
Abstract
This study examines the risk associated with inconsistent use of condoms as a risk factor for human immunodeficiency virus/sexually transmitted infections (HIV/STIs) and sexual risk behaviours. The Malawi Demographic Health Survey 2010 data were used. Out of a sample of 2987 males and 9559 females aged 15–24 years, 511 males and 675 females were filtered in the present study. A Chi square test and logistic regression techniques were performed. About 147(28.7%) males and 240(35.6%) females reported inconsistent condom use. The likelihood of inconsistent condom use was higher among females with secondary/higher education (odds ratio’s (OR)=1.46), with more than one partner (OR=4.27), and married males (OR=8.76), with more than one sex partner (OR=1.78).There is a need to raise condom use awareness and improve sexual education about consistent condom use, especially among females, in order to curb the spread of HIV/STIs and reduce sexual risk behaviours.
Keywords
Introduction
An estimated thirty-four million people worldwide are currently living with the human immunodeficiency virus (HIV) and other sexually transmitted infections (STIs), and 67% of these people live in Sub-Saharan Africa (UNAIDS, 2010). This number is expected to increase due to young people’s risky sexual practices and inconsistent condom use (Global AIDS Response, 2011). While the overall health status of youths who use contraceptives is expected to improve, it has been reported that most sexually active youths do not use condoms consistently (Nakaie et al., 2014). The inconsistent use of condoms has resulted in the rapid increase in sexual and reproductive health problems such as unintended pregnancies, and the increased rate of newly infected HIV and other STIs. Although some progress has been made in the rate of condom use, inconsistent and incorrect use of condoms and the likelihood that partners might discontinue their use is still a challenge, thus impeding the progress of condom programmes in fighting the spread of HIV and other STIs (Beksinska et al., 2012). The consistent use of contraceptives such as the condom among sexually active youths has been a major intervention factor toward the reduction of HIV and other STIs, especially in Sub-Saharan Africa, where the numbers of HIV/AIDS and other STIs infected persons are on the rise (Nagarajan et al., 2013). Unfortunately, the rate of condom use among sexually active youths has been very low compared to the knowledge they have regarding their role in sexual relationships (Munthali et al., 2004), thus the risk of HIV and other STIs continues to rise. Incorrect and inconsistent condom use has been associated with an increased chance of contracting STIs. Although studies in Sub-Saharan Africa reported some stability in the number of new STIs cases, the rate continues to increase due to young people’s risky sexual practices (UNAIDS, 2009).
Malawi has a youthful population, with 73.8% of the country’s population being below the age of 30 years (UNAIDS, 2013). The country has the highest rate of teen births in the Sub-Saharan region, with 193 per 1000 girls, unlike Zimbabwe and South Africa with 101 per 1000 and 54 per 1000 girls respectively. The average HIV prevalence rate is at 10.6%, with 12.9% of women living with the virus compared to 8.1% of men (MDHS, 2010), indicating that, women and girls are more vulnerable to HIV and other STIs than men due to a low and inconsistent rate in the use of condoms. This gender variation is at its most disadvantaged when it comes to consistent condom use as women and girls have little negotiating power in most relationships in Sub-Saharan Africa (Wirtz et al., 2015). Although young people are encouraged to use condoms consistently and effectively through numerous campaigns in order to reduce the spread of STIs, a greater proportion still do not use them. Increased alcohol consumption, drugs and substance abuse have been evident to be a contributing factor to low condom usage (Hutton et al., 2011), thus facilitating the spread of HIV/STIs. A recent report indicates that inconsistent use of condoms has been a major factor for the high rate of HIV and other STIs among sexually active youths in Malawi (UNFPA, 2011). The prevalence of STIs, especially HIV, is higher among young men who do not use condoms consistently compared with those who use condoms consistently (National Statistical Office, 2011). It is difficult to actually predict if an individual has used a condom or not, especially among sexually active youths, and it is even more difficult to gauge whether young people who claim to have used a condom, do so consistently. Misconceptions such as fear of side-effects, condoms causing sores on the penis (Marisen, 2014), lack of self-efficacy among intimate partners (Ghimire et al., 2011), service providers not being youth friendly (Maluwa-Banda and Lunguzi, 2002) and lack of communication from parents (Limaye et al., 2012) on the proper and consistent use of condoms have been a contributing factors toward inconsistent condom use among sexually active youths.
In the United States, about 89% of sexually active females who do not want to become pregnant often go to clinics for contraceptives (Frost and Darroch, 2008), but unfortunately, more than half of all unintended pregnancies occur mostly among contraceptive users. This therefore implies that they do not use these contraceptives consistently, thus facilitating the spread of HIV and other STIs. Most pregnancies in the United States are unplanned (Finer and Kost, 2011), and it has been evident that these unintended pregnancies are the result of inconsistent use of contraceptives (Finer and Henshaw, 2006). In China, Wang L et al. (2015) reported mixed findings whereby the prevalence of consistent condom use with different sex partners among money boys is higher (82.4%), while Cai et al. (2010) reported a prevalence rate of 69.6%. In Uganda, the likelihood of inconsistent condom use with a new sex partner is 37.4% and 49.2% among males and female students respectively (Mehra et al., 2014). Young people aged 15–24 years have been severely affected, and 75% of all new HIV cases within this age group occur in females (Barker and Ricardo, 2005).The economic background of youths determines whether they use condoms or not, especially in a society where condoms are not made available for sexually active youths. In Malawi, a combination of poverty and poor sex education is a contributing factor toward inconsistent condom use and this leads to risky sexual behaviour among young people (UNAIDS, 2013). Young people from a background where there is greater wealth inequality are more likely to have extramarital partners (Paul, 2015). Therefore, considering the economic status of Malawi, where poverty is regarded as a driver of early pregnancies and HIV/AIDS/STIs among young people, the issue of using a condom and even its consistent use is probably the last thing on young people’s minds. The government, in collaboration with UNFPA, has launched the ‘Condomise Malawi Campaign’ which is aimed at increasing the consistent use of condoms among youths since it offers dual protection against STIs such as HIV, syphilis, gonorrhoea and chlamydia, as well as unwanted pregnancies (UNAIDS, 2014). Despite this effort by the government, young people still do not use condoms consistently, thus facilitating the spread of HIV and other STIs.
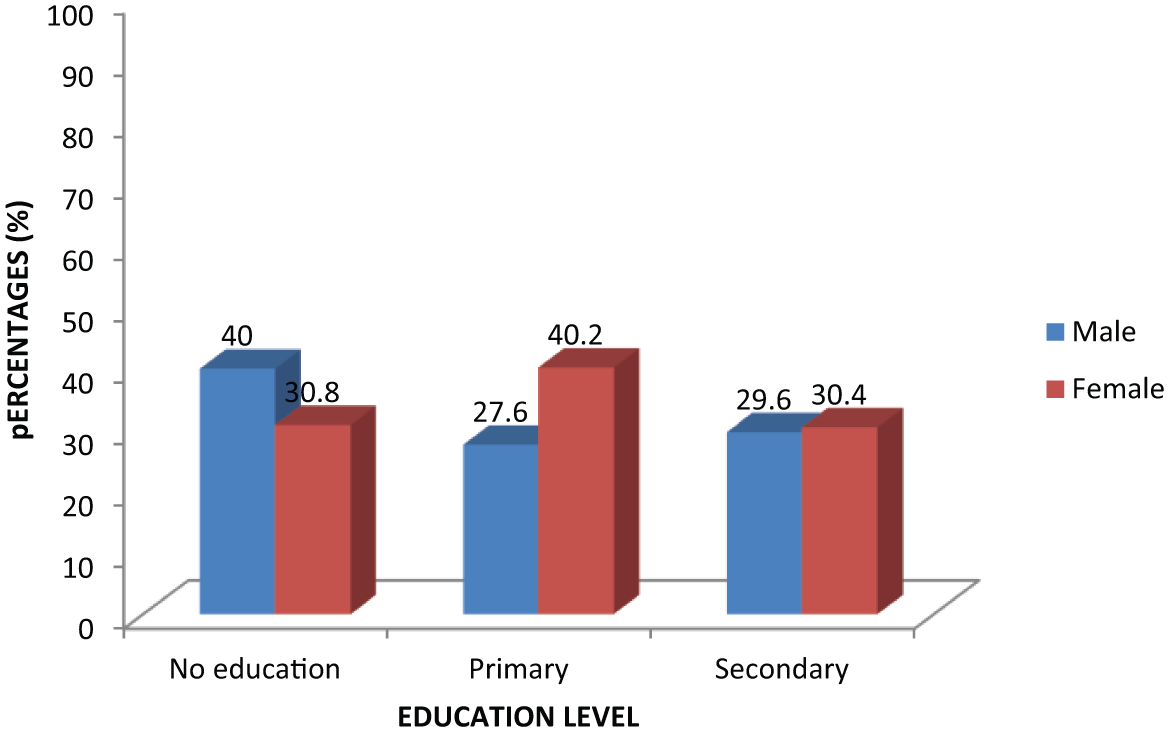
Percentage of males and females aged 15–24 years with inconsistent condom use by education level in Malawi 2010.
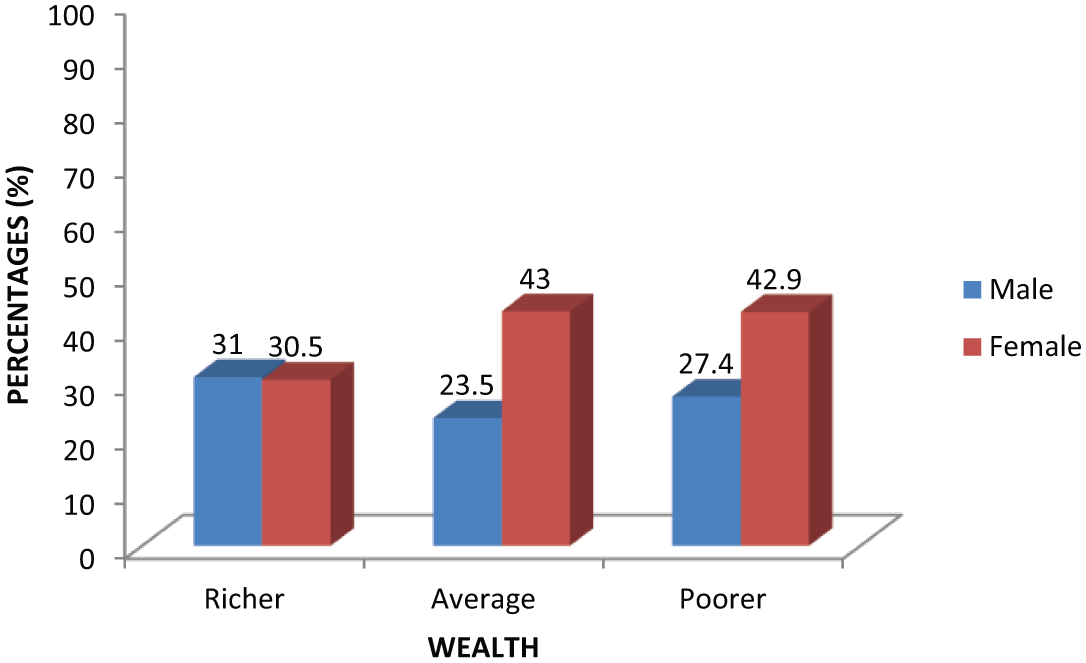
Percentage of males and females aged 15–24 years with inconsistent condom use by wealth in Malawi 2010.
According to the Malawi Demographic and Health Survey (National Statistical Office, 2011), 79% of young women and 89% of young men know where to get a condom, but most young people are not allowed to access and use condoms consistently and correctly. This contributes to the spread of HIV and other STIs. Although the consistent use of condoms is one of the most effective strategies in reducing the spread of HIV and other STIs, certain cultural practices hinder the effective use of these devices, since certain policies do not allow the distribution of condoms among young people in primary and secondary schools (Munthali et al., 2004). Since the introduction of the female condom in 2004, its acceptance has been very slow, with less than one per cent of women reporting its use. Thus, its consistent use is therefore out of the mind of most young people due to certain misconceptions that surround it (National Statistical Office, 2011). The female condom was introduced because it was the only available technology that women could initiate and control in order to prevent the spread of HIV and other STIs. Though the use of these contraceptives was not consistent, it has been evident that women who are planning to conceive still recognize that they and their sex partners are at risk of STIs (Finocchario-Kessler et al., 2012).
There is a general conception that education determines young people’s level of condom use. Huneeus et al. (2014) found that learners who complete primary education in public schools have a higher likelihood of inconsistent condom use than those in private schools. Thus, the proportion of youths who consistently use condoms increases with the level of education. The relationship of condom use and education is more than simply a function of increased knowledge that leads to positive health behaviour. Sex education needs to be included in the school curriculum for uninfected persons to better understand the epidemic (Dalal et al., 2014). Young people with more education will tend to use condoms more consistently since inconsistency leads to unintended pregnancies that will consequently lead to school dropout. Although much has been documented regarding young people’s sexual behaviour, risky sexual behaviours, and condom use in sub-Saharan Africa, little emphasis has been put on inconsistent condom use, especially among sexually active youths in Malawi. It is from this background that the current study aimed at closing the knowledge gap by examining the risk factors associated with inconsistent condom use, and its implication in the transmission of HIV/STIs among sexually active youths in Malawi.
Data
The data used for this paper were obtained from the Malawi Demographic and Health Survey ((MDHS, 2010) which was downloaded free of charge from www.measuredhs.com after permission was granted to do so by the ICF Micro International). The MDHS (2010) produced cross-sectional data based on a nationally representative survey conducted in Malawi from June to November 2010 (MDHS, 2010). The survey collected data on different topics from a multistage cluster sample of 27.340 households. Each district was demarcated into enumeration areas (EAs), and sampling was conducted within the district and EA levels. Within the districts, the primary sampling units were the EAs and within each EA, the households were considered the secondary sampling units. A total of 849 EAs and 27,307 households were selected, and of these, 25,311 were occupied. Of the 25,311 households found, 24,825 were successfully interviewed, yielding a response rate of 98 per cent. Within each sampled household, only men aged 15–54 years and women aged 15–49 years were eligible for the survey.
The survey used structured questionnaires; the household, female, and male questionnaires with several modules which included an HIV module that was administered to eligible members of the sampled households. The 2000 and 2004 surveys had used these questionnaires. The 2010 survey team obtained ethical clearance from the Malawi Health Sciences Research Committee, the Institutional Review Board of ICF Micro, and the Centers for Disease Control and Prevention in Atlanta, USA (National Statistical Office, 2011). Although the number of explanatory variables for both males and females were not the same, the study focuses on those who did not use condoms consistently with their most recent sex partner. For the current study, inconsistent condom use was used to describe those who do not use condoms regularly, and this was derived from the variable ‘use condom every time had sex with last partner’ which was defined as 0= Yes and 1=No to represent those that use condoms consistently and inconsistently respectively.
Method
The data were extracted and the relevant sample was weighted according to the design of the 2010 MDHS in order to obtain a representative sample for the study. For the current study, sexually active youths aged 15–24years were retained for analysis. Thus, 511 males and 675 females were filtered out of the total sample of 2987 males and 9559 females. The variable ‘use condom every time had sex with last sex partner’ was used in the study as the dependent variable. This variable was redefined as No= 1 (to define those who report inconsistent condom use and Yes=0 otherwise). Data were cross-tabulated, and the statistical significance of the association between the dependent and categorical variables was tested by Chi-square in order to fulfil the study objectives. Furthermore, the binary logistic regression technique was performed to examine the association between socio-economic and demographic characteristics on inconsistent condom use, and its association with young people’s risky sexual behaviours using version 22 of the Statistical Package for Social Sciences (SPSS).
Selected variables
Some selected variables were extracted from the 2010 MDHS survey on risky sexual behaviour, condom use every time had sex with last sex partner, age group, marital status, ethnicity, number of sexual partners, wealth, age group, and place of residence. Those who did not use condoms every time they had sex with their last sex partner were described as inconsistent condom users. Other variables were defined as follows: age group was stratified into two age groups spanning five years (15–19 and 20–24); place of residence was defined as urban or rural; education level was defined as those with no education, primary or secondary/higher; wealth was stratified into richer, average and poorer; marital status defined as married/living together, never married/not living together/divorced/widowed; number of sexual partners was defined as 0 (for those with one sex partner) and 1 (for those with more than one sex partner); and ethnicity was defined into Chewa, Lomwe, Ngoni, Tumbuka, Yao and others (the category others included: Tonga, Sena, Nkhonde, Other; Lambya, Other; Ndali, Other; Mang’anja, and Other; Nyanja).
Statistical analysis
The extracted data for males and females were weighted so that the sample was representative of 15–24 years old respondents in the 2010 MDHS. Analysis was performed using SPSS version 22, which accounted for the sample strata, the primary sampling unit and population weights. A descriptive statistic of youth’s inconsistent condom use, stratified by gender, was presented. Chi-square comparisons were conducted to identify differences between adolescent males and females relating to inconsistent condom use, and these were made within socio-economic and demographic characteristics. The binary logistic regression technique was then used without an offset to examine the relationship between inconsistent condom use, and socio-economic and demographic characteristics. This model provided an estimate of the prevalence ratio for the relevant outcome. All analyses presented were stratified by gender regardless of the significance of any interactions. However, one model was created and it examined whether the difference in inconsistent condom use was associated with the youth’s sexual behaviours, and this was controlled using the socio-economic and demographic variables to examine the association of inconsistent condom use with youth’s sexual behaviours.
Results
There were more females than males considered in the study as indicated in Table 1. About 54% of male respondents were aged 20–24 years, residing in the rural area (about 76%), and being married (12.1%). More than half of them had one sexual partner (about 80%), with primary education (about 54%), from the richer households (about 56%) and being Chewa (29.2%) ethnic origin. Most females were aged 15–19 years (50.1%), residing in the rural area (66.7%), and never married (63.3%). The majority had more than one sex partner (60.5%), with primary education (52.7%), in the richer households (59.3%) and were from the Chewa (22.1%) ethnic group.
Socio-economic and demographic characteristics of participants in the study area.

Source: Malawi Demographic and Health Survey (2010), weighted cases.
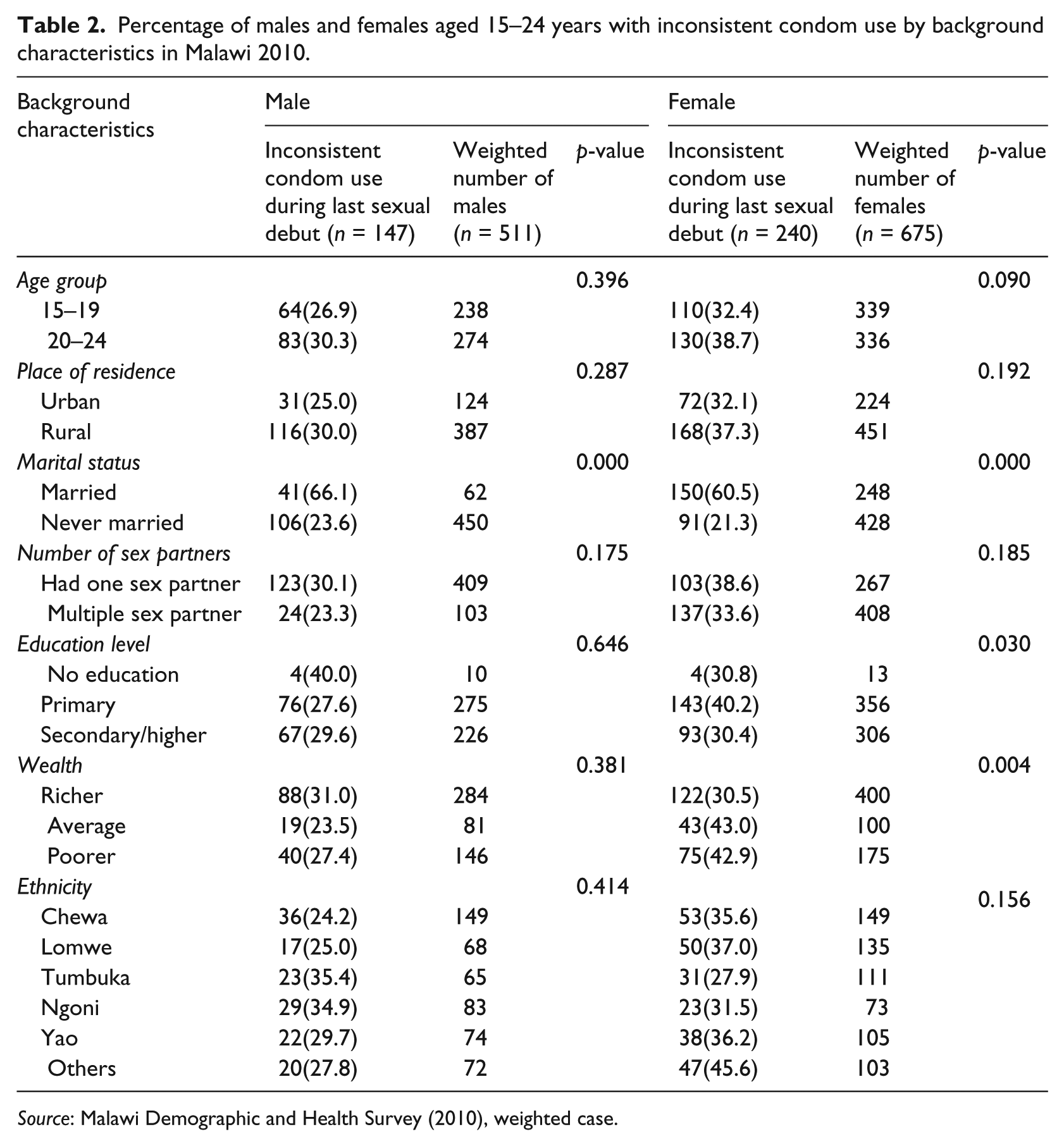
The prevalence of inconsistent condom use was higher among females 240(35.6%) than males 147(28.7%) as indicated in Table 2. The prevalence was statistically significant among males who were married (66.1%, p<0.000). However, most males who reported inconsistent condom use were aged 20–24 years (30.3%), reside in the rural area (30%), with one sexual partner (30.1%), with no education (40.0%) and from richer household income (31%), and being from the Tumbuka (35.4%) ethnic group. All these variables did not give any significant results except marital status. Among females, the prevalence of inconsistent condom use was statistically significant among married females (60.5%, p<0.000), with primary education (40.2%, p<0.030), and from an average household income (43.0%, p<0.004).
Percentage of males and females aged 15–24 years with inconsistent condom use by background characteristics in Malawi 2010.
Source: Malawi Demographic and Health Survey (2010), weighted case.
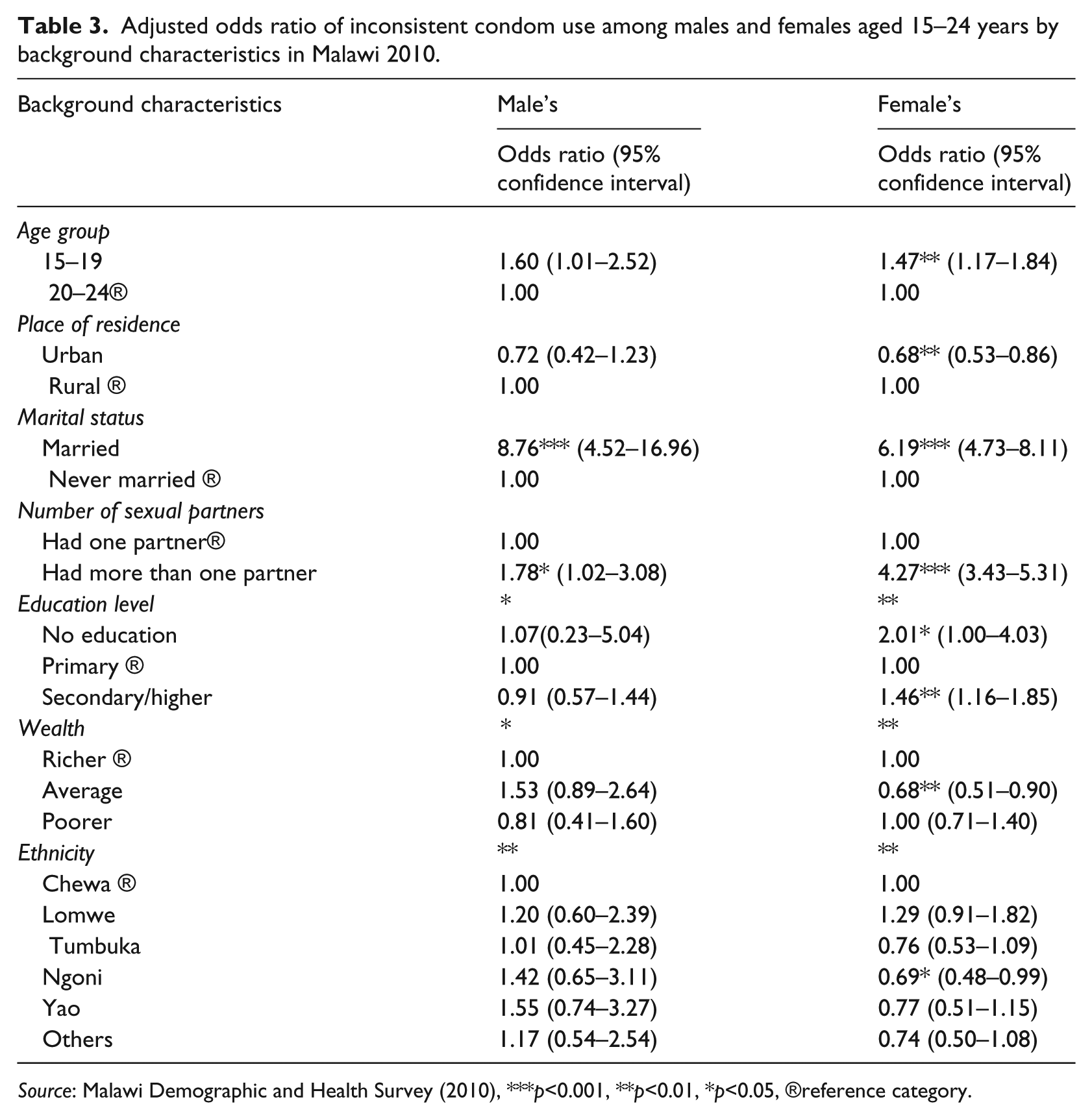
Based on the logistic regression results in Table 3, the likelihood of inconsistent condom use was higher among males aged 15–19 years (odds ratio (OR)=1.59), who were married (OR=8.76), and with more than one sexual partner (OR=1.78). Among females, the prevalence was higher among those aged 20–24 years (OR=1.47), who were married (OR=6.19), with one sex partner (OR=4.72), no education (OR=2.01), and secondary/higher (OR=1.46). Meanwhile, those in the urban area (OR=0.68), from average households (OR=0.68), and from the Ngoni ethnic group (OR=0.69) were significantly less likely to use condoms inconsistently. The study therefore indicates that females were more likely to use condoms inconsistently, and this facilitates the spread of HIV and other STIs among young people. The overall model for inconsistent condom use was therefore statistically significant for females, but not for males.
Adjusted odds ratio of inconsistent condom use among males and females aged 15–24 years by background characteristics in Malawi 2010.
Source: Malawi Demographic and Health Survey (2010), ***p<0.001, **p<0.01, *p<0.05, ®reference category.
Discussion
The use of condoms among young people is determined by individual behaviour and social factors. However, perceived self-efficacy among young people is one of the factors that can influence an individual to either use a condom or not. This concept is derived from social cognitive theory and it is a factor that could potentially lead to health-related behaviour (Bandura, 2004). Condom efficacy is therefore an individual’s confidence in his or her ability to use a condom successfully during sexual intercourse (Black et al., 2011). However, having these skills and being able to execute them under difficult conditions is an issue that is difficult for young people. Such efficacy therefore requires a reduction of risk and self-regulation of skills.
This study has shown that inconsistent condom use was more common among females 240 (35.6%) than males 147(28.7%), and this facilitates the spread of HIV/STIs, and is a major reason for female vulnerability to infections, thus increasing sexual risk behaviours. This finding is similar to other studies carried out in some parts of Sub-Saharan Africa. Mehra et al. (2014) found among Ugandan students that 37.4% males and 49.2% females did not use condoms consistently when they meet with new sex partners. Wang X et al. (2013) found in China, that 26.4% of HIV-infected adults inconsistently use condoms and this increases the risk for STIs. Ayoola et al. (2014) reported mixed findings in Nigeria that 40.5% men who have sex with other men in their last 10 sexual encounters, use condoms consistently. In another study, Matseke et al. (2012) found that 63.5% of tuberculosis infected persons in South Africa do not use condoms consistently, and this increases the risk for HIV and other STIs.
It has been evident that, lower education level, poverty, and partner’s abuse of alcohol before sex, and being married are contributing factors toward inconsistent condom use. Similarly, early sexual debut before 14 years, sex work not being a profession, and continuous consumption of alcohol have been evident to be contributing factors towards inconsistent condom use among female sex workers in Uganda (Bukenya et al., 2013). In another study, Haddad (2011) reported a higher rate of inadequate use of contraceptives and high unintended pregnancy due to partner’s refusal to use condoms consistently among women with HIV in Lilongwe. Furthermore, a study of female sex workers in Ethiopia found that, work related violence was a contributing factor to unprotected sex among young people, thus facilitating the spread of sexually transmitted infections (Mooney et al., 2013). In another study, Patel et al. (2014) reported that 10% of couples in India use condoms inconsistently in the past three months and the likelihood of inconsistent condom use was higher among partners who have suffered violence.
Wealth was also given considerable attention in the study as a contributing factor toward inconsistent condom use. Davidoff-Gore et al. (2014) found that lower income, food insufficiency and material transfer from partners were determinants of inconsistent condom use. According to findings from the study, those from rich households were more likely to use condoms inconsistently. A possible explanation of this could be the fact that, rich people have greater partner change and autonomy in most relationships, and studies have shown that, those with more than one sexual partner use condoms less frequently, and are more likely to transmit HIV and other STIs. As evident in the literature, having more sexual partners reduces the rate of condom use, thus facilitating the spread of STIs. Another group of researcher (Adebowale et al., 2014), found a higher prevalence of condom use of 82.4% among Malawian women in the richest wealth quintile than (66.8%) those in the poorest quintile. Morris et al. (2014) found among adolescents with a negative or unknown HIV status in the north-west of Cameroon that the majority (72%) of sexually active youths do not use condoms consistently. In another study, Kimani et al. (2013) found in a slum settlement of Nairobi, Kenya that, the risk of STIs, especially HIV, was associated with those that are married/divorced/widowed and being in the older age group, while Paul (2015) found that those with greater wealth inequality were more likely to have extramarital partners. In another study, Durevall and Lindskog (2012) found no effect of an individual’s poverty level on inconsistent condom use. This was different from the current study findings. Moreover, cultural taboos when talking of sexually related issues among heterosexual men affect consistent use of condoms (Stutterheim et al., 2013).
Study limitations
This study shows some strength, particularly because it is the first study on inconsistent use of condoms among sexually active youths in Malawi, and it has shown that inconsistent use of condoms accounts for an increasing number of HIV cases in Malawi. However, it focuses on the risk of HIV and other STIs among youths which is of high significance, especially to policy makers and planners. The survey data used for the study were self-reported and dependent upon the respondent’s ability to recall information such as condom use during last intercourse, and this may have resulted in either under or over reported responses. The limitation of the study therefore provides room for further research, particularly, the cross-sectional design which precluded the testing of explanatory models. Moreover, most of the scales and items had not been previously tested or validated in Malawi. Although these limitations might have affected the results in one way or the other, the study findings are useful in informing programmes and educating young people about the risk of HIV and other STIs when initiating risky sexual practices.
Conclusion
Although young males reported low levels of inconsistent condom use, factors such as communication among partners, and male dominated decision making in most sexual relationships create a lot of challenges when it comes to negotiating condom use. Moreover, since an individual’s behaviour can change over time, counselling programmes for HIV/STIs that encouraged safer sex through consistent condom use are of high priority, especially among females who reported a higher likelihood of inconsistent condom use. Considering the exploratory nature of the current study, it is recommended that in-depth studies be carried out in order to investigate an individual’s reasons for inconsistent condom use so as to reduce the risk of HIV and other STIs.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.