
Abstract
Low- and middle-income countries, including Nigeria, are often associated with poor health outcomes, such as the prevalence of human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS). Mother-to-child transmission (MTCT) is a dominant driver of HIV/AIDS in these countries, necessitating the need to prevent such mode of transmission. With the availability of prevention of mother-to-child transmission (PMCTC) services in Anambra State, Nigeria, it becomes important to investigate the utilization of these services. This is needful given the relatively high percentage of vertical transmission in the state. To conduct this study, data were sourced using six focus group discussions involving 15 health workers and 24 HIV-positive mothers selected from three health facilities that dispense PMCTC services. Findings revealed that PMTCT services in the study area had setbacks owing to facility-based inefficiencies, low-level awareness and-coverage of the services at the grass-roots level, weak social support and cultural/religious beliefs, among others. To contain these setbacks, social workers as welfare/human rights professionals were recommended to be engaged.
Keywords
Introduction
The prevalence of human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) among Nigerian children is considered one of the leading causes of Nigeria’s high child mortality rate. The United Nations Programme on HIV/AIDS (UNAIDS, 2016) reported that an estimate of 41,000 children are infected with HIV in Nigeria. However, it is believed that this number could be largely underreported since Nigerians prefer to keep their medical conditions secret, usually for fear of stigmatization (Federal Ministry of Health [FMH], 2007; Igwe et al., 2015). Studies reveal that mother-to-child-transmission (MTCT) remains the most common way through which HIV is transmitted to the child population (Agwu, 2017; Anigilaje et al., 2016; Deressa et al., 2014). MTCT means the spread of HIV from an infected woman to her child, which can also be referred to as vertical or perinatal transmission (Abiodun et al., 2015). This may occur at pregnancy or during the process of delivery. As a result, the issue of prevention of HIV infection from mother to child becomes necessary in health sciences, leading to the conception of prevention of mother-to-child transmission (PMTCT) prophylaxis or services.
Generally, PMTCT as one of the health-protective measures against HIV/AIDS comprises HIV testing and counselling, antenatal care (ANC) services, routine family planning, antiretroviral (ARV) medications and community health sensitizations, among other clinical- and community-centred interventions. A combination of these services is expected to foster decreased paediatric infections, an increased HIV-free population and improved maternal and child health (Abajobir and Zeleke, 2013; World Health Organization [WHO], 2009). In other words, the essence of PMTCT services is to ensure the protection of the foetus or offspring from the virus, while promoting better quality health for the mother. In Nigeria, PMTCT services are domiciled in selected secondary and tertiary health facilities and considered the best health-protective model to promote an HIV-free child population (Nigeria Demographic and Health Survey [NDHS], 2014).
So far, Nigeria has made efforts in curbing the spread of HIV to infants and also sought to implement the United Nations’ resolution of reducing the proportion of infants infected with HIV (UNAIDS, 2002; WHO, 2010). However, these efforts are not enough. Between 2009 and 2015, Nigeria only achieved a 21 percent decline in new child HIV infections (NDHS, 2014). This implies that the country still trails behind in attaining the 2010 United Nations’ resolution on reducing new infant HIV infections by 50 percent (WHO, 2011). Thus, the question of access and utilization of PMTCT services becomes crucial.
The WHO (2009) observed low access and utilization of HIV counselling and testing (HCT), as well as ARV medications among Nigerians (11.7% and 17.1%, respectively). The WHO (2011) recorded an estimate of 210,000 HIV-infected Nigerian pregnant mothers annually, and further reported that only 22 percent of the infected mothers do have access to and equally make use of ARVs in Nigeria. This is further corroborated by UNAIDS (2017), stating that just 32 percent of Nigerian HIV pregnant mothers utilize ARVs. Therefore, it appears that poor utilization of PMTCT services in Nigeria persists (National Agency for Control of AIDS [NACA], 2016). Even across Africa, Nigeria still trails behind. In 2015, Uganda, South Africa and Burundi, respectively, recorded 86 percent, 84 percent and 84 percent in curbing new HIV infections, while Nigeria recorded below 50 percent (Agwu, 2017).
Heedless of the fact that Nigeria adopted PMTCT services in 2001 and has over 7000 healthcare facilities providing the service, the country is yet to record significant success in curbing new HIV infections (Hembah-Hilekaan et al., 2012). It becomes needful to investigate why availability has failed to translate into utilization, and what likely factors could be responsible. A few of the factors, bordering on awareness, stigma and transport difficulties to distant facilities, are mentioned in some studies (Abajobir and Zeleke, 2013; Enwereji and Enwereji, 2010; Iwelunmor et al., 2014; Ogundipe et al., 2017; WHO, 2009). It is against this backdrop that social workers become relevant.
The issue of public health has always taken a multidisciplinary aspect, which is consequent on various professionals being involved in sustaining the health of a population. Studies have shown that professional support is one factor that exercises influence on conformity to acceptable health practices by people (Gourlay et al., 2013; Muchacha and Matsika, 2017; Peng et al., 2017). The issue of MTCT in Nigeria is being marred with barriers alluding to fear, low-level awareness, facility-based inefficiencies, and also stigma and discrimination associated with utilizing PMTCT services (Mepham et al., 2011; Osakwe, 2017; Theilgaard et al., 2011).
Against this backdrop, significant agencies and ministries of the Nigerian government have been expressing concerns in recent times about the spread of HIV through MTCT, and less utilization of PMTCT services (FMH, 2010; NACA, 2016; President’s Emergency Plan for AIDS Relief [PEPFAR], 2010). It is in this vein that the responsibilities of social workers in areas of psychosocial determinants of health, as well as monitoring and evaluation of programmes, stand to be relevant (Bywaters, P and L. Napier, 2008; Okoye, 2019).
Nigeria has a PMTCT programme management which is coordinated by the HIV/AIDS Division in the Public Health Department of the Federal Ministry of Health (Agboghoroma et al., 2015). A snapshot of the technical composite of this management shows exclusion of social workers at the top rank, not minding the existence of the Association of Medical Social Workers of Nigeria (AMSWON). However, at the base, where there are PMTCT site committees for health facilities providing the service, it reads that social workers should be part of the PMTCT site committees (Agboghoroma et al., 2015). Yet the under-employment of social workers at the facility level persists (Cataldo et al., 2017; Onalu et al., 2019). In a case study by Okoye (2013), the employment of non-social workers to take up social work jobs, even in the healthcare setting, was critically discussed as a key challenge for social workers in Nigeria.
The dearth of adequate social workers within healthcare settings in Nigeria cannot be unconnected with issues of recognition and professionalization facing the profession in the country (Ogbonna, 2018; Okoye, 2019). In filling this void in Nigeria’s public health sector concerned with HIV/AIDS, the ‘expert-mothers’ (EMs) model is one that has emerged (Cataldo et al., 2017). This entails engaging mothers who are HIV/AIDS positive and have undertaken PMTCT services for a long time, to render social care services to other infected mothers, and equally act as PMTCT advocates in their communities. EMs are paid a stipend to carry out these services. While this idea is indeed a great one, sustaining it will need the expertise of social workers who are trained in psychosocial care and community work. Social workers can help with identifying the EMs, and likewise monitor and encourage them as they go about their activities.
Generally, with the involvement of social workers within PMTCT management, it is expected that they should advocate for respectful attitudes through civil rights platforms towards utilizers of PMTCT and HIV patients; facilitate the provision of psychosocial support and strengthening of community-based initiatives for HIV mothers in Nigeria; challenge cultural practices and faith-based objections that dehumanize HIV patients; make efforts to include the male population and relatives of the HIV-positive mothers in the web of sensitization and care; monitor funds provided by donors to combat HIV and MTCT and challenge inefficiencies in the health sector that will mar the efficacy of PMTCT services (Muchacha and Matsika, 2017; Okafor et al., 2018; Onwujekwe et al., 2018).
Factors militating against the uptake of PMTCT services in Nigeria have been discussed in studies, with emphasis on awareness, knowledge and the stigma associated with utilizing PMTCT services (Abajobir and Zeleke, 2013; Abiodun et al., 2015; Agboghoroma et al., 2013; Balogun and Odeyemi, 2010; Balogun and Owoaje, 2015; Deressa et al., 2014). However, the studies barely rose over the above-mentioned factors that influence the utilization of PMTCT services, and did not include the need to involve social workers in the framework. We sought to unearth these factors using a qualitative study involving health workers and HIV-positive mothers, because the stakeholders were the primary source of the information that would answer the research questions and this qualitative format would allow the participants to freely narrate their experiences. The following research questions guided the study: To what extent are community members aware of PMTCT services? What is the state of utilization of PMTCT services in the study area? What are the factors affecting the utilization of PMTCT services? What roles can social workers play to increase efficiency and patronage of PMTCT services? It is believed that our findings will provide information to international and local campaigns that promote the utilization of PMTCT services, as well as stimulate measures to combat militating factors.
Materials and methods
Study area
The study area is Anambra South Senatorial Zone, which is one of the three senatorial zones in Anambra State. The state is located in the southeast geopolitical zone of Nigeria. Anambra State had a population of 4,418,032 as at the 2006 national census. With a 2.8 percent annual growth rate, the population of the state as at 2017 when the study was done stood at 5,986,226. Women of childbearing age constitute about 25 percent of the population (National Population Commission, 2010). The prevalence rate of HIV/AIDS in Anambra State as at 2014 stood at 8.7 percent, which is the fourth highest in the country (Chukindi, 2014; NACA, 2016). Of the prevalence rate in the state, vertical transmission constitutes about 4 percent (Anambra State Ministry of Health, 2013). The Anambra State Ministry of Health (2013) listed a total of 1485 health facilities in the state, of which 1153 provide ANC services, with just 63 of them providing ARVs for PMTCT, while only one provides polymerase chain reaction (PCR) testing for early infant diagnosis (EID) of HIV. To this end, the prevalence rate of HIV and MTCT in the state, as well as the limited scope of PMTCT services, justifies the focus of our study on Anambra State, with particular reference to Anambra South Senatorial Zone.
Sampling procedure
Using a purposive sampling technique, the researchers selected three hospitals from Anambra South Senatorial Zone, Anambra State. The three hospitals were purposively selected because these were the only hospitals in Anambra South Senatorial Zone that provide ARV drugs and PMTCT. The selected hospitals were Nnamdi Azikiwe Teaching Hospital (NAUTH), Nnewi, Our Lady of Lourdes Hospital, Ihiala, and Trauma Center, Oba. With the help of the Chief Medical Directors (CMDs) of the selected hospitals, five health workers and eight HIV-positive mothers of reproductive age were purposively selected from each of the hospitals. On the whole, 15 health workers inclusive of 3 social workers and 24 HIV-positive mothers participated in the study. The recommendation by the CMDs of just one social worker per facility, in addition to the complaints of the focus group discussion (FGD) participants that social workers are barely employed, is a reflection of the poor recognition of the social work profession in Nigeria (Ogbonna, 2018; Okoye, 2013, 2019; Onalu et al., 2019). It is important to state that there is no record of the number of social workers in Anambra State, nor in Nigeria. State-level associations of social workers in Nigeria are silent, and those at the national level are still in the process of gaining strong recognition.
Finally, participants for the FGD were recruited based on convenience and willingness to participate. Health workers were recruited on the basis of affiliation with units concerned with HIV/AIDS patients, such as obstetrics/gynaecology, community medicine, social welfare and infectious disease units. For the mothers, given the objectives of the study, we recruited reproductive-active mothers who are HIV/AIDS positive and have ever been in receipt of PMTCT services from the facilities we visited.
Data collection
Discussion sessions were conducted in the three hospitals. Respondents first gave their oral consent and participated willingly, having understood the aims of the research. The discussions comprised two differently categorized FGDs (health workers alone and HIV-positive mothers alone) in each of the facilities. The FGDs were conducted in November and December 2017. Based on the permission of respondents, discussions were recorded with an electronic recorder, while a note-taker took notes. The authors shared responsibilities among themselves, involving the FGD facilitator, note-taker and recorder. All authors were proficient in the Igbo language since it was used alongside the English language to communicate. Cost-effective reasons influenced the decision of the authors to disregard the use of research assistants. The research instruments (FGD guides for health workers and HIV-positive mothers) were collectively developed by the researchers. The instruments were pretested using an FGD session organized for health workers and a simulated group of HIV-positive mothers (mothers who are aware of PMTCT services and pretended to be HIV positive) from a health facility in the Capital of Enugu State, Nigeria. The researchers could only have access to a simulated group since the process of recruiting real HIV-positive mothers in Enugu State would entail ethical clearance, for which the researchers could only afford just one, which was used for the main study. Nevertheless, the pre-test occasioned some sense of reliability, in that unclear questions were spotted and those needing more probes were highlighted.
Data analysis
The data collected were transcribed in the English language by an expert in the Department of Linguistics, Nnamdi Azikiwe University, Awka. The transcribed discussions were compared with the notes taken, to ensure that no response was lost. The transcribed data were arranged in themes with the aid of NVivo9 software. The rationale behind the use of themes was to help with classifying responses. Themes were collectively developed after we modified the research questions as a result of experiences from the field. This alludes to grounded theory in research (Barbie, 2010). The researchers equally adopted peer debriefing and observer triangulation (Padgett, 2008). Using observer triangulation, the researchers ran the analysis independently on an already collectively designed analysis template in NVivo9 software. Later, a collective analysis was completed, making sure quotes and themes were appropriately matched. On peer debriefing, the collated analysis spreadsheet was given to two peers who made revisions. The FGD guide and the concept note of the study assisted the peers. After the rigours were followed, the data were categorized into two major themes, which are (a) evidence of weak utilization of PMTCT services and (b) factors necessitating weak utilization of PMTCT services.
Ethical approval
The study instrument and methodology was reviewed and approved (IRB00002323) by the Ethical Review Board of the Nnamdi Azikiwe Teaching Hospital Nnewi.
Results
We begin presenting our results by first describing a summary of the demographic features of the participants. Second, we present evidence to show weak utilization of PMTCT services, before presenting militating factors, which point out the need for social workers.
Demographic characteristics of participants
All participants of both groups were of the Igbo tribe, but seven stated they were from other Nigerian tribes. Ages of the participants ranged from 21 to 49 years. Just 7.7 percent of all participants had no formal education, that is, they never had primary, secondary or tertiary education. For the HIV-positive mothers’ group, 54.2 percent of the participants had nursed more than one baby, and 66.6 percent of them gave birth to children who are HIV negative. Just 2 percent of the participants were housewives, as virtually all the participants were engaged in farming, civil service, vocational occupations or trades.
Evidencing community awareness and poor utilization of PMTCT services
The participants understood the meaning of PMTCT. They saw it as the prevention of passing the HIV virus from a mother to her child during pregnancy, labour, delivery or breastfeeding. A 32-year-old mother said, To my own understanding, PMTCT means prevention of passing HIV virus from a mother to her child during pregnancy, labour, delivery, and childbirth. When you utilize PMTCT services, listen to PMTCT programmes and talks, they make you know more about PMTCT services, how to prevent and protect your child from contracting the virus. When you go for treatment and obey all the instructions given to you starting from the first day of conception till the day of delivery and during breastfeeding, your child will never contract the virus, just like my children.
Another mother added that ‘PMTCT provides antiretroviral treatment (ART) to HIV pregnant women to stop their infants from acquiring the virus’.
Heedless of the positive responses we received from participants regarding understanding what PMTCT services are, utilization was found to be weak. Some participants mentioned that they were newly introduced to the service, owing to the absence of PMTCT services at the Primary Healthcare Centres (PHCs) they visited. PHCs are closest to the grass-roots level, and they do not provide PMTCT services. The implication is that the patients would have to visit the secondary or tertiary facilities where PMTCT services are domiciled. Participants complained of the transport costs they incur, which diminishes their chances of utilizing the services. As a mother narrated below, It was just last month when I registered for antenatal care service in the health centre in my home town that it was dictated that I am HIV positive and was referred to this hospital for treatment. So, this is my first time of coming here for treatment and everything you people are saying here is strange to me.
Another, 45-year-old mother added, There is no PMTCT centre in my area. If I want to go for treatment, it will cost me 1,000Naira [$3] to transport myself from my village down to the Teaching Hospital. For example, between January and February this year, I couldn’t come for treatment because there was an increment in the price of fuel, which increased transport fare thrice the usual amount.
While coverage was found to be an issue accounting for weak utilization of PMTCT services, participants still felt that more work should be done in scaling up the awareness of PMTCT services. A doctor recounted his experience: I had this patient who never knew she was HIV positive until when she got pregnant and came for antenatal care. It was very surprising that she registered for antenatal care in the 6th month of her pregnancy. It was too late. Sadly, the baby had contracted the virus and there is nothing anybody can do about it.
A 25-year-old mother further commented, ‘if not for my friend who is a staff of this hospital, I wouldn’t have known about this service’.
Specific factors influencing the utilization of PMTCT services
The weak utilization of PMTCT services hinged on coverage and awareness as findings have shown. However, there are other factors that influence the utilization of PMTCT services, and they include (a) cultural and religious barriers; (b) social support systems; (c) facility-based inefficiencies. We present data explaining these factors below.
Cultural and religious barriers
Findings from the study show the connection between cultural and religious beliefs and the utilization of PMTCT services. The belief by Christians that prayers to God could heal them featured strongly across the quotes of participants. A health worker said, . . . I once had a client who used to come to the general hospital for treatment, but for some time now, she stopped. She told me that her pastor prayed for her and told her that God has healed her that she should not go for any treatment again nor take any drug. Can you imagine?
A 23-year-old mother corroborated the above assertion: I was once a victim of religious belief. I stopped going for treatment because I believed that God will deliver me from this disease. But with what happened to me last year (perennial crisis), nobody preached to me. I went back to the hospital for treatment myself.
The traditional practice of using traditional herbs to combat illnesses and the patronage of traditional birth attendants were reported to likewise encourage weak utilization of PMTCT services. A 48-year-old mother said, ‘my friend once told me to stop orthodox medicine and go for traditional herbs, that they are better. I almost listened to her. Thank God I discussed with one of the workers here who talked sense into me’.
Furthermore, a 35-year-old mother sadly narrated, In my own case, I gave birth three weeks before my due date. The labour started around 1.00am. I had to call a traditional birth attendant. And you know the health centre is very far from my home town. As a result of this, I missed out on the drugs which were supposed to be taken during labour and after delivery. By the time I could take my child to the health centre the next day for Nevirapine (NVP) prophylaxis syrup, I got the news . . . She was already HIV positive. I cried my eyes out . . .
Finally, the stigma placed on HIV/AIDS patients as ingrained in the culture of the study area deterred HIV-positive mothers from giving birth in facilities where they were diagnosed. They did so to avoid stigma from their relatives and husbands, who are compelled by culture to be with them at the point of child delivery. They said that their status would eventually be in the open by the time the health workers were putting them through the PMTCT medications right before their husbands and relatives. The quote below by a 41-year-old mother reveals further: It is in our culture that the husband or any of the relatives of the pregnant woman has to be present during labour. Any HIV positive mother who doesn’t want people to know her HIV status may avoid returning to the facility where she was diagnosed, and would instead prefer a traditional birth attendant, or deliver in a facility where nobody would know her status.
Social support system
Participants revealed the relationship between support networks’ encouragement or discouragement and their compliance with PMTCT services. One of the HIV-positive women who was 28 years old talked about the encouragement she gets from her husband. She said, . . . Since I started coming for treatment here, doing everything they ask us to do, I look healthier . . . My husband reminds me to take my drugs. Though, his concern is the child in my womb because we have been married for the past seven years and no issue. So my husband is doing everything within his reach to ensure that the baby in the womb is safe and that I should also be strong to take care of the baby. He makes sure that I take my drugs as and when due.
Adding to the above, another 23-year-old mother said, ‘My family people know I am HIV positive, though they hide it from non-family members. My mother especially reminds me not to give up. She sometimes helps to pay for my antiretroviral medications’.
On the contrary, a 37-year-old mother said, I have really suffered in the hands of my husband. He has refused to check his status in my presence. He keeps insulting me because I am HIV positive. Because of this, I don’t feel motivated to come for PMTCT, but for the sake of this child, I try . . .
In order to complement support networks, health facilities organize support groups comprising HIV-positive patients. Members of the support groups share experiences, which serve as a motivation for the mothers, especially those who lack support from their homes. One of the mothers said, I got to know the details of PMTCT because one of the health workers placed me in a support group. I was encouraged because I discovered I am not the only one with the problem. I am sure that my child will not contract the virus because of all I learned from those who started using the services before me . . .
Facility-based inefficiencies
Weak utilization of PMTCT services is also encouraged by certain inefficiencies we found obtainable in the health setting. The first, as mentioned, was the dearth of social workers and public health professionals in the health setting. These professionals, particularly the social workers, are supposed to champion awareness promotion of PMTCT services, facilitate sessions for support groups, as well as protect disempowered individuals and assist them in keeping up with utilizing PMTCT services. One of the health workers commented that ‘People are yet to know the usefulness of PMTCT services. In an ideal setting, social workers and public health professionals would go into communities or use the media to enlighten people’.
Another health worker added, ‘You don’t expect me as the doctor to treat and still do some other social jobs like helping patients to raise money for ARV or facilitate counselling sections. Health management should employ enough social workers because we need them’.
Second, the cost of ARV medications expected to be relatively cheap was challenging for the patients and affected their utilization of PMTCT services. The fact that there are no professionals to help patients fight for their rights in accessing these services relatively for free makes matters worse. Thus, some health workers take advantage of the stigma experienced by the HIV patients to sell the ARV medications to them at exorbitant prices. Sometimes, they even create artificial scarcity, so that the price can soar. One of the health workers said, We all know that ARV medications are free or at best subsidized by the government or donor bodies, so patients can pay little amount. In PEPFAR [President’s Emergency Plan for AIDS Relief] project centres, they are outright free. But the truth is that some patients are not aware of this. So because of the stigma on HIV positive patients, they secretly liaise with some doctors who sneak out the drugs from facilities and sell to them at exorbitant prices. Of course, the patient will prefer buying at an exorbitant price than being stigmatized.
A different health worker added, Sometimes, facilities could create artificial stock-outs of ARV to increase demand which would shoot up the price and make people buy exorbitantly from their private clinics which they will refer them to. I know of a case where this lasted for eight months. How then do you expect PMTCT to be effective?
Finally, another facility-based inefficiency found is that the mothers complained of their status not being effectively protected by the health workers. They wished to have effective mediums who can receive their complaints regarding the poor treatment within their neighbourhoods. We feel that an effective social service centre within healthcare facilities could be one of such mediums. The quote below reveals further: If someone talks to me anyhow because I am HIV positive, who will I meet? Some of my neighbours got to know I am HIV positive because they saw me in this hospital doing PMTCT. Are there no ways our identity can be protected? The stigma is too much.
For further illustration of the data presented under the themes in this section, Figure 1 below makes a succinct description, further highlighting the need for social workers in the PMTCT framework.
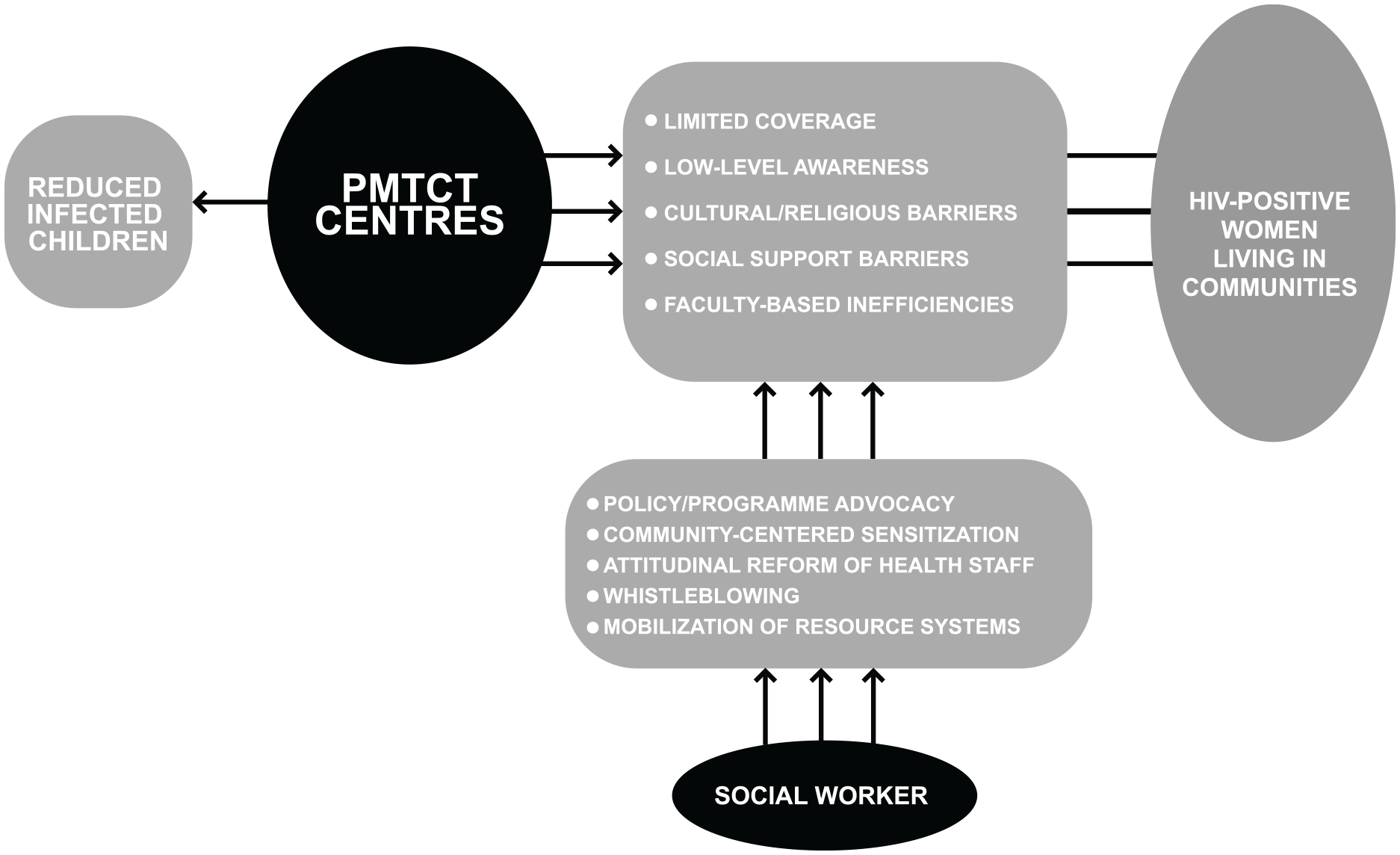
Snapshot of barriers preventing utilization of PMTCT services and hypothesized roles of social workers in Nigeria.
Discussion
The study investigated the utilization of PMTCT services in Anambra South Senatorial Zone and practice considerations for social workers in Nigeria. In this study, findings reveal that the participants have a good knowledge of PMTCT services. They were aware that PMTCT services provided preventive measures of passing HIV virus from a mother to her child during pregnancy, labour, delivery or breastfeeding. However, utilization of PMTCT services in the study area was poor. Participants broadly attributed poor utilization to coverage and low-level awareness.
On coverage, the participants complained about the long distance between them and the health facilities that provide PMTCT services. In Nigeria, PHCs are the closest to the grass-roots level. Pregnant women in most communities utilize the PHCs more than the secondary and tertiary facilities. Most often, they visit secondary and tertiary facilities on referrals from the PHCs. The participating women felt that it would be convenient for them if PHCs could provide PMTCT services, as this would not just be cost-effective for them in terms of transport cost, but would encourage awareness about PMTCT services in the communities since community members are more familiar with PHCs than facilities at secondary and tertiary levels. Therefore, the need to encourage and establish the provisions of PMTCT services at PHCs would help improve coverage, awareness and utilization of the services. Social workers could help with this advocacy, and where this is not forthcoming, they could help facilitate transportation services to and from the PMTCT centres. This hypothesized role would certainly boost PMTCT service coverage. Studies abound that show the relationship between health service coverage and effective utilization (Abajobir and Zeleke, 2013; Laar et al., 2009).
We further investigated some specific factors that account for poor utilization of PMTCT services. These specific factors have been categorized into cultural/religious factors, social support influence and facility-based inefficiencies. On the first, we discovered the connection between utilization of PMTCT services and certain cultural and religious inclinations or practices. Findings show that respondents fell short of utilizing PMTCT services because their pastors gave them the hope of being HIV free after they had prayed to God. Others felt that traditional herbs would best take care of their ailment, which eventually was not the case. It was equally discovered that respondents who hold to the culture of patronizing traditional birth attendants risked their babies acquiring the virus. However, while patronizing traditional birth attendants could be a cultural practice of child delivery in the study area, the long distance between communities and facilities that provide PMTCT left them with the option of patronizing the traditional birth attendants who obviously lack the wherewithal to prevent vertical transmission. Some might not want to go to the PHCs close to them because they would want to hide their status for fear of stigma, which is another reason they patronize traditional birth attendants. Here comes the importance of public sensitization – a role so natural to social workers (Okoye, 2019): the aims of this role are to promote understanding about HIV/AIDS, and reduce the stigma and discrimination associated with the ailment which is considered a major barrier to utilizing PMTCT services. Some studies have tried to establish that certain religious and cultural influences can have an effect on poor health outcomes (Balogun and Odeyemi, 2010; Irin, 2008; Laar et al., 2009; Mepham et al., 2011; Peng et al., 2017; Shah et al., 2007).
Second, encouragement or discouragement received from husbands and other family members consequently reflect on the utilization or non-utilization of PMTCT services. We discovered that some support networks tend to be interested in saving the child, and for the child’s sake will encourage the mother to utilize PMTCT services. Also, women whose husbands refuse to check their HIV status felt reluctant to uptake or continue PMTCT services. Nevertheless, the need to save their babies spurs them to utilize PMTCT services. In this vein, a strong recommendation is put forward to ensure that campaigns for PMTCT services, among other HIV-related campaigns, do well to capture the attention of spouses and other family members of HIV-infected mothers. In fact, such campaigns should be community-wide. The influence of support networks on health outcomes can be found in some studies (Agboghoroma et al., 2013; Anambra State Ministry of Health, 2013; Deressa et al., 2014; Hembah-Hilekaan et al., 2012).
In addition, findings reveal that support groups consisting of women who utilize PMTCT services should be encouraged, so as to motivate and bring to the knowledge of other infected women the need to utilize PMTCT services. This will also give them a sense of understanding that they are not alone in the exercise. This is akin to the ‘expert-mothers (EMs)’ model, where HIV-positive mothers are paid to connect with mothers who are infected, for the purpose of helping them to cope with the ailment and encouraging those who are pregnant to seriously pay attention to PMTCT services (Cataldo et al., 2017). The efficacy of support groups in bolstering positive health behaviours is documented in the literature (Emma-Echiegu et al., 2014; FMH, 2007; Muchacha and Matsika, 2017).
Finally, inefficiencies and poor practice obtainable in facilities that provide PMTCT posed a challenge to the utilization of the services. Participants, including health workers, lamented gaps that can be closed only if social workers and public health professionals are sufficiently employed. They mentioned the need to monitor pricing and disbursement of ARV medications, which are diverted or stolen for private sales at outrageous prices. Thus, the need for whistleblowing in order to apprehend fraudsters, as well as combatting artificial stock-outs, could be championed by social workers. Corroborating the irregularities that mar effective distribution of ARV medications are Adegboyega and Abdulkareem (2012). They narrated that in 2008, benzyl benzoate, which is required by HIV patients and sold for 200 naira per unit, was claimed to have been bought by officials of the Nigerian Health Ministry from some facilities for 119,000 naira per unit (about 55,000% higher than the actual market price). Similar irregularities tend to have clamped on the humane face and efficacy of PMTCT, and preponderantly affect the poor. Given the social justice focus of social workers, confronting such issues falls within the purview of the profession. In addition to whistleblowing, advocacy for strong policies including stiff sanctions on those who compromise the objectives of PMTCT services could be championed by social workers through civil society organizations and human rights groups. Social workers can participate proactively in attitudinal reforms of healthcare staff so they desist from all forms of irregularities in dispensing ARV medications. This can be achieved through management review groups, short courses, patient support groups and seminars/workshops.
In conclusion, other facility-based and health system inefficiencies that social workers can help contain include protecting the image and rights of HIV-positive patients, promoting community-based awareness about PMTCT services across all members of the community, facilitating support groups and other resource systems for infected persons, and ensuring accountability of donors’ funds for curbing HIV generally in Nigeria. Such gaps in the health sector signal more inclusion of social workers, and especially the professionalization of the social work occupation in Nigeria. All in all, the relationship between psychosocial determinants of health – an area of social work practice – and compliance with positive health behaviours cannot be overemphasized (Emma-Echiegu et al., 2014; Igwe et al., 2015; Okafor et al., 2018; Theilgaard et al., 2011).
Finally, the study was not void of limitations. The limited sample being restricted to just a senatorial district is one, therefore the researchers encourage similar studies in other parts of Nigeria. The fact that support networks were not captured in this study accounts for just a one-sided perspective. Hence, subsequent studies would do well to include close relatives of HIV/AIDS patients in the sampling frame. Future studies should consider exploring determinants and consequences of male involvement in the uptake of PMTCT services and the perceptions women hold towards PMTCT services. Such findings will provide more insights into concerns that will scale up the efficiency and uptake of PMTCT services, which would further strengthen efforts towards achieving global health goals. More so, due to the sensitive nature of the study, researchers were very careful with some questions that elicited heightened emotional responses and flashbacks. Where necessary, they completely avoided such questions. This notwithstanding, the ethical review board helped to ensure that questions were ethically compliant. Regardless of these limitations, findings from this study remain relevant to ministries of health in Nigeria, health policymakers and providers in Nigeria, HIV/AIDS organizations, social workers and public health professionals, and donor agencies, all of whom are concertedly making efforts to curb HIV/AIDS and child mortality in Nigeria as well as improve the efficacy of PMTCT in the country.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.