
Abstract
This exploratory article gives a cross-sectional account of how established health-care systems have responded to the novel challenge of drug shortages. In line with previous research, our analysis confirms the existence of strong path dependence in the adoption of policy responses. This path dependence is manifested in a pronounced typology of response patterns where jurisdictional approaches to the management of drug shortages differ along two core dimensions. These are the salience attributed to the problem, and the level to which state organisations engage with the problem. These patterns are mirrored in the conceptual framing and strategic orientation of the respective drug shortage policies, with: Spanish and Irish drug shortage policies focusing on the individual product level and being largely reactive; US policies focusing on the therapeutic level, with a focus on mitigation; and German and Austrian policies seeking to address the active ingredient level, with a proactive focus on shortage prevention. Despite the importance of legacies, we find evidence of innovation and path creation particularly in relation to the US and German approaches, which we explain by the simultaneous occurrence of internal crisis and pressures from local stakeholders.
Points for practitioners
This article addresses a major challenge, drug shortages, which has emerged in recent years and could be characterised as a ‘system shock’. A typology of policies adopted based on an analysis of a range of health system responses is developed. Fundamental differences across these responses are evident, such as level of action (individual product level/therapeutic level/active ingredient level), time frame (from ad hoc/short term to long term) and strategic approach (reactive/mitigating/preventive). This analysis finds fundamentally different policies, such as delegated institutional powers and census management/network governance. The typology based on the salience attributed to the problem and the nature (proactive/reactive) of policymaking may assist stakeholders in health systems to critique their approach to this challenge and, at a more fundamental level, how the system responds to disruptive events.
Introduction
The past four decades have seen wide-ranging reforms of the health-care systems (hereafter, HCSs) of industrialised nations. Simonet (2011: 823) notes that this has entailed a pervasive increase in cost awareness, with ‘rising insurer competition in Germany, the separation of care delivery and financing in the UK, health care networks in France and regional delegation in Italy all signalling a will to manage healthcare expenditure more efficiently’. This cost awareness is known to encompass virtually all aspects of health care, including service and goods components in the broadest sense (Simonet, 2017).
Up until about 2009, pharmaceuticals spending by HCSs had largely been seen within this cost-centred lens, with authors such as Vuorenkoski, Toiviainen and Hemminki (2008) documenting the prioritisation of pharmaceutical expenditure control in various HCSs. More recently, the increased extent and severity of global pharmaceutical shortages has added a new, unwelcome dimension to the management of medicines within HCSs (Fox et al., 2014). There is now an ever-looming threat of frequently occurring pharmaceuticals shortages that affects virtually all HCSs.
Pharmaceutical shortages present a qualitatively new phenomenon that differs in fundamental ways from classical cost saving and pharmaceutical rationing. Pharmaceutical rationing is linked to ostensibly rational cost-containment decisions, arising when foreseeable limitations on financial resources necessitate the full or partial withholding of a potentially beneficial drug from patients on grounds of affordability (Williams et al., 2012). While there is no reliable estimate as to the prevalence of this type of rationing, there is evidence of HCSs making efforts to limit access to expensive new drugs (see, e.g., Gornall et al., 2016). This is perhaps not surprising given that for 2015, pharmaceutical spending comprised between 12% and 18% of total national health-care expenditure in Organisation for Economic Co-operation and Development (OECD) countries (OECD, 2018).
By contrast to classical rationing decisions, which are usually based on detailed cost–benefit data, the challenge of pharmaceutical shortages relates to the unexpected unavailability of a drug, often without precise knowledge of when, or if, the desired drug will be available again, what alternatives are available, and/or which risks the use of these alternatives entails. As such, drug shortages (hereafter, DSs) present unfamiliar territory to HCSs, which usually have little or no experience in managing uncertainty as regards the availability of drug supplies. In other words, while reforms may have prepared HCSs to cope with constraints in financial resources, there is little or no experience, or precedent, in terms of managing uncertainties in key supplies.
The purpose of this article is to identify the primary policy trajectories and approaches that a mix of jurisdictions have adopted to cope with the DS crisis. In investigating this issue, our approach is both data driven and selective. The jurisdictions chosen for analysis (the European Union (EU), as represented by the European Medicines Agency (EMA), the US, Germany, Spain, Austria and Ireland) include entities for which there is both accessible information in relation to the incidence of pharmaceutical shortages, and documentation that allows for an analysis of key policies adopted in response to this problem. Additionally, our analysis suggests that these jurisdictions represent demonstrably different response patterns. The article gives a cross-sectional account of how established HCSs have responded to this emerging challenge, and examines the degree to which these responses mirror historical policy trajectories, or, alternatively, have led to the adoption of novel approaches.
Pharmaceutical shortages as a global problem
Pharmaceutical shortages have come to present an increasing problem to HCSs since the mid- to late 2000s (Fox and Tyler, 2009). The problem has been recognised by the World Health Organisation (WHO) from about 2009 onwards (Fox et al., 2014). Active measures to address this issue were taken by the WHO from 2015 onwards, when the organisation called a consultation meeting on global pharmaceutical shortages (WHO, 2016). Resultant WHO reports noted that medicines shortages were increasing, particularly for older, off-patent drugs and treatments that are difficult to formulate. DSs also included many commonly used medicines, such as antibiotics, cancer and cardiovascular medicines, and anaesthetics (WHO, 2016: 180). The WHO summarised the primary causes of shortages as: difficulties in acquiring raw materials; manufacturing problems; competition issues; business decisions; the impact of new technology; expensive medicines; and market fragmentation (WHO, 2016: 181).
This article focuses on approaches to the management of pharmaceutical shortages as they have emerged within developed countries’ HCSs. This focus on developed-country HCSs relates to the observation made by the WHO that such approaches have not developed significantly elsewhere because ‘unreliable data from peripheral facilities continue to be a major problem in most low- and middle income countries, hindering coordinated stock management and effective forecasting’ (WHO, 2016: 2). The discussion here centres on the US and Europe, where responses have evolved and data and policy documents in relation to shortage management are available.
Our article is structured in three parts. The first part discusses definitions of pharmaceutical shortages and summarises the literature on their causes. The second part describes policy measures across a number of jurisdictions, with a focus on shortage lists as they are currently collated and disseminated. The third part categorises existing approaches with a view towards identifying continuities and novelty in this emerging area of policymaking.
Defining pharmaceutical shortages
De Weerdt et al. (2015) highlight how definitions of a DS differ at organisational levels. They suggest that the objectives of the institution constructing a definition will mirror their own perception as to whether shortages are a technical supply-chain issue or one based on market issues, such as pricing, the level of competition and/or the policies of funding agencies. They find 20 different definitions, with variances arising from ‘when does a supply problem become a shortage, permanent and/or temporary shortages, the typology and time frame of DS’, as well as differences resulting from the fact that some regulatory agencies focus on clinically essential drugs and/or limit the definition of shortages to those drugs for which there is no alternative (De Weerdt et al., 2015: 1). Despite this variety of definitions (WHO, 2017), De Weerdt et al. (2015) observe that many of these classifications are not comprehensive in that some do not include permanent discontinuations of drugs. Bogaert et al. (2015: 2) suggest that differing national timelines for identifying shortages, and different national emphases on the locus of a shortage, can make cross-national comparisons difficult. Even where definitional approaches are seemingly uncomplicated or apolitical, they can sometimes reflect complex assumptions about the institutional capacities of key components of HCSs, such as those of prescribers.
A key source of complexity in this matter is the degree of granularity with which a shortage is considered. Product, and especially detailed branded product-based, definitions and indicators of shortages can be unhelpful if the focus is on ensuring and managing an adequate supply of therapeutic options, as one would expect it to be from a public health perspective. Here, a whole other range of considerations may come into play before the absence of a specific product represents genuine DSs from a HCS perspective. These include the availability of therapeutic alternatives that provide the same or similar benefits without posing significant risks to patients (Ventola, 2011).
The original US Food and Drug Administration (FDA) definition of DSs reflected such an ambitious approach. Here, DSs were described as ‘a situation in which the total supply of all clinically interchangeable versions of an FDA-regulated drug is inadequate to meet the current or projected demand at the patient level’ (FDA, 2011: 1). This definition had the potential for establishing relatively narrow parameters for the definition of shortages in that it identified shortages as situations where there were no other clinical options to the drug that was unavailable (Ventola, 2011). The FDA has now adopted a more basic definition of DSs that defines these as ‘a period of time when the demand or projected demand for the drug within the United States exceeds the supply of the drug’ (FDA, 2017: 14).
Both past and present US FDA approaches differ from the somewhat narrower focus taken by the EMA. The EMA (2013a: 1) provides an implicit definition of DS as part of its shortages list (launched in 2013) by stating that this includes ‘medicine shortages that affect or are likely to affect more than one European Union (EU) Member State, where the EMA has assessed the shortage and provided recommendations to patients and healthcare professionals across the EU’. This is coupled with the statement that the organisation ‘does not give a complete overview of all medicine shortages occurring in the EU, as most shortages are dealt with at a national level’ (EMA, 2013a: 1). Accordingly, it is not medical necessity alone, but multi-jurisdictional unavailability, that is required for a shortage to be identified. Further complexity arises in monitoring quality and DSs because EU requirements to list manufacturers on drug labels are not mirrored in the US (Woodcock and Wosinska, 2013).
A widely recognised problem in assessing the extent of pharmaceutical supply deficiencies is that it is difficult to distinguish between specific stock-keeping unit shortfalls, arising, for instance, from a specific dosage unit being unavailable while the drug itself is accessible in other forms/doses, as opposed to more insurmountable or genuine DSs at the level of active ingredient. In response to this, professional organisations such as the American Society of Health-System Pharmacists (ASHP) have suggested that the focus of attention should be on upstream impact with a DS being understood as a ‘supply issue that affects how the pharmacy prepares or dispenses a drug product or influences patient care when prescribers must use an alternative agent’ (ASHP, 2009: 1399). This approach, if fully developed, would classify DSs according to the potential harm that they could cause and/or the resources and efforts that it would take to manage and ameliorate them. The ASHP’s own DS list accordingly provides information on: (1) the specific product affected by dosage and trade name; (2) reasons for the shortage; (3) estimated resupply dates; and (4) related shortages.
From a regulatory or health policy standpoint, this type of information can present valuable input into DS management processes in which very short-term, replaceable/manageable or non-essential shortages, and hence relatively harmless DSs, are clearly distinguished from others, and the attention of regulators and policymakers is then paid to chronic, recurring and dangerous shortages of significant public and health policy relevance. We discuss the extent to which such an approach has been adopted in different jurisdictions later in this article. Additionally, the current ASHP list, with its identification of specific underlying causes of a shortage, allows for broader policy interventions that could involve multi-stakeholder high-level discussions in line with the current German ‘pharmaceutical shortages’ jour fixe, where senior representatives from government, industry and medical and pharmaceutical services providers meet to discuss how to address existing or projected shortages (BfArM, 2016). While in the US, communication between the FDA and pharmaceutical suppliers and producers has increased, there is little evidence that the organisation is posed to follow a similar model (Medina and Richmond, 2015; Schweitzer, 2013).
Causes of shortages
There is now a substantial literature that examines the causes of DSs in developed countries. EMA (2012) groups these into three broad categories: (1) economic and regulatory reasons; (2) business reasons; and (3) manufacturing and supply-chain problems. Economic and regulatory causes of DSs include: issues arising from austerity, restrictive fiscal policy and related government policy changes; increasing regulatory requirements; and shifts in demand due to new therapeutic applications. Business reasons contributing to DSs include: increasing price volatility; reduced margins; increasing dominance by a limited number of producers; parallel sales; tendering systems that favour larger-scale producers; and the impact of medico-legal considerations. Lastly, some of the key manufacturing problems associated with DSs relate to: problems in adapting to increasing governmental requirements; transfers of production due to mergers and acquisitions; long production lead times; increasing raw material bottlenecks (active substances, excipients); the quality-related failure of production batches; and multi-authority approval requirements arising from outsourcing practices (IMS Health, 2011, 2015).
A review of this literature highlights the intertwined nature of a number of underlying triggers. These include: complex global supply chains (EMA, 2012: 3); production system issues (ISPE, 2014; Ventola, 2011); market demand and production planning (Saedi et al., 2016); poor market attractiveness (Gupta and Huang, 2013); fiscal policy and pricing mechanisms; and compliance and quality issues (ISPE, 2014; Ventola, 2011). Industry concentration also emerges as an underlying driver of many ‘business reasons’ (Weaver, 2010). It appears that concentration, in turn, is linked to the ‘end of patent’ status of certain drugs and the introduction of generics, with concomitant price reduction and resultant product portfolio decisions influencing supply. This seems to be compounded by tendering processes that favour larger suppliers (IMS Health, 2015). While some causes, such as quality and compliance issues, may be reduced through good practice (FDA, 2013; Pew Charitable Trusts and ISPE, 2017), the intertwined nature of a range of causes contributes to increasing the uncertainty of supply. This suggests that only a holistic response will be successful, which involves coordination among, or at least consultation with, multiple stakeholders (Van Bueren et al., 2003).
Emerging policy responses
The first formal high-level regulatory response to pharmaceutical shortages was the US Executive Order 13588 on reducing prescription DSs of 2011 (White House, 2011). This legislative intervention instructed the FDA to broaden the reporting of potential DSs, expedite regulatory reviews and examine whether potential shortages have led to price gouging, while earlier proposals for more hands-on interventions such as creating a national stockpile of drugs or addressing pricing issues in order to alleviate shortages were not followed up (see, e.g, Chabner, 2011). Further Acts included the US DS Prevention Act of 2012 and the Food and Drug Administration Safety and Innovation Act (FDASIA), which allowed for the extension of expiry dates and a relaxation of import regulations (FDA, 2013). More limited measures had been introduced in Germany in 2009, such as amendment 15 to the AMG (medicines law), which focused on manufacturer and wholesaler responsibilities to maintain adequate stock and supplies (Preuschhof, 2009); this is mirrored by Austrian regulations (AGES, 2017). Since 2011, Spanish governmental authorities have undertaken measures to limit the export of medicines from the domestic market due to European parallel trade, but this seems to have had only limited success (Leopold et al., 2014). No comparable legislative measures have been adopted in Ireland (IPU, 2017).
Classification of policy responses
Methodology
One of the main responses to DSs has been the creation of shortages lists by government ministries or arm’s-length organisations. As previously indicated, these lists differ in terms of processes of identification, ownership and, ultimately, the objectives that motivate data collection. Table 1 includes summary data for a number of jurisdictions for which there is a level of comparability. The data were collected by the authors on 12–13 July 2017 from the webpages of agencies that have a recognised responsibility for collecting these data for their respective jurisdiction. Specifically, jurisdictional data were derived from the following sources: for Europe, the EMA; for the US, the FDA; for Germany, the Federal Institute for Drugs and Medical Devices (BfArM in German); for Spain, the Spanish Agency of Medicines and Medical Devices (AEMPS in Spanish); for Austria, the Federal Office for Safety in Health Care (AGES in German); and for Ireland, the Irish Pharmaceutical Union (IPU). In order to account for the fact that some countries excluded vaccines and veterinary medicines while others did not, which would adversely affect data comparability, these were excluded from the analysis for all countries.
Number of DSs listed by jurisdiction/organisation on 12–13 July 2017.

Notes: aExcluding, for all countries, vaccines and veterinary medicines, which were variously included or excluded by individual national/regional shortlists. bInformation not provided.
Exploratory empirical findings
According to this snapshot, the largest number of DSs was listed by Spain’s AEMPS, with 215 shortages, followed by the Irish IPU, with 127 drugs. Next came the US FDA, with 60 listed shortages, followed by the Austrian and German health agencies, with a near-identical number of 28 and 27 shortages, respectively. Coming last, the EMA listed only eight DSs.
Some of these differences are directly attributable to variations in the objectives underpinning data collection. The EMA bases its reporting on information received from member states and only identifies a European shortage when more than one state has reported a drug as being unavailable (EMA, 2013b). The FDA, meanwhile, monitors manufacturers and collates information provided by them. It identifies shortages when, based on information from all manufacturers, the market is not covered. The market is considered covered when supply is available from at least one manufacturer to cover total market demand, which does not preclude the possibility that some manufacturers may not have all presentations available (FDA, 2011). The German regulator also bases its list on information provided by manufacturers, but it supplements this with data from a federal information system. There is a requirement on industry to inform BfArM of drugs where the number of licence-holders, the end-user producer or the active substance producer falls below a critical limit for a particular active ingredient. BfArM also asks industry to report foreseeable bottlenecks without delay, no later than six months in advance (BfArM, 2017). The Spanish regulator, meanwhile, bases its listing on voluntary reports received by both licence-holders and health authorities (AEMPS, 2017). Similar to Germany, Austria relies on a mix of voluntary reporting by licence-holders and legal requirements for this to take place in case of essential medicines (AGES, 2017). The IPU, lastly, has perhaps the most liberal approach to shortages by relying on the voluntary contributions of manufacturers and suppliers (IPU, 2017), with no governmental involvement.
The high count of 215 shortages for Spain can be partly attributed to the fact that this includes clinically essential as well as non-essential pharmaceuticals. This is mirrored by the Irish approach, which gives similar information to the Spanish listing but sorts shortage drugs by manufacturer – without giving additional information on the therapeutic use of drugs, as provided in the Spanish listing. Both approaches contrast with the Austrian and German listings, which, at the time of our analysis, listed only hospital-relevant and/or essential drugs, with a focus on active ingredients. The US approach seemed to fall between these two extremes in that this DS approach listed active ingredients and also identified specific brands, with a focus on drugs that have been identified as clinically relevant by a government agency.
The underlying reasons for these different approaches are difficult to disentangle. In some sense, the Spanish approach, and even more so the Irish approach, seems to lie at the lower end of regulatory input (or administrative reach) in that any medication that is unavailable can enter the shortage list. This would perhaps be expected in the case of Ireland as this is the only jurisdiction in this sample where a DS list is provided by a voluntary professional organisation rather than a ministry. However, this logic would obviously not apply to Spain, where the DS list is compiled by a branch of the Health Ministry. The German and Austrian approaches, by contrast, require a higher degree of regulatory input that focuses on active ingredients or components whose absence could lead to a shortage of hospital-relevant or essential drugs. As such, these two approaches appear to prioritise public health concerns and their centralised management, while potentially paying less attention to the immediate information needs of users. This could again be seen as an expected outcome as, in both cases, branches of the respective health ministries own, collate and manage these lists, together with providing a host of supplementary information. Matters in the US are complicated with regard to ownership, with the FDA controlling and compiling a shortage list while the ASHP plays a key role in advising health-care practitioners with clinically relevant information, including data on potential substitutes.
Each of these approaches, needless to say, has advantages and disadvantages. The Spanish and Irish approaches give a largely unfiltered picture of specific product types that community or hospital pharmacies cannot obtain. This may be useful for health-care practitioners who seek to verify whether a shortage they encounter affects the country more broadly. The US, and to a greater degree Germany and Austria, by contrast, focus on clinically essential drugs. In the case of the US, information is presented primarily from a therapeutic perspective, with a focus on shortages for which there is no immediate substitute and that could therefore adversely affect the health outcomes of patients. The German and Austrian regulators seem to have approached the management of their lists from a similar perspective, while additionally focusing on shortages from the perspective of the ingredient availability level. This is similar to the EMA approach, which additionally imposes the criterion of multi-state unavailability.
It stands to reason that engagement with DSs at the therapeutic level is particularly useful where a regulator seeks to encourage the adoption of mitigation strategies that focus, for instance, on the identification of alternatives, the extension of expiration dates or similar measures. A focus on the ingredient level, lastly, appears to be reflective of a broader, long-term public policy lens, where efforts are made to centrally identify potential future at-risk medicines and to remedy root causes accordingly.
The level of institutional engagement with shortages as a policy issue is also reflected in the way designated jurisdictional organisations provide supplementary information as part of DS lists – albeit that the relationship is not absolute. This is illustrated by Table 2, which is again based on data collected on 12–13 July 2017 for the same set of countries and organisations as shown in Table 1. According to this analysis, most countries provide information on the active ingredient of shortage drugs. The only exceptions to this are the Spanish and Irish listings. In both instances, some of this information may be available via the interface of a number code – which, in the Irish case, represents a reimbursement number. Only a small number of countries – namely, the US, Germany and Austria – give contact details of manufacturers and suppliers of DS pharmaceuticals, and only two countries – Germany and Austria – provide information on potential future shortages.
Characteristics of, and supplementary information given by, DS lists on 12–13 July 2017.

While definitional difference makes comparisons difficult, other studies would suggest that Spain and Ireland, which we identified as the European jurisdictions listing the most pharmaceutical shortages, have indeed been particularly hard hit by DSs (Costelloe et al., 2015; Pauwels et al., 2014). This contrasts with Austria and Germany, which we show as listing a relatively small number of DSs and that past research has identified as being less affected by these pressures (Leopold et al., 2014). No comparable conclusion, meanwhile, can be drawn for the EMA as definitional differences are too pronounced. The US position in between the extremes of low German/Austrian and high Spanish/Irish DS figures reflects a reality of limited successful engagement with DS management.
Analysis
Within this small sample of countries, overall DS management approaches seem to be distinguishable along two dimensions (see Figure 1). The first is the level of salience attributed to DSs, with EMA, Spain and Ireland attributing relatively little urgency or prominence to DSs as a policy issue and Germany, Austria and the US giving DSs major attention. The second is the level of active state involvement with DSs, with the state acting as major policymaker and driver in case of EMA, Spain, Germany and Austria, and the state delegating functions to private agencies and playing a relatively limited role in the case of Ireland and, perhaps to a lesser degree, the US. Accordingly, we find the least developed levels of DS policy among jurisdictions of the third quadrant (Ireland), where both salience and levels of state engagement are low. More evolved levels of DS policy are found in jurisdictions of the first quadrant (EMA, Spain), where salience is low but level of state engagement is more pronounced. A further step up in terms of the development of DS policy can be found for the fourth quadrant (US), where salience is high but levels of active state engagement are relatively low. Lastly, we observe relatively highly evolved DS policies for second-quadrant jurisdictions (Germany, Austria), where both salience and levels of active state engagement are high.
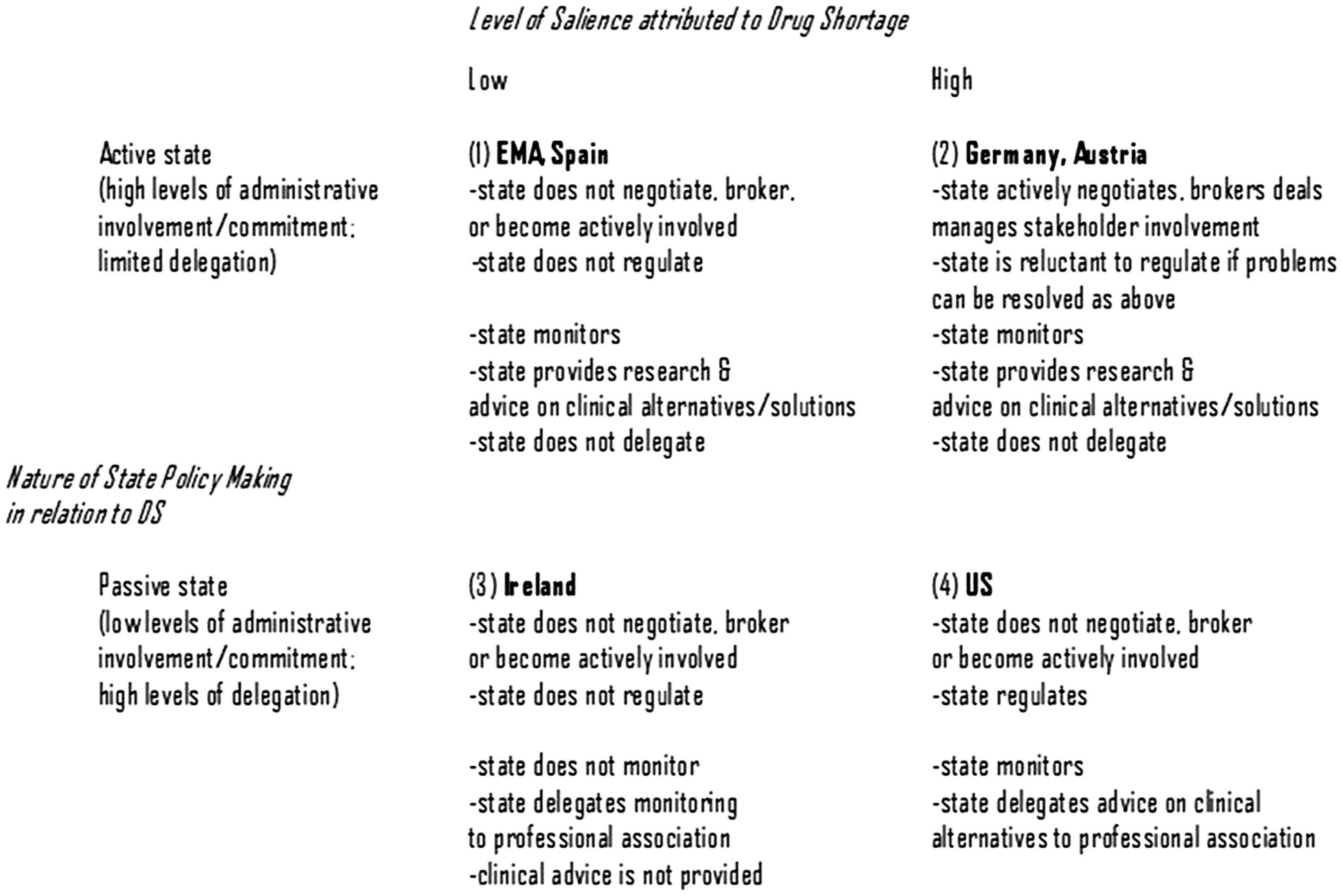
Key dimensions, and jurisdictional types, of DS policy.
These broad policy differences are closely mirrored by the conceptual strategic orientation of DS policy within these jurisdictions, whereby the level at which shortages are perceived, the key perspectives adopted, the time frame towards which solutions are geared and the nature of the response are closely related (see Table 3). Accordingly, in Ireland and Spain, DSs are detected at the individual product level, with individual prescribers playing a major role, while attempts at resolving these problems are largely ad hoc and short term in nature, being typically designed as a reaction to problems as they arise. In the US, by contrast, the focus of DS management is on the level of therapies, and this thinking guides the identification of shortages, while policies focus on the medium term of problem resolution and risk mitigation. The German and Austrian approaches, lastly, seek to identify shortages at the active ingredient level, emphasise long-term solutions and are focused on prevention.
Conceptual framing and strategic orientation of DS policies.
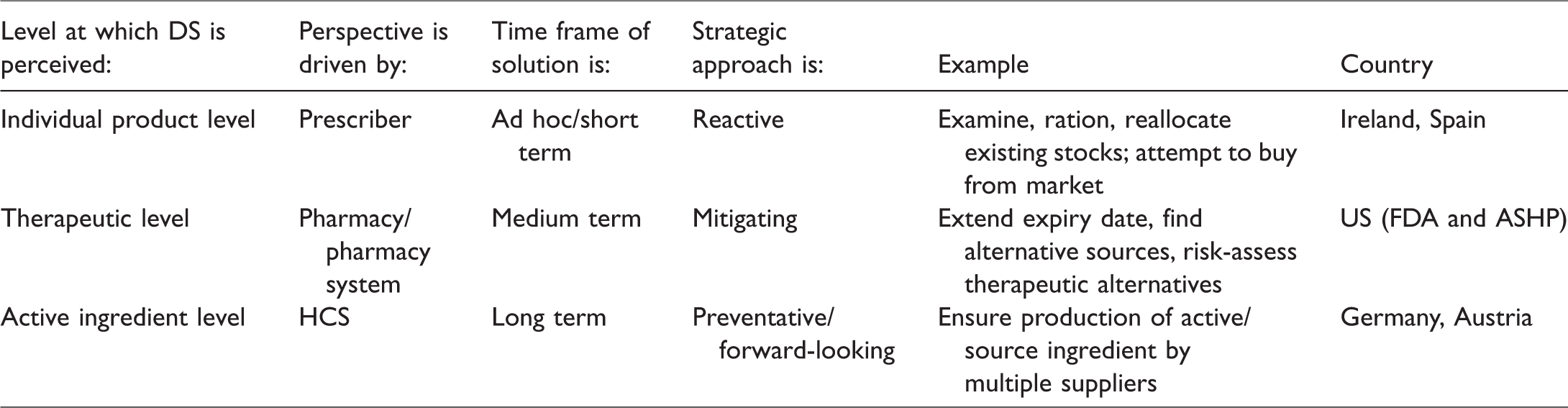
Figure 1 and Table 3 obviously contain an element of simplification, if only because this static analysis does not adequately reflect policy changes and dynamics within each jurisdictional unit. However, the proposed classification is supported by a number of observations at different levels, and can therefore serve as at least a temporary, cross-sectional typology of DS policy.
Discussion
Our analysis confirms the existence of strong path dependence in the adoption of policy responses (Béland, 2010; Feder-Bubis and Chinitz, 2010), which we find manifest in a pronounced typology of pathways where jurisdictional approaches to pharmaceutical shortage management differ along two core dimensions, namely, the salience attributed to the problem and the level at which state organisations engage with the problem. Specifically, we find the US to have attributed a high level of salience to DSs while maintaining a relatively low level of direct state involvement in their management. This contrasts with Germany and Austria, where levels of salience attributed to DSs are also high but where the state has additionally adopted a direct and active role in their management. For the EMA and Spain, we identify a relatively low level of salience in terms of DS problem characterisation, while state organisations maintain a direct and active role in the monitoring and provision of advice on alternatives and substitutes. Ireland represents a case of delegation to a weak arm’s-length professional organisation, where DSs are given low salience and state involvement in their management is virtually non-existent. These patterns are mirrored in the conceptual framing and strategic orientation of the respective DS policies, with: Spanish and Irish DS policies focusing on the individual product level and being largely reactive; US policies focusing on the therapeutic level, with a focus on mitigation; and German and Austrian policies seeking to address the active ingredient level, with a focus on shortage prevention.
Conclusions
This article has sketched out divergent patterns of policymaking in relation to the novel and evolving problems of DSs. Overall, these patterns exhibit strong characteristics of path dependence, with the US approach to DS management reflecting a preference for small government, delegation and legislative solutions, and the German and Austrian approaches signifying a preference for an active, state-resourced involvement of ministries in DS management. This mirrors observations made in connection with the now well-established strong or weak state literature (Atkinson and Coleman, 1989), which observed that these concepts are most appropriately applied to the sectoral level, such as health policy, as some states can be weak in some areas and not in others. At first sight, then, these divergent policy preferences are not new, with the literature on path dependence having highlighted a strong role of legacies in health policymaking in particular. Despite the importance of legacies, we find evidence of innovation, particularly in relation to the US and German approaches, which we explain on the basis of Djelic and Quack’s (2007) prediction that perceived internal crisis can lead to path creation, particularly where external pressures relate to local stakeholders (Djelic and Quack, 2007; Jacobs and Weaver, 2015).
Thus, in the case of the US, delegation is pronounced in that core DS management and communication activities are increasingly resourced and performed by a professional organisation – the ASHP – which, in conjunction with the University of Utah, is providing many functions that the FDA is not resourced or equipped to provide (Fox et al., 2014). This collaboration, however, is also novel in that it involves close cooperation, communication and coordination between the two organisations. Accordingly, this evolving collaboration involves a pattern where information is routinely shared between the FDA and ASHP for posting on the websites of both organisations, while the ASHP is given a wide remit for providing therapeutically and practitioner-relevant information for health-care providers and patients (Fox et al., 2009).
In the German case, meanwhile, the innovation and path creation centres on the jour fixe arrangements introduced in 2013. As a semi-formal meeting of key stakeholders, this involves representatives from a number of permanently participating organisations, including manufacturing, prescribing and overseeing bodies, as well as federal state representatives (BfArM, 2016). While this approach to problem solving or crisis management could be seen as borrowing from the neo-corporatist ‘konzertierte Aktion’ approaches utilised in the context of economic policymaking (Schlecht, 1968) and later in health policymaking (Wiesenthal, 1981), its application to DSs seems far closer to network governance than the negotiation-centred orientation of earlier forums (BfArM, 2016).
Common to both the US and Germany is a widely shared perception of DSs as a major national crisis (BfArM, 2016; Fox et al., 2014). This has been driven, in part, by strong professional organisations in the health-care sector, which have problematised DSs as an urgent national policy issue. In both jurisdictions, clinical professionals have acted as key voices and informers to the public and to governmental organisations. Simultaneously, insurers, hailing either from the heavily individualised US private systems or the increasingly outcome-focused and competitive semi-state German insurance systems, have demanded action on this issue. Meanwhile, in both cases, existing parameters of health-care problem-solving have revealed themselves to be inadequate. This has engendered creative solutions in both jurisdictions, though the German jour fixe arrangement and the comparable approaches of Austria are arguably more holistic and further developed. Reflecting a US preference for small government, reliance on the ASHP offers temporary advantages but potentially lacks in terms of both holism and long-term financial sustainability.
Spain and Ireland have so far experienced a low prioritisation of DSs as a health problem. This may be due to such factors as a recent past of severe austerity (Leopold et al., 2014) and, in the case of Ireland, a high degree of fragmentation of the health system, combined with a significant national economic reliance on the pharma industry (Turner, 2015). Most interestingly, EMA also seems not to have embraced the more advanced approaches developed by the US, Germany and Austria. This could be due to it holding a number of mandates, with DS management being de-prioritised in favour of its role in drug authorisation (Gehring and Krapohl, 2007).
Given the exploratory nature of this article, it may be worthwhile for future research to examine in greater detail the drivers and obstacles that have shaped jurisdictional responses to this important and ongoing contemporary policy challenge. A number of researchers have, like us, investigated initiatives and approaches to the problem of DSs (Bochenek et al., 2018; De Weerdt et al., 2017), and it is likely that the ongoing complexity of the issue will engage researchers for some time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.