
Abstract
Background:
Research has extensively documented inequalities in inpatient psychiatric care provided to people of minoritized ethnic groups. Nonetheless, the role of their previous engagement with community mental health care has been little studied.
Aims:
We aimed at exploring whether previous clinical care can influence key domains of subsequent psychiatric inpatient care for people of ethnic minorities.
Methods:
We identified patients with a first hospital admission between 2016 and 2022, from a representative, highly diverse, catchment area of Northern Italy, using electronic health data of the NOMIAC study. We aimed at testing the impact of clinical care prior to admission on indicators of poor inpatient care, as identified by a participatory expert panel, that is, compulsory admission, insufficient length of stay, administration of Long-Acting Antipsychotics (LAI) during the last 7 days before discharge. Multiple regression models, predicted and counterfactual proportions and path analyses from generalized structural equations modeling were used to explore the association between belonging to ethnic minorities and these indicators.
Results:
Among 1,524 participants, 18% were from minoritized ethnic groups. While these were more likely to experience an involuntary admission, regardless of previous care received, they were offered appropriate length of stay if had previous engagement with community mental health care. Both belonging to ethnic minorities and mental health care prior-to-admission were independently associated with early LAI administration.
Conclusions:
Several ethnic inequalities in inpatient care continue despite previous community mental health care provided. Future research should examine how these disparities translate into clinical outcomes. Nonetheless, there is the need to actively promote equity, improving the quality of inpatient care of minoritized ethnic groups.
Keywords
Introduction
Research has extensively documented inequalities in mental health care provided to people of minoritized ethnic groups compared with the native populations (Halvorsrud et al., 2018), showing negative and even coercive pathways through services, as experienced in particular by individuals with a psychotic disorder (Morgan et al., 2019). Indeed, black, Asian, minority ethnic, and migrant people have a greater risk of psychiatric detention, although there may be variations across different cultural groups (Barnett et al., 2019). In addition, inpatient care offered to minoritized ethnic groups seems associated with a number of unpleasant characteristics as well as with more frequent readmissions and use of physical restraint (Mohan et al., 2006; Priebe et al., 2009; Tarsitani et al., 2013), which altogether lead to a poor subjective experience of the hospital-stay journey (Pedersen et al., 2023). Several possible explanations have been hypothesized for these burdensome differences, including an increased perceived risk of violence, resulting in more police involvement, a poorer engagement with general practitioners compared with native subjects, and even some inherent ethnic disadvantages involving for example an increased prevalence of psychosis (Barnett et al., 2019; Halvorsrud et al., 2018). However, several of these accounts lack evidential support (Singh, 2019), add little to our understanding, and, albeit involuntarily, may support narratives of racial determinism. Among this kind of risk factors with a limited evidence base, despite its potentially modifiable nature, there is the role of detection, diagnosis, and referral for mental illness treatment for people from ethnic minorities in community settings, which, if not adequately provided, might lead to subsequent poor inpatient care (Barnett et al., 2019). Some research from the UK has shown that – relative to White British people – service users with psychosis from ethnic minorities are generally less likely to be offered evidence-based pharmacological and psychological treatment and are also less involved in their care planning (Das-Munshi et al., 2018). Some evidence from other European countries (Koopmans et al., 2013; Spinogatti et al., 2015) and the US (van der Ven et al., 2022), also shows substantial underutilization of mental health care services in general and especially prior to hospital admission. Nonetheless, the role for minoritized ethnic groups of earlier engagement with outpatient mental health care services on later inpatient care has been little studied so far. A large, retrospective cohort study, using data from the South London and Maudsley NHS Trust, has recently shown that the magnitude of the ethnic disparities in involuntary admission is not substantially explained by differences in clinical care prior to admission (Freitas et al., 2023). However, NHS organizational specificities in England, as well as cultural attitudes of the general population – and in particular of mental health care staff – toward people of minoritized ethnic groups, may be different as compared with other countries (Scheppers et al., 2006).
The aim of our exploratory study was thus to investigate, in a distinct cultural and organizational context, whether previous clinical care provided by any community mental health services can influence key elements of subsequent psychiatric inpatient care for people of ethnic minorities. In particular, we hypothesized that there would be differences in inpatient care as influenced by users’ ethnicity and that previous clinical care plays a role in fading potential inequalities.
The Northern Milan Area Cohort (NOMIAC) project provided an unmatched opportunity to do this, since it longitudinally investigated people from a defined catchment area admitted over a number of years for acute inpatient mental health care, while similarly collected data from the electronic health records of outpatient mental health services, assessing clinical care prior to the first admission. Therefore, this exploratory work hypothesized that people from ethnic minorities did not experience poorer inpatient care as compared with their native counterpart, if they had been previously offered community mental health care.
Methods
Setting and data sources
In this retrospective cohort study, we used data from the electronic health records of the Nord Milano Mental Health Care Trust. The study was approved by the local Ethics Committee as a part of the broader Northern Milan Area Cohort (NOMIAC) project (registration number: 672-17112020). Further active patient consent was not required, since we used regularly collected information, apart that from people who chose not to share their data for research purposes (less than 2%). We included individuals consecutively admitted for their first ever inpatient treatment to any of the two psychiatric intensive care units, accounting for a total of 27 beds. The Trust provides also community mental health care for the same 280,000 inhabitants of the northern area of the Metropolitan City of Milan, by means of four community mental health teams with multidisciplinary staff. The relevant catchment area comprises highly urbanized, both deprived and affluent, districts, whose proportion of people from minoritized ethnic groups, including second generation immigrants, ranges from 25% to 30% (ISTAT, 2023).
In addition, in one of the local boroughs it has been established a Red Cross regional hub for special hospitality of refugees and asylum seekers, whose 300 places are used for the legal assessments of adult guests. This process may take up to 12 months and can result in a court order of relocation across the Lombardy region either of involuntary repatriation. Provision of mental health care for this special population is provided by a dedicated outpatient clinic, based in the same Mental Health Care Trust, where interpreters and cultural mediators are available, along with health and social care clinical staff.
Sample
This study sample is a cohort of 1,524 people, who had the first hospital admission between January 2016 and December 2022, aged 16 years and over and with a personal or general practice address in the NOMIAC area at the time of admission. The definition of various ethnicities was based on national data from the Ministry of the Interior, that is, as stated in the electronic health records or as self-reported in the health card for temporarily present foreigners, to which are entitled also people who are illegally on National territory. We thus merged available data of people not from a white Italian background, assuming this as consistent with the purposes and the exploratory nature of our research, though this approach lacks the breadth and specificity of other ethnic classifications (e.g. UK ONS). The most prevalent ethnic groups were White Western Europe (82.2%), followed by White Eastern Europe (5.4%), South and Central America (4.4%), North Africa Arabs (4.1%), Asian (2.4%), and Black African (1.5%) people.
ICD-10 psychiatric diagnoses at the discharge included the following groups of disorders: schizophrenia spectrum (F20–F29: N = 498); affective psychosis (F30.2, F31.2, F31.5, F32.3, F33.3: N = 275); Mood [affective] disorders (F30–F39: N = 291); Disorders of adult personality and behavior (F60–F69: N = 207); Intellectual disabilities (F70–79: N = 22); Organic (F00–F09: N = 3); Anxiety, dissociative, stress-related, somatoform and other non-psychotic mental disorders (F40–F48: N = 228).
Measures
In order to identify characteristics of poor inpatient care, and following participatory research principles, we purposefully set up a panel whose members (N = 12) included three caregivers and three former users themselves of the psychiatric intensive care units, along with two psychiatrists, two mental health nurses, and two health workers from these clinical services: caregivers, users, nurses, and health workers were also from minoritized ethnic groups. Two trained research assistants, who had no clinical involvement with the group participants, used a three-round Delphi procedure (King et al., 2021; Jorm, 2015) in order to reach experts consensus about the domains which most contribute to a negative experience of hospital admission. The procedure progressed from an initial qualitative round, focusing on available evidence about factors determining poor inpatient psychiatric care, followed by two survey rounds for initial scoring and disagreement resolving by discussion.
First, the compulsory nature of the admission (i.e. inpatient admission against the will of the patient as recorded following National Mental Health Act) was considered as inevitably leading to poor inpatient care, since it is obviously perceived as the main element influencing users’ negative experience of the hospitalization (e.g. Längle et al., 2003). Secondly, despite the relevant literature was relatively limited (e.g. Babalola et al., 2014; Johnson et al., 2022), a reduced length of stay in hospital (i.e. days from admission to discharge) was deemed as an indicator of poor care. Supporting reasons involved a shared view that short admissions can offer only quick assessment, sedation and acute stabilization on the grounds of an immediate risk of suicide or violence (Allison et al., 2017), whilst an adequate inpatient trial of antipsychotics or antidepressant medications is at least 6 weeks, simply because of their pharmacodynamics (e.g. Sherwood et al., 2006). In addition, a short duration of hospital stay was considered an obstacle for appropriately benefiting from the non-specific treatment factors of inpatient psychiatric care in terms of structure (e.g. setting, staff, and resources) and processes (e.g. communication and interpersonal relations) (Schmidt & Uman, 2020). We thus considered a length of stay (LOS) in hospital shorter than mean LOS during the study period (cut-off point) as an additional marker of poor inpatient care. Finally, the early administration of Long-Acting Antipsychotics (LAI), which is often considered by users more coercive than oral formulations and as a means of control (Kane et al., 2021; Lindenmayer et al., 2020; Riboldi et al., 2022), was defined as LAI administration during the last 7 days before discharge from hospital and was considered an indicator of poor inpatient care. This was deemed as particularly meaningful because we examined the first ever admission to psychiatric intensive care units. Information on compulsory hospital admissions, LOS, and LAI treatment were collected from electronic health records.
As for the exposure of interest, we explored any kind of mental health care from community services received during the 12 months prior to admission, which made these subjects officially included into the outpatient services caseload: data were thus extracted from the electronic community health records of the Nord Milano Mental Health Care Trust and linked with hospital records.
Data analysis
Standard statistics were estimated for both categorical and continuous variables for descriptive purposes. Potential differences between minority ethnic and native subgroups were evaluated by comparing sample characteristics, using parametric and non-parametric tests.
According to the study objectives, there was the need to (a) better understand potential differences in various inpatient care indicators based on ethnicity; (b) investigate whether prior community mental health care may mitigate any disparities observed for subsequent inpatient care experiences. Therefore, a two-step approach was followed to fit the data, capturing the multiple pathways involved.
First, in order to explore the association between belonging to ethnic minorities (independent variable) and binary indicators of poor inpatient care (dependent variables), we modeled the likelihood of being in a class of individuals experiencing poorer care as a log-odds function of ethnic minority status. In particular, three logistic regression models were separately built (i.e. for compulsory admission; LOS; early LAI administration), assessing in multiple regression models the joint contribution of both belonging to ethnic minorities groups and mental health care received from community services prior-to-admission (since it might influence the relationship studied), on characteristics of inpatient care. Hypothesizing that part of the total effect on poor inpatient care could be explained by differences in previous mental health care received, we decomposed the total effects, estimating predicted and counterfactual proportions across the native and ethnic minorities subgroups (Buis, 2010). This allowed us to distinguish the relative contribution of ethnicity, assuming equal previous community care in both groups.
However, to handle the theoretical framework complexity based on the different considered pathways, a simultaneous estimation of multiple equations was needed. Then, in order to consider all relevant relationships simultaneously, an overall model based on path analyses was carried out by using generalized structural equations modeling. Given the low proportion of missing data (less than 1%), maximum likelihood estimation was used to provide unbiased estimates, thus handling missing data under the missing-at-random assumption.
Model assumptions were carefully verified, including independence of observations according to the nature of the study design, and the log-linearity for the combination of the explanatory variables. In particular, we used link tests for model specification and Box-Tidwell regressions for model fit based on maximal likelihood estimate. Where appropriate, diagnostic measures were computed for multicollinearity (e.g. tolerance and the variance inflation factor). To balance model simplicity and explanatory power in relevant comparisons, we performed goodness-of-fit tests using the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and pseudo R-squared values. This approach allowed us to select relevant variables while leveraging existing evidence.
Odds ratio (OR) estimates were provided. Statistical significance level was set at .05.
The analyses were undertaken using Stata (StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC).
Results
Sample characteristics
The sample involved 1,524 participants at their first hospital admission (see Figure 1 for a flow diagram), of whom 271 (17.8%) were from minoritized ethnic groups. Table 1 shows socio-demographic and clinical characteristics of the sample, also stratified by ethnicity. Participants’ mean age (SD) at time of first admission was 41 (14) years and 48% of them were women. As compared to their native counterpart, participants from ethnic minorities were more likely to be women (n = 153, 56.5%) and younger, with a mean (SD) age of 33.6 (11.7) years, mostly admitted in their early 20s. The most frequent diagnoses in the sample were schizophrenia spectrum disorder (33%), mood (19%), and affective psychotic (18%) disorders. No diagnostic category was more frequent among people admitted from minoritized ethnic groups as compared with native people.
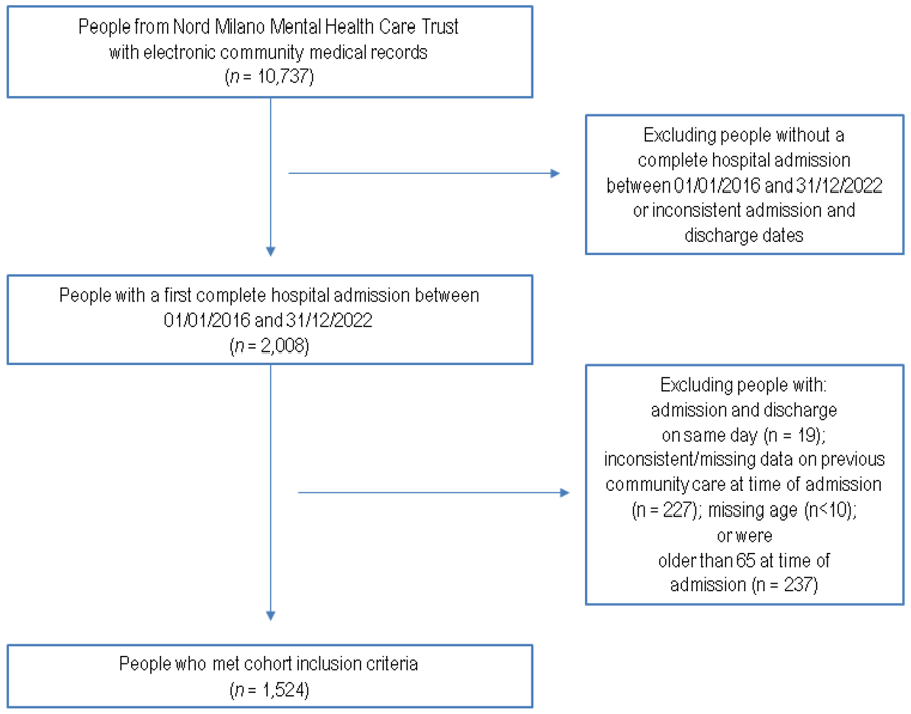
NOMIAC Cohort flow chart.
Sample characteristics of people at first hospitalization: overall and by ethnicity.
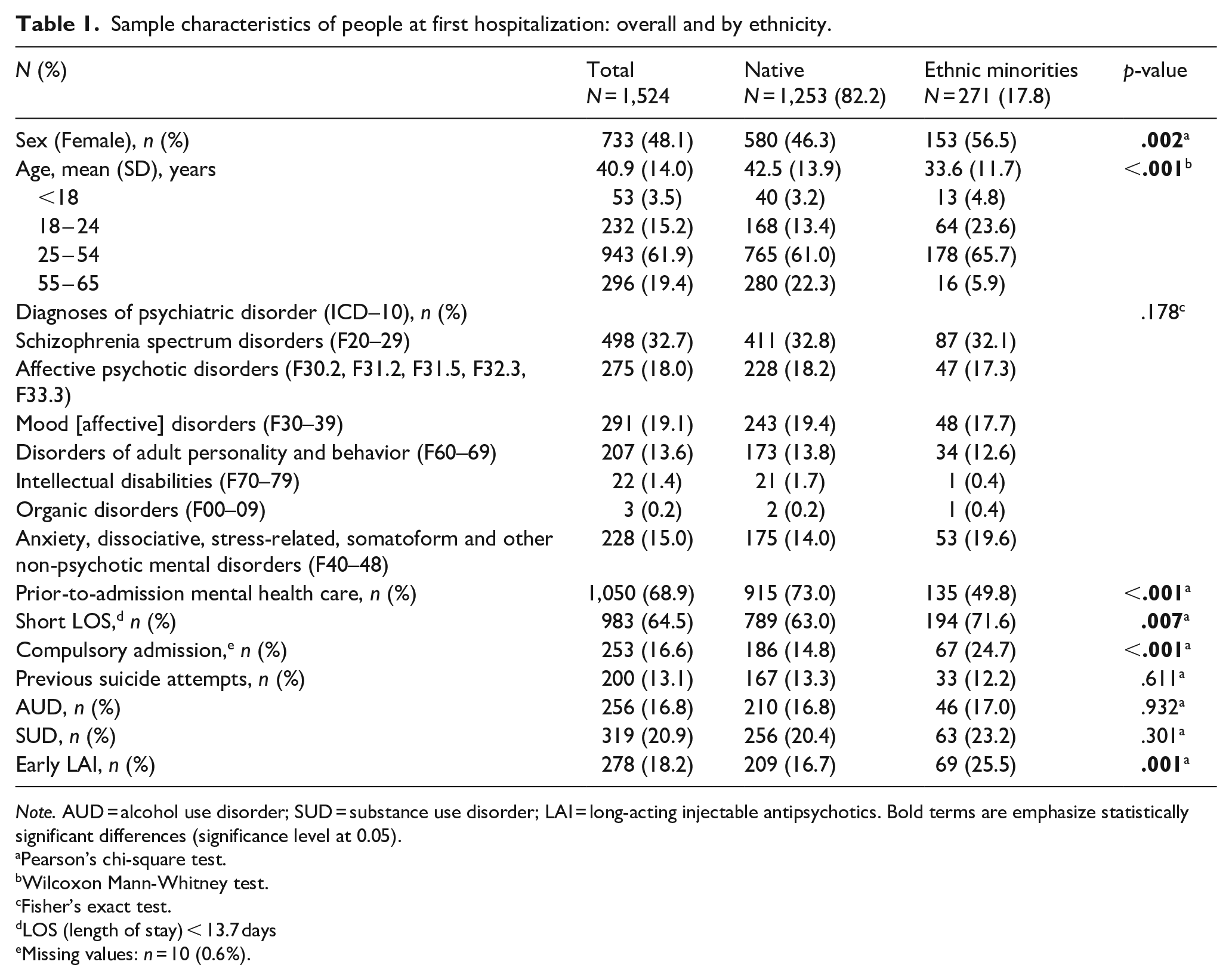
Note. AUD = alcohol use disorder; SUD = substance use disorder; LAI = long-acting injectable antipsychotics. Bold terms are emphasize statistically significant differences (significance level at 0.05).
Pearson’s chi-square test.
Wilcoxon Mann-Whitney test.
Fisher’s exact test.
LOS (length of stay) < 13.7 days
Missing values: n = 10 (0.6%).
In the 12 months prior to admission, 69% (n = 1,050) of people from the overall sample received mental health care from community services, though only 50% (n = 135) considering those from ethnic minorities. About a quarter of the first hospital admissions were of a compulsory nature (23%) or characterized by the early administration of LAI (25%): both were significantly more frequent among people from ethnic minorities (p = .002 and p = .001, respectively).
Moreover, about 64% of hospitalizations had a LOS shorter than the average (SD) from the overall sample. That is, 13.7 (12.9) days; potential observations lying an abnormal distance (i.e. LOS > 90 days) were excluded, as likely to be due to extra-clinical reasons (e.g. homelessness and rough sleeping). Statistically significant subgroup differences were found, with people from ethnic minorities more frequently reporting a LOS shorter than the average as compared to their native counterpart (72% vs. 63%, p = .007).
Ethnic minorities and poor inpatient care
Based on predicted and counterfactual proportions, participants from minoritized ethnic groups reporting compulsory admissions would have decreased from 24.8% to 15.7% if they had the same conditional probabilities as those from the native subgroup (i.e. same prior-to-admission mental health care as their native counterpart). Indeed, minoritized ethnic groups were more likely to experience compulsory admissions (Model 1, unadjusted OR: 1.88, 95% CI 1.37; 2.58, p < .001): also including prior-to-admission mental health care the logistic regression adjusted model showed that a 0.60 increase in the log-odds of compulsory admission in subjects from ethnic minorities was detectable as compared to their native counterpart (Table 2).
Ethnic minorities, poor inpatient care and role of prior-to-admission mental health care: logistic regression models.
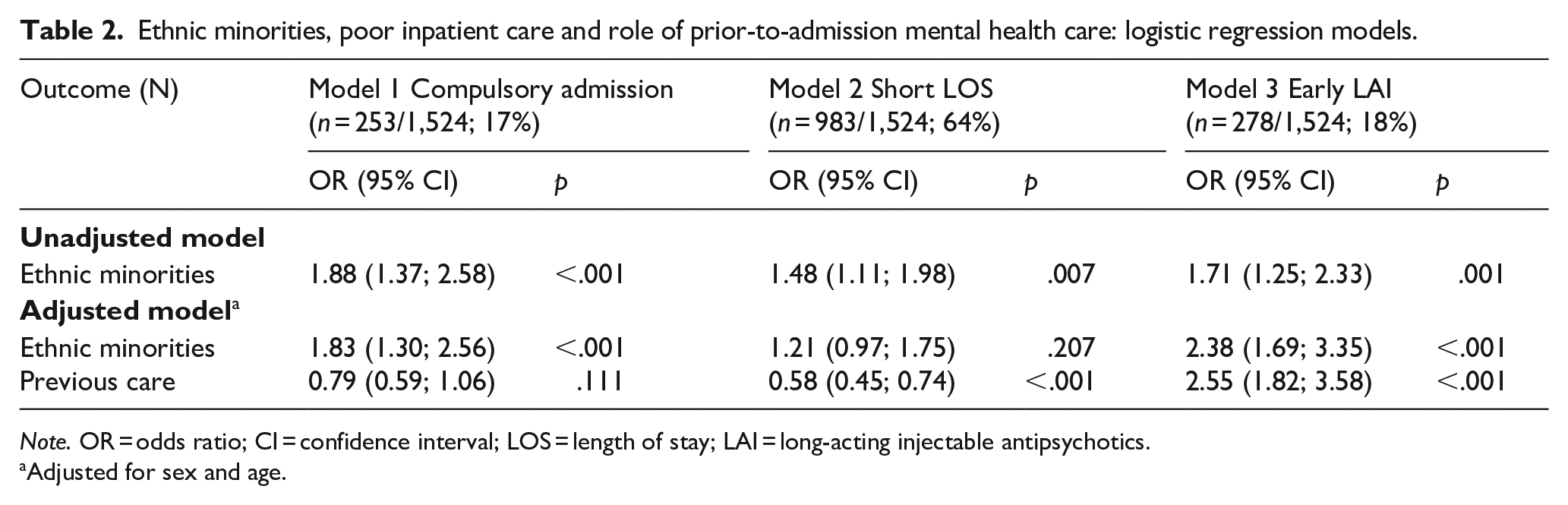
Note. OR = odds ratio; CI = confidence interval; LOS = length of stay; LAI = long-acting injectable antipsychotics.
Adjusted for sex and age.
Although we found a higher likelihood for short LOS among participants from ethnic minorities (Model 2, unadjusted OR: 1.48, 95% CI 1.11; 1.98, p = .007), the related estimate was not statistically significant any longer when considering also prior-to-admission mental health care (with predicted and counterfactual proportions equal to 71.6% and 66%, respectively). Indeed, holding ethnicity constant, those reporting prior-to-admission mental health care were more likely to have a longer LOS (Model 2, adjusted OR: 0.58, 95% CI 0.45; 0.74, p < .001).
Moreover, ethnic minorities were more likely to report early LAI administration during the last 7 days before discharge (Model 3, unadjusted OR: 1.71, 95% CI 1.25; 2.33, p = .001). Nonetheless, multiple regression models uncovered mixed results for the joint contribution of ethnicity and prior-to-admission mental health care, both showing associations with early LAI administration (Model 3, adjusted OR, 95% CI, p-value: 2.38, 1.69; 3.35, p < .001; 2.55, 1.82; 3.58, p < .001, respectively). Predicted (25.5% and 21.5%) and counterfactual (14.1% and 9.7%) proportions for early LAI administration were consistently estimated among both ethnic minorities (conditional probabilities related to same prior-to-admission care as the native counterpart) and participants with prior-to-admission care (conditional probabilities related to same ethnic background as their counterpart without prior-to-admission care). No multicollinearity issues were detected.
Finally, simultaneously testing all relevant paths (Figure 2), analyses corroborated previous results, showing an increase in the log-odds for both compulsory admission (coeff.: .60, 95% CI 0.27; 0.94, p < .001) and early LAI administration (coeff.: .87, 95% CI 0.52; 1.21, p < .001) in people from ethnic minorities, as compared to the native subgroup, with minoritized ethnic groups less likely to report prior-to-admission mental health care (OR: 0.44, 95% CI 0.33; 0.58, p < .001).
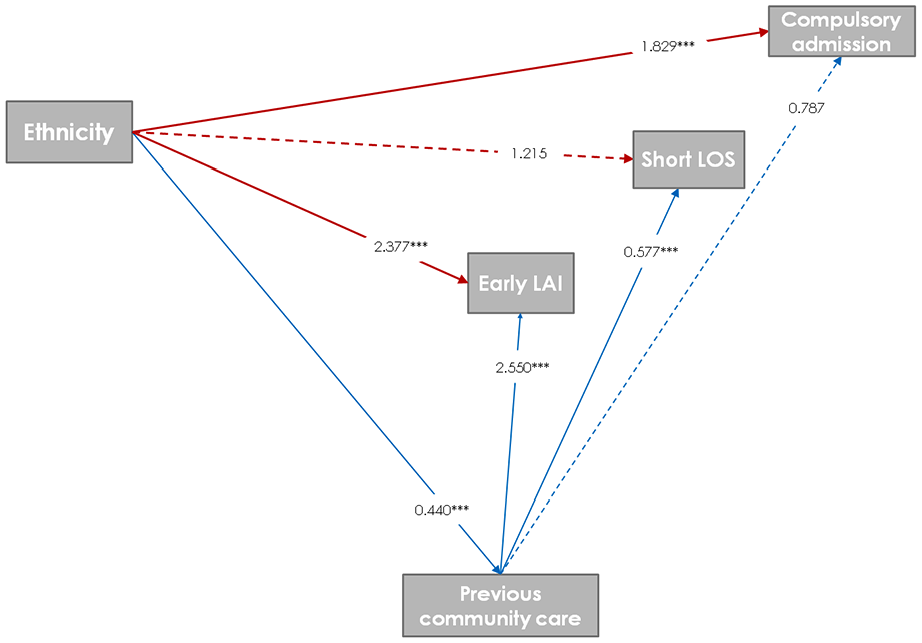
Path analyses for the associations (ORs) between ethnicity and indicators of poor inpatient care (red lines) with prior-to-admission mental health care as observed covariate and adjusted for sex and age.
Discussion
Main findings
We explored ethnic differences on a number of indicators of poor inpatient care, in a cohort of people aged 16 years and over, with a first hospital admission across 7 years. They were from a representative, highly diverse catchment area of Northern Italy and we focused on the role of prior contacts with community mental health services (Ruggeri et al., 2008).
Although in the 12 months prior to admission over two thirds of subjects from the entire sample received some kind of mental health care from community services, this was true for only half of those from ethnic minorities. About a quarter of the admissions were of a compulsory nature or ended up with an early LAI administration: both these characteristics were significantly more frequent among people from ethnic minorities. Looking at the role of prior contacts with community mental health services on compulsory admissions, people from minoritized ethnic groups were more likely to experience an involuntary hospital stay, regardless of previous care received, whose influence remained limited. However, as far as for short, insufficient, length of stay in hospital, despite participants from ethnic minorities seemed to experience that more frequently, this was not true any longer when considering also prior-to-admission mental health care. In other words, native participants were equally likely to experience this characteristic of poor inpatient care, if they had no previous engagement with community services.
Regarding early LAI during first ever admission, the picture is somehow more complex, since both belonging to ethnic minorities groups and mental health care received prior-to-admission were independently associated with LAI administration in the last 7 days before discharge from hospital. Finally, when simultaneously exploring the relative contributions of both ethnicity and prior contacts with community mental health services on all indicators of poor inpatient care, generalized structural equations modeling confirmed the role of ethnicity on both compulsory admission and early LAI administration.
Ethnicity, prior-to-admission mental health care and compulsory admissions
Overall, this study confirms the burden in terms of ethnic inequalities for compulsory admission, consistently with the latest meta-analytic evidence (Barnett et al., 2019). However, the results did not support our original hypothesis, since we did not uncover any protective role of previous care received from community mental health services as regards subsequent compulsory admissions. This is consistent with similar, recent UK research (Freitas et al., 2023), though not with other evidence from North America (Rodrigues et al., 2019). Nonetheless, there may be explanations of this finding. Reasons why community mental health care is offered certainly include perception of risk as detected by local social and health care agencies. This perception is also strongly associated to increased odds of compulsory admission (Walker et al., 2019). However, mental health legislative framework in Italy prescribes unusually stringent criteria for compulsory admission, which do not include risk as a justification, probably leading to the lowest rate of involuntary hospitalization (14.5 per 100,000 individuals) among Western countries (Sheridan Rains et al., 2019). However, regardless of formal mental health care previously received, people of minoritized ethnic groups still have higher odds of compulsory admission, as if risk assessment were a relevant, substantial criterion for these special populations. A distinct and culturally sensitive approach, alternative to standard clinical care, is clearly needed for assessing and managing mental health crisis of minoritized ethnic groups in the community: hopefully this might decrease the odds of compulsory admission also for non-native people in our National context (Carrà et al., 2022; Johnson et al., 2022).
Ethnicity and influence of prior-to-admission mental health care on short LOS and early LAI
There are certainly different views about LOS as an indicator of quality of psychiatric inpatient care and this is likely to be associated with peculiarities of the various mental health care delivery systems in terms of outpatient and inpatient services, staff resources and acute bed space availability (Bruce & Smith, 2020). Longer lengths of psychiatric inpatient stay in systems where the pressure on acute bed resources is relatively low and National legislations on compulsory admission and involuntary treatment allow extensive lengths of placement, are reasonably considered indicators of poor inpatient care. For example, recent research from the UK, along with other sociodemographic and clinical correlates, found an association between belonging to ethnic minorities and longer LOS, deemed as disproportionate and clinically unjustified (Bruce & Smith, 2020; Newman et al., 2018). However, in our setting in which reductions in bed capacity – 8.0 psychiatric care beds per 100,000 inhabitants nationwide in 2023 (EUROSTAT, 2023) – drive pressure on early discharge leading to shorter LOS, this should inevitably be considered an indicator of poor inpatient care. Within this framework, the finding of our study that those people from ethnic minorities who had some previous contact with community mental health care did not experience shorter LOS, clearly shows the importance of earlier engagement with local mental health care facilities, in order to offer equitable and fair inpatient care also to these special populations.
As for early-LAI administration in the last 7 days before discharge from hospital, findings from our study are less straightforward as both having previous contacts with community mental health services and being of an ethnic minority background, separately increased the odds of early LAIs. It is likely that two different paths are in place to explain this finding. Prior-to-admission mental health care probably provides clinical information about poor adherence for oral formulations, suggesting a safer LAI prescription, even though it is proposed at the end of the first ever admission (Bartoli et al., 2022). However, our study shows also distinct ethnic disparities in disproportionate LAI prescription, replicating an established bulk of evidence (Aggarwal et al., 2012; Li et al., 2023; Wang et al., 2023). Thus, other factors relating to poor adherence with medications and contributing to ethnic inequalities in prescribing LAI are likely to be in place. Along with patients’ views and preferences, possibly influenced by socioeconomic and living conditions as well as by cultural and linguistic barriers (Wang et al., 2023), implicit ethnic bias from providers in terms of risk perception at discharge could be again a possible driver contributing to ethnic disparities in LAI prescriptions (Hall et al., 2015). In other words, there might be a misleading discernment among mental health care staff, assuming that people from ethnic minorities are less willing to adhere to oral medication and more prone to risky behaviors, than their native counterparts (Das-Munshi et al., 2018). This bias, coupled with clinicians’ legal liability in terms of preventing patients from engaging in self-harm or exhibiting harmful behaviors toward others (Morena et al., 2023; Terranova & Rocca, 2016), are likely to play a key role at least for recent refugees and asylum seekers, whose legal status and residential instability are often complex and poorly managed by other statutory agencies.
Ethnicity, prior-to-admission mental health care and overall poor inpatient care
Assessing the quality of inpatient care remains a challenge, in particular because some of the proxy measures of poor care we chose are likely to be mutually interdependent. Thus, the finding from our structural equations modeling, assessing the joint contributions of ethnicity and previous community mental health care simultaneously on all available indicators are particularly meaningful, because it confirms how being from an ethnic minority increases the likelihood of both compulsory admission and early LAI administration. It may be useful for service providers to reflect on this increased vulnerability, turning into disadvantage in terms of care, system, and discrimination-based variables (Bruce & Smith, 2020).
Limitations and strengths
This study makes use of a large cohort to assess ethnic group differences in first ever inpatient care. In addition, good quality electronic health record data were from a large, diverse catchment area, representative in terms of different ethnic minorities across Italy.
Nevertheless, a number of limitations should be acknowledged. First, available classification of ethnicities lacked the specificity of other studies from countries where more detailed data are routinely accessible. The rough, though inevitable, merging might have obscured variations across different cultural groups. Similarly, we had no measure available on socioeconomic status as well as on area-level deprivation, despite its established influence on a number of features such as compulsory admission. Furthermore, we used indirect measures of quality of inpatient care. This is a major, ongoing, gap in the research literature: despite its ubiquity in mental health care systems, there has been surprisingly little definition or discussion on the characteristics, design and quality of acute care in mental health wards (Johnson et al., 2022). Finally, another limitation of this study includes its generalizability to other countries, where differences in legislations and acts for compulsory admission and criteria for involuntary treatment of mentally ill people are likely to be major – though external – drivers of inpatient psychiatric care characteristics (Salize et al., 2002).
Conclusion
The current study corroborates previous research about ethnic inequalities as regards a number of indicators of poor inpatient care. However, some of these may be mitigated by prior-to-admission mental health care. Future research should examine how these disparities in use translate into clinical outcomes. Meanwhile, our findings emphasize the ethical public health imperative to actively promote equity (Dykxhoorn & Kirkbride, 2018), developing appropriate interventions which can overcome cultural and organizational barriers, in order to facilitate early access to community mental health care for people of minoritized ethnic groups: this is likely to improve, whenever necessary, also their experience of inpatient care.
Footnotes
Acknowledgements
We thank Elisabetta Mascazzini M.D., for her passionate contribution running the refugees and asylum seekers outpatient clinic and Matteo Berlanda for support with electronic community medical health records.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
The datasets supporting the conclusions of this article are not available as the original source has not granted permission to share that information.