
Abstract
Background:
Few studies have examined whether social support contributes to better consequences among chronic patients with severe mental illnesses (SMI) in their community recovery stage and whether self-stigma would be a mechanism through which social support impacts psychiatric symptoms and personal and social functioning.
Aims:
This study aimed to examine prospective associations of social support with long-term self-stigma, psychiatric symptoms, and personal and social functioning, and to investigate whether self-stigma would mediate the associations of social support with psychiatric symptoms and personal and social functioning among patients with SMI.
Methods:
A total of 312 persons with SMI (schizophrenia and bipolar disorder) in their community recovery stage participated in the study. Social support, self-stigma, psychiatric symptoms, and personal and social functioning were evaluated at baseline. The follow-up assessment was conducted at 6 months with the baseline measures except for social support. Hierarchical linear regression and mediation analysis were performed.
Results:
The results showed that baseline social support predicted decreases in stigma (β = −.115, p = .029) and psychiatric symptoms (β = −.193, p < .001), and increases in personal and social functioning (β = .134, p = .008) over 6 months, after adjusting for relevant covariates. Stigma at 6 months partially mediated the association between baseline social support and 6-month psychiatric symptoms (indirect effect: β = −.043, CI [−0.074, −0.018]). Stigma and psychiatric symptoms at 6 months together mediated the association between baseline social support and 6-month personal and social functioning (indirect effect: β = .084, 95% CI [0.029, 0.143]).
Conclusion:
It is necessary to provide comprehensive social support services and stigma reduction interventions at the community level to improve the prognosis of SMI.
Keywords
Introduction
Mental disorders are both leading causes of disability and significant risk factors for premature mortality (Charlson et al., 2015; Rehm & Shield, 2019). Epidemiological and economic estimates suggest that the global burden of mental disorders is considerable, both in its impacts on human health and losses to societal welfare (Arias et al., 2022). In China, the prevalence of mental disorders is 9.32% in adults, imposing a tremendous burden on the healthcare system (Huang et al., 2019). Severe mental illness (SMI), such as schizophrenia and bipolar disorder, is chronic mental disorder. The estimated lifetime prevalence of schizophrenia is 0.59% and bipolar disorders is 0.6% in China (Huang et al., 2019). The prolonged course of illness and the persistent psychiatric symptoms can cause serious damage to personal and social functioning, such as unemployment, poverty, and social isolation, which seriously affects patients’ quality of life and further increases the burden of social and family care (Owen et al., 2016). Therefore, it is crucial to identify the factors associated with the changes in social functioning among patients with SMI.
Social support is commonly construed as a salutary factor in health promotion due to its direct positive effect on health or as a buffer against emotional distress (Merritt et al., 2022). A longitudinal study with 1-year follow-up found that regular social support from both family members and non-family members predicted better subsequent social functioning and quality of life among patients with schizophrenia (Goodsmith et al., 2023). Another study examined the factors influencing the psychiatric symptoms and duration of hospitalization of patients with schizophrenia and demonstrated that the existence of social support contributed to the improvement of psychiatric symptoms and the recovery of the disease (Velelekou et al., 2022). Similar findings are indicated in patients with bipolar disorder. A study demonstrated that social support significantly predicted psychosocial functioning in bipolar patients (Dou et al., 2021). Another longitudinal research evaluated psychosocial risk factors of mood symptoms among patients with bipolar disorder (Weinstock & Miller, 2010). The results showed that social support alone emerged as a unique predictor of depressive symptoms at the 1-year follow-up. Although social support is widely acknowledged as a predictor of psychiatric symptoms and social functioning of patients with schizophrenia and bipolar disorder, the mechanism through which it takes effect is underinvestigated.
Stigma is widely recognized as a barrier for patients to engage in treatment for mental disorders, resulting in aggravation of the negative outcomes associated with mental illness (Thornicroft et al., 2009, 2016). A longitudinal study found that increased stigma levels predicted greater psychiatric symptom severity over a 4-year period among SMI patients (Von Mach et al., 2022). In addition, several longitudinal studies reported that the reduction in self-stigma positively predicted changes in social functioning over time among patients with mental disorders (Chien et al., 2015; Yanos et al., 2012). Lam et al. (2010) found that the mental health stigma might be particularly deeply rooted due to cultural factors in China. Patients with SMI and their family members commonly conceal the fact of their mental illnesses, which largely hinders the treatment and recovery of patients (Lam et al., 2010).
Social support and stigma are not only important predictors of psychiatric symptoms and social functioning in SMI patients, they are also closely associated with each other. On the one hand, perceived stigmatization of mentally ill people may impair their social connections. On the other hand, social isolation often exacerbates patients’ internalized stigma (Mueller et al., 2006). A longitudinal study examined the reciprocal effects between stigmatization and social support among persons with mental problems and indicated that social support strongly predicted perceived stigma 1 year later in the group with a more recent onset of illness, suggesting that the social support modified the perception of stigma (Mueller et al., 2006). Moreover, according to the results of a cross-sectional study conducted in Hong Kong among persons with SMI, social support contributed to the reduction in self-stigma (X. H. Li et al., 2021).
Considering that internalized stigma is closely associated with both social support and negative mental health outcomes, such as severe psychiatric symptoms and chronic impairment of personal and social functioning (Chien et al., 2015; X. H. Li et al., 2021; Mueller et al., 2006; Thornicroft et al., 2009, 2016; Von Mach et al., 2022; Yanos et al., 2012), it may act as a mediator between social support and psychiatric symptoms or personal and social functioning. Social support may work by decreasing the perception of self-stigma and further contribute to better mental health consequences among persons with SMI. However, few studies have investigated whether self-stigma would be a mechanism through which social support impacts psychiatric symptoms and personal and social functioning, especially in the Chinese context. Moreover, although the protective effect of social support on mental health outcomes is widely documented in existing literature, it was mainly examined among those hospitalized or newly onset population (Dou et al., 2021; Goodsmith et al., 2023; Mueller et al., 2006; Velelekou et al., 2022). Few studies have examined whether social support contributes to better consequences among chronic SMI patients in their community recovery stage.
This study aimed to examine the prospective associations of social support with long-term self-stigma, psychiatric symptoms, and personal and social functioning, and to investigate the mechanisms through which social support would affect psychiatric symptoms and personal and social functioning. It was hypothesized that the initial level of social support would predict decreases in self-stigma and psychiatric symptoms, as well as the increase in personal and social functioning at follow-up over 6 months. In addition, it was postulated that self-stigma would mediate the associations of social support with psychiatric symptoms and personal and social functioning in a longitudinal timeframe.
Methods
Ethical approval
This study was reviewed and approved by the Ethics Committee of Peking University Sixth Hospital (approval reference number: 2012-3) prior to its initiation. All participants provided written informed consent, and their caregivers provided written or verbal informed consent.
Participants
Participants were patients with schizophrenia or bipolar disorder recruited from communities located in three cities (Taiyuan, Chongqing, and Zigong) across three provinces (Shanxi, Chongqing, and Sichuan) in China from September 2021 and April 2022. The description of study sites within the three cities and the number of participants recruited from each site is shown in Table 1. The recruitment of participants was based on posters and recommendations from community doctors. The inclusion criteria of participants were (1) diagnosed with schizophrenia or bipolar disorder according to the medical record; (2) age between 18 and 60 years old; (3) mental illness conditions stable for at least 3 months; and (4) no drug or alcohol abuse. A total of 312 participants were recruited at baseline. The follow-up assessment was conducted at 6 months after the initial evaluation and 311 participants (response rate 99.7%) replied at the 6-month follow-up.
Description of study sites and the number of participants recruited from each site.
Procedures
At the baseline assessment, the participant was interviewed individually and face-to-face by a psychiatrist in the research team to evaluate his/her eligibility and to collect socio-demographic information and relevant medical history. The severity of psychiatric symptoms and personal and social functioning were also evaluated during the interview. Stigma and social support were assessed by self-report or a trained research assistant if the participants felt difficult to read by themselves. Participants who completed the baseline assessment were reevaluated at 6 months with the measures of stigma, psychiatric symptoms, and personal and social functioning. All the evaluations were individually face-to-face interviews conducted by psychiatrists and trained research assistants in the research team. Participants received small incentives in money, gifts, or other forms for their time and effort to take part in the study upon the completion of each assessment.
Measures
Social support
The Social Support Rating Scale (SSRS) was used to measure social support at baseline (Xiao, 1994). The scale has been widely applied in the Chinese population and its validity and reliability have been confirmed in different samples (Leung et al., 2007; Qi et al., 2020; Xiao, 1994). There are a total of 10 items on the scale, including three dimensions of subjective support (four items), objective support (three items), and utilization of support (three items). Item scores of the SSRS were added, generating a total support score ranging between 12 and 66. Higher scores indicated stronger social support. The Cronbach’s α coefficient of this scale was .63 at baseline.
Self-stigma
The Internalized Stigma of Mental Illness Scale (ISMI) was used to measure self-stigma at baseline and 6 months (Boyd et al., 2014; Q. Li et al., 2009). It contains 29 items with high reliability and validity. There are five subscales including alienation, stereotype endorsement, perceived discrimination, social withdrawal, and stigma resistance. Each item score ranges from 1 (strongly disagree) to 4 (strongly agree). Sum scores of all items were computed to demonstrate the patients’ awareness of self-stigma. The score ranges between 29 and 116 with higher values representing more severe internalized stigmatization. The internal consistency of the scale in this study was high with Cronbach’s α being .90 and .93 at baseline and 6 months, respectively.
Psychiatric symptoms
The Positive and Negative Syndrome Scale (PANSS) was used to assess psychiatric symptoms at baseline and 6 months (Bowie et al., 2010; Kay et al., 1987). It was evaluated by the psychiatrists in the research team. The scale is a well-developed scale with good reliability and validity. It contains 30 items with 7 measuring positive symptoms, 7 measuring negative symptoms, and 16 items measuring general aspects of psychopathology. Each item score ranges from 1 to 7 with 1 representing the absence of symptom and 7 representing extremely serious symptom. Sum scores of the whole scale were calculated to represent the overall psychiatric symptoms, with the range being between 30 and 210. Higher scores indicated more severe symptoms. The Cronbach’s α coefficients were .96 and .95 at baseline and 6 months, respectively.
Personal and social functioning
The Personal and Social Performance Scale (PSP) was used to measure personal and social functioning at baseline and 6 months (Morosini et al., 2000; Tianmei et al., 2011). It was developed based on the social functioning component of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) and was evaluated by the psychiatrists in the research team. The scale is a 100-point single-item rating scale with higher scores representing better personal and social functioning. The ratings are based on four main areas: (a) socially useful activities, including work and study; (b) personal and social relationships; (c) self-care; and (d) disturbing and aggressive behaviors. The internal consistency reliability of this scale was high in this study, with Cronbach’s α being .82 and .85 at baseline and 6 months, respectively.
Demographic characteristics
A self-designed questionnaire was used to assess participants’ demographic characteristics, including age, gender, education, marital status, whether living alone, diagnosis, and duration of their mental illness.
Statistical analyses
Continuous variables were reported as means ± SD, and discrete variables were reported as N’s and percentages. Hierarchical linear regression analyses were conducted to test whether baseline social support would predict stigma, psychiatric symptoms, and personal and social functioning, separately, at 6 months. Relevant demographic variables, including education, diagnosis, and duration of illness, were adjusted as covariates, given that they were correlated with the outcomes (rs = −.20 to 12). Baseline stigma, psychiatric symptoms, and personal and social functioning, respectively, was also included as a covariate. In each hierarchical regression model, covariates were entered as a block in the first step, followed by baseline social support in the next step.
Moreover, mediation models were fitted through the PROCESS SPSS macro (Hayes, 2009; Preacher & Hayes, 2008) to examine whether stigma would mediate the longitudinal associations between baseline social support and psychiatric symptoms or personal and social functioning at 6 months. The total mediation effect of stigma and psychiatric symptoms between baseline social support and personal and social functioning at 6 months was also tested. All mediation models were adjusted for baseline psychiatric symptoms or personal and social functioning and relevant demographic variables, including education, diagnosis, and duration of illness. The 95% confidence intervals (95% CI) were calculated with 5,000 bootstrapped samples. To create the 95% CI, the 5,000 estimates of the indirect effect were sorted from low to high, and the 2.5th and 97.5th percentiles were taken as the lower and upper limits, respectively. All statistical analyses were conducted with the SPSS 26.0 for Windows.
Results
Participant characteristics
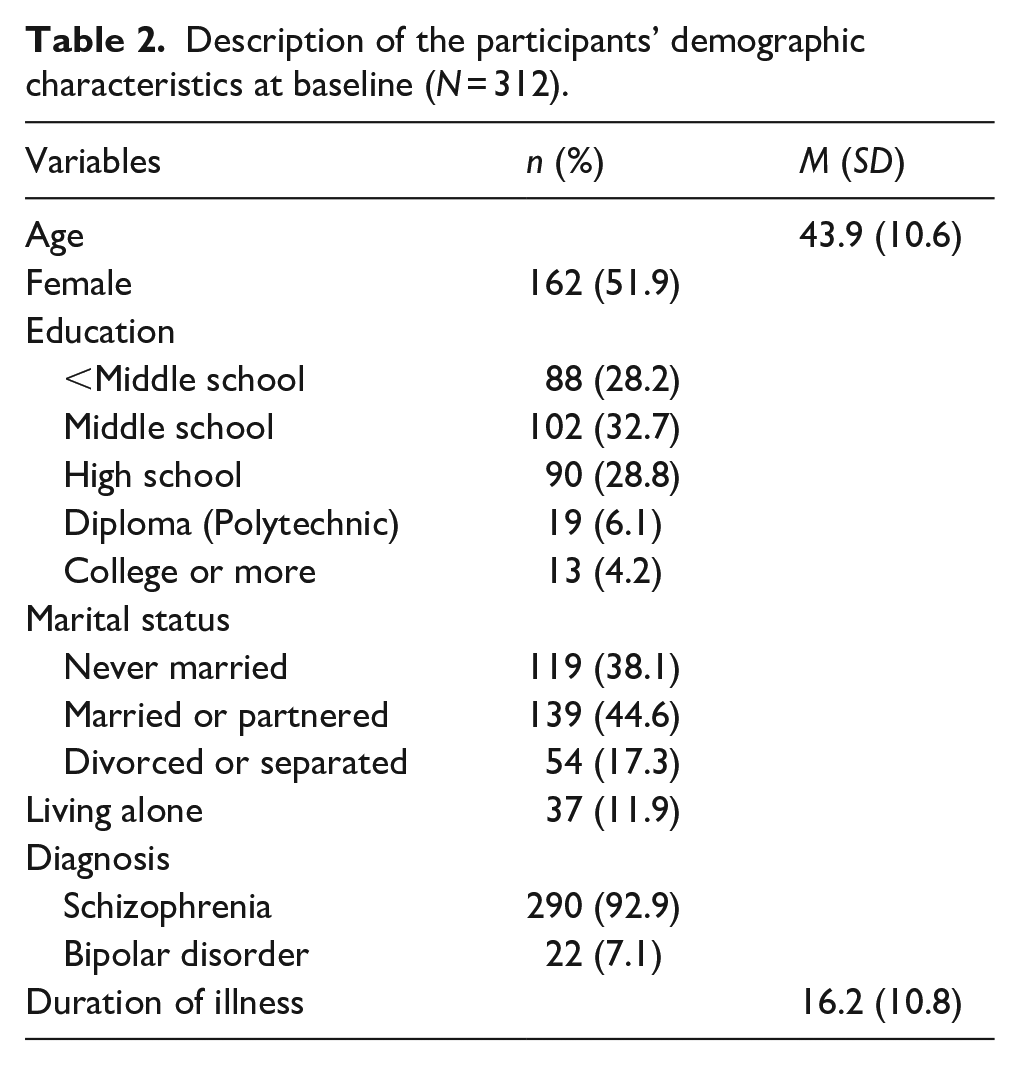
There were 312 participants (150 males and 162 females) with a mean age of 43.9 years (SD = 10.6 years) at baseline. The participant characteristics are listed in Table 2. Most of the participants had achieved an educational level of middle school (32.7%) or high school (28.8%); 44.6% were married or partnered; and 11.9% were living alone at the time when they were interviewed. The diagnoses of participants’ included schizophrenia (92.9%) and bipolar disorder (7.1%). The mean duration of illness was 16.2 years (SD = 10.8 years). One participant dropped out at 6 months.
Description of the participants’ demographic characteristics at baseline (N = 312).
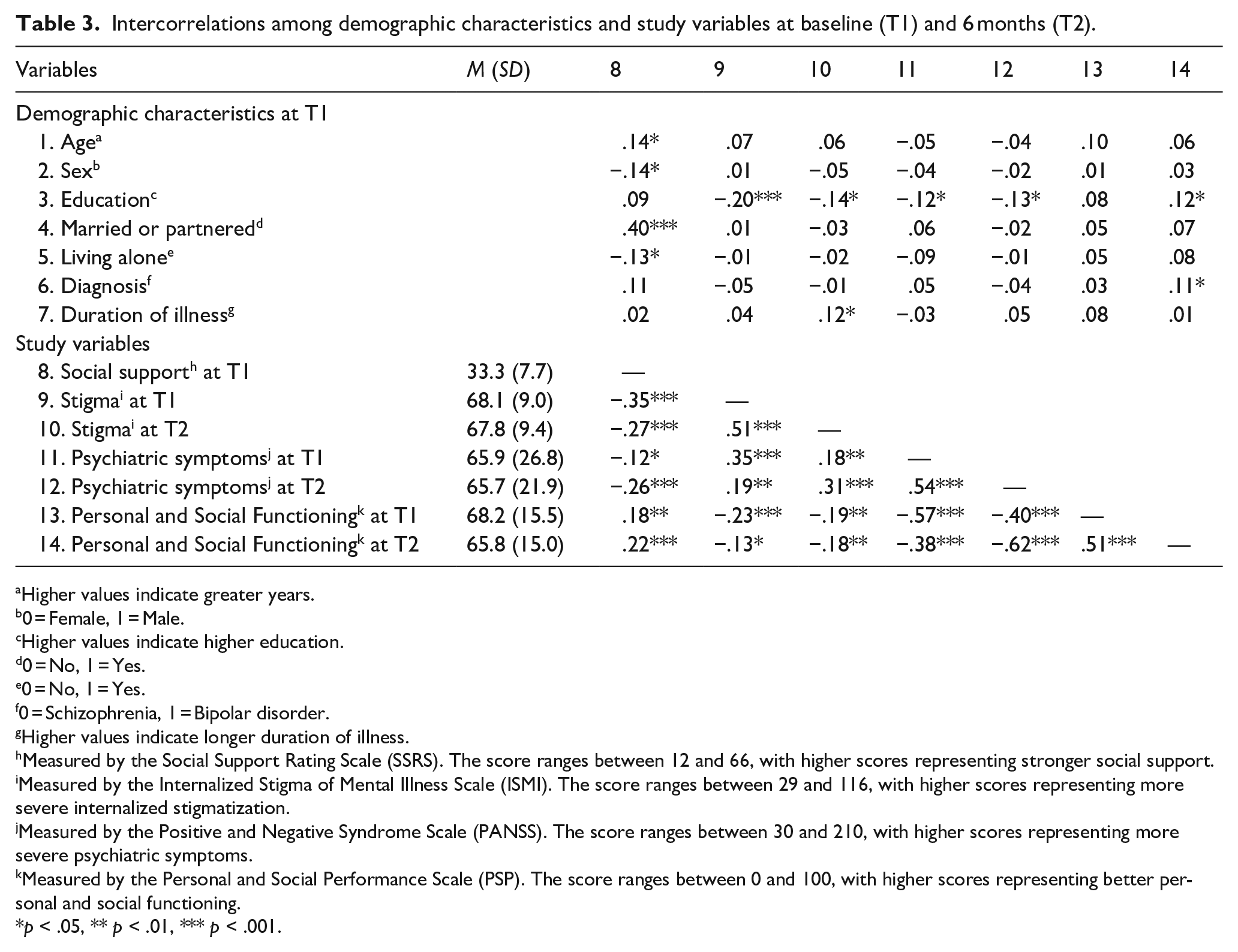
Correlations among demographic characteristics and the study variables, including social support, stigma, psychiatric symptoms, and personal and social functioning are shown in Table 3. Participants who were older (r = .14), female (r = −.14), married or partnered (r = .40), and not living alone (r = −.13) were more likely to have higher social support. Those with higher education were associated with lower stigma at baseline and 6 months (rs = −.20 to −.14), fewer psychiatric symptoms at baseline and 6 months (rs = −.13 to −.12), and better personal and social functioning at 6 months (r = .12). In addition, baseline social support was associated with lower stigma (rs = −.35 to −.27), less psychiatric symptoms (rs = −.26 to −.12), and higher personal and social functioning (rs = .18 to .22) at baseline and 6 months.
Intercorrelations among demographic characteristics and study variables at baseline (T1) and 6 months (T2).
Higher values indicate greater years.
0 = Female, 1 = Male.
Higher values indicate higher education.
0 = No, 1 = Yes.
0 = No, 1 = Yes.
0 = Schizophrenia, 1 = Bipolar disorder.
Higher values indicate longer duration of illness.
Measured by the Social Support Rating Scale (SSRS). The score ranges between 12 and 66, with higher scores representing stronger social support.
Measured by the Internalized Stigma of Mental Illness Scale (ISMI). The score ranges between 29 and 116, with higher scores representing more severe internalized stigmatization.
Measured by the Positive and Negative Syndrome Scale (PANSS). The score ranges between 30 and 210, with higher scores representing more severe psychiatric symptoms.
Measured by the Personal and Social Performance Scale (PSP). The score ranges between 0 and 100, with higher scores representing better personal and social functioning.
*p < .05, ** p < .01, *** p < .001.
Social support in prediction of stigma, psychiatric symptoms, and personal and social functioning over 6 months
As shown in Table 4, baseline social support significantly predicted lower stigma at 6 months (β = −.115, p = .029), while adjusting for baseline stigma and other relevant demographic covariates. The model accounted for 28.0% of the variance in 6-month stigma, and baseline social support explained 1.1% of the variance. There was no issue of multicollinearity (VIFs = 1.02–1.18).
Regression analyses of social support predicting stigma, psychiatric symptoms, and personal and social functioning at 6 months.
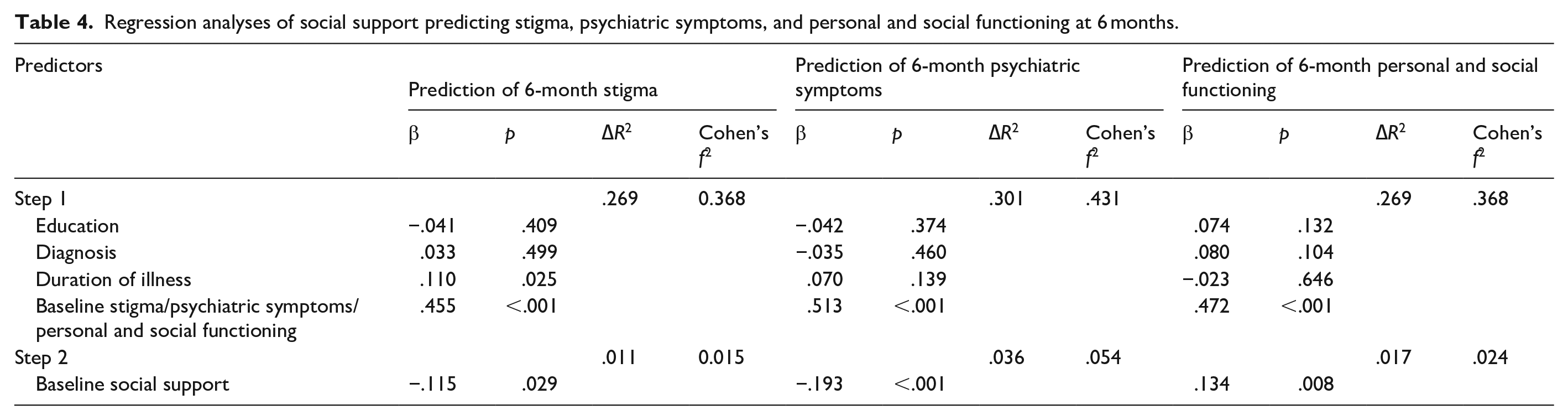
The effect of baseline social support on 6-month psychiatric symptoms was significant (β = −.193, p < .001), after adjusting for baseline values of psychiatric symptoms and other covariates. The model accounted for 33.7% of the variance in 6-month psychiatric symptoms, and baseline social support explained 3.6% of the variance. There was no issue of multicollinearity (VIFs = 1.02–1.04).
In prediction of 6-month personal and social functioning, the effect of baseline social support was significant (β = .134, p = .008), while adjusting for the baseline personal and social functioning and other covariates. The model accounted for 28.6% of the variance in 6-month personal and social functioning, and baseline social support explained 1.7% of the variance. There was no issue of multicollinearity (VIFs = 1.01–1.05).
Mediation effect of stigma on the associations of social support with psychiatric symptoms and personal and social functioning over 6 months
As shown in Figure 1(a), higher stigma (β = .169, p < .001) significantly predicted more severe psychiatric symptoms at 6 months when examined in the same model with baseline social support. The model was adjusted for baseline psychiatric symptoms and relevant demographic covariates. The relationship between baseline social support and 6-month psychiatric symptoms was partially mediated by 6-month stigma, as the direct path was reduced from β = −.193 to −.150 but still significant (p = .002) upon the addition of 6-month stigma into the model. Bootstrapping analyses demonstrated that the indirect effect was significantly different from zero (β = −.043, 95% CI [−0.074, −0.018]). The percentage of mediation was 22.3%.
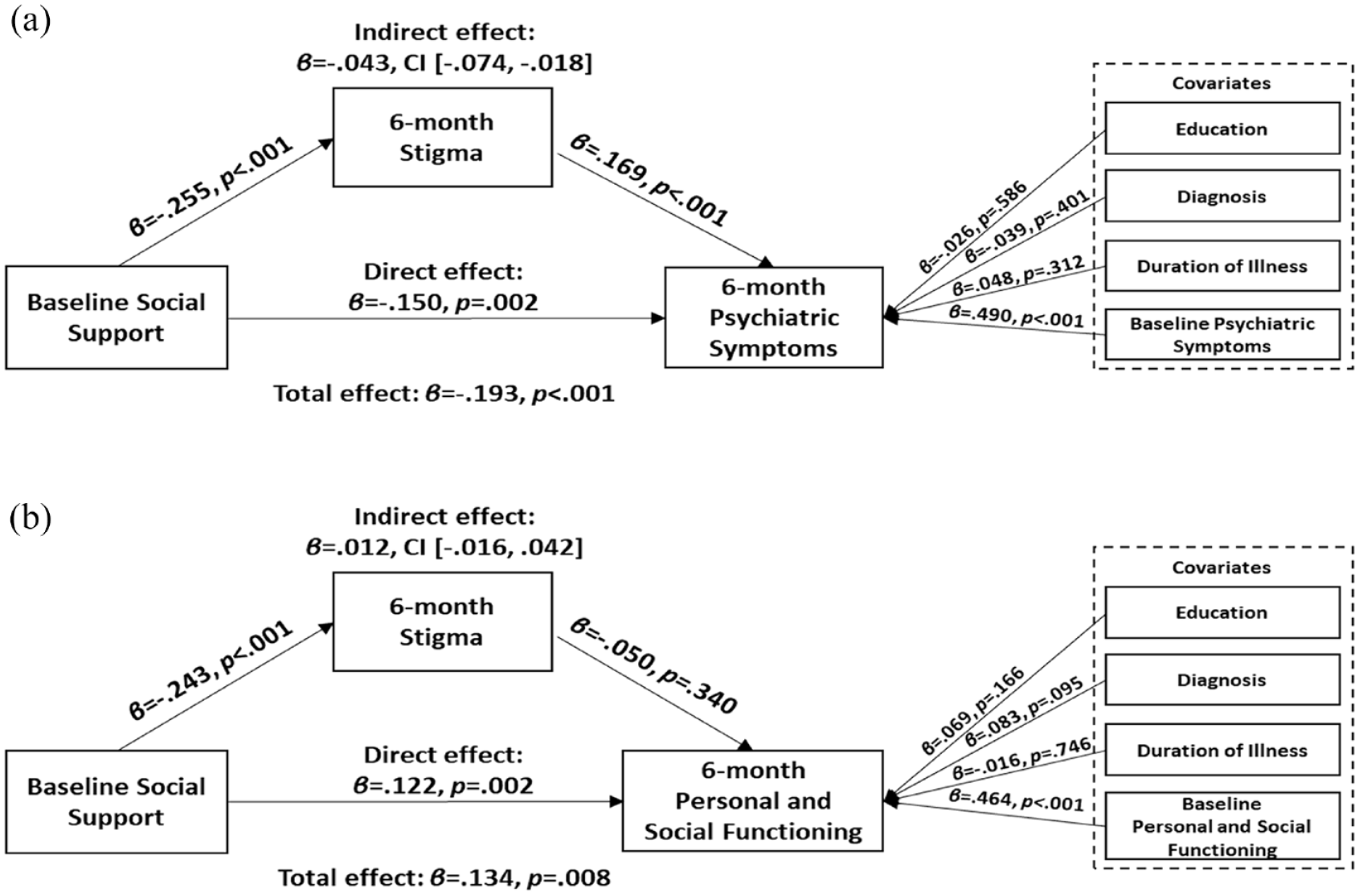
The coefficients of the mediation effect of stigma on the association of social support with psychiatric symptoms and personal and social functioning: (a) stigma at 6 months partially mediated the association of baseline social support with psychiatric symptoms at 6 months and (b) stigma at 6 months did not mediate the association of baseline social support with personal and social functioning at 6 months.
For prediction of personal and social functioning at 6 months (see Figure 1(b)), the effect of stigma was not significant (β = .050, p = .340) when included in the same model as baseline social support. Stigma at 6 months did not mediate the association between baseline social support and 6-month personal and social functioning, as the indirect effect of 6-month stigma was not significantly different from zero (β = .012, 95% CI [−0.016, 0.042]).
Mediation effect of stigma and psychiatric symptoms between social support and personal and social functioning over 6 months
As shown in Figure 2, more severe psychiatric symptoms (β = −.502, p < .001) were associated with worse personal and social functioning at 6 months when examined in the same model with baseline social support and 6-month stigma. The model was adjusted for baseline personal and social functioning and other covariates. Stigma and psychiatric symptoms at 6 months fully mediated the association between baseline social support and 6-month personal and social functioning (total indirect effect: β = .084, 95% CI [0.029, 0.143]). The direct path from baseline social support to 6-month personal and social functioning was reduced from β = .134 (p = .008) to β = .050 (p = .268). The percentage of mediation was 62.7%.
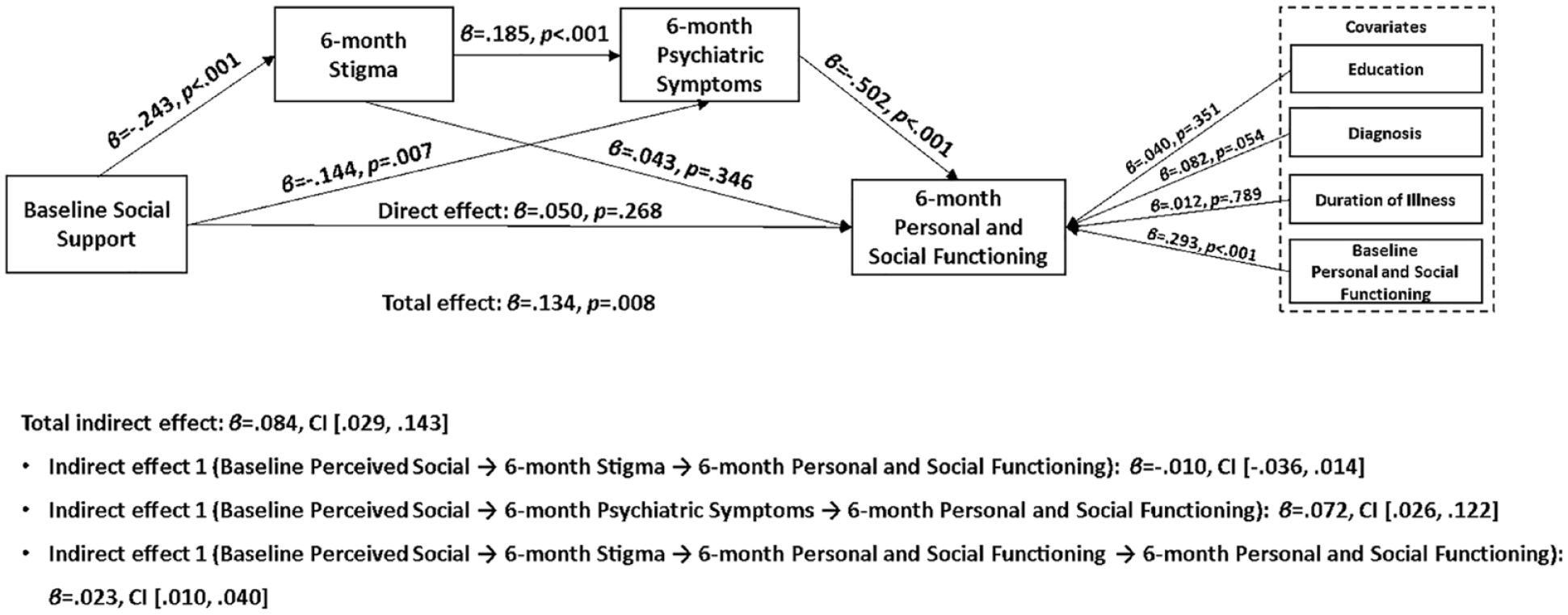
The coefficients of the mediation effect of stigma and psychiatric symptoms between social support and personal and social functioning.
Discussion
This longitudinal study investigated the associations of social support with self-stigma, psychiatric symptoms, and personal and social functioning over 6 months among people with SMI and provided a comprehensive understanding of whether and how self-stigma explains the associations of social support with long-term psychiatric symptoms and personal and social functioning. The results indicated that baseline social support predicted stigma, psychiatric symptoms, and personal and social functioning at 6 months, even after adjusting for the impact of their respective baseline values. In addition, stigma was found to partially mediate (22.3%) the relationship between social support and psychiatric symptoms over 6 months. However, stigma alone did not mediate the relationship between social support and personal and social functioning, while stigma and psychiatric symptoms together mediated (62.7%) the association.
Being consistent with prior studies (Dou et al., 2021; Goodsmith et al., 2023; Merritt et al., 2022; Velelekou et al., 2022; Weinstock & Miller, 2010), baseline social support was found to be a predictor of psychiatric symptoms and personal and social functioning at 6 months among persons with SMI. Several theories have highlighted the protective effect of social support on mental health promotion (Bedaso et al., 2021; Cobb, 1976; Harandi et al., 2017). Cobb explains that social support provides individuals the feeling of being loved, cared for, respected, and belonging to a network of communication, protecting individuals against stress and largely improving their social health and performance (Cobb, 1976). In addition, social support from family members and friends is salutary to reduce negative emotional experiences and develop a feeling of security. People with positive social connections and higher social support enjoy more efficient communication skills, directing them away from mental problems (Bedaso et al., 2021).
Prior studies have highlighted the importance of social support in the reduction of self-stigma in persons with newly onset mental illness (X. H. Li et al., 2021; Mueller et al., 2006). This study further confirmed this relationship among those with prolonged courses of mental illnesses. Compared with the findings from Western contexts (Bal et al., 2023; de Filippis et al., 2022), participants in this study reported slightly higher internalized stigma. This is aligned with existing evidence that mental health stigma may be particularly deeply rooted in Chinese culture even among SMI patients in their recovery stage (Lam et al., 2010). The process of internalized stigma begins with an awareness of the negative stereotypes about individuals who experience mental health problems and treatments from the public and surrounding people (Thornicroft et al., 2009). Support from close others (e.g. relatives, friends, or peers) may diminish SMI patients’ internalized public views, thus reducing their internalized stigma (Wang et al., 2022).
Moreover, the findings in this study innovatively revealed that self-stigma acted as a mediator between social support and psychiatric symptoms. Greater social support was able to decrease subsequent stigma and further improve psychiatric symptoms. However, self-stigma alone did not mediate the relationship between baseline social support and 6-month personal and social functioning. It is speculated that it might take a longer time for stigma to show its impact on personal and social functioning for people with SMI, as a prior prospective cohort study followed up patients with affective disorders over 12 months and found that self-stigma predicted changes in community living skill (Chien et al., 2015). Future studies may extend the follow-up period and re-evaluate the association between stigma and personal and social functioning. The chain mediation model indicated that stigma and psychiatric symptoms together mediated the relationship between initial social support and subsequent personal and social functioning, suggesting that the influence of stigma on psychiatric symptoms is more immediate than on personal and social functioning. The explanation is that the decrease in patients’ stigma may encourage them to engage in timely treatments and actively seek help from professionals, resulting in an instant recovery of illness symptoms (Thornicroft et al., 2009, 2016; Von Mach et al., 2022). The improvement in psychiatric symptoms further impedes the chronic impairment in social functioning and promotes social engagement (Owen et al., 2016).
The strengths of this study included a relatively sizable clinical sample, a longitudinal design with low attrition, a comprehensive measure of social support, and a clinical evaluation of psychiatric symptoms and personal and social functioning. In addition, the participants were recruited at the community level with stable mental illness conditions in the Chinese context, representing a generally under-studied population in clinical research. Given the sample size of this study, its power to detect a medium (Cohen’s f2 = 0.15) or large (f2 = 0.35) effect was excellent (>0.99), and the power to detect a small effect (f2 = 0.02) was at 0.70 at 6 months. It suggested that the significant findings were robust and their effects were noticeable.
In contrast, there were limitations of this study that should be heeded, which also suggested directions for future research. First, participants were followed up for only 6 months. It may need a longer time to observe the effect of self-stigma on personal and social functioning. Future studies are recommended to use a longitudinal design and follow-up participants for more than 12 months to re-evaluate the association between stigma and personal and social functioning. Second, this study was conducted during the COVID-19 period. Although the participants’ recruitment was not obviously affected by the restriction measures, social distancing restrictions due to COVID-19 pandemic might increase the lack of social connection and impact participants’ psychological conditions. More research should be conducted after the COVID period to verify the findings of this study. Third, the specific origins of social support were not assessed in this study. As support from family, friends, professionals, and others may play different roles in the impact of mental health outcomes, future research may specify the sources of social support and investigate their roles in mental health promotion. Fourth, as participants were voluntary to take part in the study, they could represent a group of SMI patients with good personal and social functioning. This self-selection bias in patient-focused research could be an issue affecting clinically oriented studies.
Conclusions
The findings of this study highlight how social support and self-stigma can play an important role in psychiatric symptoms and personal and social functioning among persons with SMI. Social support can be built into mental health rehabilitation programs as essential or required components (Ski et al., 2016) to facilitate long-term mental health outcomes. Moreover, strategies to reduce the internalized stigma of people with SMI, such as psychoeducational interventions and cognitive behavioral interventions (Diaz-Mandado & Perianez, 2021), are encouraged to be implemented to promote the disease prognosis in the long run.
Footnotes
Acknowledgements
The authors would like to thank all participants and investigators involved in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Capital’s Funds for Health Improvement and Research (Grant No. 2022-2-4113) and the Enhance Mental Health Community Service Capability by Promoting through Peer Support in China 2021 Program. The funders had no role in study design, data collection, data analysis, data interpretation, or writing of the report.