a comprehensive clinical assessment evidence-based tool (Hogeveen et al., 2017) developed to assess a wide range of a person’s life to determine which services best meet that person’s need. The 236-item electronically recorded assessment includes demographic, physical, psychological and cognitive domains. In New Zealand, the interRAI assessment, which has been mandatory since 2013, is a prerequisite for older adults who need additional support services in their home or need to transfer to residential care (Barak et al., 2020; Leitch et al., 2018). Data for this study was drawn from participants, from across all New Zealand District Health Boards, who had undergone their first interRAI assessment during the period September 2012 to September 2022. The data were included from those participants who (1) had provided consent for their anonymized data to be used for research purposes; (2) received a formal diagnosis of Schizophrenia; and (3) were living independently in the community (e.g. home, apartment and rented room). Only data from the initial (first) interRAI assessments were reviewed, even if multiple assessments had been completed.
Compliance with ethical standards
Ethical approval for this study was obtained from the University of Otago Ethics Committee, approval # HD22/078.
Social wellbeing ‘functional recovery’
As a working model and proxy of functional recovery for PwS we used three measures from the interRAI: social engagement (engagement, no engagement), social adversity (no adversity, possible adversity) and loneliness (lonely, not lonely). We defined poor social wellbeing as those who reported feeling lonely or having no social engagement or experiencing possible social adversity, and good social wellbeing as those who reported no loneliness together with social engagement and no social adversity.
Psychosocial variables of recovery
We selected 11 additional interRAI variables that measure seven psychosocial domains of recovery (mood and behaviour; cognitive performance, communication, functional status, health conditions, medication adherence and social support). Each item was rescaled in a similar fashion to previously published data to provide a suitable scoring system for analysis.
Analytic strategy
Descriptive demographic (age, gender, ethnicity and marital status) statistics and descriptive statistics for the 11 additional psychosocial variables (depression rating scale, disruptive behaviour scale, decision making, self-expression, understanding verbal information, self-performance, activity level, self-reported health, alcohol use, medication adherence and living arrangements) are presented for each social wellbeing group – poor social wellbeing and good social wellbeing. Bivariate analyses (chi-square) were used to explore associations between the proportion of PwS in the two social wellbeing groups for each of the demographic variables and the 11 psychosocial variables of recovery. Where a relationship was found, post hoc analysis and calculations of Z-scores and p-values with Bonferroni correction for type-1 error were used to further evaluate pairwise relationships. Cramer’s V measures were included to present effect sizes. Logistic regression analysis was used to determine whether any of the 11 psychosocial factors significantly associated with social wellbeing could differentiate between PwS who were in the poor or good social wellbeing groups. We analysed the data using SPSS Statistics 25 (StataCorp, 2021). For all the analyses, unless otherwise stated, statistical significance was determined by (two-sided when appropriate) p < .05.
Results
A total of 2,620 interRAI first assessments were undertaken for people with schizophrenia across District Health Boards in New Zealand between September 2012 and September 2022. We selected interRAI assessments for two social wellbeing groups: ‘poor social wellbeing’ (n = 1,378) where PwS reported loneliness or no social engagement or possible social adversity; ‘good social wellbeing’ (n = 693) where PwS reported no loneliness together with no social adversity and had social engagement on their interRAI assessment. The remaining assessments (n = 549) did not have sufficient social wellbeing data to be included. The analysed sample (N = 2,071; mean age = 70 years 4 months, range = 23–102 years; SD = 11.01 years) consisted of 1,192 (57.7%) assessments for females and 874 (4.3%) for males (gender was not reported for five clients); 559 (27.0%) were aged 64 years and under and 1,512 (73.0%) were aged 65 years and over; and identified as NZ Europeans (1,369; 66.1%), Māori (291; 14.1%), Pacific People (102; 4.9%) and other ethnicities (309; 19.9%), see Table 1.
Demographic characteristics by social wellbeing group (poor social wellbeing; good social wellbeing).
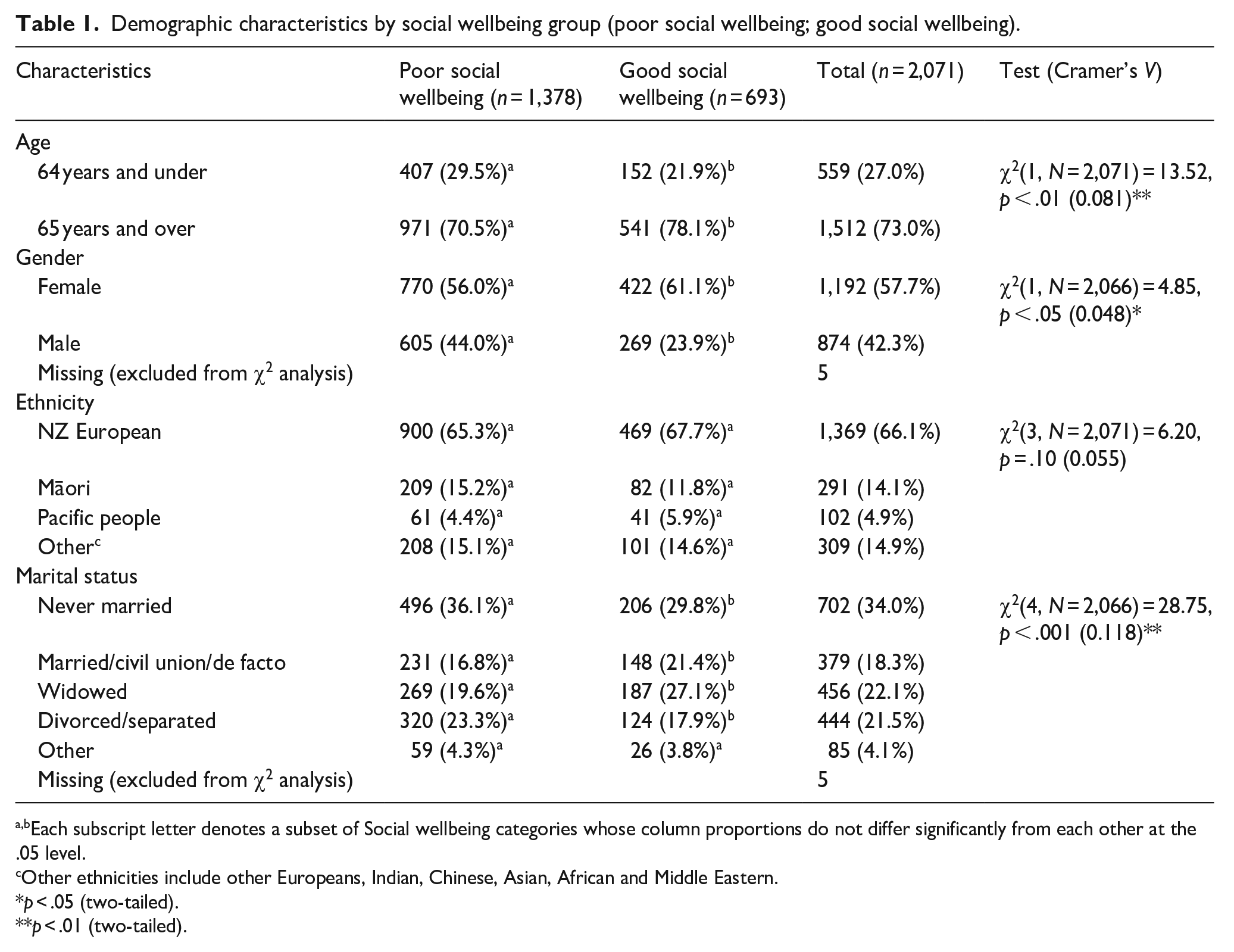
Each subscript letter denotes a subset of Social wellbeing categories whose column proportions do not differ significantly from each other at the .05 level.
Other ethnicities include other Europeans, Indian, Chinese, Asian, African and Middle Eastern.
p < .05 (two-tailed).**p < .01 (two-tailed).
Demographic factors
We ran four independent chi-square analysis to investigate possible associations between social wellbeing group (poor, good) and ethnicity, age, gender and marital status. Significant associations between social wellbeing group and age, gender and marital status were found. The good wellbeing group was made up of a significantly greater proportion of PwS in the 65 years and over group (78.1%), a greater proportion of female PwS (61.1%) and a significantly greater proportion of PwS who were married (21.4%) or widowed (27.1%) compared to the poor wellbeing group. No significant association between social wellbeing group and ethnicity was found. All results are presented in Table 1.
Additional psychosocial variables of functional recovery
We conducted a series of independent chi-square analyses to investigate associations for each of the additional 11 psychosocial variables (depression, disruptive behaviour, decision making, self-expression, understanding verbal information, self-performance, activity level, self-reported health, alcohol use, medication adherence and living arrangements) with social wellbeing group (poor social wellbeing: loneliness or no social engagement or possible social adversity; good social wellbeing: no loneliness and no social adversity and social engagement). Significant associations between social wellbeing group and depression, disruptive behaviour, decision making, self-expression, understanding verbal information, activity level, self-reported health and medication adherence were found. The good wellbeing group was made up of a significantly greater proportion of PwS with no depression (76.2%), no disruptive behaviour (92.5%), intact decision making (56.9%), who are always understood by others (62%), who always understood verbal information from others (58.3%), who were active (67.7%), who adhered to their medication regime (96.4%) and a significantly smaller proportion of PwS who self-reported poor health (11.9%) compared to the poor wellbeing group. No significant association between social wellbeing group and self-performance, alcohol use or living arrangements was found. All results are presented in Table 2.
Psychosocial variables of recovery by social wellbeing group (poor social wellbeing; good social wellbeing).
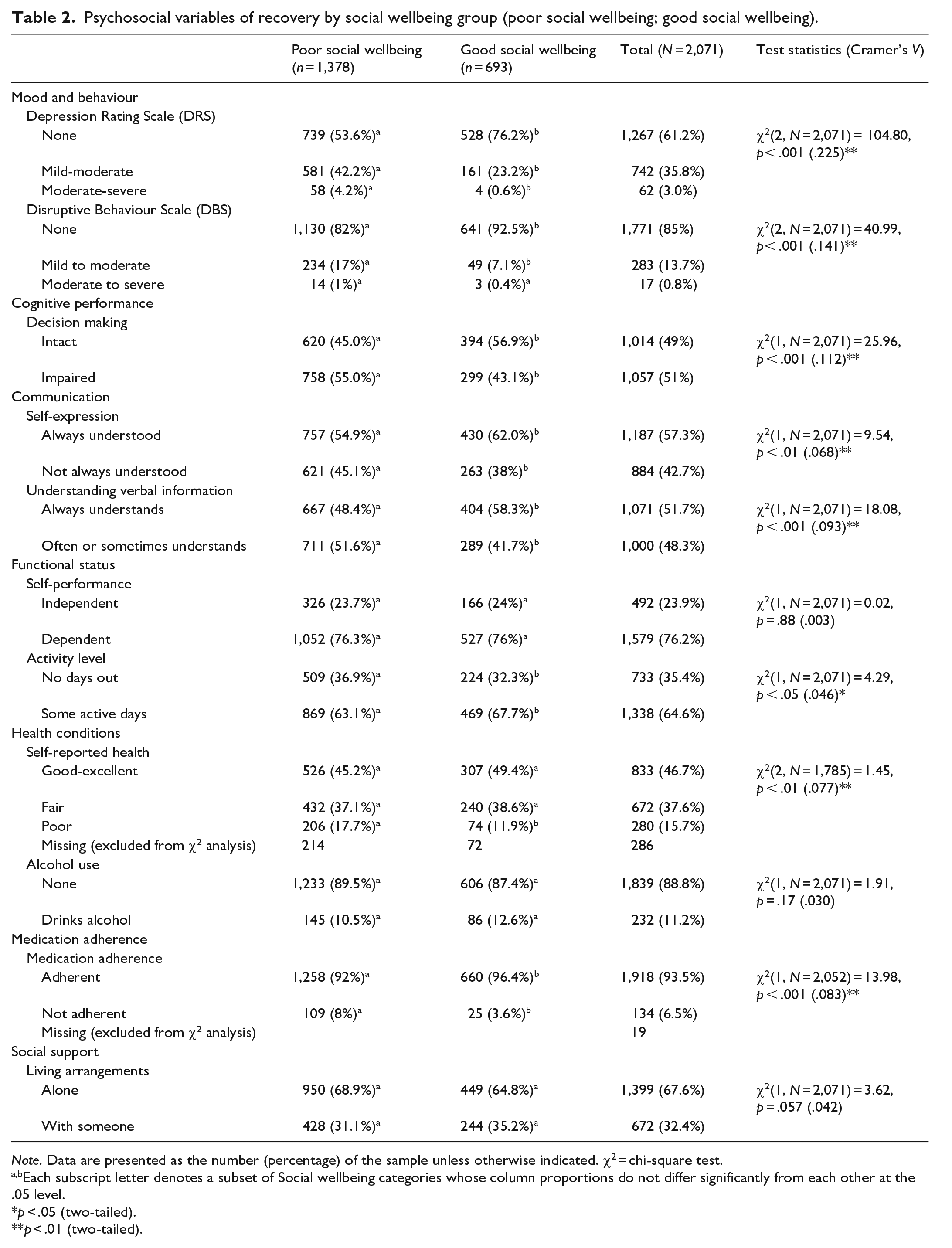
Note. Data are presented as the number (percentage) of the sample unless otherwise indicated. χ2 = chi-square test.
Each subscript letter denotes a subset of Social wellbeing categories whose column proportions do not differ significantly from each other at the .05 level.
p < .05 (two-tailed).**p < .01 (two-tailed).
Predictors of social wellbeing
To determine whether any of the psychosocial variables could differentiate between PwS who were in the poor and good social wellbeing groups, we performed a logistic regression analysis using only those independent variables that showed a significant association in the previous chi-square analyses. That is, we used Depression Rating Scale (DRS; none, mild-moderate, moderate-serve), Disruptive Behaviour Scale (DBS; none, mild-moderate, moderate-serve), decision making (intact, impaired), self-expression (always understood, not always understood), understanding of verbal information (always understands, often or sometimes understands), activity level (no days out, some active days), self-reported health (good-excellent, fair, poor) and medication adherence (adherent, not adherent) as the predictor variables with social wellbeing (poor, good) as the dependent variable. Overall, the logistical regression model was statistically significant (χ2 (11) = 111.12, p < .001). The model explained 9.3% (Nagelkerke R2) of the variance in wellbeing group and correctly classified 65.1% of cases. We found that low to moderate depression (β = .78, p < .001, Wald = 43.35, Exp(B) = 0.46) and moderate to severe depression (β = 2.21, p < .001, Wald = 13.36, Exp(B) = 0.11) both predicted a high probability of poor social wellbeing. Mild disruptive behaviour was also a predictor of poor social wellbeing (β = .63, p = .002, Wald = 9.26, Exp(B) = 0.53). Although all other variables included in the logistic regression model were significantly associated with social wellbeing group, they did not significantly predict probability of wellbeing.
To further investigate the role of ‘any’ depressive symptomology in predicting wellbeing, we conducted a second logistical regression where depression was recategorized from three categories to a binomial measure of depressive symptoms reported as present or not present. We found that PwS who reported some degree of depressive symptoms were 2.31 (CI [1.84, 2.91]) more likely to be in the poor social wellbeing group than PwS who reported no depressive symptoms (β = .84, p < .001, Wald = 51.01, Exp(B) = 2.31).
Discussion
The number of older adults suffering from schizophrenia is increasing yet less than 1% of published studies about schizophrenia focus on older PwS. Research indicates these individuals may age differently from the general population due to lifestyle, medication factors and effects of the disease itself (Taube et al., 2023). Functional recovery or social wellbeing has rarely been a focus of study in older PwS as long held ageistic assumptions about rates of dementia, need for long-term facilities placement and acceptance of loneliness were not challenged. The outcome of schizophrenia in later life can be evaluated from several different perspectives – physical and mental health, recovery and remission. Longitudinal data on measures of recovery in older individuals with schizophrenia are scant. Not only do we know very little about recovery in older individuals but the processes that are associated with functional recovery in older PwS (Mentzel et al., 2023) are also not known or studied. In the present analysis we focussed on untangling the indicators associated with or predictive of social wellbeing, used in this study as a proxy for functional recovery in older PwS. Of the 11 psychosocial variables analysed – depression rating scale, disruptive behaviour scale, decision making, self-expression, understanding verbal information, self-performance, activity level, self-reported health, alcohol use, medication adherence and living arrangements – most were associated with social wellbeing (i.e. either good or poor wellbeing) except for alcohol use, self-performance and living arrangements. Good wellbeing was associated with no depression, no disruptive behaviour, capable of decision making, intact communication skills, being active and adhering to medication.
Predicting social wellbeing is an important step in allocating resources and designing appropriate interventions. In the present study, we found that both depression and disruptive behaviour predicted likelihood of poor social wellbeing. Schizophrenia is associated with a range of symptoms, typically separated into positive and negative. It is widely accepted that mood disturbances are often observed alongside a diagnosis of schizophrenia (Als et al., 2023). Specifically, depression may occur in any phase of schizophrenia and can have far reaching consequences. The socially inappropriate or disruptive behaviours as defined by the interRAI manual are behaviours that are distressing or disruptive to the person or others with whom the person lives. Such behaviours include for example making disruptive noises or sounds, screaming, smearing or throwing food or faeces, hoarding or rummaging through others’ belongings.
It is beyond the scope of this study to assess the directionality of relationships between psychosocial variables such as depression, disruptive behaviours and social isolation. Studies suggested higher depression rates in PwS compared to healthy controls during the COVID pandemic. Isolation during this period emerged as a risk factor for the development of depressive symptoms emphasizing the directionality of the association between these variables. Identifying the risk factors for developing depression in this population helps find new, suitable approaches to address patients' needs and lower the adverse psychological effects of social isolation (Seyedmirzaei et al., 2023). In other studies higher level of loneliness was associated higher severity of depression, poorer quality of life and higher use of maladaptive coping in PwS (Suman et al., 2023). Furthermore, PwS loneliness scores predicted a diagnosis of drug abuse (Trémeau et al., 2016). We may tentatively suggest that the association of depression, loneliness and disruptive behaviours in PwS is bidirectional.
The identification of depression and disruptive behaviours as predictors of poor social wellbeing in PwS indicate particular treatment interventions. Given that PwS who reported some degree of depressive symptomatology had a much higher risk (i.e. 2.31 more likely) to be in the poor wellbeing group, depression should be screened for in this population and treated. Disruptive behaviours can also be effectively treated. Recent studies analysing the evolution of social functioning and behaviour problems amongst PwS emphasize the need for and effectiveness of implementing psychosocial intervention programmes that promote functional recovery and keep disruptive behaviours from becoming chronic (Vázquez-Reyes et al., 2022).
In particular, the findings of the present study that depression is predictive of a poor outcome for older PwS fits with existing research demonstrating poor outcomes for those with depression. For example, a history of depression in the chronic phase predicted the future worse clinical outcome in PwS in older age (Yamada et al., 2022). Another study that examined data from a cohort of individuals with Schizophrenia, aged 55 years or more in the US, demonstrated that the majority had either subsyndromal or syndromal depressive symptoms and these were independently associated with lower quality of life (Hoertel et al., 2019). Furthermore, a recent study examined the prevalence of depressive symptoms and their associations with quality of life in clinically stable older PwS and again demonstrated that the presence of depressive symptoms negatively impacted quality of life. The authors concluded that considering the negative impact of depressive symptoms on QOL, regular screening for and appropriate treatment for depression are recommended as paramount for this population (Li et al., 2021). Clearly, given the small but growing body of research indicating an association between depressive symptomatology and poorer outcomes of older PwS this is an important issue to consider and address.
Furthermore, the present study highlights the association of several clusters of indicators with social wellbeing in older PwS. The psychosocial variables that we found were associated with social wellbeing can be usefully grouped into the following three clusters: demographic that included age, gender and being married currently or in the past; neuropsychiatric composed of depression, disruptive behaviour, decision making and communication with others; and health behaviours that included activity levels, self-reported health and adherence to medications. The interplay and connections between these clusters of psychosocial variables is unknown and warrants further investigation. Additionally, the relationship between clinical recovery and functional recovery is yet to be untangled. Functional recovery could be compared to clinical recovery with the use of psychometric scales. Since its publication in 2005, the symptomatic remission scale in schizophrenia has been examined in more than 200 studies. Refinement however is greatly needed, particularly in relation to psychosocial function and dysfunction. Clinician ratings of patients’ behaviour are common however typically rely on brief contact with the patient and do not adequately reflect on patients’ ability to function in the real world (Barak et al., 2010). In a comprehensive European project in only 18% of cases did patient, relatives and psychiatrists agreed in their assessments of patient remission of schizophrenia. A more thorough consideration of patients' and caregivers' perspectives should supplement the experts' assessment (Karow et al., 2012). A few studies have examined wellbeing in older age persons with schizophrenia and indicate that wellbeing can improve with age and that particular demographics may be associated with wellbeing. For example, a Dutch study evaluated the 5-year outcome of clinical recovery, that is symptomatic remission, and subjective well-being in a sample of older Dutch patients with schizophrenia. At baseline, only 5.5% of participants qualified for clinical recovery, while at 5-year follow-up this rate more than doubled. Subjective well-being was reported by more than 20% of participants at follow up however, clinical recovery and subjective well-being were not correlated (Meesters et al., 2021). An Australian study examining the lives of people who live with psychotic disorders into middle age and beyond focussed amongst other outcomes on social functioning. The older group contained more women, were more likely to have an affective component and more likely to be living alone. The authors concluded that the characteristics of people with psychosis change significantly as they progress into the middle age and beyond and emphasized that a better understanding of these differences is important in informing targeted treatment strategies for older people living with psychosis (Galletly et al., 2022). Symptomatic remission, psychosocial remission and functioning could be achievable goals for a considerable number of patients. New approaches should include multidimensional measures such as remission, cognition, psychosocial functioning and quality of life, to assess functional outcome in schizophrenia research (Valencia et al., 2015). The scant existing studies of wellbeing, and relationships between clinical recovery and functional recovery in an aging population of PwS all indicate the need for further research in this area.
Limitations
There are limitations that we need to acknowledge to place the findings of this study in perspective. The interRAI assessment surveys a sample of older adults who are frailer than the general older population as they are needing assessment related to their health issues and needed care (Ludwig & Busnel, 2017). In this way, the study may include a sample that is biased in terms of poorer health outcomes. On the other hand, however, we may have captured the less frail PwS as our sample was limited to those able to be still living independently in the community whereas many PwS in this age group, if still alive, are already in long-term care facilities. Given this, further studies are needed that include a complete representation of older PwS. Also, fundamentally the concept of functional recovery or social wellbeing is a continuum with excellent functional recovery at one end and poor functional recovery at the other (Davidson et al., 2005; Jacobson & Greenley, 2001; Liberman & Kopelowicz, 2005). The file data collected via the interRAI does not readily lend itself to defining social wellbeing as a continuum, so we therefore relied on a dichotomous definition of social wellbeing. Further studies are needed that more exactly define social wellbeing and functional recovery as a continuous concept. Further, the data presented here are a snapshot taken at one time-point in a person’s life (i.e. at time of first interRAI). It is highly likely that throughout their lifetime a PwS may experience ebbs and flows of functional recovery and social wellbeing and that may be influenced by different psychosocial variables at different stages of life. There is need for longitudinal studies to investigate lifetime changes in functional recovery and wellbeing for PwS across time and life stage.
In conclusion, the present study analysed data from a large and comprehensive set of assessments and focussed on social wellbeing, as a proxy for functional recovery of older PwS. This study presents a complex picture of psychosocial variables associated with wellbeing and functional recovery. The main finding of the association between presence of depression and poor wellbeing in the analysed cohort is strongly indicative that by addressing the comorbidity of depressive symptoms in older PwS we may be able to improve their wellbeing as they age.