
Abstract
Team-based organizational designs are increasingly used to improve the fit between tasks and available human resources in modern organizations, and team empowerment represents an important means of enhancing team performance. At the same time, the growing complexity of work often results in task interdependencies that cross team boundaries, increasing the importance of interteam coordination in multiteam systems (MTS). Based on a longitudinal case study of a municipality that has implemented an innovative multiteam organizational model for home-based healthcare services, this article investigates how interteam coordination influences team empowerment. The results show that interteam coordination is central to team empowerment, highlighting the significance of the interplay between inter- and intrateam functioning in MTS. Overall, interteam coordination was a key factor in making the new organizational model work as intended and required careful attention and ongoing measures throughout the implementation process.
Introduction
Teams have become ubiquitous in modern work life (Groulx et al., 2023; O’Neill & Salas, 2018), and their functioning is highly influential for organizational performance (Carraro et al., 2024). Mathieu et al. (2019) explain the increasing adoption of team-based organizational designs by the need for maximization of human capital through aligning competencies and task demands in fluid environments. Tasks are allocated to teams based on the problems to be solved and their associated competence requirements, and teams are provided with autonomy and responsibility for task accomplishment, meaning that they are structurally empowered (Baird & Baard, 2021). Structural empowerment is, however, a necessary but insufficient condition for teams’ perceptions of being in control of their work and for the belief that they can perform their work on their own, that is, for being psychologically empowered (Maynard et al., 2012, 2013). This is important as team empowerment is central to achieving agility and internal process efficiency and can also positively influence product and service quality (Kirkman et al., 2004).
While team empowerment has traditionally been examined through the lens of internal team processes, increasing organizational complexity necessitates a broader perspective that accounts for interteam dynamics. This aligns with the recognition that teams do not function in a vacuum (Leicht-Deobald et al., 2023) and that collective task performance among interdependent teams is a significant factor for organizational effectiveness (Porck & van Knippenberg, 2023). The concept of multiteam systems (MTS), referring to “two or more teams that interface directly and interdependently in response to environmental contingencies toward the accomplishment of collective goals” (Mathieu et al., 2001, p. 289), has therefore grown in popularity in team research (e.g., Shuffler et al., 2015), and one critical topic concerns the role of coordination and collaboration for the achievement of superordinate goals (Wagner, 2024). A meta-analysis conducted by Leicht-Deobald et al. (2023) shows, for example, that active boundary and coordination management with the environment enhances team performance, and Wagner (2024) identifies important mechanisms for successful interteam coordination. Recent work by Ziegert et al. (2022) further demonstrates that a balanced pattern of intrateam and interteam interaction enhances system-level performance, enabling teams to maintain internal cohesion while contributing effectively to collective goals. In short, without effective coordination between teams, MTS cannot realize their full potential (Porck & van Knippenberg, 2023; Xie et al., 2022).
Drawing on theories of coordination in organizations and team empowerment, this study addresses the challenges of developing team empowerment in MTS where interdependencies across teams exist, and hence where the characteristics of interteam coordination may influence the internal functioning of individual teams. Guided by the research question “(How) does interteam coordination influence team empowerment?,” we investigate the idea that teams’ external relations and functioning in terms of interteam coordination play an important role in shaping their (psychological) empowerment. This reasoning is based on the recognition that, while team members often collaborate closely within their own teams to solve problems, make decisions, and carry out tasks, the growing complexity of work increasingly gives rise to interdependencies that extend beyond team boundaries. As the work of one team may have implications for the work and progress in other teams, planning, timing, and synchronization of tasks, as well as management of changes across teams, become critical. Through mechanisms such as shared routines, boundary-spanning roles, and mutual feedback, interteam coordination can play a critical role in enhancing team empowerment by reducing uncertainty, increasing information sharing, enabling mutual support, and aligning teams with superordinate goals.
Supporting this view, prior research indicates that when teams working toward common objectives succeed in breaking down barriers between them, they simultaneously develop a stronger sense of ownership over their work and a shared understanding of tasks that improve decision-making (University of Minnesota, 2025). For example, in a study of a large-scale automotive R&D project, Hoegl et al. (2004) found that interteam coordination was positively related to project commitment and teamwork quality, indicating that efforts to facilitate coordination enabled teams to align their outputs and feel more in control of their contributions to the final product. Similarly, several studies of software development teams suggest that reaching beyond team boundaries to access external knowledge and gather feedback is associated with conditions in which teams feel secure and confident in their ability to manage complex tasks (e.g., Faraj & Sproull, 2000; Sablis et al., 2021).
The empirical context of this study is the healthcare sector, where the use of teams has gained widespread acceptance (e.g., Dinh et al., 2020), partly due to the increasing complexity of patients’ conditions, which require diverse expertise and coordination to provide effective care, and partly due to the growing need to efficiently exploit scarce resources and competencies. The research question is examined through a qualitative longitudinal case study of a Norwegian municipality that has implemented an innovative multiteam organizational model for the production and delivery of home-based healthcare services. The empirical material on which the analysis is based consists of 45 interviews with 73 informants, conducted over a 54-month period spanning different phases of model implementation. The interviews were exploratory in nature, and the themes discussed included informants’ experiences with changes in work tasks, roles, collaboration, and coordination practices related to the implementation of the new model. A combination of thematic coding and directed content analysis was applied to examine how informants described their relationships and interactions with other teams and how they related these experiences to the internal functioning of their own teams. Through this approach, the study assesses how the use of different coordination mechanisms to manage interdependencies across teams is related to various dimensions of team empowerment.
Despite the surge of research on interdependencies and dynamic interplay of various components of work teams in recent years, most studies emphasize within-team processes (Park et al., 2020). Within healthcare, there is increasing emphasis on interprofessional collaboration (e.g., Doornebosch et al., 2022), but interteam dynamics are generally not emphasized, with some exceptions (e.g., DiazGranados et al., 2014; Taplin et al., 2015; Weaver et al., 2018). Overall, there is therefore a lack of knowledge concerning the dynamics of external ties and between-team factors (Park et al., 2020), and to our knowledge, no studies have directly examined interteam coordination as a contributing factor to team empowerment. By addressing this gap, the present study responds to the call for research on organizational factors and structural arrangements that serve as antecedents to various dimensions of team empowerment (Hempel et al., 2012; Maynard et al., 2012), as well as conditions that support the functioning of MTS (Salas et al., 2018; Wijnmaalen et al., 2019).
Conceptual Background
Interteam Coordination
Teams are widely used building blocks in modern organizational designs (Davison et al., 2012), and a way of matching tasks to the appropriate members of the organization (Mathieu et al., 2019). When work tasks are complex and interdependent, and when demands stemming from the external environment are unpredictable, teams will be dependent on also accessing the specialized knowledge situated in other, adjoining teams (Mell et al., 2022). That is, complex, specialized, and nonroutine work tasks, which increasingly characterize knowledge work, cannot easily be broken into separate sequences and performed in isolation from other similarly complex work tasks (Marrone, 2010). Actors performing such tasks depend on each other, and on others performing their own tasks effectively. However, it is often challenging to know and obtain a clear overview of exactly how tasks are interdependent, of which actors are needed to perform them effectively, and what the most efficient sequence of tasks would be (Okhuysen & Bechky, 2009). Coordination, understood as “the integration of organizational work under conditions of task interdependence and uncertainty” (Faraj & Xiao, 2006, p. 1156), has therefore become central.
Individual teams cannot operate as isolated units; they depend on contributions from other teams to achieve their goals. Multiple teams may be combined into a MTS, which refers to a collective of two or more interdependent teams organized as a tightly coupled activity system (Davison et al., 2012; Mathieu et al., 2001). In a MTS, each team is specialized in ways that enable them to contribute to the fulfillment of shared, organizational goals (Davison et al., 2012). If organizations are to achieve maximal effectiveness, we need to understand how teams are able to meet both external demands and maintain a productive internal dynamic at the same time (Marrone, 2010).
Interteam coordination, which involves “orchestrating work activities, sharing constrained resources, and acquiring feedback from other teams to accomplish goals” (Xie et al., 2022, p. 149), is hence central in MTS. Such coordination may have positive effects for individual teams, as they are more likely to achieve their goals, but also enable teams to integrate their work in ways that contribute towards the achievement of common, organizational goals (de Vries et al., 2014). However, this may be difficult to achieve as “differentiation generates boundary-enhancing forces” (Luciano et al., 2018, p. 1067), and research has shown that interteam coordination is challenging in work systems characterized by high levels of autonomy at team level (Ingvaldsen & Rolfsen, 2012; Zaccaro et al., 2020). MTS therefore need coordination mechanisms that enable them to overcome barriers for collaboration inherent to organizational designs that consist of autonomous and structurally empowered teams as building blocks (Luciano et al., 2018; Mathieu et al., 2001).
Okhuysen and Bechky (2009) describes coordination mechanisms as “the organizational arrangements that allow individuals to realize a collective performance,” which “often involve tools, technologies, and interactions that bring interdependent elements together” (p. 472). Scholars have delineated a variety of mechanisms that can be used to enact coordination among interdependent parties. Based on a review of the literature on coordination in organizations, Okhuysen and Bechky (2009) identify five coordination mechanisms that capture how work is coordinated through emergent action: plans and rules, objects and representations, roles, routines, and proximity. These mechanisms contribute to the integrating conditions of coordination—accountability, predictability, and common understanding—defined as “the means by which people collectively accomplish their interdependent tasks in the workplace” (p. 483). In this study, the categorization of coordination mechanisms presented by Okhuysen and Bechky (2009) guides the empirical analysis, which is followed by a discussion of integrating conditions and their links to team empowerment.
Team Empowerment
Increased emphasis on team-based organizational models has motivated practitioners and scholars to consider contingency factors for team performance (Baird & Baard, 2021). Several studies have in this regard shown that team empowerment is positively related to team performance (e.g., Kirkman et al., 2004; Kirkman & Rosen, 2000; Mathieu et al., 2006; Maynard et al., 2013). Although empowerment has been defined in many ways and has received most attention at the individual level (Mathieu et al., 2006), it is considered to be an isomorphic construct that retains the same meaning and functional relationships across levels of investigation (Seibert et al., 2011).
Extant research distinguishes between two major perspectives on empowerment: structural and psychological. The former views the phenomenon in terms of structures, policies, and practices that decentralize power, authority, and responsibility in the organization (Kanter, 1977; Mathieu et al., 2006). Psychological empowerment, on the other hand, refers to the beliefs of employees (and team members) regarding their authority, control, and responsibility for their work (Maynard et al., 2012; Spreitzer, 1995). This distinction also implies that structural factors can be seen as contextual antecedents of an emergent state of team psychological empowerment (Baird & Baard, 2021; Rapp et al., 2021).
This study focuses on team psychological empowerment, which is commonly understood to be manifested through four experiences of team members: (a) potency—reflecting collective confidence in the team's competence and ability to perform tasks and be effective; (b) autonomy—referring to discretion in deciding how to carry out tasks; (c) impact—experienced when team members see that their work is significant and important for the organization; and (d) meaningfulness—occurring when team members perceive their work to be important, valuable, and worthwhile (Kirkman & Rosen, 1999). Based on the premise that interteam coordination may play an important role in creating and sustaining psychologically empowered teams in work systems characterized by task complexity, changing requirements, and a need for ongoing reassessment of task allocation, the objective of this study is to examine the relationships between the use of interteam coordination mechanisms and teams’ experiences of the dimensions of psychological team empowerment.
Method
Study Context and Design
The context of this study is primary home-based healthcare services. This is a highly relevant context for studying MTS, as efforts to improve the exploitation of scarce resources and competences by developing new organizational models, including MTS, have gained increased attention in many countries in recent years, driven in part by a large and growing elderly population (e.g., McPake & Mahal, 2017). The focus of primary care has shifted from institutional care toward home-based care, and there has accordingly been a substantial increase in expenditures related to this type of service. As people live longer in their own homes, the need for efficient coordination among different health professionals increases in parallel with the growing complexity of services required to provide both specialized and integrated care (Doornebosch et al., 2022). Designing organizational structures and processes that adequately account for this complexity in a resource-efficient manner is therefore critical for providers of home-based healthcare.
This article draws on empirical data from a research project that followed the piloting, implementation, and operation of a new multiteam organizational model for home-based healthcare in a Norwegian municipality over a 4.5-year period (54 months). Spanning distinct phases of organizational reconfiguration, the project provided a unique opportunity to analyze the evolution of a multiteam model (de Vries et al., 2022), while also enabling the development of rich contextual descriptions and a thorough analysis of real-world phenomena (Eisenhardt & Graebner, 2007).
The objective of the reorganization project was to more effectively utilize the capacity of human resources, particularly that of registered nurses, and involved the modularization of work based on task characteristics and competence requirements rather than purely geographic considerations. The project also aimed to strengthen autonomy and independent responsibility among healthcare workers, provide more professionally rewarding roles for registered nurses, foster closer integration across professional groups, and enhance overall service quality.
The research project was designed to follow the municipality's work in developing and implementing the multiteam model across five municipal districts. The primary objectives of the research were to identify organizational barriers and opportunities for implementing effective healthcare teams and care service teams within the municipality, and to describe and analyze the innovation work conducted at different organizational levels throughout all phases of the innovation process. Key research questions concerned whether the new organizational model resulted in changes in employees’ perceptions of professionalism, responsibility, mastery, trust, and motivation in their work, as well as whether the model led to changes in work practices, collaboration, and coordination within and across professional groups.
Before the reorganization, services were organized into multidisciplinary units consisting of registered nurses (bachelor's/master's degree), healthcare workers (professional training without college education), and assistants (no formal educational requirements), who were jointly responsible for providing services to all patients within a defined geographic area. In the new model, tasks, patients, and employees were allocated to two different types of permanent (as opposed to temporary) teams: healthcare teams, consisting of registered nurses and physical and occupational therapists, and care service teams, consisting of healthcare workers and assistants.
During the reorganization process, the municipality made two significant changes to the model. The first involved the inclusion of physical and occupational therapists in the multiteam model, who prior to the reorganization had worked independently of the home-based services and were employed by a separate municipal department. One objective of the pilot was to test two slightly different organizational “sub-models” for healthcare teams with respect to the inclusion of physical and occupational therapists.
In the first sub-model, these employees were formal members of the healthcare teams and reported to the same manager as the registered nurses (i.e., all team members were employed by the same department and were physically co-located on all workdays). In the second sub-model, physical and occupational therapists were employed by a different municipal department than the registered nurses, as they had been prior to the introduction of the multiteam model, but interacted frequently and regularly with the other team members. Following the piloting phase, a hybrid version of these two sub-models was implemented, in which physical and occupational therapists were employed by their own department but spent two workdays per week working together with the registered nurses.
The second change concerned a specific role in the multiteam model referred to as the professional supervisor. Employees in this role were registered nurses with primary responsibility for professional development activities, such as training, education, and the provision of professional support for both types of teams. Initially, professional supervisors were embedded in each team, combining responsibility for professional development with a de facto assistant manager role. After the pilot phase, however, they were reorganized into a separate group within the healthcare team. This change was based on the need to ensure sufficient attention to the intended core functions of the role, at the expense of involvement in daily operations and care-related duties.
In all versions of the multiteam model, a set of criteria was used to allocate patients to either the healthcare teams or the care service teams. Some patients, however, required services from both types of teams; in such cases, responsibility was assigned to the team performing the majority of tasks. Although the teams were intended to operate largely autonomously, interdependencies across teams still existed, necessitating interteam coordination and interaction. This was, for example, required in situations where tasks and patients were initially allocated to and handled by one type of team, but where changing circumstances, such as changes in patients’ conditions or the need for additional services and competencies, called for evaluation and reassessment of task allocation.
It should also be noted that the pilot, after 6 months of planning, was put into operation on March 2, 2020, only ten days before the coronavirus lockdown in Norway. The pilot therefore turned out to be more challenging than expected, leading to increased strain on personnel and, to some extent, affecting the nature of interteam collaboration. Some forms of physical coordination, particularly interdisciplinary meetings involving physiotherapists and occupational therapists in sub-model two, were, for example, not carried out and were partly replaced by digital meetings.
Data Collection
The research was based on interviews with key informants, observations of steering committee meetings, and reviews of governing documents, including presentations delivered to the steering committee, meeting minutes, and project reports. The main data material on which this article is based constitutes a subset of the data collected in the research project. It consists of 45 semi-structured interviews, both individual and group interviews, with a total of 73 informants, conducted in one municipal district at four points in time. Figure 1 presents the distribution of interviews across the study timeline, including the informant groups involved in each phase.
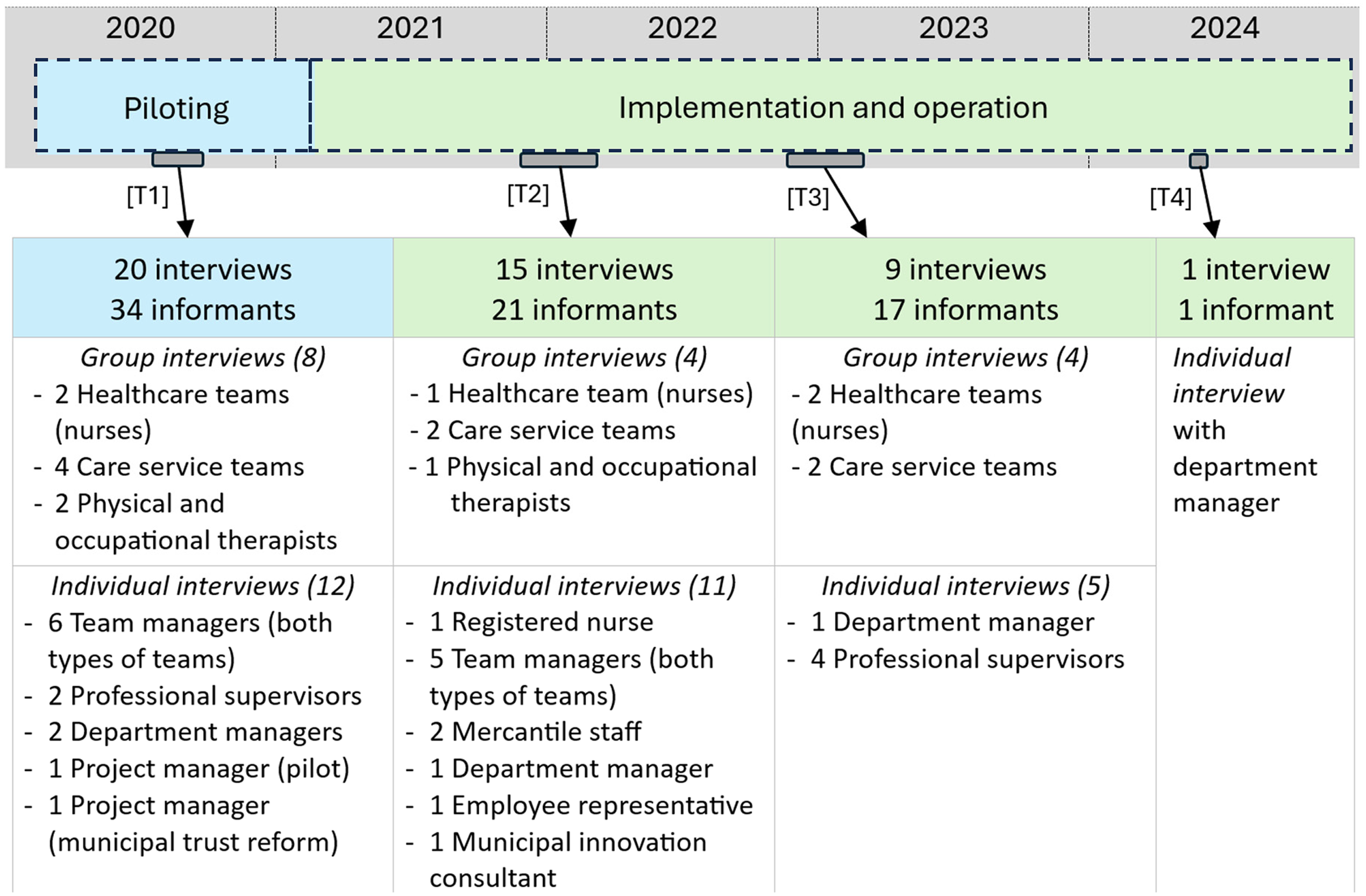
Overview of interviews and informants.
The selection of informants was conducted by the research team in consultation with the project's steering committee. At the individual level, informants were recruited by their respective managers. While this recruitment approach introduces a potential risk of selection bias, the strategy was considered appropriate for ensuring access to individuals with relevant experiential knowledge of the new organizational model and its operating context. This approach aligns with purposive sampling principles commonly employed in qualitative research, which prioritize depth and contextual richness over statistical representativeness (Creswell & Poth, 2018). The heterogeneity of reflections elicited during data collection suggests that, despite the inherent limitations of the recruitment method, the informant group provided a balanced and credible representation of experiences and viewpoints, thereby supporting the validity and trustworthiness of the findings.
To capture diverse perspectives, the study combined group interviews with individual interviews, as shown in Figure 1. Group interviews were conducted with members of the same team, focusing on work-related issues and providing rich insights into team empowerment, internal dynamics, and perceptions of relationships with other teams. Informants from different teams were not included in the same group interviews, as this could potentially restrict free expression and inhibit open discussion. Individual interviews were conducted with managers and staff responsible for service delivery and the reorganization process, offering a broader perspective on the functioning of the multiteam model and allowing for in-depth exploration of strategic considerations and organizational context. This combination enabled a comprehensive understanding of both team-level and organizational experiences during the reorganization, while potentially limiting insight into cross-team dynamics that might have emerged in mixed-group settings.
All interviews in the first round, as well as all group interviews in rounds two and three, were conducted face to face. All individual interviews in the second round, one individual interview in round three (with a department manager), and the interview in the final round were conducted digitally using Teams. All interviews were based on a thematic interview guide covering topics related to work organization and work practices, including interaction and collaboration with colleagues both within and across teams, perceptions of professionalism, autonomy, responsibility, trust, mastery, and motivation, as well as overall perspectives on the advantages and disadvantages of the new organizational model and perceived challenges related to the change process. The interview questions were formulated as open-ended inquiries, allowing informants to elaborate on issues they considered significant. Data collection was not guided by existing theories or analytical frameworks; consequently, informants were not explicitly probed about specific coordination mechanisms or particular dimensions of team empowerment. All interviews were recorded, and verbatim transcripts were subsequently produced.
Data Analysis
The data analysis for this paper was conducted in two distinct phases, combining thematic analysis (Braun & Clarke, 2006) with directed content analysis (Hsieh & Shannon, 2005). This two-step process enabled an initial broad identification of themes, followed by a focused examination of mechanisms critical to the functioning of the new organizational model.
Phase One: Thematic Analysis
The first phase employed a template-based approach (Brooks et al., 2015). Initially, both authors independently read all interview transcripts to gain an overall understanding of the material. Using qualitative data analysis software, text segments were coded and categorized based on (a) a predefined list developed prior to analysis, informed by the research questions in the project and the detailed interview guide, and (b) additional codes and categories that emerged as relevant during iterative engagement with the data. This approach ensured flexibility and allowed new insights to be incorporated as the analysis progressed. The analysis in this phase provided a comprehensive overview of patterns in professional practice and organizational factors influencing the implementation process. Preliminary findings were then discussed between the authors. These discussions highlighted interteam coordination as a critical factor for the success of the new model, closely linked to team empowerment. This insight motivated a second, more targeted phase of analysis to examine how interteam coordination influences team empowerment.
Phase Two: Directed Content Analysis
The second phase adopted a directed content analysis approach, which is appropriate when researchers seek to use existing theory to guide the interpretation of research findings (Hsieh & Shannon, 2005). In this phase, the authors revisited relevant theory and refined the coding scheme for the concepts of coordination mechanisms and team empowerment. The former was informed by the work of Weaver et al. (2018), who apply the coordination framework developed by Okhuysen and Bechky (2009) in a multiteam healthcare context and identify mechanisms pertaining to the categories of plans and rules (e.g., schedules, protocols, policies, and guidelines), objects and representations (e.g., prototypes, care plans, and treatment summaries), roles (e.g., formal and informal job or role descriptions), routines (e.g., care meetings, training, simulation, and rehearsal), and proximity (e.g., patient- and family-centered rounds, informal discussions, huddles, and call-outs). Regarding team empowerment, the development of the coding guidelines was informed by the conceptualization and operationalization of the dimensions of potency, impact, autonomy, and meaningfulness, as presented by Kirkman and Rosen (1999).
This approach allowed for systematic identification of coordination mechanisms and their relationship to team empowerment. In this phase, the dataset was divided into two segments, with each author responsible for coding one segment. After completing their respective analyses, the authors reviewed each other's coding and engaged in joint discussions to reconcile interpretations and ensure consistency. The analysis involved identifying and coding textual segments that represented occurrences where coordination mechanisms and empowerment dimensions appeared in connection. Three types of potential linkages were considered relevant: (1) occurrences indicating how the use of coordination mechanisms might positively influence team empowerment; (2) occurrences suggesting that the absence or insufficiency of such mechanisms could negatively affect empowerment; and (3) temporal reflections, where informants discussed how efforts to improve coordination over time were perceived to impact team functioning (for interviews in T2‒T4). This structured approach enabled a systematic exploration of both direct and evolving relationships between coordination practices and empowerment experiences.
Supplementary Data and Credibility Measures
Analysis of meeting minutes, presentations, and municipal reports complemented the interview data by providing additional insights into issues related to interteam coordination and team functioning throughout the reorganization process. Furthermore, findings were regularly presented to and discussed with key municipal personnel involved in the implementation, thereby strengthening the credibility and practical relevance of the results.
Results
Overall, the results provide strong indications of the importance of interteam coordination for the development of team empowerment in work contexts characterized by task complexity and interdependence. In our case, interteam coordination was a central factor in enabling the new organizational model to function as intended and required careful attention and targeted measures throughout the implementation process. Several coordination mechanisms were used and had an impact on team empowerment, while the absence or insufficiency of such mechanisms, as perceived by informants, was also influential for intrateam functioning.
The results indicate that some coordination mechanisms and empowerment dimensions may be more salient than others, at least in the early phases of multiteam working arrangements. With respect to coordination mechanisms, routines and roles were most frequently referred to in interviews when informants discussed issues related to interteam interaction, whereas coordination through objects and representations appeared to play a more limited role (with some exceptions). Regarding team empowerment, the dimensions of potency and impact occurred most frequently in the empirical material, while discussions of interteam interaction that could be related to meaningfulness were largely absent. Possible explanations for these findings are addressed in the discussion section. In the following, the different categories of coordination mechanisms are used to structure the presentation of results. Selected quotations are included to illustrate both the presence and the perceived absence of interteam coordination and how these relate to team empowerment.
Roles
Overall, the results show that role clarity represents an important foundation for interteam coordination in situations characterized by task uncertainty and ambiguity, where advice from and involvement of members of other teams in assessing task requirements may be a determining factor for work quality and, consequently, for team potency and impact. Role clarity entails that team members are confident in their knowledge and skills, understand the importance of their work for the MTS, and are able to recognize and act upon interdependencies across team boundaries. It also involves being comfortable with and knowing when, how, and what to communicate to other members of the MTS in order to obtain accurate and useful responses. The quotations below show that a lack of role clarity, manifested as limited confidence in knowledge and skills and a weak shared understanding of interdependencies and mutual goals within the MTS, was associated with reluctance among some healthcare workers to contact nurses in the healthcare team. This reluctance had negative implications for the perceived quality of care. It can also be related to a lack of confidence in their own knowledge and skills. “Should I do this on my own? Will I be able to detect changes in the patient's condition?” They may also hesitate to contact the nurses and think that they should manage on their own and carry out their work independently. (…) This has been challenging for me as well. There have been some misunderstandings: employees think that they are left on their own and that we should not use the nurses at all. They feel alone, and I tell them that “they are not alone” and that we should use the competence [in other teams] when we need to. But it is difficult to find that balance. (Team manager, care service team [T1]) In the beginning, we were met with responses such as “can’t you do that task… you are supposed to know this by now”. After that, we barely dared to ask. It became less comfortable. (…) It would have been nice to have someone to contact. The threshold for asking for advice is high; then you drop it, and it may influence the quality of care. (Group interview, care service team [T1])
This also indicates that expectations of team autonomy, as communicated in descriptions of the intentions underlying the new organizational model, reduced the likelihood of team interaction in situations requiring the involvement of other teams, which in turn negatively affected team potency and impact. Building team empowerment therefore required emphasizing role interdependencies across teams, both at the initiating and the receiving end, to reduce the risk that team members would refrain from initiating interteam interaction when such interaction was needed. This issue was identified as a significant risk during the piloting of the organizational model, and improvement efforts aimed at strengthening interdependencies across teams were subsequently initiated. These efforts contributed to lower barriers to interteam communication and increased support, which were important for team members’ perceptions of their ability to solve problems, be productive, and accomplish their objectives within the multiteam system. If I’m uncertain about something and feel the need to confer with a nurse, I can always call them, and they always answer the phone. It's very reassuring to have them as backup. I think it was supposed to be like this. But this hasn’t always been the case. (Group interview, care service team [T2])
The importance of role clarity for team potency and impact may be particularly evident in situations where the range of available coordination mechanisms is limited. Such situations may arise during periods of reduced staffing and potentially increased geographic distance between members of different teams, resulting in fewer opportunities for both formal and informal communication.
In addition to highlighting the need to improve the overall understanding of roles within the MTS, several informants emphasized the importance of the professional supervisor as a boundary spanner between teams. Acknowledging that interteam coordination had the potential for improvement, the professional supervisor was viewed as a key mechanism for establishing a unified “one-team culture.” Informants further highlighted that enactment of this role could facilitate boundary-spanning activities grounded in task-related knowledge. The professional equivalence between registered nurses in the healthcare teams and professional supervisors, both in terms of type and level of knowledge as well as work style, appeared to facilitate interteam interaction and foster a sense of safety and reassurance that both types of teams were capable of delivering high-quality work.
Several informants reported that this role was important for the functioning of the organizational model, which was perceived to involve risks related to not detecting changes in patients’ conditions. A central aspect of the role in this regard was the ability to access both internal and external information and to disseminate information that was relevant for task accomplishment among employees in the care service team. [Expression of concern from manager]: (…) that we are not able to detect and report deterioration in patients’ conditions, such as changes in blood pressure. The professional supervisor takes responsibility for such matters (…). She reads the reports every day, so we are dependent on people reporting. She also discusses the reports with the team during lunch breaks and seeks to identify any issues that require action. She then either asks them [employees in the care service team] to contact a nurse [in the healthcare team] or takes responsibility for sending e-notes to the doctor. (Team manager, care service team [T1])
The results thus indicate that successful enactment of the role in terms of supporting healthcare workers in assessing when to seek advice from others and, consequently, in making decisions and taking appropriate action based on patients’ needs (i.e., enhancing team potency, autonomy, and impact), depended on systematic information flow from employees in the care service team to the professional supervisors. The findings also show that the use of additional coordination mechanisms to support information flow, like reporting systems (objects and representations), interdisciplinary meetings (routines), and reporting procedures (plans and rules), was important for effective role enactment.
Plans and Rules
When it comes to plans and rules, the results show a lack of guidelines and agreed-upon expectations regarding interaction between teams, particularly in the initial phases. This was especially problematic for healthcare workers and assistants who experienced major changes in tasks and responsibilities and therefore posed a challenge to the ambition of creating empowered care service teams. As a result, informal communication was initiated, which was perceived as distracting by the receiving end (i.e., registered nurses) and not aligned with the intention of developing more independent care service teams. This issue was therefore identified as an area for improvement and addressed systematically during the implementation process. We may not have all the procedures and guidelines fully in place with regard to cooperation between teams. We have some. When we identify a need for improvement, we create a new procedure, and then we think it's sufficient. But afterwards we realize that no, we also need to establish a procedure for this as well. So we are still working on it. During the pilot, we were very divided, you know, and at the same time the pandemic created a great deal of distance between the teams. This is something we are still struggling to break down (…). (Higher-level manager [T2])
A lack of clearly defined rules and procedures for interteam coordination also appeared to be related to poor role descriptions and limited role understanding. Missing, inadequate, or poorly understood role descriptions resulted in ambiguity regarding responsibilities across both types of teams, leading to confusion and diverging perceptions of when interteam coordination was required, as well as uncertainty about how and when specific coordination mechanisms should be used. Relatedly, members of the healthcare team called for more clearly defined and mutually agreed-upon requirements concerning the knowledge base underlying communication, that is, which tasks care service teams should complete before contacting the healthcare team. The development of this knowledge base involved performing tasks that were new to employees in the care service teams and thus held potential for increasing team potency and impact. Achieving this, however, required competence development, which in turn depended on interaction between teams. In this regard, the data show that it was unclear how the healthcare teams should support the care service teams, particularly in the initial phases. The message we received was that they [the care service teams] should be responsible for conducting tests and making assessments so that they are able to determine whether a patient needs other medical services. But we are supposed to back them up and provide safety. (…) [Question from researcher: “What does that mean; what does “backing up” imply?”] That's the question. I don’t know. (Group interview, registered nurses in healthcare team [T1])
The results also indicate that a lack of clearly defined and agreed-upon rules for interteam interaction made interaction more person-dependent and informal, which could facilitate the initiation of interteam contact to discuss issues in uncertain situations. On the other hand, personal relationships could be prioritized at the expense of formal meeting structures for discussing issues of concern, potentially reducing the likelihood of involving the specific expertise required by the situation.
Although most informants who discussed uncertainty regarding how, what, and when to contact other team members emphasized its negative consequences, the interviews also indicate that such uncertainty may lead to a greater variety of topics being discussed across teams. This can be framed positively, as it holds potential for increased interteam learning and competence development and may, in turn, contribute to improved team potency and impact.
Routines
The results show that the task characteristics of home-based healthcare services, combined with new ways of organizing work as well as allocating and executing tasks, led to a perceived need for new routines for interteam interaction. In general, informants reported a lack of cross-team meeting points during the initial phases of model implementation. Together with care service team members’ hesitation to contact registered nurses on an as-needed basis, due to perceived expectations of independence, lack of guidelines, and/or experiences of hostile feedback, this resulted in a reduced quality and frequency of interteam interaction. Moreover, reduced formal contact was particularly challenging when combined with the abrupt changes in task allocation and the perceived expectation that new tasks should be completed without consulting registered nurses.
In the first round of interviews, several informants expressed concerns about the ability to detect changes in patients’ conditions and needs. Although the professional supervisor played an important role in this regard, it was also necessary to develop an interteam system for quality checking that could function as a safety mechanism. This was subsequently followed up by the establishment of routines designed to address this concern. Weekly use of assessment lists implies that we [the healthcare team] are notified of patients whom the care service teams find challenging. (…) This is related to changes in patients’ conditions and situations in which they perceive that they are not able to provide sufficient care. Then we can see what we can do about it. (Group interview, registered nurses in healthcare team [T3])
Related to this, in the initial phases of model implementation informants spoke about the need for a system to keep track of patient allocations. This concerned the need for increased visibility of patient transfers across teams, which would simplify and improve the ability to identify patients requiring particular attention from the healthcare team and thereby enhance team impact. This issue was also addressed during the organization's work on developing and refining routines. One such routine that was implemented was regular transfer meetings among team managers, involving discussions of whether patient transfers across teams were needed and, if so, when they should take place.
The organization also designed and implemented other routines to facilitate interteam interaction, including interdisciplinary whiteboard meetings and interteam training and lecturing. Regarding the former, informants reported that such meetings, where participants from both types of teams discussed patients’ status and needs by using a whiteboard (objects and representations), resulted in improved involvement and team impact. Regarding interteam training and lecturing, two types of routines were initiated: systematized one-to-one observational learning in the field (when visiting patients) and lecturing sessions. The observational learning routine aimed to enhance care service team potency and impact by improving the performance of tasks previously carried out by registered nurses, such as administering insulin injections and providing wound care. The lecturing sessions involved registered nurses delivering lectures and conducting training sessions for care service teams to build the general competence of healthcare workers and assistants, thereby contributing to team potency.
The process of selecting topics for training and lecturing further illustrates the interdependencies among different types of coordination mechanisms in fostering team empowerment. The quotation below demonstrates how the professional supervisors’ functioning as knowledge intermediaries (roles) was important for identifying and prioritizing topics to be emphasized in lectures and training sessions (routines), and how reports (objects and representations) constituted an important means in this process. If we see recurring themes, we can talk with the professional supervisor and discuss the need to give a lecture on the topic. This is also something they try to identify through the reports, if they notice recurring issues that healthcare workers should be able to manage. (Group interview, registered nurses in healthcare team [T1])
Proximity
Regarding proximity, several informants reported that informal meeting points, such as lunch breaks, constituted important arenas for observation and spontaneous dialogue and were therefore regarded as significant for the transfer of tacit knowledge. Such cross-team interaction was reduced in the new organizational model, which was perceived as particularly negative by care service teams, who linked this reduction to decreased opportunities to build competence and make progress in their work (i.e., reduced impact).
The lack of proximity and opportunities for ongoing communication between teams was associated with perceptions of being unable to accomplish tasks and resolve problems as they arose. This was regarded as particularly disadvantageous by care service teams and influenced team potency, as members reported low confidence in their own abilities and perceived the work as overly demanding and overwhelming. The negative consequences of low proximity for team confidence were further amplified by instructions (perceived by some members of care service teams) directed at the healthcare team to maintain physical distance between teams, based on management's anticipation that collocated work would lead to increased demands for ongoing communication, which was viewed as contrary to the ambitions underlying the new organizational model. I think the ambition is that we should be as independent as they are. (…) They have been instructed not to sit with us. The reason is that they think the nurses would receive too many requests from us. (…) We don’t have any backup—you feel so alone. The nurses are here, but not in the way they used to be. (Group interview, care service team [T1])
This perspective was not shared by all employees in the care service teams, however. On the contrary, physical proximity was also highlighted as providing a sense of safety in uncertain situations, which typically occurred during periods of low staffing in evenings and weekends. This view became particularly evident after the model had been in operation for some time and may therefore reflect the effects of efforts initiated to build a unified, cross-team culture. In the evenings and on weekends, there is often only one healthcare worker present, filling the role of work coordinator. In such situations, it becomes vulnerable if the distance between us and the nurses is long. (…) If I’m uncertain about something and need to ask a nurse for input, and I know them, I can get an answer right away. I think that is very important. (Group interview, care service team [T3])
Objects and Representations
The findings indicate that the introduction of the new organizational model created a need for more structured approaches to interteam interaction. In particular, the use of whiteboards to support interdisciplinary discussions was highlighted as a key factor in fostering involvement and enhancing team impact. Importantly, effective use of this tool depended on participants being physically present (i.e., proximity), whereas hybrid meetings conducted by phone or video were generally viewed as less desirable. Another tool introduced after the model had been in operation for some time to improve the quality of interteam discussions was a “communication book,” which the care service teams used to document needs for patient assessment by physical and occupational therapists.
Organizational and physical distance between teams further resulted in increased reliance on journal systems for documentation of work and interteam information flow. The use of such systems also represented a new task for healthcare workers and assistants, thereby requiring training and the development of a shared understanding of how the systems should be used (e.g., what information to include in reports). In this regard, the results indicate that suboptimal use of these systems may constitute a barrier to the development of team impact. Specifically, inadequate use may reduce both the frequency and quality of interteam feedback on important areas for improvement, thereby limiting teams’ ability to make progress in their work. (…) When you receive a large pile of papers after three public holidays, you know there is a lot in there that should not be registered. Not that it is incorrect, but it is simply too extensive. They have completed the work according to the work description, but it should not be documented in the journal. It is deviations, or work that, for some reason, has not been completed, that should be logged. So, there is a lot to read. Part of the explanation is that there are many unskilled workers who think this is how it should be done. It takes a lot to change that way of working. (Group interview, registered nurses in healthcare team [T1]) There are issues described in the reports that require attention and action. I feel a great responsibility to be attentive to and look for such things and to be helpful. (…) But we hardly ever have time for that, which we have also reported. Then we have been told to skim through the reports. The feeling of going home from work on those days without having read the reports (…) I feel that responsibility. (Group interview, registered nurses in healthcare team [T1])
Evolvement of Interteam Coordination and Team Empowerment Over Time
Overall, the analysis points to potency as a salient aspect of team empowerment and indicates that routines and roles were especially visible coordination mechanisms (both positively and negatively) as the new organizational model was implemented and put into operation. However, the analysis also suggests that the relative importance of routines increased in later phases. This development may be explained by an initially underestimated need for interteam coordination, combined with uncertainty about how such coordination could be achieved, which subsequently led to greater emphasis on building structures to support it. That is, the municipality gradually came to recognize that effective interteam functioning was critical for achieving team empowerment and, accordingly, acknowledged significant potential for improvement. As a result, considerable attention was directed toward establishing routines, clarifying associated plans and rules, and refining role definitions in order to improve interteam coordination and support team empowerment. After a while, we realized that we had to establish structures for how the care service teams should interact with the healthcare teams in order to obtain the necessary guidance and the sense of safety they need to perform their work. (…) It was important for us to clarify roles, establish structures, and define “rules of conduct” for how the teams should function, as well as to ensure that they got to know each other. (Mercantile staff representative [T2])
Informants also reported that the gradual development of meeting structures for discussing the allocation and integration of tasks within the interteam system was associated with an increased focus on patients, indicating that these routines contributed to enhanced team impact (i.e., the teams’ work having a positive impact on patients). Confirming this development, informants from the care service teams stated that their need to seek advice from the healthcare team decreased over time. Moreover, the nature of interaction appeared to shift from being primarily “interrogative” to more “informative.” The healthcare workers now use the physical and occupational therapists much more, and on their own initiative. They seem more confident when they visit patients. They know what to look for, and they provide more feedback. Previously, we received many requests and information about trivial issues that the nurses had to take care of, but now they get the work done themselves and take more responsibility. [T2]
Related to this, in later interviews several informants also described a development toward increased team autonomy without explicitly linking this development to interteam coordination. However, informants emphasized that awareness of the availability of other teams remained important, that is, employees felt secure knowing that support was accessible if needed. This may suggest that interteam coordination plays a more prominent role in the development of team potency and impact than in autonomy and meaningfulness, while still constituting a necessary condition for improvements in these latter dimensions of team empowerment within a multiteam system. What we have learned is that when the structure is in place, the teams feel safe, and they know where to turn if they need input. Then the focus on patients starts to evolve, and on how we can manage this together. It is very exciting (…) I think the teams are well equipped to deliver positive results. (Higher-level manager [T2])
Discussion
To synthesize the main findings, Table 1 provides an overview of how specific coordination mechanisms are linked to the various dimensions of team empowerment. This summary highlights the nuanced ways in which roles, plans and rules, routines, proximity, and objects and representations contribute to team potency, autonomy, impact, and meaningfulness.
Summary of Results.
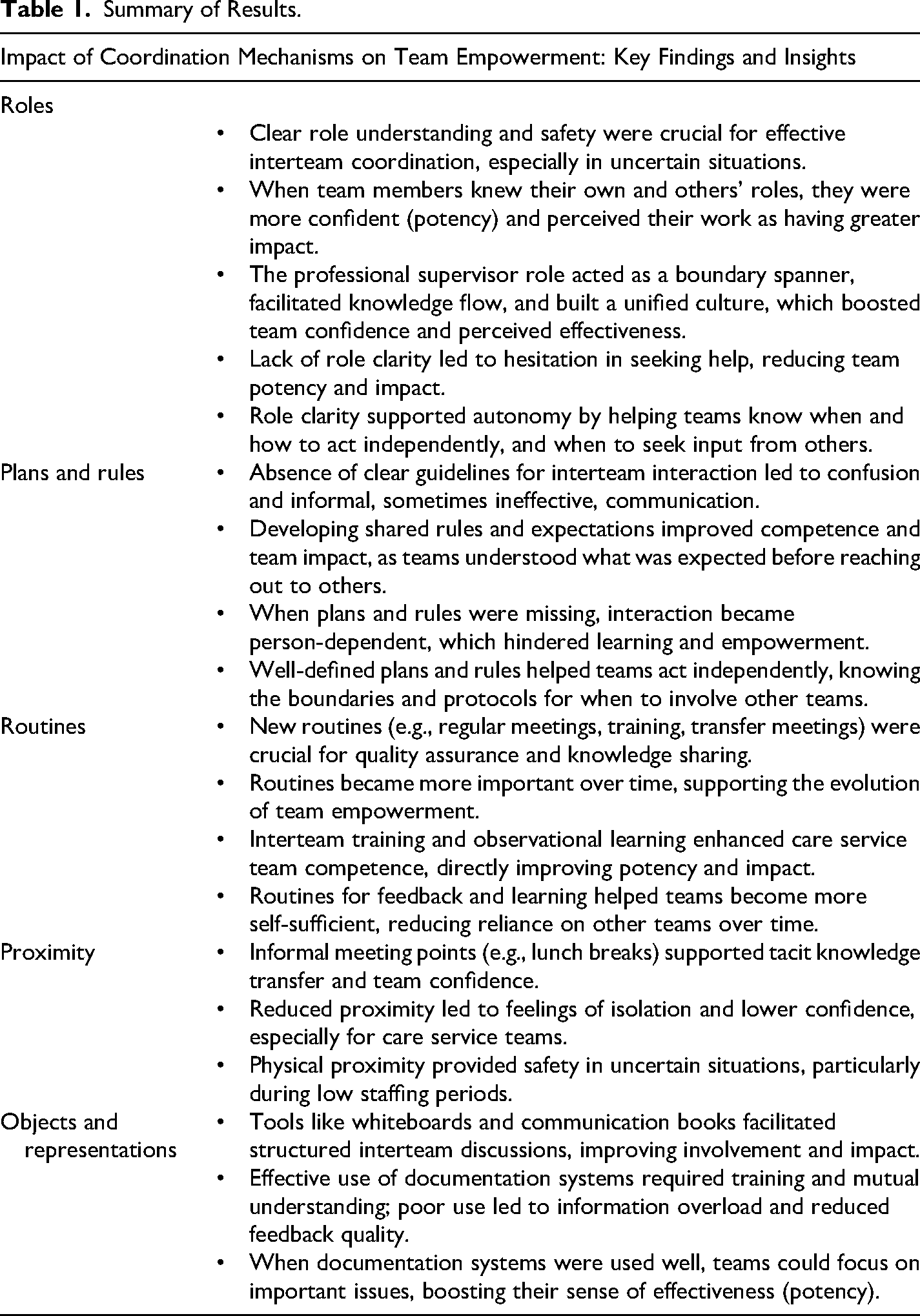
The results show that interteam coordination influences team empowerment in work systems characterized by variation in competence requirements and a need for ongoing assessment of the conditions that determine task division and allocation. Different dimensions of team empowerment may be affected, both positively and negatively, by the presence or absence of specific types of coordination mechanisms. Routines and roles appear to be particularly influential for team potency and impact in the early phases of a new organizational model, which may indicate that these mechanisms are especially important in situations characterized by uncertainty and requiring adjustments of work processes in MTS. Furthermore, the results draw attention to two aspects that need to be interpreted in light of the study context: the interrelationships among coordination mechanisms and the interrelationships among dimensions of team empowerment.
Interrelationship Between Coordination Mechanisms
The results indicate that coordination mechanisms matter for team empowerment both individually and in combination. For example, team potency was influenced by the combined effect of a lack of routines and formal interaction processes, a reduction in informal meeting points between different professional groups, which had occurred naturally in the previous model due to organizational and geographic proximity, and reluctance to initiate and use informal communication following negative responses experienced by one type of team. These findings indicate that a holistic perspective on coordination is necessary, as understanding the effects of specific mechanisms requires consideration of the presence or absence of a broader set of mechanisms, including the availability of alternative coordination practices.
This aligns with the view that different coordination mechanisms fulfill similar functions by creating awareness and understanding of how individual components fit within a broader system (Okhuysen & Bechky, 2009), in this case, how the work of individual teams fits with that of others in the MTS. That is, all coordination mechanisms contribute to the development of the integrating conditions of accountability, predictability, and common understanding, which appear to constitute important foundations for intrateam empowerment in MTS. For example, enactment of the professional supervisor role illustrates how boundary-spanning activities can increase awareness of interdependencies between tasks and thereby promote predictability across teams. More generally, mechanisms that support clear role understanding by developing shared knowledge of when, how, and what to communicate to other teams contribute to the development of interteam accountability, in terms of knowing who is responsible for specific task elements and what can be expected from others. This study shows that such mechanisms may be particularly important in situations where there are limited alternative means for emergent coordination and interpersonal interaction (Ziegert et al., 2022), for example due to differences in working hours and/or geographic distance between teams. This finding further highlights that work schedules in MTS represent an important contextual factor, as the availability of coordination mechanisms for interteam interaction may vary over time. Consequently, the significance of specific coordination mechanisms may change throughout the day depending on the availability of alternative coordination options.
The availability of a variety of coordination mechanisms also appears to be important for creating common understanding as a foundation for team empowerment in situations characterized by uncertainty. Uncertainty regarding the roles of different actors and diverging perspectives on how the MTS should function affects both the amount and quality of interteam interaction, which in turn influences team members’ work conduct. This indicates that the development of common understanding among actors in MTS is significant for team empowerment. Promoting common understanding by lowering barriers to initiating interteam interaction through the use of multiple coordination mechanisms holds potential for increased learning and competence development, as it enables a broader range of topics to be discussed across teams. This also enhances the likelihood of developing a shared knowledge base, which may be necessary for the effective use of coordination mechanisms based on mediated, asynchronous interaction (i.e., interaction that does not involve direct human contact and does not allow for immediate feedback). For example, the results show that the usability of the journal system (objects and representations) as a coordination mechanism could benefit from interteam training (routines) aimed at developing a mutual understanding of how the system should be used.
Interrelationship Between Dimensions of Team Empowerment
As for the analysis of interrelationships between coordination mechanisms, the context of the study is also relevant to the findings regarding team empowerment. The data analysis revealed that potency and impact were the most salient dimensions of team empowerment associated with interteam coordination. Some references to autonomy were also identified, whereas meaningfulness occurred to a much lesser extent in the empirical material. Considering that the study took place in the early phases of the functioning of a multiteam organizational model, this pattern suggests that the interrelationships among team empowerment dimensions may have a temporal dimension, such that the dimensions do not necessarily develop or manifest simultaneously. Rather, internal dependencies among the dimensions constituting the empowerment construct may help explain this finding.
Existing research shows that the dimensions of team empowerment are highly interrelated and together represent a unitary or global construct (Seibert et al., 2011). However, this does not imply that all dimensions follow identical developmental trajectories, either in terms of timing or antecedent conditions. The results of this study indicate that potency and impact may function as preconditions for autonomy by enabling team members to develop the competence and confidence required to make decisions regarding task prioritization and execution. In turn, this may lay the groundwork for teams to experience their work as important, valuable, and worthwhile, that is, as meaningful.
Regarding the interrelationship between team empowerment dimensions, it is also noteworthy that diverging expectations of team autonomy, stemming from a lack of established shared understanding among teams in the MTS, may negatively affect team potency and impact. Specifically, the results indicate that expectations of independent work conduct within the MTS shape the nature of interteam interaction (e.g., whether teams are inclined to consult others in uncertain situations, how such interactions are initiated, and how requests are received and responded to). In turn, these interaction patterns influence teams’ perceptions of their ability to produce high-quality work, solve problems as they arise, and accomplish their objectives.
Implications
The interrelation between autonomy expectations and team potency and impact entails that developing role understanding in situations characterized by changing needs and requirements requires balancing an emphasis on team autonomy with attention to the need for interteam interaction to foster team potency and impact. Overall, the study indicates that guidelines for interaction aimed at securing adequate information flow across teams constitute an important component of role descriptions in contexts marked by task ambiguity, interdependence, and a constant need to reassess task allocation. This may be particularly important in the early phases of organizational change in order to overcome initial communication barriers arising from unclear and divergent understandings of how work should be carried out. It is therefore essential to define structures and processes for interteam interaction and to allocate sufficient time and resources during the initial phases of multiteam working arrangements to build competence, clarity, and psychological safety, thereby enabling teams to operate more independently over time. As such, this study contributes to MTS research by illustrating how formal and informal coordination mechanisms interact to shape the functioning of individual teams within MTS (Wagner, 2024; Ziegert et al., 2022). The findings also demonstrate the value of process-oriented methods for capturing the complexity of MTS dynamics.
The results are consistent with the conclusions of de Vries et al. (2014) and other research (e.g., Marks et al., 2005) indicating that interteam coordination is positively related to team performance. Our study further underscores the importance of fostering team members’ identification with the overall organization in order to create both motivation to engage in interteam coordination and a shared understanding of the significance of such efforts for achieving high-quality organizational outcomes. This may be particularly important in situations where the multiteam model is constructed around disciplinary similarity and specialization, as limited functional diversity among teams may reduce communication across team boundaries (Ancona & Caldwell, 1992) and increase the risk of reinforcing in-group and out-group perceptions (Joshi & Jackson, 2003).
Regarding the use of coordination mechanisms, the study shows that organizations initiating MTS need to develop guidelines for interteam interaction and ensure sufficient resources to overcome initial barriers. This finding supports the conclusions of Hoegl and Weinkauf (2005), who emphasize that team interface management is particularly important during the concept phase of multiteam projects. Although coordination mechanisms may fulfill similar functions, interdependencies among different mechanisms need to be taken into consideration. The results indicate that organizations should initially emphasize the clarification of roles and routines, as this is important for developing a common understanding among the various teams, which is fundamental to the development of team empowerment. Such a shared understanding further enhances the effective use of coordination mechanisms based on computer-mediated asynchronous interaction, which is particularly beneficial in work systems characterized by geographic (i.e., different locations) and temporal (i.e., different working hours) boundaries (Espinosa et al., 2015).
Limitations and Directions for Future Research
The study has some limitations that should be considered when interpreting the results and that also point to directions for future research. First, the reorganization process was affected by the coronavirus lockdown, which significantly influenced the strain on personnel and opportunities for collaboration during the initial (piloting) phase. This may have affected both the quantity and quality of intra- and interteam interaction, for example, by influencing the availability and suitability of various coordination mechanisms.
Second, the study was conducted during the early phases of working in a multiteam system. Although the study covered a timespan of 54 months, the organizational model was not yet fully established or internalized within the organization and instead underwent ongoing structural and processual adjustments. As the interrelationships among dimensions of team empowerment may evolve over time, and the relative importance of different coordination mechanisms may vary across phases of multiteam functioning, future research should examine more mature stages of MTS and place greater emphasis on temporal aspects of multiteam work (Park et al., 2020). Relatedly, future research should also examine temporary teams, in contrast to the ongoing or permanent nature of the MTS studied in this case, as the duration of team existence may influence team stability, norm development, skill development and exploitation, and communication characteristics (Chae et al., 2015; Saunders & Ahuja, 2006).
Future research should further investigate this topic across different contexts and work domains, both within healthcare and in other sectors, as potential differences in environmental demands, complexity, interdependencies, and associated coordination requirements may influence the interplay between intra- and interteam functioning. Finally, future studies should also examine performance outcomes related to interteam coordination and team empowerment. In this regard, innovation represents a particularly relevant theme, as cross-boundary teaming is considered a viable strategy for innovation (Edmondson & Harvey, 2018), and empowerment has been linked to team creativity and innovation (e.g., Burpitt & Bigoness, 1997).
Conclusions
This study demonstrates how interteam coordination can influence intrateam empowerment in MTS characterized by interdependencies across teams and responds to calls for research on factors that serve as antecedents to distinct dimensions of team empowerment (Maynard et al., 2012). Furthermore, the study contributes to a deeper understanding of how MTS evolve in response to coordination challenges, that is, how such systems become, rather than offering a static analysis of systems after they have already taken form (de Vries et al., 2022). A particularly prominent finding concerns the importance of routines and roles as coordination mechanisms for achieving team potency and impact in the early phases of a new MTS.
The study also contributes to the literature on work organization by examining the interplay between inter- and intrateam functioning in MTS, and by highlighting the importance of alignment between organizational structures (team organization) and processes (interdependency management) in complex work systems more generally. It thus illustrates how alignment between structure and process is instrumental in the design of organizational models based on personnel specialization, as such models inherently involve intra-unit competence homogeneity and interunit competence heterogeneity, which in turn require well-functioning processes to integrate interdependent tasks. Finally, with regard to the empirical domain, the findings offer relevant insights into organizational conditions for the effective utilization of scarce resources in healthcare.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Research Council of Norway (grant number 326932).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Note
Olaug Øygarden has moved to a new institution since completing the research. Her current role is Advisor, Department of E-Health and Welfare Technology, Stavanger Municipality.
Appendix. Interview Guide (main questions/themes related to work conduct,organization,and interteam coordination)
Not all themes were equally relevant to all informants, and the time allocated to different themes was therefore adapted to the informants’ knowledge and perspectives. The questions were formulated as open-ended inquiries, thereby affording informants the opportunity to elaborate on issues they regarded as significant.