
Abstract
Background:
A substantial proportion of persons with psychosis (PWP) remain untreated in the community across the world. Factors that preclude them from accessing psychiatric treatment are poorly studied. In this study, we explored the factors that prevented persons with schizophrenia and their caregivers from accessing psychiatric treatment using an interview schedule specifically developed for this purpose.
Methods:
We identified individuals with schizophrenia and related disorders who had never accessed psychiatric treatment. We interviewed 67 such individuals and their family members using a validated tool, the Schedule of Factors Influencing Access to Treatment (SOFIAc) and analysed the data using descriptive statistics.
Results:
The M (SD) number of factors reported to preclude individuals with psychosis and families from seeking psychiatric treatment was 10 (3.32). No PWP/family reported any single factor as the sole reason for not accessing treatment. Distance to the nearest psychiatric centre (97%), PWP’s/family members’ knowledge and attitude towards symptoms of psychosis and treatment (92.5%), financial problems (91%), lack of insight and active resistance to efforts towards treatment (86.6%), lack of support from the family (83.6%) and family issues and dynamics (79.1%) were reported to be the commonest factors that precluded them from accessing psychiatric treatment.
Conclusions:
The reason for individuals with psychosis and their family members not accessing psychiatric treatment was invariably multifactorial, involving, on average, 10 factors. Programmes that target the reduction of the treatment gap should be cognizant of the multifactorial nature of the challenge of reaching psychiatric treatment for persons with psychoses.
Introduction
The treatment gap for psychiatric illnesses in general, and severe mental illnesses (SMI) in particular, is considerable (Gautham et al., 2020). In the absence of treatment, patients with SMI suffer substantial disability (Kohn et al., 2004), and families experience a substantial burden of care (Niu & Zhang, 2020). To improve access of persons with SMI to psychiatric care, it is critical to understand the factors that influence access to care. A few factors are well-known to be associated with poor access to care treatment. These include a lack of human resources (Eaton et al., 2011), poor awareness regarding the nature of the psychiatric condition and its treatment (Prince et al., 2007), the stigma associated with mental illness (Sharp et al., 2015), Perceptions of stigmatization by Others for Seeking psychological help and self-stigma associated with seeking psychological help like negative attitudes towards mental health treatment, or individuals’ own recognition of need for mental health care, to help further understand the low proportion of help-seekers for mental health problems.
Factors influencing treatment-seeking can vary across countries due to differences in healthcare services and socioeconomic and cultural factors (Sadock et al., 2017). Research on never-treated persons with schizophrenia has highlighted the role of poor awareness and tolerance of deviant behaviour by families and communities (Kurihara et al., 2005). Treatment-seeking for any health condition, specifically psychiatric conditions, is a complex phenomenon (Kane et al., 2022). It involves complex interactions of several factors. Using checklists and directive questioning are poorly suited to studying such a phenomenon. Our earlier work, which adopted in-depth interviews with participants who remained untreated in a rural community in South India and their family caregivers, identified 15 distinct factors that influence access to psychiatric care (K. S. Reddy et al., 2013). Based on this work, we developed the Schedule of Factors Influencing Access to Treatment (SOFIAc) to systematically assess the factors influencing access to psychiatric care among these individuals (K. S. Reddy et al., 2013). In our continued engagement with this community, we identified 83 individuals with psychotic disorders who had remained untreated. We interviewed them using the SOFIAc to assess the frequency of different factors that precluded them from accessing psychiatric treatment. In this paper, we describe the results of this work.
Methods
Study site
This study was conducted in a rural taluk (an administrative block), Turuvekere, in the Tumkur district of Karnataka. According to the 2011 national census, this taluk has a population of 1,68,994. Of them, 13,281 live in two towns, 4,236 in one suburban town and 1,56,780 in 243 villages (a total of 42,101 families in the taluk). Turuvekere taluk has one sub-divisional hospital in Turuvekere town and 11 Primary Health Centres distributed across the taluk. The community intervention programme involves the identification of persons with schizophrenia and related disorders irrespective of their current treatment status, treating them with pharmacotherapy and low-intensity psychosocial interventions (C. N. Kumar et al., 2017) and assertively following them up.
Sample
Individuals with features of psychosis were identified as part of a community intervention programme. The research team trained health assistants, doctors and nurses to use a validated tool, Symptoms in Others (Kapur & Isaac, 1978), to identify persons with psychotic disorders. Besides, doctors were trained in the management of patients with severe and common mental disorders. All potential cases were asked to be referred to the research team. Consultant psychiatrists made the diagnosis by interviewing PWP and their close relatives and by reviewing their medical records. The diagnosis was confirmed by using the Mini-International Neuropsychiatric Interview (Sheehan et al., 1998). We identified 222 PWP in total. About 42 of them were receiving treatment from psychiatrists; 97 of them had received treatment from psychiatric settings sometime in the past but were presently out of treatment; 83 had never visited a medical or psychiatric professional. Among the latter, 16 participated in the qualitative study to understand the factors associated with not accessing psychiatric treatment (S. K. Reddy et al., 2014). The other 67 formed the sample for this study. Of these, 10 had taken part in the study on the feasibility of administering the SOFIAc (K. S. Reddy et al., 2013).
Assessments
Mini-International Neuropsychiatric Interview (Sheehan et al., 1998): The MINI was used by qualified psychiatrists to confirm the diagnosis of schizophrenia (F20), schizoaffective disorders (F25) or unspecified non-organic psychosis (F29).
SOFIAc
Administration of the SOFIAc involves interviewing individuals who have never sought psychiatric treatment for their psychiatric condition and their family caregivers. The interview typically takes about 40 to 50 minutes and assesses 15 factors that could adversely influence treatment seeking in persons with schizophrenia or related disorders. Each factor is rated as having no (score of 0), some (score of 1), moderate (score of 2) or profound (score of 3) adverse influence on treatment seeking. Each factor assessed can have a distinctive influence on the individual’s final decision and/or his/her family; it may or may not interact with other factors.
Positive and Negative Syndrome Scale (Kay et al., 1987): The PANSS was used to assess the participants’ psychopathology during recruitment. The PANSS measurement is derived from behavioural information plus a four-phase 35- to 45-minute clinical interview. This is followed by 7-point ratings on 30 symptoms, for which each item and each level of symptom severity are defined. The ratings provide summary scores on a 7-item positive scale, a 7-item negative scale, a 16-item general psychopathology scale and a composite (positive minus negative) index.
Perceived Social Support Scale (Pillay, 2002): This 12-item questionnaire assesses perceived social support across three dimensions: emotional (showing concern, listening), informational (giving suggestions, advice and guidance) and instrumental (financial or physical aid). There are 4 items in each dimension, each rated on a Likert scale ranging from 1 to 5 (1 – available none of the time and 5 – available all the time). The total rating on all 12 items indicates the overall perceived availability of support.
Knowledge about Schizophrenia Interview (KASI; Barrowclough et al., 1987): This interview assesses what family caregivers know about schizophrenia and related disorders. The following aspects of schizophrenia are covered: diagnosis, symptomatology, aetiology, medication, course, prognosis and management. Each topic is covered in a different section. Most questions are structured, with choices of ‘yes/no/don’t know’; for each of the six sections of the KASI, the relative’s responses are allocated a score of 1 – negative, 2 – neutral, 3 – positive and 4 – positive and well-informed. Several studies have used this tool to assess the knowledge about schizophrenia (C. Reddy et al., 2021; Singh et al., 2016).
Indian Disability Evaluation and Assessment Scale (Grover et al., 2014; Mohan et al., 2005): This measures and qualifies disability in psychiatric conditions across four domains: self-care, interpersonal activities, communication and understanding and work. The score for each item included 0 – no disability, 1 – mild disability, 2 – moderate disability, 3 – severe disability and 4 – profound disability.
Burden Assessment Schedule: (Thara et al., 1998): It assesses both objective and subjective burden experienced by the primary caregivers of chronically mentally ill patients. It has 40 items rated on a 3-point scale, marked 1 to 3, with the responses being ‘not at all’, ‘to some extent’ or ‘very much’. The burden is assessed across 9 domains of caregiving.
The first author (KSR) administered these assessment tools (except for the MINI) to all participants and their caregivers. This paper focusses on the results of the SOFIAc. The study was approved by the ethics committee of the National Institute of Mental Health & Neurosciences (NIMHANS), Bengaluru. All participants and/or their family caregivers provided written informed consent to participate in this study.
Statistical analysis
Statistical Package for Social Sciences (SPSS version 16) was used to analyse the data. M (SD) was used to describe the continuous variables, and percentages were used to describe the categorical variables.
Results
Table 1 describes the sociodemographic and clinical details of the sample.
Describes the sociodemographic and clinical details of the sample.

M (SD).
N (%).
Average family education’ was calculated as the sum of the number of years of education of all family members divided by number of family members in the household.
The average age of PWP was about 43 years; nearly half were women. Just over half had at least primary education, while over a third had not received any formal education. Around half of the population was married, and just over a fifth of the sample was unmarried. A large majority (over nine-tenths) of the sample was earning below 2,000 rupees per month with minimal variation in religious diversity. Over one-half of the sample was unemployed, and a fifth was engaged in farming, followed by over a seventh of the sample being housewives. The average highest family education was around 9 years of formal schooling. Just under half of the sample had fewer than four members living in the household, over a fourth of the sample had four-member families and another fourth had five or more members in the family. A large part of the sample was represented by village dwellers, at just over nine-tenths.
Most PWP had moderate levels of positive symptoms (average PANSS positive score of 24.42) followed by negative symptoms (average PANSS negative score of 20.28). Most of the PWP had a severe disability in interpersonal communication followed by self-care. A majority of the PWP were either moderately ill (32.8%) or markedly ill (29.9%), as per the CGI severity. Caregivers’ knowledge about different dimensions of the illness was fairly low (M (SD) total score on KASI was 8.06 (1.9)). The overall total burden score of the M (SD) was 80.34 (11.3), suggesting a moderate level of burden of care. The perceived social support score was fairly low with M (SD) total PSSS score of 7.85 (2.01).
Table 2 describes the frequency of individual participants who acknowledged different factors as barriers to seeking psychiatric treatment. The most commonly acknowledged factors were distance to the nearest psychiatric centre (97%), individuals’/family members’ knowledge and attitude towards the symptoms of psychosis and treatment (92.5%) financial problems (91%), lack of insight and active resistance to efforts towards treatment (86.6%), lack of support from the family (83.6%) and family issues and dynamics (79.1%). These were followed by the community’s attitudes and beliefs about mental illness (70.2%) and its acceptance of changed behaviour and support for the person with mental illness (68.7%) and stigma (65.7%).
Frequency of individual participants who acknowledged different factors as barriers to seeking psychiatric treatment.
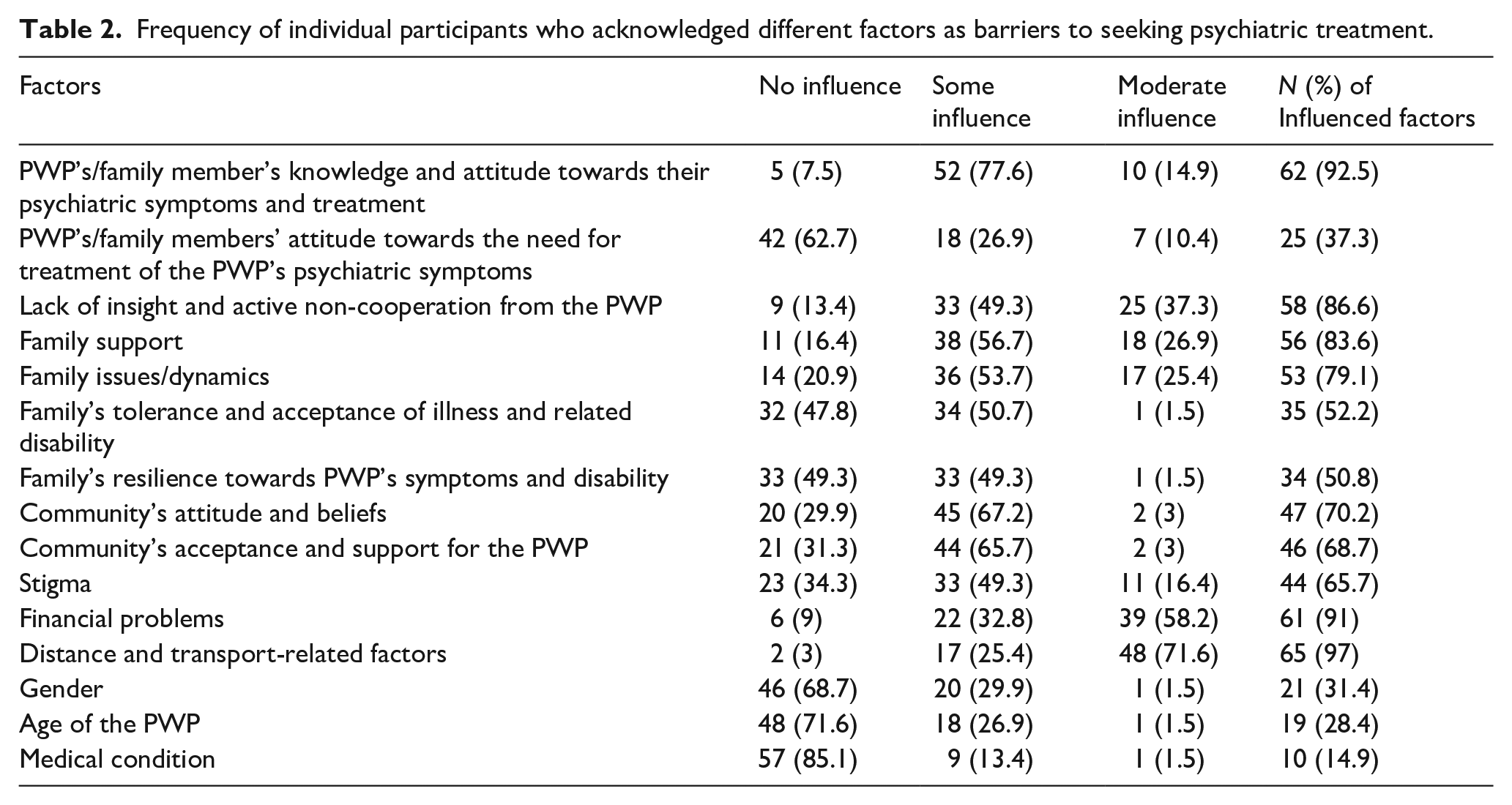
Table 3 describes the frequency and percentage of factors considered barriers to accessing psychiatric treatment. The M (SD) of a number of factors considered as barriers by each participant was 10 (3.32); the median was 10. The majority of the PWP and family members reported a minimum of seven factors that acted as a barrier to accessing psychiatric care; in 3.4% of the PWP, all fifteen factors acted as barriers to accessing psychiatric care.
Frequency and percentage of factors considered barriers to accessing psychiatric treatment.

Discussion
This study explored the factors associated with not accessing psychiatric care in a rural community in South India using a validated interview schedule. The place of the study is a remote rural area; the nearest psychiatric centre is about 70 km from the place, and at the time of conducting this study, only private psychiatrists were available there. However, many PWP and family members were unaware that these facilities were available. The other centres were >200 km away. The identified PWP were ill for a M (SD) of 96.49 (9.71) months, yet were not treated. As can be observed in Table 3, invariably, the factors that precluded PWP from seeking psychiatric treatment are multiple in all cases. It is not surprising, given that treatment-seeking, in general, is a complex phenomenon, as theorized by Sheeran (1996) and empirically observed elsewhere (H. K. Kumar et al., 2019; Omotoso, 2010) Clearly, efforts to improve access to treatment for persons with psychosis would necessarily have to be multi-pronged (Weaver et al., 2023) showed that making treatment accessible per se is unlikely to bridge the treatment gap for psychiatric conditions. For instance, a substantial proportion of PWP in a study by Padmavathi et al. (1998) remained untreated in the metropolitan city of Chennai, where treatment was readily available. It also follows that isolated attempts like improving awareness in the communities alone may not improve access to care. Our earlier publication on this population described the complex nature of the interaction across these factors (S. K. Reddy et al., 2014).
Distance to the nearest psychiatric centre was the most commonly acknowledged factor. This was followed by PWP’s/family members’ knowledge and attitude towards their symptoms and treatment, and financial problems Lack of insight coupled with active resistance to efforts towards treatment, family-related issues, the community’s attitudes and beliefs about mental illness and its acceptance of changed behaviour and support for the person with mental illness were the other important factors that influenced the PWP’s and families’ decision of not accessing psychiatric treatment. Stigma was mentioned as a barrier to seeking treatment by about two-thirds of the participants.
Several barriers to access to treatment can be overcome by making affordable psychiatric care available close to where PWP live. Such a move can potentially eliminate several factors, including distance and financial problems. Travelling to a distant psychiatric centre with a symptomatic and reluctant PWP adds additional stigma, which can be avoided if treatment is available close to where PWP live. Thus, making affordable psychiatric care available close by would also likely reduce the impact of stigma to that extent. The Government of Karnataka, a southern state in India, has been running a programme called the Manochaitanya, under which, multi-disciplinary mental health teams visit sub-district level places (Taluks) and provide mental healthcare free of cost. This has proven to be beneficial to a large number of service users (Agarwal et al., 2019; Manjunatha & Singh, 2016). Further, the importance of enhancing mental health literacy cannot be overemphasized (Mathur Gaiha et al., 2014). This potentially has the effect of changing the attitude of the families and the community itself. As was observed in this study, families’ and the community’s supportive attitude towards persons with SMI also acted as a barrier to treatment. The community should have a supportive attitude, but if the community can supplement this by encouraging individuals with SMI and their families to seek treatment, that would result in greater help to PWP and their families.
Interestingly, a report from Bali suggests that individuals with schizophrenia who do not show violent behaviour are less likely to receive treatment (Kurihara et al., 2005). Communities seem to ignore deviant behaviour as long as it does not lead to violence. As mental health literacy is inversely associated with stigma (Simoes de Almeida et al., 2023), enhancing mental health literacy among people could reduce the stigma associated with mental illnesses. For example, this can be done using school-based interventions – a recent systematic review has shown that such interventions improve mental health literacy as well as reduce stigma related to mental illnesses (Ganasen et al., 2008). Field has suggested several strategies that could help in the reduction of stigma, specifically in low-middle-income countries. These include increasing awareness among healthcare workers, traditional healers and the use of mass media, including the Internet. There is a need for more empirical research in this area.
This study has several strengths. Most importantly, we used a validated interview schedule, which comprehensively assesses factors that influence access to psychiatric care in persons with schizophrenia. We identified individuals with schizophrenia using a comprehensive case-finding methodology using key informants and healthcare workers who were familiar with local communities and were able to identify persons with symptoms of schizophrenia with minimal training. Participants were diagnosed by qualified psychiatrists using the MINI. It is important to note an important limitation of this study. The sample was drawn from a specific rural community in South India. It may be noted from the information in Table 1 that the sample came from a relatively impoverished and less educated, and lower socioeconomic background. Many of the factors identified in this research may be linked to this disadvantaged background. The generalizability of the findings to other regions and other socioeconomic backgrounds is questionable. Studies conducted across diverse regions of India may provide information that would be more useful for planning at a national level.
In conclusion, not seeking psychiatric treatment for psychosis is a complex, multifactorial challenge. Distance to treatment centres, knowledge and attitude of family and community members, financial problems, lack of insight and active resistance by the PWP are the commonest factors that preclude PWP from seeking treatment. Programmes that aim to reduce treatment gap for psychotic disorders should consider these aspects at the planning level itself.