
Abstract
Background:
Mental health problems are high among refugees due to their traumatic experiences of fleeing war and witnessing disasters and deaths due to violence and conflict. Refugees are exposed to various socio-cultural stressors during their migration journey before, during, and after arriving at the host country, which may increase their risk of mental health problems. Strength-based interventions may be beneficial to address their socio-cultural and psychological stressors by strengthening individual’s strengths to address their problems.
Aims:
This study evaluated the effect of a Social and Emotional Wellbeing intervention on mental health (stress, anxiety, and depression) and emotional health outcomes (coping, self-efficacy, social support, and conflict resolution) among Ukrainian refugees in Massachusetts.
Methods:
We implemented intervention (once-weekly/5-week) among 31 Ukrainian refugees with pre-and post-assessment of mental and emotional health outcomes (2022–2023). The intervention consisted 5-module: managing stress and mind-body exercise, strengthening communication and social networking, problem-solving, and creating a healthy family environment. Validated scales were used to measure mental and emotional health outcomes, such as the Hopkins-Symptom-Checklist-25 for anxiety and depression and the Cohen-Perceived-Stress scale for stress. Paired t-test was used for data analysis.
Results:
The pre versus post-intervention proportion reduced for anxiety (61.29% vs. 22.58%) and depression (58.06% vs. 22.58%). The mean scores significantly decreased from pre- to post-intervention by 6.26 points for stress, by 7.07 points for anxiety, and by 6.29 points for depression (both p’s < .01). The mean scores significantly increased for coping (by 15.71), emotion-focused engagement (4.48), problem-focused engagement (4.80), social support (8.77), problem-focused coping self-efficacy (14.93), stop unpleasant emotions and thoughts (12.74), and friends networking (3.48; all p’s < .01).
Conclusions:
The stress, anxiety, and depression were reduced, and coping, self-efficacy, and social support networking skills were improved among Ukrainians after intervention. This program should be replicated in the larger community for a wider benefit.
Introduction
Refugees bear the highest burden of mental health problems due to their traumatic experiences of fleeing war and witnessing separation, disaster, and deaths due to violence and conflict (Bogic et al., 2015; Coventry et al., 2020; Kaufman et al., 2022; Scoglio & Salhi, 2021). During their migration journey, refugees were exposed to various sociocultural stressors before (fear of persecution, family member loss, or disruption of social structure and support), during (long arduous journeys, hunger, deprivation, being abused, or uncertainty), and after arriving to the host country (economic hardship, legal uncertainties, language difficulties, social isolation, racism, or family conflicts; Hodes, 2023; Kirmayer et al., 2011) which may increase their risk of psychological distress and mental health problems. The prevalence rate for depression (44% vs. 20%) and anxiety (40% vs. 21%) was higher for refugees than for labor migrants, according to the systematic review and meta-analysis study including 37 publications (Lindert et al., 2009). Another systematic review based on clinical interviews also highlighted the high prevalence of depressive disorders (31.5%), anxiety disorders (11.1%), post-traumatic stress disorder (31.5%), and psychoses (1.5%) among refugees than those in the general population (Blackmore et al., 2020).
Worldwide, the number of displaced persons has been increasing due to persecution, violence, and conflicts. In 2021, approximately 89.3 million people were displaced forcibly, compared to 42.7 million in 2012, according to the UN Refugee Agency (United Nations High Commissioner for Refugees, n.d.-a). Recently, Ukrainian refugees (over 6 million) have been one of the largest groups of refugees who have fled their country due to the Russian-Ukrainian war since February 24, 2022 (United Nations High Commissioner for Refugees, n.d.-b). After the first year of the Russian invasion, a nationwide cross-sectional study among 3,173 Ukrainians, including refugees abroad, internally displaced persons, and not displaced persons, reported that the prevalence of high stress, severe anxiety, and high levels of post-traumatic stress disorder was higher for Ukrainian refugees (25.2% vs. 21.6% vs. 15.5%) as compared to the displaced persons (25.8% vs. 23.4% vs. 19.0%), and not displaced Ukrainians (47.2% vs. 39.4% vs. 32.9%; Lushchak et al., 2024). A study among Ukrainian refugees resettled in Germany also reported the high prevalence of mental health burden (anxiety: 51%, distress: 23%, severe distress: 41%; Buchcik et al., 2023). This data suggests that mental health problem is a serious concern among Ukrainian refugees.
In the United States, >271,000 Ukrainian refugees have been resettled through various immigration channels (Ainsley, 2023). Addressing refugees’ psychosocial, emotional, and mental health needs has become the norm of humanitarian response (Jones & Ventevogel, 2021). Mental health promotion intervention and social support activities should be a priority to address their socio-cultural stressors to prevent or reduce the mental health burden among the increasing number of war-afflicted refugees resettled in the United States. Strength-based interventions aim to empower individuals to solve their problems utilizing their strengths (Ruch et al., 2020), which may be beneficial for mental health promotion, such as counseling and health promotion workshops to build up life skills in promoting quality of life (Peterson et al., 2020).
Guided by strength-based intervention and community needs, the social and emotional wellbeing (SEW) intervention was developed for refugees, incorporating their strengths and skills required to manage stressors by building up their stress management, problem-solving, and social networking skills (Poudel-Tandukar et al., 2021, 2022). The SEW intervention was effective in reducing stress, anxiety, and depressive symptoms and improving coping, family networking, and family conflict resolution skills among Bhutanese refugees in group and family settings delivered by peers (Poudel-Tandukar et al., 2021, 2022). By observing its significant benefit on the social and well-being of refugees, we replicated this intervention among Ukrainian refugees resettled in Massachusetts. We aimed to assess the effect of SEW intervention on social and emotional well-being (coping, social support, self-efficacy, and social working) and mental health outcomes (stress, anxiety, and depression) among Ukrainian refugees resettled in Massachusetts. We hypothesized that the program would result into improved social, emotional, and mental well-being among Ukrainian refugees. Incorporating community strengths to address their mental health needs would give them the responsibility to take care of their health and sustain the program’s effect.
Methods
Study participants
We implemented SEW intervention among 31 Ukrainian refugees resettled in Massachusetts in collaboration with Ascentria Care Alliance, which has been providing refugee resettlement services to refugees from different countries, helping them achieve independence and stability. The inclusion criteria for participants were Ukrainian refugees aged 18 years older, living in Massachusetts, and willing to provide written informed consent to participate in the program voluntarily. The first and last authors prepared a program information sheet including program objectives, procedures, inclusion criteria, and informed consent procedures. The native Ukrainian staff of Ascentria Care Alliance (third author) circulated program information to the community members via word of mouth, phone, formal and informal gatherings, and staff mobilization during their regular program in western Massachusetts. All individuals who were interested to participate in the study contacted the third author, who then invited them to the program. The first and last authors provided detailed program information to the interested participants in group. They answered any queries participants had about the program and program procedures with the help of an interpreter. Each participant read the informed consent and provided their consent by writing their initials or signed the informed consent. Participants were compensated $100 and an exercise mat for completing the baseline and after-program surveys and five intervention sessions. The study procedures were reviewed and approved the University of Massachusetts Amherst Institutional Review Board.
Intervention
We developed a SEW program incorporating skills required to strengthen stress management, problem-solving, and self-efficacy to integrate into the new culture of the United States using community-engaged participatory research. The detailed program development procedure of five modules was described in our previous publications (Poudel-Tandukar et al., 2021, 2022). In brief, the
We delivered program content in five sessions. In the first hour of each session, we discussed culturally tailored health education, problem-solving, and practice skills. In the second hour, participants enjoyed breathing and mind-body exercises (20 simple low-risk exercise poses). We implemented a program in two groups between October 2022 and February 2023 in collaboration with Ascentria Care Alliance in its office in West Springfield. Feedback was taken from each participant after the program. Handouts on tips, including stress management, communication, and social networking skills, as well as pictographs on breathing and mind-body exercises, were distributed to the participants. We encouraged participants to practice the problem-solving lesson they had learned and do mind-body exercises with their family members.
Theoretical framework
Our intervention delivers skills required to strengthen their acculturative skills to help reduce stress and mental health burdens, guided by two main theoretical constructs. According to Lazarus and Folkman’s stress and coping theory (Lazarus & Folkman, 1987), individuals feel stress when there is a gap between demands created by the situation and their ability to cope with stressors. When individuals are stressed, they may be unable to make efficient use of resources. According to Bandura’s self-efficacy theory (Bandura, 1997), an individual’s coping skills depend on their skills to use available coping resources effectively. Positive enforcement increases positive adaptive strategies that predict better mental health outcomes, which rely on self-cognitive evaluation of the development of positive coping skills and self-efficacy (Bandura, 1997). Based on these theoretical constructs, our intervention aims to strengthen coping and self-efficacy skills that ultimately help to reduce stress, anxiety, and depressive symptoms. Identifying and enhancing individual’s strength will improve the effective use of coping resources that promote mental health and social well-being.
Data collection
A structured self-administered questionnaire translated into Ukrainian language was used to collect information from participants at baseline and post-intervention. Third author (a bilingual researcher) briefed each question in their Ukrainian language and answered participants’ queries during the survey process. Participants took about 45 to 60 min to complete the survey. We maintained participant’s confidentiality by using numerical codes instead of their names in their survey documents.
Measures
Depression and anxiety
We measured anxiety and depression symptoms experienced over the past month using the Hopkins Symptom Checklist-25 (HSCL-25; Derogatis et al., 1974). It consists of a 10-item subscale for anxiety and a 15-item subscale for depression. The responses were scored on a Likert scale from 1 (not at all) to 4 (extremely). The score of 25 items was summed up to calculate a total score, with higher scores indicating higher perceived anxiety and depressive symptoms. We calculated the mean score of anxiety and depression separately by summing up responses and dividing by the number of answered items. A cut-off score of >1.75 was used to categorize depressed participants as it has been used in a previous study assessing mental health status among Russian refugees resettled in Finland (Rask et al., 2015). The Cronbach’s α for anxiety was 0.92, and for depression was 0.92 for this study.
Perceived stress
We used a Cohen Perceived Stress Scale that consisted of 10-item version to measure perceived stress of the past month (Cohen et al., 1983). The responses were scored on a 5-point Likert-type scale, ranging from never (0) to very often (4). The score of 10 items was summed up to calculate a total score, with higher scores indicating higher perceived stress. The Cronbach’s α for stress was 0.81 for this study.
Coping strategies
A 32-item Coping Strategies Inventory-Short Form (CSI-SF) was used to measure coping strategies (Tobin, 2000). The responses were scored on a 5-point Likert-type scale, ranging from not at all (1) to very much (5). The score of 32 items was summed up to calculate a total score, with higher scores indicating a better coping style. It consists of four secondary subscales, each including 8-item: problem-focused engagement, problem-focused disengagement, emotion-focused engagement, and emotion-focused disengagement coping strategies. The Cronbach’s α for coping strategies was 0.83 for this study.
Social support
We used a 12-item Multidimensional Scale of Perceived Social Support (MSPSS) scale to measure support from friends and family (Zimet et al., 1988). The responses were scored on a 5-point Likert-type scale, ranging from strongly disagree (1) to strongly agree (5). The score of 12 items was summed up to calculate a total score, with higher scores indicating a greater social support. The Cronbach’s α for social support was .95 for this study.
Social networks
The social networks with family and friends will be measured using a 12-item Lubben Social Network Scale-Revised (LSNS-R) scale (Lubben et al., 2006). This scale consists of measures for size, closeness, and frequency of family and friend networks. It consisted 6-item to measure kinship ties, and a comparable set of 6-item to measure friend ties. The score of 6-item was summed up to calculate a total score, with higher scores indicating a greater family or friend network. The Cronbach’s α for kinship ties was .80 and for friend ties was .80 for this study. Participant’s responses ranged from none (0) to 9 or more or always (5).
Family conflict resolution
The discussion of differences, effective communication, and measures in coming to a solution were measured using the 17-item Family Conflict Resolution Scale (FCRS; Roskos et al., 2010). It consists of positive (11-item) or negative resolution (6-item). Participant’s responses ranged from strongly disagree (1) to strongly agree (7). The high scores on the favorable resolution indicated high positive resolution levels, and the low scores on the negative resolution indicated the high levels of negative resolution. The scale has high internal consistency (Cronbach’s α = .83) in this study.
Coping self efficacy
An individual’s perceived skill to cope effectively with challenges and threats was measured using 26-item coping self-efficacy (CSE; Chesney et al., 2006). We asked participants about their confidence in dealing with their problems when their situation is not going well. It consists of three sub-components: problem-focused coping (12-items), stopping unpleasant emotions and thoughts (9-items), and getting support from friends and family (5-items). Participants responded to their self-efficacy on an 11-point scale of 0 (cannot do at all), 5 (moderately certain can do), and 10 (certain can do). The scale has high internal consistency (Cronbach’s α = .92) in this study.
Socio-demographic and lifestyle variables
We collected information on socio-demographic variables such as age, sex, marital status, education, employment, and years residing in the United States. Information on life style factors such as smoking, alcohol consumption, and history of any chronic diseases such as hypertension, diabetes mellitus, heart diseases, and kidney diseases were also collected.
Data analysis
We tested the normal distribution of each outcome variable before performing analysis. The difference between pre and post-intervention outcomes was measured using paired t-tests for continuous and McNemar test for categorical variables. The alpha values for significance testing was determined by Bonferroni correction based on three primary outcomes, using multiple statistical tests, using 0.05/3 = 0.016. SAS statistical software version 9.1 (SAS nstitute, Inc., Cary, NC) was used to analyze the data.
Results
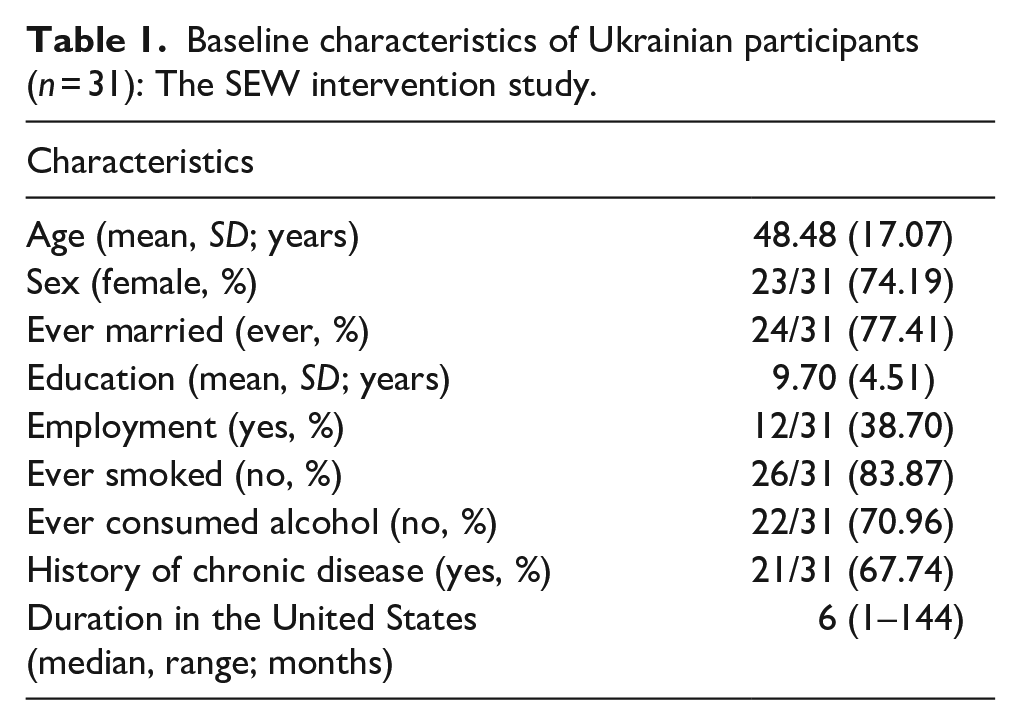
Altogether, thirty-one participants attended the intervention and completed the before and after intervention surveys and five intervention sessions. The mean age of the participants was 48.48 (17.07) years, and of school years was 9.70 (4.51). Majorities of participants were female (74.19%) and married (77.41%; Table 1). Similarly, 38.7% of participants were employed, 83.87% never smoked, 70.96% never consumed alcohol, and 67.74% had a history of any chronic diseases. The median duration in the United States was 6 months (Table 1).
Baseline characteristics of Ukrainian participants (n = 31): The SEW intervention study.
The proportion of participants with above-threshold anxiety and depressive symptoms was reduced by >50% from before to after intervention (Figure 1). For example, the proportion of participants with above-threshold anxiety reduced from 61.29% before and 22.58% after intervention. Similarly, the proportion of participants with above-threshold depression reduced from 58.06% before to 22.58% after intervention (both p’s < 0.01). The mean scores of mental health outcomes significantly decreased from before to after intervention: by 6.26 points for stress (21.09 (5.11) vs. 14.83 (3.22)), 7.07 points for anxiety (21.74 (7.51) vs. 14.67 (4.16)) and 6.29 points for depression (29.22 (9.63) vs. 22.93 (7.33); all p’s < 0.01; Table 2).
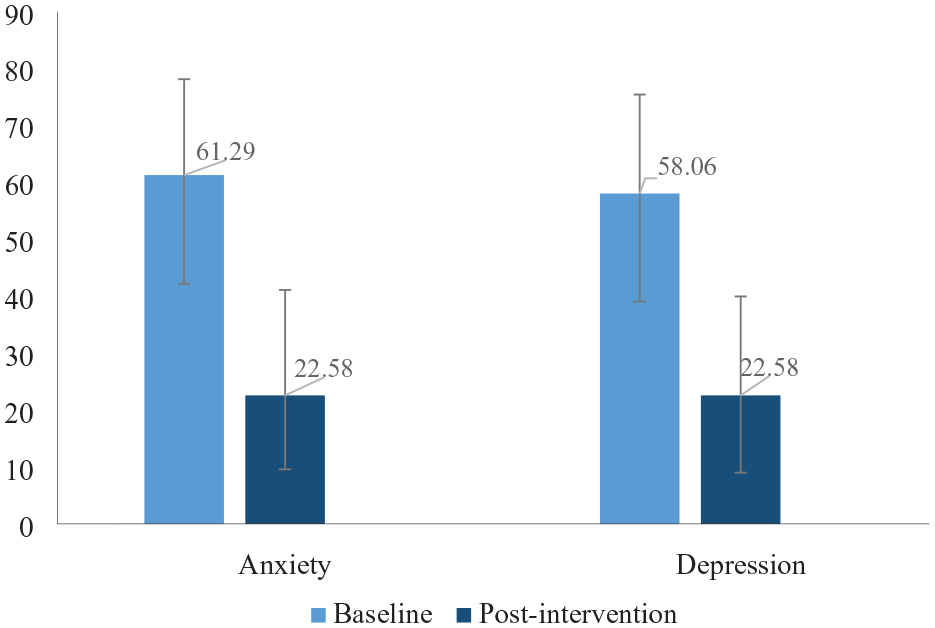
Prevalence (percentage) and confidence intervals of anxiety and depressive symptoms at baseline and post-intervention (n = 31; both p’s < 0.01): The SEW intervention study. We used a cut-off point score >1.75 (averaged across each set of items) to identify anxiety and depressive symptoms using the Hopkins Symptom Checklist-25 (HSCL-25).
Intervention effects on mental health and social and emotional well-being measures (n = 31): The SEW intervention study. .
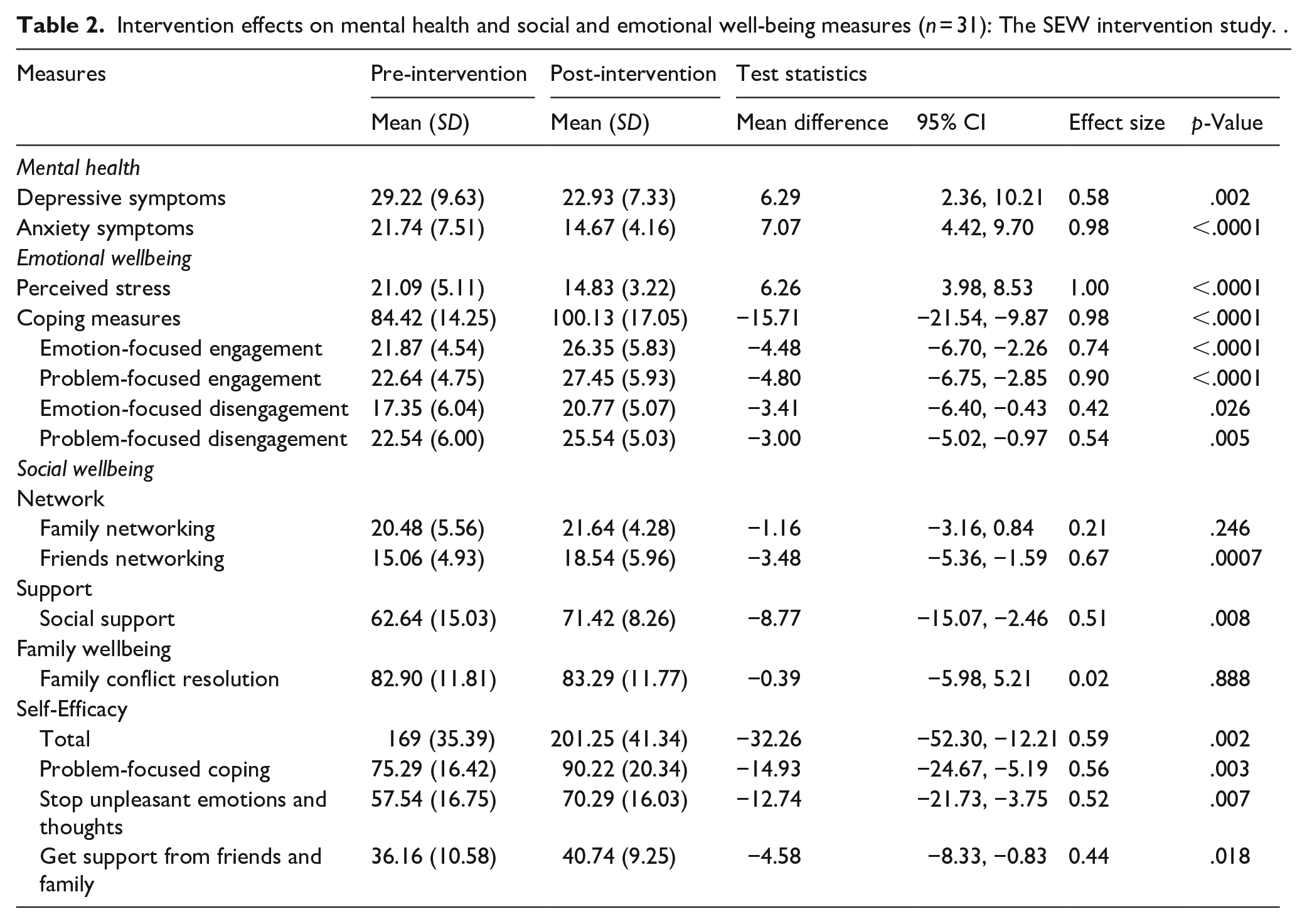
Our participants’ social and emotional well-being outcomes improved significantly after the intervention. The mean scores of social and emotional well-being outcomes increased from pre- to post-intervention by 15.71 points for coping (84.42 (14.25) vs. 100.13 (17.05)), by 4.48 points for emotion-focused engagement (21.87 (4.54) vs. 26.35 (5.83)), by 4.80 points for problem-focused engagement (22.64 (4.75) vs. 27.45 (5.93)), and by 3 points for problem-focused disengagement (22.54 (6.0) vs. 25.54 (5.03); all p’s < 0.01). For support, the mean scores increased by 3.48 points for friends networking (15.06 (4.93) vs. 18.54 (5.96)) and 8.77 points for social support (62.64 (15.03) vs. 71.42 (8.26)). For self-efficacy, the mean scores increased by 14.93 points for problem-focused coping (75.29 (16.42) vs. 90.22 (20.34)) and by 12.74 points for stop unpleasant emotions and thoughts (57.54 (16.75) vs. 70.29 (16.03); all p’s < 0.01; Table 2).
Discussion
The mean scores of acculturative hassles, stress, anxiety, and depressive symptoms decreased, and the mean scores of coping, friend’s networking, and self-efficacy increased from pre- to post-intervention among Ukrainian refugees resettled in Massachusetts. Our strength-based intervention was associated with a >50% reduction in the prevalence of anxiety and depressive symptoms. The program was also helpful in improving other life skills of participants, such as coping, self-efficacy, and friend networking, which have been proven as essential target mechanisms to reduce mental health burdens. Our multi-component strength-based intervention successfully addressed various socio-cultural stressors of community members due to their engagement in designing and implementing the program for their benefit.
The social and emotional well-being intervention was developed by engaging community members in all decision-making processes, from designing to implementing and evaluating the program (Poudel-Tandukar et al., 2021, 2022). We identified community strengths such as coping, resilience, self-efficacy, and social support and incorporated relevant required skill development program components in the intervention to advance their life skills. Initially, we tested the effect of SEW intervention in group settings. We found it effective in reducing mental health burden and improving coping, self-efficacy, and networking skills among Bhutanese refugees resettled in Massachusetts (Poudel-Tandukar et al., 2021). With this program’s success, we scaled up the SEW intervention delivered by trained community interventionists among Bhutanese refugees in family settings. We found the SEW intervention was equally effective in reducing >50% of mental health burdens, such as anxiety and depressive symptoms among Bhutanese adults (Poudel-Tandukar et al., 2022). We shared this program experience with community members and partners working with Ukrainian refugees. By understanding the need and benefit of the program, we replicated it for newly arrived war-afflicted Ukrainian refugees. The results of our intervention suggest that the SEW program was effective in reducing stress, anxiety, and depression among Ukrainians. This result is in line with a previous study (Poudel-Tandukar et al., 2022) that revealed positive effects of the intervention among Bhutanese refugees who were resettled in the same environmental settings with a similar trauma exposure of deportation. Thus, navigating community strengths to address their needs by integrating them into intervention design via community-academic partnership helped to make the program effective and successful. Community engagement is one of the most practical strategies for addressing health disparities (O’Mara-Eves et al., 2015).
Interventions that address social, emotional, and cultural stressors are essential to promote the mental health of refugees as they have gone through them during their migration journey from their home country and to resettlement and post-resettlement to the host country due to their limited language and other personal and social skills required to integrate into the new system. Thus, realizing the interwoven complexities of stressors in refugee’s lives, various evidence-based interventions such as mind body interventions (Prathikanti et al., 2017), psychoeducation (Zlotnick et al., 2001), problem-solving (Cuijpers et al., 2018) were incorporated into our SEW intervention to address their needs. Participants expressed the benefits of lessons learned from each component in their physical, mental, and social well-being. For example, stress management education gave them skills to strengthen positive thoughts and interactions related to their daily activities. They became optimistic and happier and learned to change their vision toward life by doing meaningful activities to advance their skills. They learned to take responsibility for taking care of themselves by working on their problems by breaking them into simple pieces through learning skills from problem-solving exercises. Overall, participants mentioned that the intervention helped them advance their skills to solve their problems, boost their coping, confidence, and self-efficacy, promote their intra and intercultural networking, and become optimistic and happy in their lives. These traits promoted their mental, social, and emotional well-being, which ultimately helped reduce their stress and mental health burden. Coping measures such as problem-solving planning, instrumental support, self-distraction, and behavior disengagement were used by the Ukrainians during the war conflict (Xu et al., 2023). Studies suggest that coping (Xu et al., 2023), self-efficacy (Piotrowski et al., 2023), and social support (Piankivska, 2022) skills may reduce stress and mental health burdens among Ukrainians.
Our intervention included culturally tailored educational materials, problem-solving and practice exercises, and a pictograph on mind-body exercises that focused on strengthening interpersonal processes on coping, self-efficacy, and social networking. The contents of the intervention were simple and easy to digest, which had a meaningful impact on their daily behavior to bring change in their lives. The practice exercises were culturally tailored and easy to work on every week. Most importantly, after working on their problem-solving exercises, they felt happy after feeling differences in their thought process and behavior. Participants highly appreciated the positive impact of mind-body exercises on their physical, mental, and emotional health. They mentioned that pictographs on exercises were helpful to continue their practices even after the program. They also built up friends’ networking with new community members and work together to advance their skills and careers. Our strength-based intervention helped participants work on their problems by utilizing their strengths. Strength-based interventions helped to improve personal confidence, self-esteem, life satisfaction, hope, and goal attainment (Fukui et al., 2010; Green et al., 2013).
Our study has some limitations. First, our study design was a single pre- and post-intervention group without a control group, so we cannot draw causal inferences. Second, recruitment of participants for a control group was not feasible for newly resettled Ukrainian refugees, who valued including all members in the intervention group to provide them with benefits. Third, we recruited participants motivated to attend the intervention on a first come, first served basis; thus, there may be a selection bias. Fourth, the HSCL-25 scale was used to measure anxiety and depressive symptoms, though clinical diagnosis is the gold standard. Such a clinical diagnosis measure was not feasible in community-based studies. Several studies have used this scale among refugees (Hollifield et al., 2002; Poudel-Tandukar et al., 2021, 2022) and Ukrainians (Rask et al., 2015). Fifth, the sample size of this study was small due to limited resources. However, this pilot study’s findings would help design a large randomized controlled trial study by scaling up an intervention. Finally, most participants were middle-aged in our study; thus, we should be careful in generalizing the study findings to the older adult population.
In conclusion, our intervention resulted into significant improvement in coping, self-efficacy, and friend networking behaviors and reduction in stress, anxiety, and depressive symptoms scores after intervention among newly resettled Ukrainian refugees. A strength-based intervention like ours would be helpful to reduce mental health burdens by promoting individual’s strength to cope with stressors and self-efficacy to adjust to their new cultural settings. Furthermore, a large-scale study with a randomized controlled trial is needed for rigorous program impact evaluation before replicating it among refugees nationwide.
Footnotes
Acknowledgements
We would like to thank our Ukrainian community participants for participating in the program. We also want to thank the Ascentria Care Alliance staff members for their support in recruiting participants, translating intervention and survey materials, and interpreting the intervention sessions and program documents. We sincerely appreciate the effort of Pamela Burris, a holistic nurse and certified yoga trainer, who provided yoga training to community members.
Author contributions
KP-T contributed to the study conception and design, prepared study materials, implemented program, analyzed and interpreted the data, and prepared the manuscript. KCP contributed to preparing study materials, program implementation, and data collection supervision. CD and YM contributed to data collection and program implementation. All authors contributed to interpret data and commented on previous versions of the manuscript. All authors read and approved the final manuscript
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project is funded by a grant from the Blue Cross Blue Shield of Massachusetts Foundation. Created in 2001, the mission of the Blue Cross Blue Shield of Massachusetts Foundation is to ensure equitable access to health care for all those in the Commonwealth who are economically, racially, culturally, or socially marginalized through grantmaking and policy initiatives. (PIs: Kalpana Poudel-Tandukar and Krishna C Poudel)
Ethical approval
The Institutional Review Board of the University of Massachusetts Amherst, USA, approved the study and certified that it was performed according to the ethical standards in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Disclaimer
The contents expressed in the manuscript are solely the authors’ responsibility and do not represent the official views of the Blue Cross Blue Shield of Massachusetts Foundation.