
Abstract
Introduction:
Secure extended care units (SECUs) are low-secure locked inpatient units. They are considered the most restrictive intervention within the continuum of mental health rehabilitation programmes for patients within non-forensic public mental health services. Limited information about psychosocial and forensic aspects of patients referred to such units is available.
Aim:
This study explored the psychosocial and forensic characteristics and predictors of acceptance in an Australian SECU programme over a 5-year period (2019–2023).
Methods:
A retrospective study design investigated 121 consecutive referrals. The 98 first-time patient referrals were included in the main analysis. Descriptive statistics were used with non-parametric comparisons (Chi-square and Fisher exact test where appropriate). Logistic regression was undertaken to assess the influence of covariates.
Results:
Referral from an inpatient mental health setting was the only predictor that influenced acceptance onto the SECU (OR 3.168, 95% CI: [1.129, 8.913], p = .029). More than four-fifths had a forensic history. Only 14 % had a history of youth offending, but 73% had a past conviction before referral. Sixty percent had a history of Family violence and two-thirds were on Bail. Services prioritised containment and abstinence, whereas patients sought skills development and employment. Patients had least contact with a Psychologist among all allied health disciplines before referral.
Conclusions:
The study provides evidence that the SECU is receiving patients with high forensic and psychosocial needs, which are unmet within community mental health programmes in the absence of medium and high-secure units. There is a need for a balanced approach between containment, rehabilitation, and community reintegration for this cohort.
Introduction
Incarceration rates in Australia have increased significantly over the past decade (Carroll et al., 2021). Prisoners are three times more likely than those in the general community to have a mental illness. They are 15 times more likely to have a psychotic disorder, with significant numbers reporting lifetime suicidal ideation and attempting suicide (Carroll et al., 2021; Mullen & Ogloff, 2009). Poor access to inpatient rehabilitation has led to inappropriate use of acute inpatient beds and lengthy delays in finding placements and re-incarceration (Allison et al., 2018; Das, 2025; Sisti et al., 2015).
Mind the Gap report (Smith-Merry et al., 2018) indicated that 91% of patients with severe mental illness in Australia will continue to be supported within public mental health services (MHS). There are challenging presentations related to substance use and homelessness; MHS environments are not purpose-built or safe for managing individuals at high risk of harm to themselves and others (Allison et al., 2018; Hodgins et al., 2009; McKetin et al., 2018). This then leads to a revolving door of hospitalisation, homelessness, and transfers between prison and hospitals (Allison et al., 2018; Carroll et al., 2021; Das, 2025; Sisti et al., 2015).
The National Disability Insurance Scheme (NDIS) in Australia is mandated to provide psychosocial support to this cohort of vulnerable people through Non-Governmental Organisations (NGO). However, they have only been able to support a small minority of these patients needing care (Office of Parliamentary counsel, 2024). Harvey et al. (2016) found that people with psychosis who are homeless or living in marginalised accommodation and have significant difficulties in social functioning are less likely to take up the services of rehabilitation and community linkage services of the NGO. They may be excluded as they struggle to come up with the “right goal” required by these NGO services. NDIS support services are limited in what is available. They cannot provide rehabilitation support to patients while in hospital for an extended period, or are excluded when they are in prison (Office of Parliamentary counsel, 2024).
In Victoria, Australia, secure extended care units (SECUs) are low-secure locked inpatient rehabilitation units. They are often thought of as the last resort and most restrictive intervention within the continuum of mental health rehabilitation programmes for patients within non-forensic public MHS (Boston Consulting Group, 2006; Das, 2025; Department of Human Services, 2007). Bed access is limited (Das, 2025). An internal audit of the patient cohort at a SECU in Austin, Australia, in August 2021, demonstrated that 23 of 25 patients admitted at the time had forensic histories, with a further patient having engaged in significantly violent conduct, which did not result in formal sanctions (Personal communication, August 19, 2021). This is understandable in the context that the Thomas Embling Hospital (high secure unit) in Victoria can no longer provide rehabilitation for non-forensic patients with complex needs who cannot be safely or suitably managed by the MHS (Forensicare, 2019). The Thomas Embling Hospital (TEH) is under-resourced, leading to considerable delays in bed and access flow, resulting in patients already in the forensic system being unable to access care in a timely fashion. There are no medium secure units in Victoria (Carroll et al., 2021; Forensicare, 2019). It has long been identified that a gap exists in service provision between forensic services and MHS. This leads to vulnerable and high-risk patients not getting the necessary treatment and falling through the cracks (Carroll et al., 2021; Mullen & Ogloff, 2009). It is, therefore, important to understand the needs of such a complex cohort of severe mental illness (SMI) patients and predictors of acceptance so that the right bed can be offered at the right time to maximise recovery opportunities.
Methodology
The study considered 121 consecutive referrals to the SECU between 1 January 2019 and 31 December 2023. All first referrals (as opposed to patients referred more than once) during the study period were categorised as the Total sample (N = 98). The Total sample was further classified into Accepted (n = 55) and Non-accepted groups (n = 43). Data analysis was conducted for the Total sample and the subgroups (Accepted and Non-accepted patients).
Details of the study design, social demographics, and clinical profile are described previously (Das, 2025). Most of the Total sample were male, single, younger age group (18–34 years of age), of European ethnicity, with an English-speaking background, educated to secondary school year level, and on disability benefits. Most had a clinical diagnosis of Schizophrenia (65%), with fifty-three percent of patients with schizophrenia also had comorbid personality traits/disorders and eighty-eight percent having comorbidity with substance use. Sixty percent of the Total sample had a combination of risk to self and others, followed by harm to others. The median Health of Nations Outcome Scale (HoNOS) was 20 (IQR 14, 23) and the Life Skills Profile (LSP) was 22.5 (IQR 16.25, 27). The majority of patients were involuntary under the Mental Health Act. The median contact with mental health services was 14 years, the median number of public hospital admissions was 12, and the median time since the first involuntary treatment was 8.5 years. Most referrals were received when the patient was in an acute mental health inpatient unit (67%), followed by the community (22%). More than half had a length of stay of up to 3 months before their referral 79.7%. More than eighty percent of the Total sample was on single depot and oral medication treatment. Treatments like Clozapine and Electroconvulsive therapy (ECT) were low (Das, 2025).
The researchers categorised the complexity of the presentation into three levels based on different social, clinical, and treatment factors; range from level I to III (higher complexity in level III). The categorisation enabled quantitative analysis of clinical complexity while acknowledging that psychiatric presentation exists along multiple dimensions.
This framework drew on established concepts of complex psychosis, clozapine resistant schizophrenia, difficult-to-treat schizophrenia, and the clinical and social characteristics of mental illness within forensic populations (Carroll et al., 2021; Chakrabarti, 2021; Kane, 1996; Killaspy et al., 2021). Patients were classified according to the highest complexity level for which they met the criteria.
Level I: Diagnosis of SMI, severe functional impairment, cognitive dysfunction, length of illness > 2 years, multiple hospitalisations.
Level II: Incarceration, 6 months hospital admission, significant risk behaviours, homicide and suicide attempts, unremitting illness, homelessness.
Level III: Failed clozapine attempts, ECT, repeat admissions to SECUs, multiple imprisonments.
Similarly, levels of interventions before referral to SECU were grouped, with level 3 indicating more intensive intervention. Assertive community treatment is considered the first level due to the complexity of patients compared to community case management (Harvey et al., 2012)
Level 1: Assertive community treatment.
Level 2: Assertive community treatment plus one treatment episode of ECT and or clozapine, forensic, and or family intervention.
Level 3: Assertive intervention and more than one episode of ECT, clozapine, and or forensic, family intervention, or involvement of the Office of the Chief Psychiatrist.
Outcome measures of the HoNOS (Wing et al., 1996) and LSP data (Rosen et al., 1989) were used to characterise a typical referred patient to SECU and accepted patient.
Statistical Analysis
Data analysis was conducted using IBM SPSS for Macintosh Version 28 (IBM Corp, 2021). A complete case analysis was conducted. Descriptive statistics were used with non-parametric comparisons (Chi-square and Fisher’s exact test where appropriate).
Data were missing for HoNOS (26.5%) and LSP (34.6%) in the Total sample, mainly from the Non-accepted group. As a result, no statistical comparisons were conducted for these outcome measures between the Accepted and Non-accepted groups and the data are presented descriptively.
For creating a model of acceptance into the SECU programme, the primary outcome variable was SECU acceptance (yes/no). A multivariate logistic regression analysis was employed to develop a predictive model for admission to SECU using enter method. All the independent variables whose p-value < .25 in the Chi-squared test or Mann-Whitney test were considered for inclusion (Bowers, 2008). Collinearity was assessed using Variance inflation factor (VIF) with values less than 5 deemed acceptable.
The final model included complexity of presentation, previous forensic admission, and setting of the referral. The other variables failed to predict the model of acceptance. Ten events per outcome variable rule were considered for inclusion in the final model (Ranganathan et al., 2017).
The analysis estimated adjusted odds ratios (ORs) with 95% confidence intervals (CIs) for each covariate, allowing for the quantification of associations between predictor variables and SECU admission outcomes. Significance testing was conducted at the .05 alpha level.
Ethics
The study protocol and the data sheet form were approved by Austin Hospital and Oxford Tropical Research Ethics Committee (HREC/84769/Austin-2022; OxTREC HREC 577-23).
Funding
Austin Health Foundation provided a seed grant. The funder had no role in the design, data collection, analysis, interpretation, or report writing.
Results
Complexity and Levels of Treatment
Level II complexity was the most common cohort in the Total sample (38.8%), followed by Level I (36.7%) and Level III (24.5%). The Accepted group predominantly had complexity levels I (45%) and II (38%), whereas the Non-accepted group had complexity levels II (39.5%) and Level III (34.5%; Table 1). There was a trend towards statistical significance between acceptance and lower levels of complexity (p = .05; Table 1). The odds ratio for Level I complexity to be admitted, compared to Level III, was 3.788 (95% CI [1.275, 11.254]), p = .017. Level II was not statistically different to level III.
Complexity Levels for the Total Sample, Accepted and Non-Accepted Groups.
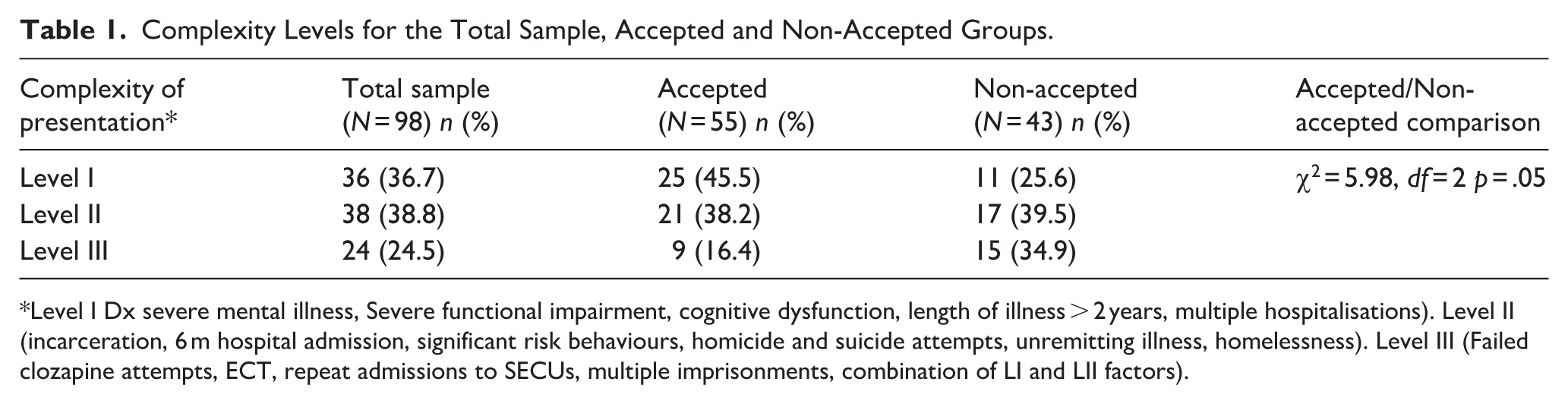
Level I Dx severe mental illness, Severe functional impairment, cognitive dysfunction, length of illness > 2 years, multiple hospitalisations). Level II (incarceration, 6 m hospital admission, significant risk behaviours, homicide and suicide attempts, unremitting illness, homelessness). Level III (Failed clozapine attempts, ECT, repeat admissions to SECUs, multiple imprisonments, combination of LI and LII factors).
Level 1 intervention patients were twice as likely to be accepted into the SECU, but this was not significant. Non-accepted patients received Level 2 and 3 interventions prior to referral (Table 2). Linear-by-linear association (Chi-square trend) indicates that higher levels of intervention were associated with a lower likelihood of SECU acceptance (Level 1 = 70%, Level 2 = 50%, Level 3 = 47.8%; Table 2); the trend was towards significance (p = .069).
Intervention Levels for the Total Sample, Accepted and Non-Accepted Groups.
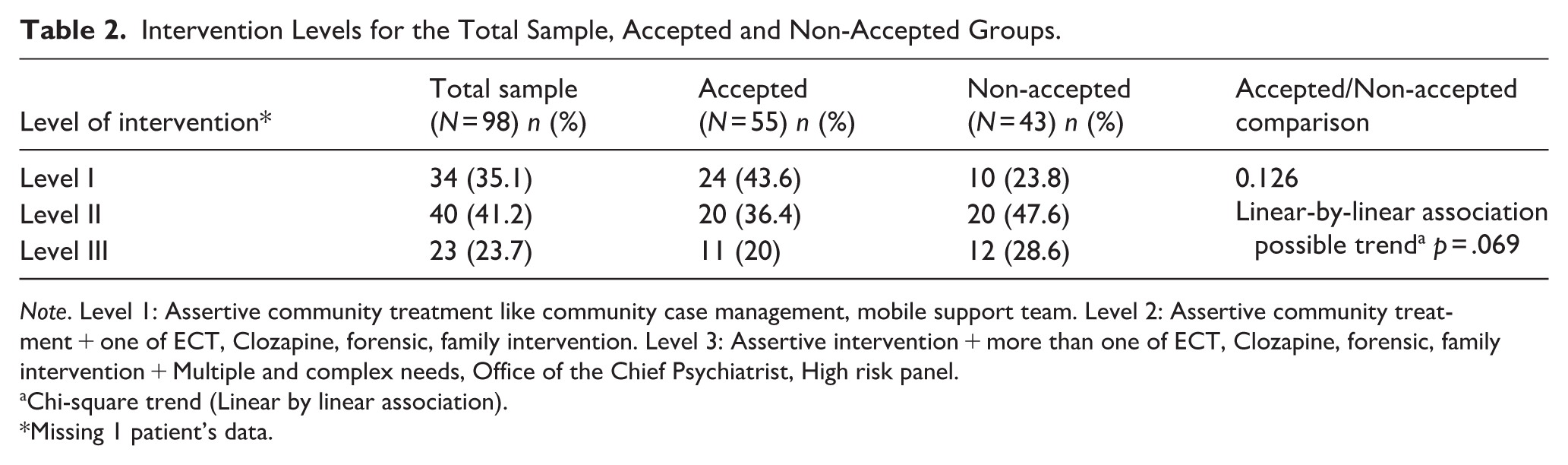
Note. Level 1: Assertive community treatment like community case management, mobile support team. Level 2: Assertive community treatment + one of ECT, Clozapine, forensic, family intervention. Level 3: Assertive intervention + more than one of ECT, Clozapine, forensic, family intervention + Multiple and complex needs, Office of the Chief Psychiatrist, High risk panel.
Chi-square trend (Linear by linear association).
Missing 1 patient’s data.
Legal Status and Advance Statement
More than a third of patients were under guardianship orders, including financial, general living, and access to care. Only nine patients in the Total sample had an advance statement of preferences (specifying a person’s treatment and support wishes when subject to compulsory assessment or treatment) and nominated persons (assist a person to express their views and preferences and exercise their rights if the person becomes unwell and needs compulsory mental health assessment or treatment) (Table 3).
Mental Health Act Status, Guardianship Act, and Forensic Order for the Total Sample, Accepted and Non-Accepted Groups.
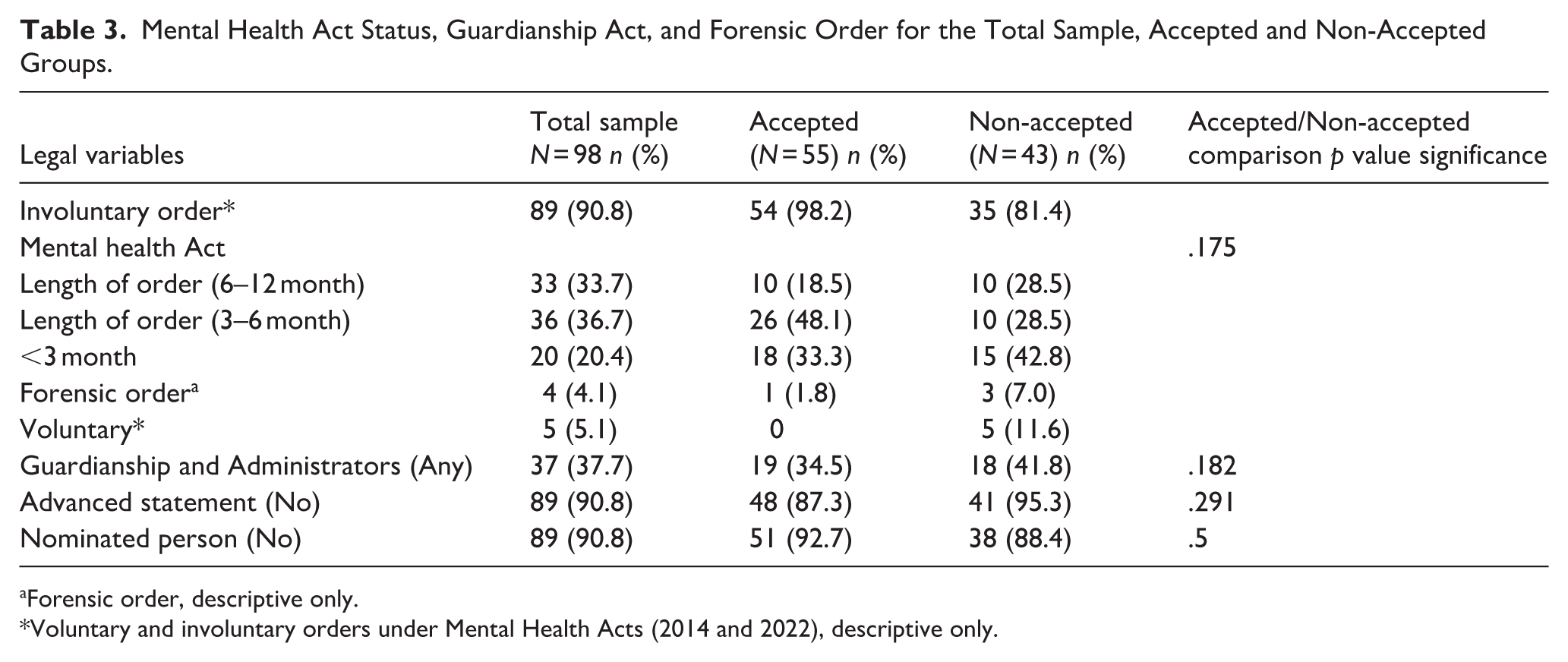
Forensic order, descriptive only.
Voluntary and involuntary orders under Mental Health Acts (2014 and 2022), descriptive only.
There was a statistically significant association between mental health legal status (involuntary) and acceptance into SECU when examining the subgroup of patients who were voluntary and involuntary (rho = −.357, p < .001). There were no voluntary patients in the Accepted group. Most voluntary patients in the Non-accepted group were in prison. Logistic regression was not run due to the small number of voluntary patients in the study; seventy-seven percent of patients were informed about their referral, out of whom only thirty-eight percent were accepting of such a referral to SECU.
The odds of being accepted from inpatient units were 2.14, and the odds of being accepted from the community were 0.69. The OR was 3.095 (95% CI [1.14, 8.37]; p = .026), indicating a statistically significant difference. The involuntary legal status and length of orders were comparable between the Accepted and Non-accepted groups. There was a statistically significant association between mental health legal status (involuntary) and acceptance into SECU when examining the subgroup of patients who were voluntary and involuntary (rho = −.357, p < .001).
Forensic History
More than four-fifths of the Total sample had a reported current or past forensic history, with a median index (first) offence age of 21 years (IQR 17.75, 28). Only fourteen percent had a history of youth offending, but seventy-three percent had a past conviction by the time of their referral to SECU. A median of 9 years (IQR 3.5, 19) elapsed between the index offence and referral to SECU (excluding patients who were previously referred and admitted to SECU).
The most common antisocial behaviour (59.2%) was a combination of different acts with violence, with seventy percent convicted of violence in the past (Table S1). Sixty percent of the Total sample had a history of Family Violence and had an Apprehended Violence Order (AVO) at some point in time. Nine percent had been victims of violence or family violence and had an AVO. Most of the violence was from current or ex-partners. Families mostly bore the brunt of violence (56%). Intimate partner violence was present in nine percent. One-third of referrals had up to three pending charges in front in courts. Almost two-thirds were on bail. Eight percent of referrals were in prison and two percent in Thomas Embling Hospital at the time of referral. The gravest offences noted were murder, attempted murder and serious sexual assaults and most frequent offence were assault, harm or endanger a person (Table S2).
There were no differences in index age, past conviction, pending charges, or nature of offences between the Accepted and Non-accepted groups. More patients were bailed in the Accepted group (45.4 vs. 25.6 %) and had a family violence perpetrator history (64 % vs. 60%) compared to the Non-accepted group. The Accepted group had patients who had committed homicide, and the Non-accepted group had more patients with sexual offences. Despite significant substance use in this population, drug offences were low (Table 4).
Forensic History for the Total Sample, Accepted and Non-Accepted Groups.
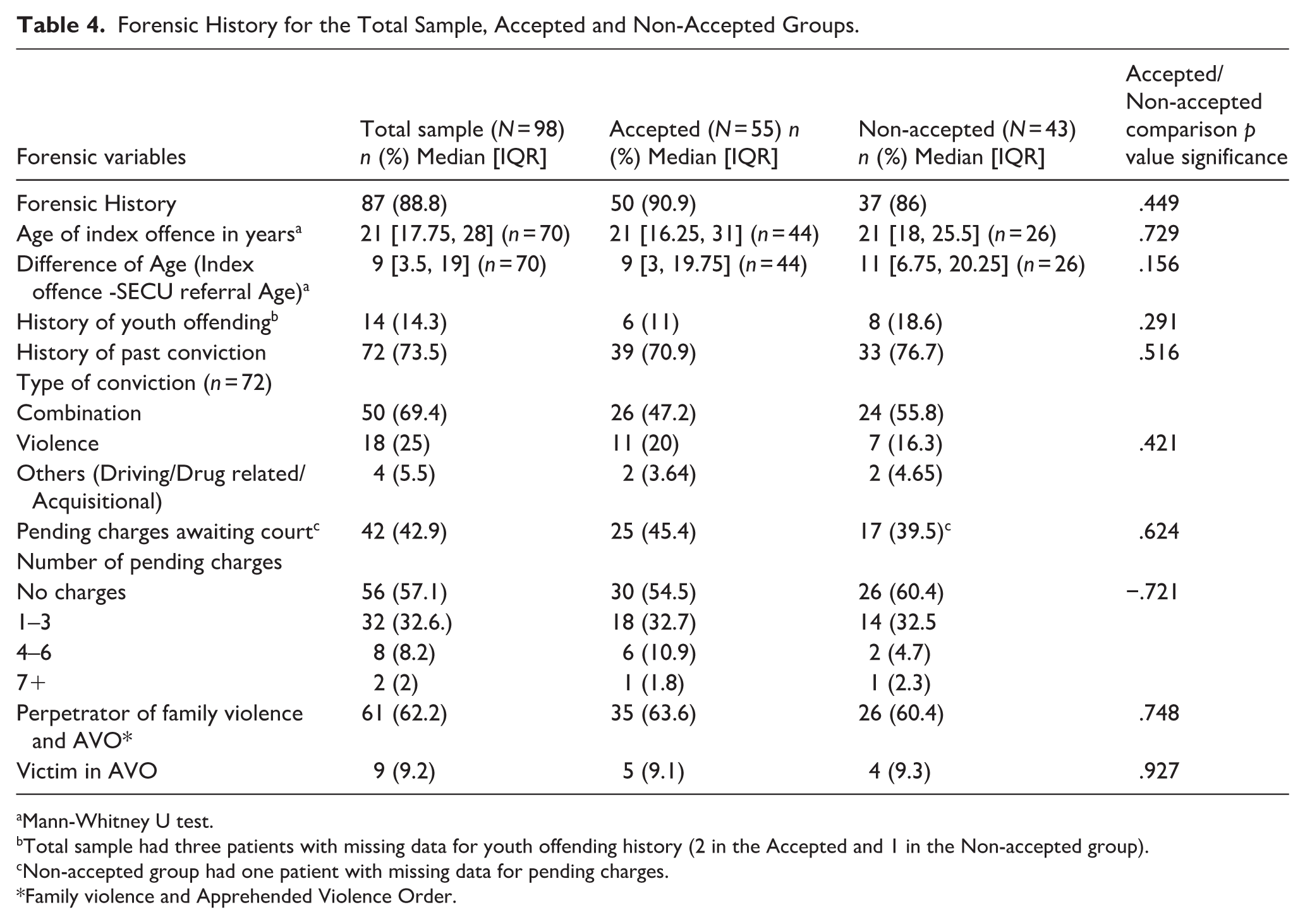
Mann-Whitney U test.
Total sample had three patients with missing data for youth offending history (2 in the Accepted and 1 in the Non-accepted group).
Non-accepted group had one patient with missing data for pending charges.
Family violence and Apprehended Violence Order.
Patient Goals (As Reported in Their Records)
For the Total sample, the top three goals reported by patients were living independently and/or having a choice of accommodation, finding work, and having lifestyle choices (Table 5). Accepted patients wanted to develop skills, find work, and live independently compared to Non-accepted patients, whose focus was on making independent living choices, community re-engagement, and substance use management (Table 5).
Broad Patient Goals of the Total Sample, Accepted and Non-Accepted Groups.

Note. ADLS = Activities of Daily Living.
discharge from prison, NDIS support, and attending community group programmes.
Getting back driving license.
A lower proportion of the Accepted patients expressed no goals on referral (43.6%) compared to Non-accepted patients (62.7%; Table 5).
Service Goals
The referring MHS’s primary aim for the patients appeared to be containment and stabilisation, and to break the revolving-door admission or offending cycle. This was followed by a review of medication and Alcohol and Other Drug (AOD) intervention for the Total sample (Table 6). Among the top four goals, containment and review of medication were important in both Accepted and Non-accepted groups. AOD intervention was higher on the MHS list for Accepted patients, and linkage with community and NDIS services was higher for Non-accepted patients (Table 6).
Broad Service Goals of the Total Sample, Accepted and Non-Accepted Groups.
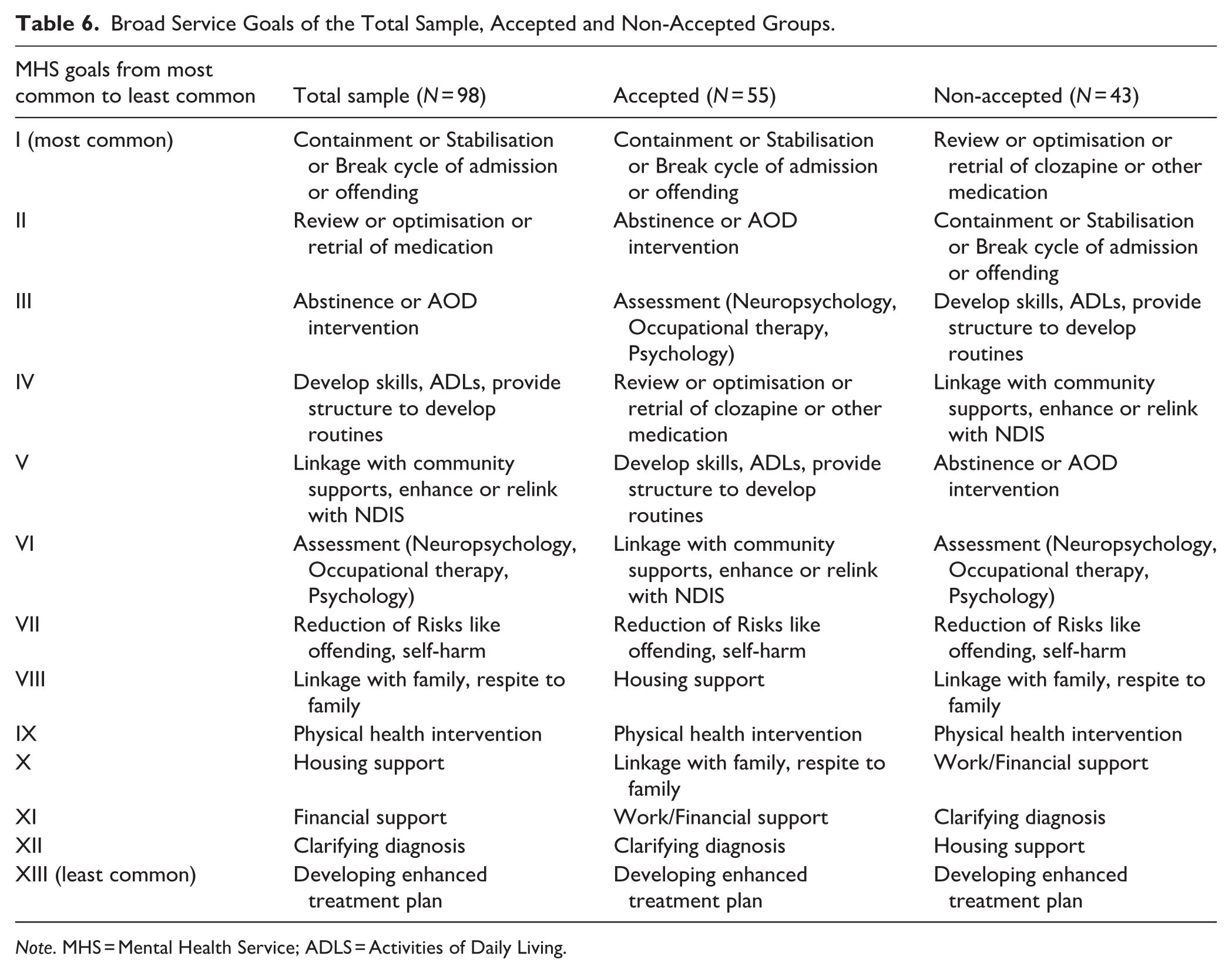
Note. MHS = Mental Health Service; ADLS = Activities of Daily Living.
Housing Situation and National Disability Insurance Scheme (NDIS)
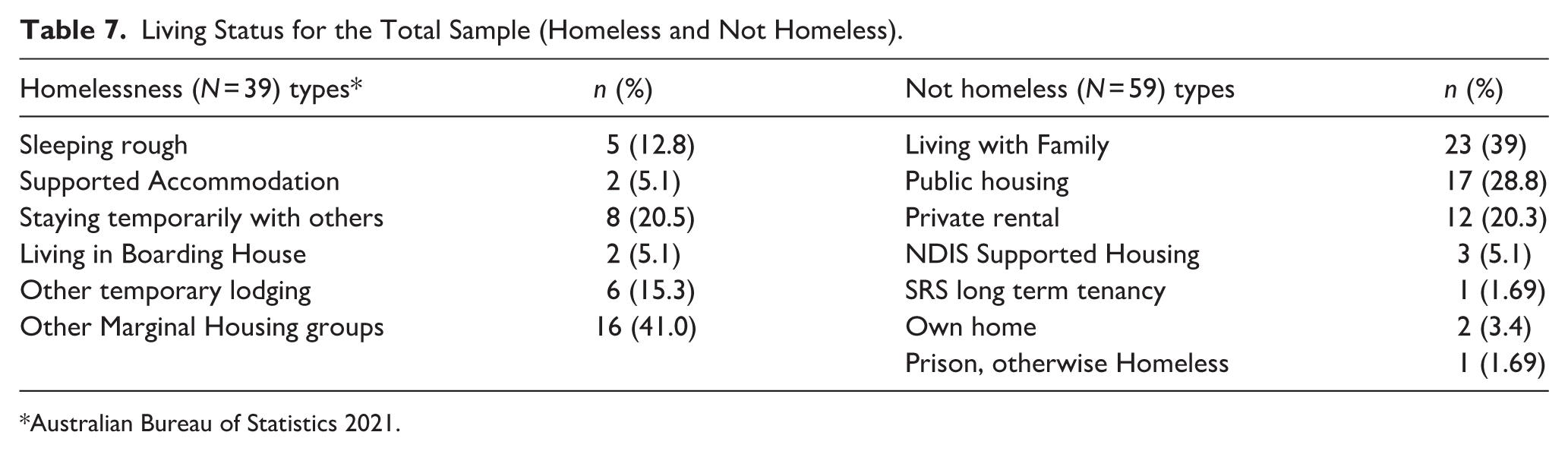
Homelessness was reported in fourty percent of the Total sample (Table 7). Most of those experiencing homelessness belonged to other marginal housing groups, which refers to people living in caravan parks and improvised and crowded dwellings (Australian Bureau of Statistics, 2021). Where people were not considered homeless, close to fourty percent were living with family, and less than thirty percent had access to public housing. A small number had their own home (Table 7). There was no statistically significant difference in homelessness predicting admission to SECU (yes, 53.8% vs. No, 57.6%; p = .836). NDIS supports were present in 38% of the Total sample, with sixty percent reporting as disengaged. There were no significant differences between the Accepted and Non-accepted groups.
Living Status for the Total Sample (Homeless and Not Homeless).
Engagement With Allied Health
Of all the allied health professionals, the social work discipline had the most contact with the Total sample, followed by occupational therapists, before referral to SECU. This cohort had the least contact with psychologists among all the professions. Behavioural plans were lacking in almost sixty-seven percent of the Total sample and more so in Non-accepted patients (74.5%).
Comparison of HoNOS Profile of the Accepted Patients and Total Sample
The HoNOS profiles indicated that an Accepted patient had mild aggressive tendencies, agitation, minor cognitive problems, minor health problems, mild delusions and hallucinations mild depressive symptoms, mild anxiety, moderate difficulties in relationships due to active or passive withdrawal, lacking in ADLs, living in less than ideal accommodation with limited choice of activities. HoNOS for the Non-accepted group was not calculated due to small numbers (n = 10; Table S3).
Comparison of LSP of the Accepted Patients and Total Sample
LSP scores indicated that Accepted patients had difficulty initiating and responding to conversation, showing warmth to others, were moderately well-groomed and clean, with neglect of physical health, rarely violent, had difficulty in maintaining friendships, moderately unreliable with taking medications, behaving irresponsibly, and capable of sheltered work. LSP scores for Non-accepted patients were not presented due to small numbers (n = 10; Table S4).
Predictors of Acceptance
The covariates of setting, complexity level and past forensic admission were examined. In the unadjusted model, being in a mental health inpatient setting prior to referral to SECU was significantly associated with the acceptance outcome, with an OR of 3.095 (95% CI: [1.114, 8.37], p = .026). Past forensic admission showed a significant negative association, with an OR of 0.265 ([0.114, 0.615], p = .002), indicating that individuals with a history of forensic admissions were less likely to be accepted into SECU. Prison and Thomas Embling referrals (Forensic admissions) made up only a small share of the Total sample (10%), and none of the people referred from prison were in the Accepted group. Under the SECU admission policy, patients cannot be transferred directly from prison. Complexity Level I, compared to the reference category (Complexity Level III), was significantly associated with acceptance (OR = 3.788, [1.275, 11.254], p = .0017).
After adjusting for the above covariates, the association between inpatient setting and acceptance remained significant, with an adjusted OR of 3.168 (95% CI: [1.126, 8.913], p = .029). However, the association for past forensic admission became non-significant (adjusted OR = 0.428, [0.150, 1.220], p = .112). Similarly, the association for Complexity Level I also diminished and was no longer statistically significant (adjusted OR 1.639, [0.431, 6.231], p = .468; Table 8).
Logistic Regression Predicting Acceptance into the SECU Programme.
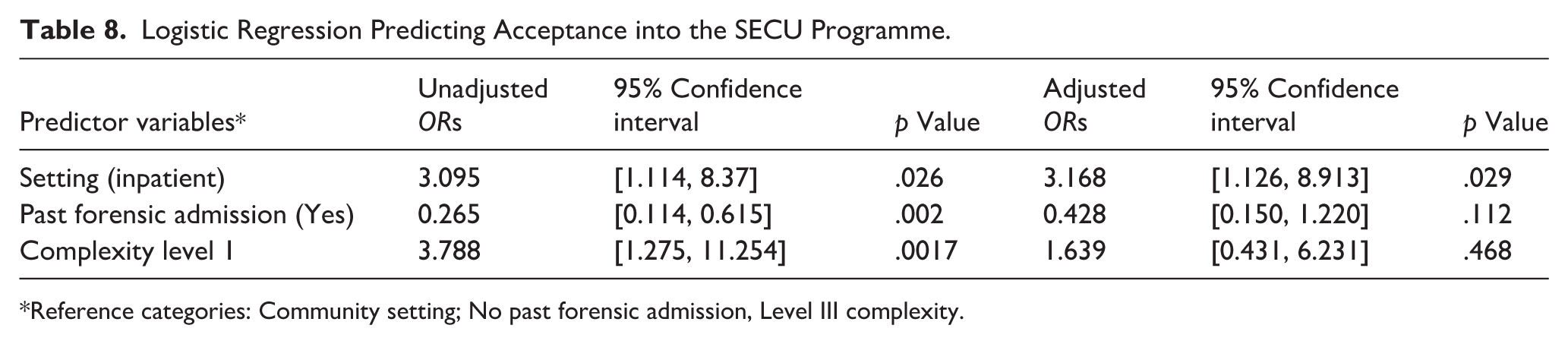
Reference categories: Community setting; No past forensic admission, Level III complexity.
Discussion
The study highlights the complex interplay between patient needs and risk considerations in psychiatric admissions of patients referred over a 5-year period to a SECU in Australia. Inpatient setting was a predictor of acceptance. It is possible that contextual factors related to inpatient care, like containment, stabilisation of mental state and abstinence from AOD, may contribute to this pattern. However, this interpretation should be considered exploratory, as the decision-making rationale was not recorded for the Non-accepted group.
This pattern may have implications for equity of access. Individuals managed in the community who require structured and intensive support may be less likely to be referred from inpatient settings, particularly if they do not meet admission thresholds or primarily present with negative symptoms such as amotivation and social withdrawal, and lower levels of overt violence or forensic involvement. As a result, referral pathways may inadvertently favour individuals with more acute behavioural disturbance, persistent positive symptoms, or ongoing legal system involvement.
None of the referrals made from prison were accepted. SECU policy does not permit direct prison-to-SECU transfers; instead, an interim inpatient admission is required, contingent on bed availability and justice procedures, and may be superseded by release from prison. Reasons for non-acceptance were not recorded, hence it was not possible to evaluate whether these pathway constraints contributed to the outcome; nevertheless, the finding raises equity and justice concerns, as additional procedural hurdles may delay access to appropriate care for people exiting custody.
The onset of significant criminal behaviour occurred later in life for most of the sample. The median gap of 9 years between index offence and SECU referral suggests possible challenges in engaging and identifying patients with high forensic risks within MHS or prioritisation of acute psychiatric needs over long-term rehabilitation (Hodgins et al., 2009). The study provides some evidence towards the criminalisation of those with a mental health problem. Addressing this is important through early diversion programmes and integrated forensic-psychiatric services to reduce the revolving-door phenomenon observed in this population (Rice et al., 2024).
Violence was the most prevalent form of antisocial behaviour. The violence within this cohort is consistent with literature linking substance use, personality disorders, socioeconomic disadvantage, and poor adherence to treatment (Grann et al., 2008; Hodgins, 2008). Hodgins et al. (2009) observed that aggressive patients with substance use and criminal behaviours did not receive more intense or different treatment to other patients in the community. Assertive community treatment traditionally has not reduced incarcerations. Therefore, accepting the Level 1 intervention cohort referred to SECU for intensive treatment makes sense in this context.
Sixty per cent of individuals had a history of family violence, and many had been subject to AVOs, suggesting a high prevalence of interpersonal violence within domestic settings. The discovery of cases where family violence was documented but not reported to police points to potential underreporting, reinforcing the need for systematic screening and intervention in MHS. Rani et al. (2023) noted that the lifetime prevalence of violent crimes against people with severe mental health problems was between 10.1% and 66.7%, but fewer than half of these crimes are reported to the police.
Two-thirds of the Total sample of patients rejected a referral to SECU when offered at the time of referral. It is understood that inpatient rehabilitation is considered a restrictive treatment option (State of Victoria. Royal Commission into Victoria’s Mental Health System, 2021). Choice and control are essential parts of the recovery journey, which may determine success in rehabilitation in this group (Brown, 2013). SECU patient goals strongly emphasise autonomy and integration into society, suggesting that psychiatric rehabilitation should prioritise areas such as housing support, vocational training, dealing with the criminal justice system and social reintegration.
Goals listed by Accepted patients focused on developing skills, securing employment, and achieving independent living, indicating a wish for functional stability and readiness for structured support. Non-accepted patients prioritised making independent living choices, re-engaging with the community, and managing substance use. These goals may reflect the higher prevalence of social instability, substance use issues, and potential behavioural risks in this group. The need for substance use management suggests that co-occurring disorders may be a key barrier to SECU acceptance, necessitating alternative models of care tailored to dual-diagnosis patients. No goals on referral could be related to patient disengagement or rejection of such a referral.
Findings from patients referred to the SECU described above are similar to those of the SHIP study (Carr et al., 2012). The most important challenges facing participants of the SHIP study were finances, loneliness or social isolation, lack of employment, poor physical health, and uncontrolled symptoms of mental health and housing (Carr et al., 2012). It is important to balance clinical and personal recovery and incorporate trauma-informed care to reduce dissonance in goal setting (Wilson et al., 2017). Shorter admission, safe and dignified treatment, patient-centred goals and alignment of goals are needed to achieve more acceptance of referral and subsequent success in rehabilitation.
The utilisation of specialist allied health professionals and behavioural management plans was low before referral, which could indicate disengagement with community teams. Cognitive assessments, the creation of behaviour management plans and the management of physical comorbidity and substance use treatment were high on the list of priorities for the referring services. This is in keeping with findings of Lavelle (2007).
Low utilisation of NDIS services is an important finding. This is in keeping with Harvey et al. (2016) who reported that a subset of patients do not engage. Further, restriction in NDIS funding during admission to SECU could mean that disengagement remains an issue even post-discharge from the facility. There is a need for change in the NDIS funding model for this subset of patients entering inpatient rehabilitation services to achieve better chances of integration back into the community.
The study cohort had a much higher proportion of homelessness than the survey of community patients reported by others (Harvey et al., 2016; Harvey et al., 2012). High homelessness could be associated with social disadvantage, forensic history, dissocial personality, childhood trauma, substance use or other factors like housing affordability, low income, and challenges with reintegrating with mental health treatment (Barry et al., 2024).
Implications for Practice
Findings reinforce the need for a balanced approach between containment, rehabilitation, and community reintegration. While the SECU programme accepts some very high-risk patients, many Non-accepted individuals possibly face ongoing barriers due to unmet dual-diagnosis needs, housing instability, continued offending and social reintegration challenges. Expanding integrated treatment models and strengthening community-based rehabilitation could enhance the accessibility and effectiveness of psychiatric care for complex, high-risk individuals. A model that integrates housing organisations and NDIS support services with clinical services could make it attractive for patients, as these are high on the list of patient goals. The NDIS regulatory framework will need to be reviewed to consider SECU as a distinct model of care from acute inpatient care. This is to remove the restriction on access to NDIS services for this vulnerable cohort once they are admitted to the programme. All individuals requiring secure extended mental health care should have equitable access to SECU services regardless of custodial status. For patients in custody or prison settings, an informal place-reservation capacity that operates independently of acute inpatient bed availability or justice procedures should be considered. Finally, a model of care that provides a personalised treatment plan with a range of treatment choices, focusing on skills creation, substance use management, with trauma informed care, could balance the restrictive nature of the unit.
Implication for Future Research
Addressing barriers to acceptance to rehabilitation for high-risk individuals requires a shift towards early referral after a period of assertive community treatment; preferably before a cycle of offending, hospitalisation and homelessness occurs. Further study, with a larger sample size, will elucidate some of these predictors. In addition, Non-accepted patients and their trajectory needs to be studied to understand referral back to the SECU and the challenges in community management of such a complex cohort.
Abuse and violence towards this cohort were possibly under-reported and under-detected. Future studies should examine factors influencing the reporting of such matters by patients, families and services. Cross-comparative analysis of referral pathways and clinical outcomes across similar units in Australia and internationally would provide essential evidence for policymakers evaluating the contemporary role of extended inpatient care within integrated mental health systems.
Limitations
The study could not compare complexity to a cohort of community patients not referred to the service to ascertain the difference better. Further, follow-up of Non-accepted patients’ post-referral could have provided greater insights into the unmet needs of this population. This could lead to selection bias, as entry into SECU is determined by factors related to both need and systems issues, rather than the true distribution of clinical complexity, which may affect the generalisability of the results.
The retrospective nature of the research has limitations, such as missing data for certain variables, such as HoNOS and LSP. This could have underestimated the complexity of the Non-accepted group.
Verified forensic histories were challenging to ascertain unless information had been provided by the referrer. This could have led to an underestimation of the patients’ complexity in both groups. Reasons for the decline of acceptance were not available for most of the Non-accepted group, which could have helped understand decision-making better. This could have provided information about risk tolerance, service capacity, and competing priorities for the receiving service at the time. This may misattribute nonacceptance to patient complexity.
Conclusions
The research adds valuable information about the complex cohort of patients referred to a SECU programme. The linear association between intervention levels and acceptance rates suggests that individuals with higher complexity and risk (Level III) face difficulties accessing SECU services despite their requirement for structured care. This highlights a need for medium and high secure beds within non-forensic settings. Containment is required for a cohort of high-risk patients whose long-term recovery calls for proactive rehabilitation strategies crafted by a specialist group of neuropsychologists, forensic behaviour specialists, and family violence specialists in coordination with NDIS. This necessitates integrating forensic and community programmes across the board, from assertive community teams to community rehabilitation programmes. This could help to manage individuals with repeated hospitalisations, serious offending, and forensic histories, as well as provide early intervention programmes to prevent patients from progressing to Level III complexity. Doing so could reduce reliance on hospitalisation as a short-term containment as both primary and secondary level intervention.
Supplemental Material
sj-docx-1-isp-10.1177_00207640261439746 – Supplemental material for Psychosocial and Forensic Characteristics of Adult Mental Health Patients Referred to an Australian Secure Extended Care Unit and Predictors of Acceptance
Supplemental material, sj-docx-1-isp-10.1177_00207640261439746 for Psychosocial and Forensic Characteristics of Adult Mental Health Patients Referred to an Australian Secure Extended Care Unit and Predictors of Acceptance by Partha Das, Emma Robertson, Victoria Harpwood and Stephanie Tierney in International Journal of Social Psychiatry
Supplemental Material
sj-docx-2-isp-10.1177_00207640261439746 – Supplemental material for Psychosocial and Forensic Characteristics of Adult Mental Health Patients Referred to an Australian Secure Extended Care Unit and Predictors of Acceptance
Supplemental material, sj-docx-2-isp-10.1177_00207640261439746 for Psychosocial and Forensic Characteristics of Adult Mental Health Patients Referred to an Australian Secure Extended Care Unit and Predictors of Acceptance by Partha Das, Emma Robertson, Victoria Harpwood and Stephanie Tierney in International Journal of Social Psychiatry
Footnotes
Acknowledgements
The study was completed as part of the dissertation in partial fulfilment of the requirement for the award of Master of Science in Evidence-Based Health Care with the Department of Continuing Education, University of Oxford, United Kingdom. We gratefully acknowledge the contribution of Sarah Funnell, Psychologist, to the study protocol, data collection and data cleaning. We sincerely acknowledge Prof. Hellen Killaspy, Professor of Rehabilitation Psychiatry, University College London, for constructive feedback about the study plan.
Ethical Considerations
The study protocol and the data sheet form were approved by Austin Hospital and the Oxford Tropical Research Ethics Committee (HREC/84769/Austin-2022; OxTREC HREC 577-23).
Author Contributions
Partha Das: Responsible for doing literature search, writing Protocol, ethics submission, data collection, cleaning, data analysis and writing the paper. Emma Robertson: Contributed towards ethics submission, organising SECU shared referrals folder, data collection and cleaning, review of paper for submission. Victoria Harpwood: contributed towards review of protocol plan and final submission. Stephanie Tierney: Supervised research study as part of MSc Dissertation and review of final submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Austin Health Foundation provided a seed grant. The funder had no role in the design, data collection, analysis, interpretation, or report writing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request.*
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.