
Abstract
In this essay, we provide an overview of a social worker-led, interdisciplinary practice model designed to combine essential online psycho-social support and local community self-governance for COVID-19 patients with minor symptoms in quarantine field hospitals in the city of Wuhan from February to May 2020. The interdisciplinary bridging response teams (IBRTs) model was designed for congregating settings to bridge offline community mobilization and online interdisciplinary professional services. We discuss the two-tier structure and organization of the practice model, the professionals’ roles and main tasks, and the key features that ensured the success of the model.
Keywords
Introduction
In early February, Wuhan city shifted its quarantine practice for COVID-19 patients with minor symptoms from home quarantine to hospital observation, amid construction of and conversion of large public structures into field hospitals, geared towards accommodating unprecedented volumes of patients. As social workers responding to volatile situations and changing public health practices, we found it imperative to devise a work plan that would enable us and allied professionals to support the patients and medical staff at these sites, in response to emerging psycho-social and logistical needs (Duan and Zhu, 2020; Qiu et al., 2020; Xiang et al., 2020), and health providers’ burdens (Liu et al., 2020). The interdisciplinary bridging response teams (IBRTs) model was born out of a larger programme of delivering professional services to COVID-19-affected populations that was designed and initiated by the first author as a practitioner–researcher. 1
The interdisciplinary model
This practice model drew on past disaster relief experiences and literature, especially in the areas of interdisciplinary disaster response teams (Adams, 2016; Briggs, 2005; Burkle, 2019), digital volunteer networking (Kaufhold and Reuter, 2016; McLennan et al., 2016; Park and Johnston, 2017), coordination between formal and informal response systems (Simsa et al., 2019; Twigg and Mosel, 2017; Whittaker et al., 2015), and community resilience/recovery (Imperiale and Vanclay, 2016; Miles, 2015; Norris et al., 2008). Our aims were (1) to provide essential logistical, informational, social and psychological support to the patients in field hospitals, (2) to facilitate the smooth workflow of field hospital care and (3) to foster self-governance among the patients within the field hospitals, so that they could regain some level of control over their life conditions.
The model featured IBRTs, each consisting of 10–12 members, including licensed social workers, medical volunteers (residency completed), licensed psychological counsellors, team helpers (primarily graduate social work students), and most importantly, community volunteers. The professionals were all online volunteers who had been screened for qualifications and trained for the IBRT programme. The community volunteers were themselves patients recruited and connected remotely from within the field hospitals at which the teams were virtually stationed, creating a ‘bridge’ between online services and the local communities. IBRTs were coordinated online and rotated through daytime shifts, ensuring the availability of at least one social worker, one medical volunteer, one counsellor and a community volunteer from 7 a.m. to midnight daily. By the end of April, eight IBRTs were in operation, involving approximately 100 professional volunteers, covering 1200 patients in two field hospitals in Wuhan.
The IBRTs received referrals from two larger chat groups, which included all patients housed at the facilities, community volunteers and IBRT professionals. The professionals drew on their discipline-specific knowledge and skills to provide coordinated services centred on patients’ needs, which were identified through (1) community volunteers’ onsite observations, (2) social workers’ active screening of chat logs in the two chat groups and (3) initial rapid assessment in IBRT case meetings. Generally, team members’ tasks included sorting and disseminating information, supporting discharge processes, facilitating virus testing logistics, providing psycho-social education or psychological counselling, and coordinating external supply donations (see Table 1). Social workers assumed a case manager role, responded to patients’ questions or requests for help, and identified complaints and potential signs of distress. Social workers on the teams also fostered self-governance among patients, under the leadership of the community volunteers, (1) to manage hygiene, noise, sleep and food delivery issues among other everyday care-related affairs within the field hospitals, (2) to promote patients’ compliance with medical observation and medicine administration and (3) to boost morale, trust and mutual care among the patients.
Roles and tasks of the IBRTs and backup team.
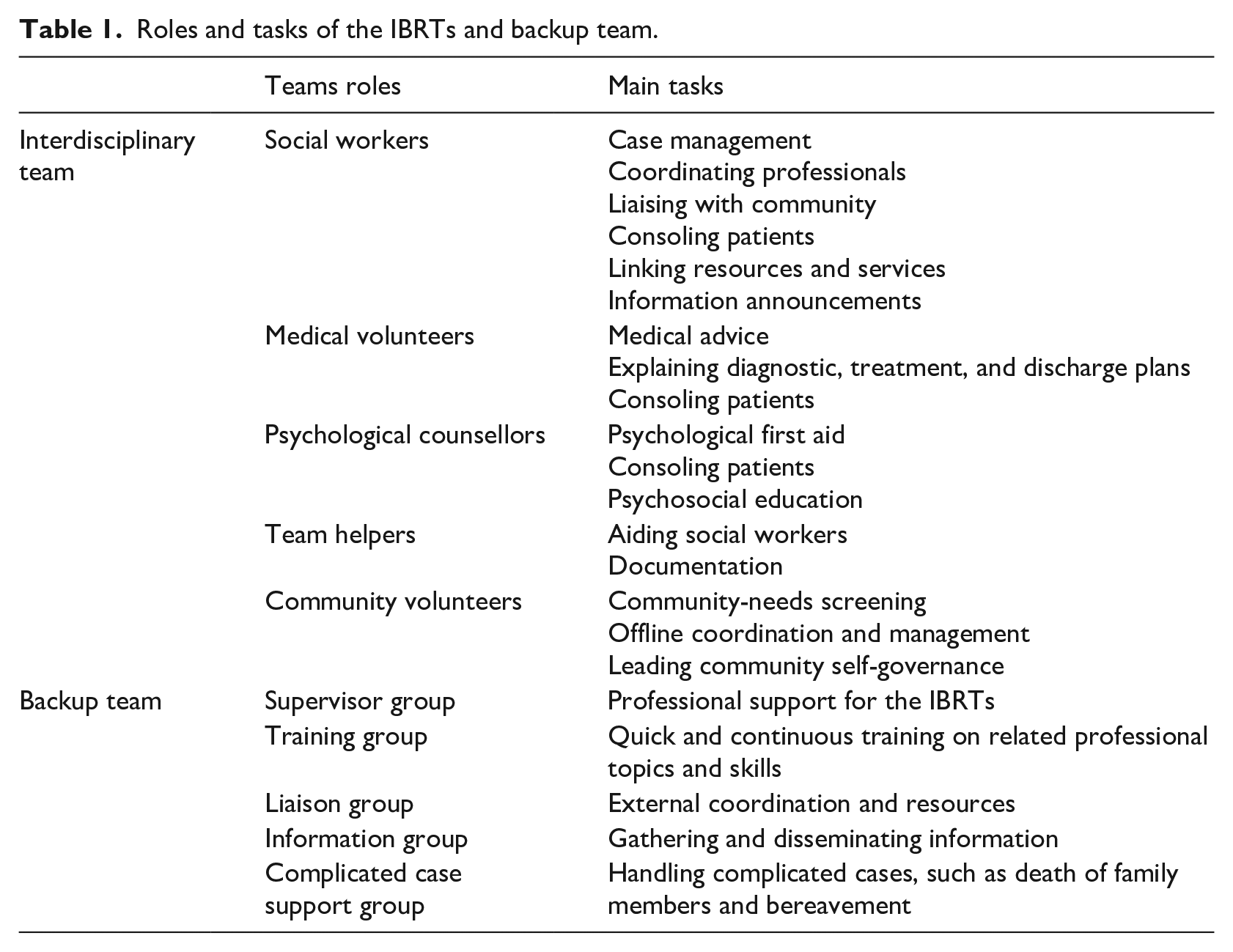
The IBRTs were supported by a backup team of highly experienced, senior professionals, who volunteered to provide training and supervision, liaised with external bodies and handled the occasional complicated cases (e.g. death of loved one). Approximately 70 senior professionals, including medical doctors, social workers, clinical psychologists and university professors from related disciplines, accepted invitations either directly from the first author or indirectly through online professional networks. Some of them were based in Wuhan, but most participated from outside of the city or outside of China. In addition to supporting the core team, professionals in the backing roles provided valuable resources and made connections with formal response systems, such as the disease control department, local hospitals and local health and welfare departments. Table 1 summarizes the roles and main tasks of the IBRTs and backup groups.
Operation of IBRTs
The online chat groups served as a virtual commons, wherein the patients raised questions and concerns about their stay at the field hospitals and communicated with the professionals. The chat groups were also channels through which social workers connected with the communities and fostered leadership and volunteerism. The operation of the IBRTs began at this level and followed a five-step recursive model (see Figure 1). Step 1: social workers reviewed the questions and concerns posted by chat group participants and identified potential cases. Step 2: potential cases were individually brought to a specific IBRT and triaged by type(s) of need(s). An appropriately matched professional was then assigned to the case. Step 3: the case was managed by the assigned professional and when necessary was discussed in IBRT case meetings. Debriefings were held at the end of each day where cases were discussed and experiences shared between the professionals. Help was sought from the supporting team to deal with complicated cases or when external support was needed. Step 4: cases were documented for ethics review, and feedback from the supporting team was shared. Step 5: if the case remained unresolved and required more complicated interventions, senior professionals stepped in and followed up. Resolved cases were closed and archived.

Operation of IBRTs.
It was crucial that the teams’ structure and organization would simultaneously allow for the mobilization of external resources, a coordination of services and its integration into local formal emergency responses. The following are key characteristics that enhanced the operation and efficacy of the IBRT practice model:
identifying gatekeepers to enable collaboration with formal response systems;
networking an entire affected community through the development of online groups;
continuous reflective training to clarify members’ roles, functions, and precautions for specific tasks;
moving beyond the virtual environment by fostering local community leadership and partnership;
triage of patients’ needs by active online screening of patients’ information and postings;
case-by-case follow-up and resolution;
daily debriefing to review and make work plans;
prompt availability of discipline-specific supervision;
safeguarding ethical practices by training and adhering to clear ethics procedures;
documentation and quick evaluation to provide feedback.
Conclusion
The IBRT model took advantage of a form of online organization suitable for overcoming the distancing requirements. Yet it went beyond the virtual world and extended into local communities, which we believe is crucial for the success of such efforts and the reactivation of community capacities. The self-governance and management efforts were particularly welcomed by the heavily understaffed medical personnel. The IBRT model is highly adaptable at a minimal cost, compared to a physical volunteering model. IBRTs are currently being used in six other countries, and it is hoped that this model will help bring more social workers, professional volunteers and communities together in our response to this pandemic.
Footnotes
Acknowledgements
The author(s) acknowledge and thank Carol Stalker and Mark Duffie for their feedback and assistance in preparing this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Keswick Foundation (Battling COVID-19: Social work services and action research project).