
Abstract
Children with disabilities and their families often experience life circumstances that lead to reduced quality of life in low- and middle-income countries. This article describes the development of a curriculum to train community volunteers to provide support to families of children with disabilities in Lusaka, Zambia, using feedback from an advisory board of local stakeholders. Stakeholders had two opportunities to offer input on the curriculum. Reviewer comments focused on three themes – making the manual more Zambian, needing additional content, and simplifying the message. Recommendations were incorporated into the manual – allowing for culturally appropriate alignment with Zambian needs and customs.
Keywords
The World Health Organization (WHO) and World Bank (2011) estimate that 93 million children worldwide between the ages of 0 and 15 have a moderate to severe disability, with higher proportions of disability reported in low- and middle-income countries (LMIC) (Maulik et al., 2011; Scior, 2016). In Zambia, the Community Development Mother and Child Health Division identified a prevalence rate of disability between 7.2 percent and 13.0 percent (Better Care Network, 2016). The causes of disability in Zambia are myriad, including malnutrition, injury, infectious disease, congenital birth anomalies, other anomalies during childbirth, and non-infectious disease (Central Statistical Office, 2018). The aims of this article are to describe the practice experiences of a pilot program in Lusaka, Zambia, where stakeholders used inclusive program development practices to obtain feedback for a curriculum designed to train local community volunteers to support families of children with disabilities. Reviews from the diverse advisory board allowed for curriculum alignment with local considerations and cultural relevance, which is consistent with implementation process strategies that seek to engage stakeholders and adapt interventions to meet local contexts (Leeman et al., 2017; Meyers et al., 2012).
Impact of having a child with a disability
In LMIC, caring for a child with a disability (CWD) is often inseparable from the experience of socioeconomic hardship. Stigma, or pejorative beliefs and prejudices about people with disabilities, leads to loss of status and disempowerment (Scior, 2016; Seewooruttun and Scior, 2014). Stigma associated with the birth of a CWD can prompt fathers to leave the family – placing mothers in the position of providing sole care to the child (Aldersey, 2012; Ditchman et al., 2016; Maswani-Mwale et al., 2016). Caregivers of children with disabilities identify stigma from community members as a source of upsetting emotions (Gona et al., 2011; Hartley et al., 2005; Van der Mark et al., 2017). Also, CWD and their caregivers often experience exclusion from their community, leading to increased levels of social isolation (Better Care Network, 2016; Tilahun et al., 2016; UNICEF, 2013; Zuurmond et al., 2019).
The healthcare system, an important point of support and assistance for parents of CWD, can also be unresponsive. In a study completed in the low-income community of Kilifi, Kenya, Gona and colleagues (2011) found that healthcare professionals gave minimal information to parents. Parents experienced difficulty accessing rehabilitation services for their children (Bright et al., 2018; Magnusson et al., 2019). In Zambia, limited access to medical rehabilitation and assistive devices represents another service delivery challenge (Central Statistical Office, 2018).
Recognizing the gaps in services and the suboptimal quality of life for individuals with disabilities, the United Nations (UN) ratified the Convention on the Rights of Persons with Disabilities (CRPD) in 2008, which unequivocally established ‘human rights and fundamental freedoms’ (UN, 2008, article 1). To accomplish these rights, the UN advocated for increased programs, awareness, and enhanced social support for people with disabilities. Zambia became a signatory to the CRPD in 2010, affirming the rights of people with disabilities in their country (UN, 2019). Yet in a recent systematic review, Yousafzai and colleagues (2014) identified only six published community-based intervention studies for CWD in LMIC from 2000 to 2014.
Constructing a pilot program
To create a more supportive environment for CWD and their caregivers, a team consisting of a local organization and faculty from the United States created the Kusamala+ program, meaning ‘caring for’ in the local language of Chewa/Nyanja. This collaborative consisted of a multidisciplinary team, including a physician assistant, and public health, physical therapy, occupational therapy, and social work professionals from a Midwestern university, located in the United States, and Catholic Medical Mission Board – Zambia (CMMB-Zambia). Embedded in Zambia for over 35 years, CMMB-Zambia uses a multifaceted approach to impact change by leveraging resources, structures, and systems, creating strong networks among service providers, and promoting horizontal learning among vulnerable families. This 2-year pilot project seeks to evaluate the effectiveness of an intervention program to provide support for CWD and their caregivers. Kusamala+ emphasizes innovation by using an ecological framework to improve the quality of life for families of CWD living in two large urban compounds, or unplanned communities, in Lusaka, Zambia: Kanyama and Misisis. The ecological perspective recognizes transactions between people and their environment as essential determinants for whether individuals thrive or experience stress (Gitterman and Germain, 2008). The ecological framework creates impact through providing additional environmental changes, supporting families of CWD, enhancing system linkages, challenging community beliefs to be more accepting of CWD, and building social support for these families. At its core, this program seeks to enhance support to families of CWD through workforce development of community volunteers who conduct home visits with families of CWD. This article describes the use of inclusive program design and implementation research methods to develop a training of trainer (ToT) curriculum and manual used in the intervention program to educate and equip community volunteers with the knowledge and skills to effectively support families of CWD.
Implementation research is a growing field of interest. Leeman et al. (2017) noted that previous research and practice emphasized a top-down approach where implementors ‘pushed’ models into practice. They emphasized the need to apply a more collaborative approach that encourages local capability to adapt interventions to meet community needs. Meyer and colleagues (2012) outlined an implementation process that involves four iterative phases, with the first phase including decisions about adapting innovations to local contexts. Meyer et al. suggest asking the following questions: Should an innovation be changed to suit the local context? What feedback can the local staff offer to make the intervention more effective in this setting? This article seeks to describe the practice of seeking feedback to adapt an intervention to fit the context in Zambia.
Background for curriculum development
Two organizations – one academic (a Midwestern university from the United States), the other an international faith-based non-governmental organization (NGO), CMMB-Zambia – partnered to develop and implement the Kusamala+ program. A multidisciplinary faculty team developing the Kusamala+ program completed a needs assessment in 2016 to understand the conditions of CWD in Zambia. Assessment outcomes revealed that families of CWD have limited access to health services and rehabilitation, experience considerable stigma about having a CWD, and face heightened risk of living in poverty. However, there were other efforts underway that sought to increase the rights of individuals with disabilities, such as an active Zambian self-advocacy organization (Zambian Agency for Persons with Disabilities), governmental officials supportive of change, and numerous local NGOs interested in developing community-based programming.
During the 2016 visit, faculty members were introduced to an international NGO, CMMB-Zambia, whose mission is to provide locally sustainable strategies for improved health outcomes of women and children. Both participating organizations recognized the potential of integrating their collective skills to complete a project of this scope, while also appreciating the difficulty of collaboratively developing this project with two international partners. Together, these organizations developed a collaboration that seeks to improve the lives of CWD and their families in Zambia.
Developing the home-visiting model
As previously noted, Kusamala+ proposed the use of a home-visiting model where community volunteers visit families of CWD to provide information, emotional support, and referrals. These volunteers did not have any formal education or skills focused on improved access and delivery of quality services for CWDs, despite most of them having been volunteers in community health clinics and involved in activities such as HIV/AIDS awareness; therefore, program developers decided on a ToT strategy allowing for sustainability. Medical and rehabilitation staff from the two pilot communities would receive in-person training from university faculty, then instruct the community volunteers using the developed curriculum. The curriculum sought to develop knowledge and skills related to stigma and language around disability, typical child development, recognition of problems and early intervention, disease prevention, and skills related to caring for CWD to increased independence and quality of life. Each of these topics was presented in individual modules, each with their own learning goals, specific content, and interactive activities to reinforce learning. The multidisciplinary faculty partners each developed curriculum modules related to their discipline. Figure 1 provides a concept map of the topics covered in the curriculum and corresponding ToT manual.
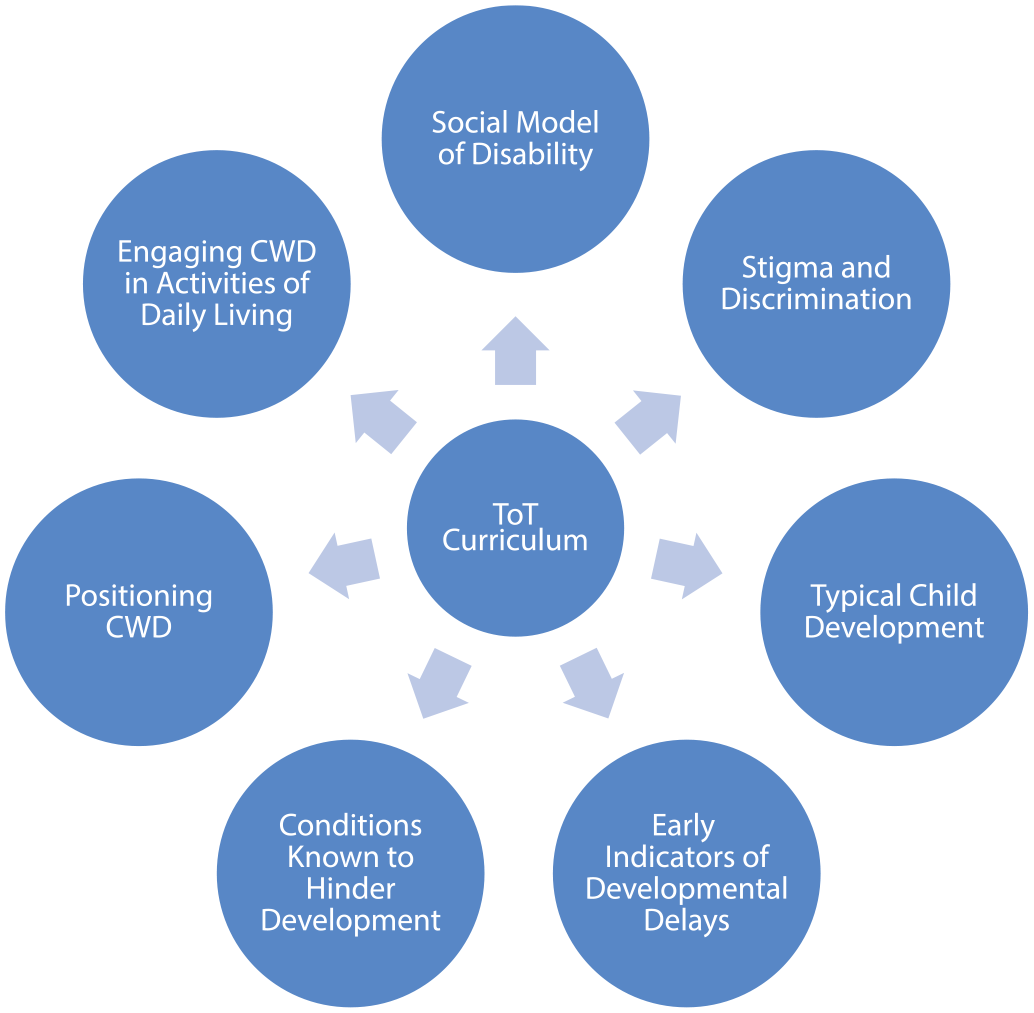
Concept map for training of trainer (ToT) curriculum.
Use of advisory boards to review the curriculum
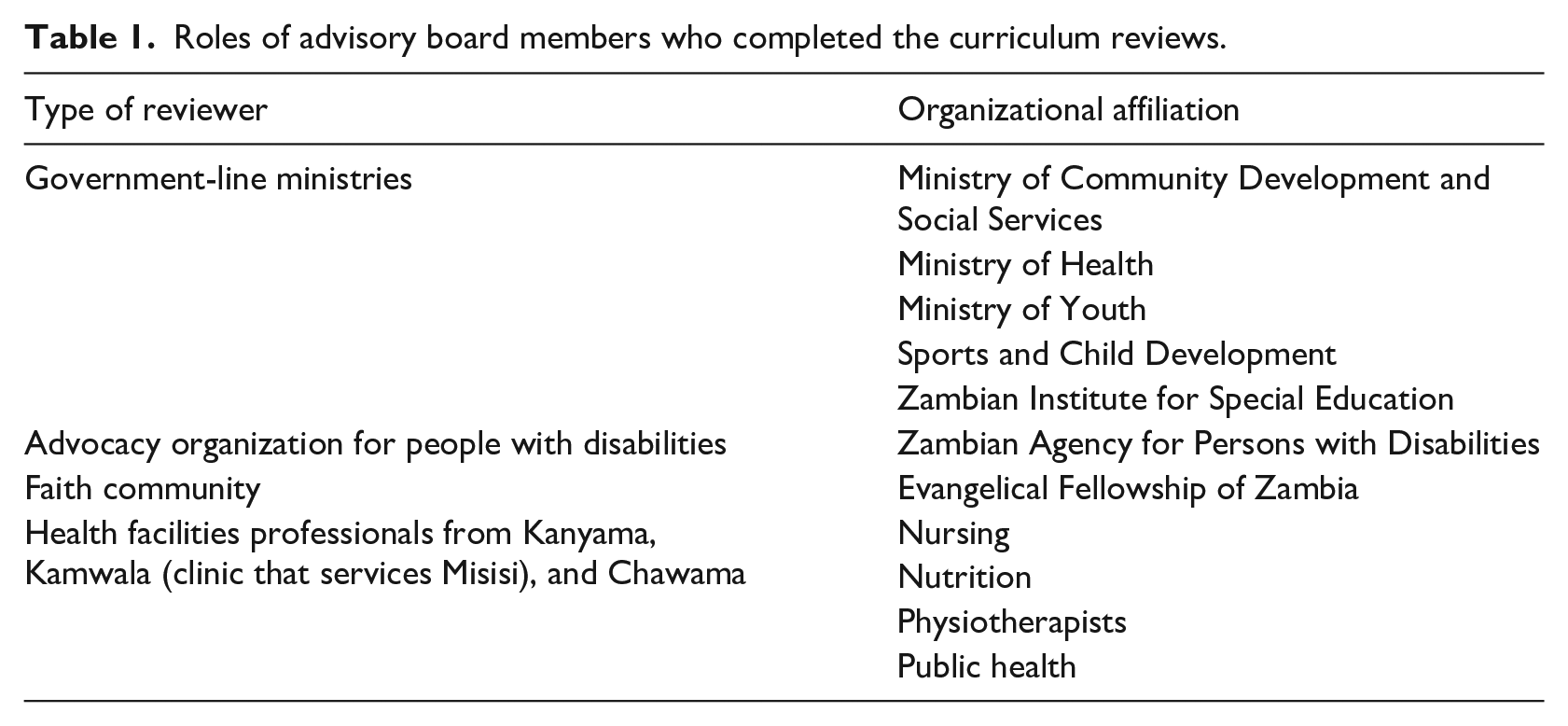
Using advisory boards, or representatives from multiple perspectives, to provide input and advise is one recommended strategy for implementation research (Powell et al., 2015). To ensure that the materials developed are consistent with Zambian context, CMMB-Zambia and university faculty sought feedback and input from various stakeholders to recommend adjusting, improving and/or aligning the curriculum. These local networks, which the in-country partner fostered, included members from diverse organizations to review the curriculum. Individuals identified as curriculum reviewers had professional training or expertise in working with vulnerable families or individuals with disabilities. Table 1 includes a list of the various government line ministries, an advocacy group, a faith-based organization, and multidisciplinary health professionals from the health facilities in the two pilot-project communities that comprised the stakeholder group. Typically, two government representatives were present for the reviews, while only one individual participated from the other organizations, including the health clinics, for a total of 15 participants in the advisory board.
Roles of advisory board members who completed the curriculum reviews.
Review of curriculum process
Stakeholders were given two specific opportunities to study, review, and provide commentary on the curriculum. Each review used a similar method where advisory board members convened as a group in a centrally located banquet facility in Lusaka. Minor and culturally consistent incentives, including a transportation stipend and lunch and tea breaks, were provided to the stakeholders.
The review process involved all members of the advisory board. CMMB-Zambia supervisory staff and faculty members facilitated the discussion, allowing advisory board members to contribute feedback. When staff and faculty members were not leading the discussion, they were taking notes on the feedback provided. These notes were then compiled at the end of the meeting and used to direct alterations to the curriculum.
CMMB-Zambia recommended a rigorous initial review of the curriculum, which occurred in April 2018. Working collaboratively, stakeholders, academic faculty, and CMMB-Zambia obtained detailed oral comments on curriculum content over 2 days – reviewing each line of the curriculum to attain feedback and clarify materials. At the first review, the curriculum was visually displayed for the entire room. Facilitators would read one or two lines of text and seek critique from the group. Considering the Zambian context, this process was familiar and acceptable to participants. Staff took notes during this meeting, which were compiled and considered for further revisions of the content. Based on this first review, faculty members addressed concerns and revised the curriculum.
The second day-long meeting considered the updated manual, seeking general module critiques in August 2018. Members had received updated written manuals several weeks in advance of this meeting. During this second review, CMMB-Zambia supervisory staff and three faculty members guided the discussion from the conveyed advisory board, considering sections of the training materials. Meeting facilitators provided a general overview of the section, displaying a summary slide of the content in each section of the training manual. Stakeholders were then given guiding prompts, such as assuring that the necessary topics were covered in the manual, seeking feedback on how to improve the content, and finally, to identify ways to make the materials easier to understand. When faculty were not leading the discussion, they were taking notes on stakeholder recommendations for change.
Responding to feedback
Seeking to enhance the cultural and social-environmental context of the material, reviewers’ comments centered on three themes. These included making the curriculum more intentionally Zambian, incorporating additional topics into the curriculum, and identifying ways to make the materials more approachable and user friendly. As was expected, each successive stakeholder review led to more alignment between their perspectives and the curriculum content.
Situating the curriculum to Zambia
Consideration of the Zambian context encompassed a broad array of points. First, stakeholders indicated their desire that the curriculum align more closely with language from the UN CRPD. Commentators also noted that the curriculum should be positioned more clearly in the Zambian legal framework. Stakeholders suggested including key points of the Policy and Rights of Persons with Disabilities from the Zambian Disability Policy. This information was added to the preface of both the ToT and the community volunteer manuals. Finally, reviewers wanted common causes of disability in Zambia highlighted to include maternal alcohol and drug use, poor maternal nutrition, malaria, neonatal jaundice, and meningitis.
Additional topics
The second feedback theme hinged on informational gaps in the training materials. Stakeholders asked for further content on the social aspects of disability stigma. They also requested additional information on supporting children with sensory impairments, such as low vision and hearing loss. Stakeholders were interested in further material on autism spectrum disorder being added, such as signs, symptoms, and suggestions for supporting these children and their families. The committee requested additional training on maintaining confidentiality of visited families.
Making the training more accessible
The last point of feedback focused on improving the training’s accessibility for the community volunteers. Despite being existing volunteers at their local health clinics, these community home visitors had not received any specialized training on supporting CWD or their families. They needed the information presented in a concrete and practical way. One consideration in developing the manual was to make it more interactive and include additional pictures to demonstrate techniques, which would facilitate experiential learning. Reviewers also found some parts of the module presentation too technical and asked for simplified language. In addition, stakeholders indicated that pictures or videos would be helpful in order to understand key concepts and skills.
Value in seeking stakeholder engagement
Seeking feedback from a diverse group of stakeholders aligns with Powell et al.’s (2015) recommendations for implementation research completed through a partnership between an academic and community organization where academics should seek input from diverse stakeholders. The purpose of this training manual is to enhance the capacity of community volunteers to provide information, care, and support to families of CWD. Board members included representatives from the government, disability rights self-advocates, and local community providers. Recommendations from this review aided the development of a ToT curriculum and manual for training community volunteers who will provide appropriate, competent, and needed services to CWD and their families.
Developing the curriculum through a stakeholder review of local partners enhanced the ToT product. Based on stakeholders’ feedback, faculty developers revised portions of the curriculum to more closely align with local needs in Zambia – highlighting Pellecchia and colleagues’ (2018) lessons learned from an academic–community partnership, where success depends on attending to a community partner’s needs. This article demonstrates the practice of using a local advisory board to support adaptation to the local context in Zambia, confirming that this process is valuable when working in an international context.
Another consideration in using an expert panel of stakeholders ties to ethical social work practice with diverse cultures and the need for cultural humility – being open, self-aware, and allowing reflection and critique, thereby dismantling power differentials across cultures (Burnette et al., 2014; Fisher-Borne et al., 2015; Foronda et al., 2016). Burnette and colleagues (2014) determined that when working with diverse cultures, methods matter. This curriculum review incorporated several of their recommendations, including the use of cultural readers, or individuals embedded in the culture and community who reviewed the materials, to assure they aligned with local contexts. The use of local stakeholders to seek reviews also situates with the International Federation of Social Workers (2018) principles of respect for diversity and building solidarity. In seeking feedback from the community, this review process endeavored to build consensus through stakeholder review for a ToT curriculum that will be used to develop a workforce of educated and inclusive community volunteers to support caregivers of CWD and for CWD to live more inclusive and independent lives.
Since this practice example described the use of an advisory board in the early phases of developing a program, additional articles could chronicle the use of other implementation strategies or other phases of implementation research when working internationally. For example, Powell and colleagues (2015) identify a number of additional steps of implementation research that this article does not consider, such as creating a credentialing program to encourage practice consistent with a new program. In addition, Meyers et al. (2012) describe implementation research phases, with this article focusing on aspects of the first phase of implementation. Other practice articles could consider how to sustainably continue to develop this training program.
This stakeholder review process represents one initiative in a multifaceted approach that strives to improve the quality of life for families of CWD in these communities. Our findings show how the use of a stakeholder group serving as an advisory board is very useful in refining training materials that are fully aligned with the local context. Representation from key stakeholder groups, in our case government officials, people with disabilities, the faith community, and health facility representatives, allowed for a comprehensive revision process. This process demonstrates how international partners implemented an inclusive program design to develop a customized and culturally relevant curriculum to train a workforce of community volunteers in two communities in Lusaka, Zambia.
Footnotes
Authors’ note
The views expressed in the submitted article are those of the authors and not an official position of the institution or funder.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the GHR Foundation.