
Abstract
This study examined the association between health condition and conversion factors (i.e. environmental, individual and social) among workers in the ready-made garment (RMG) industry in Bangladesh. It used data gathered from a cross-sectional survey of 775 RMG workers in the Dhaka and Narayanganj districts. Using multiple logistic regression, the study found that: (1) achieving good health among RMG workers is hindered by various factors including high job-related demands, high noise levels, workplace crowding, heavy workloads, and low level of educational attainment; (2) job-related rewards and marital status have contributed to achieving good health; (3) health condition of workers is worse for women than for men; and (4) poor health condition is more prevalent among the oldest age group than in the lowest age category. The main contributions of this research: (1) this study develops a comprehensive framework to determine the factors affecting the health condition of manufacturing workers in general, and RMG workers in particular; and (2) it also examines the effects of both psychosocial and physical working conditions on the health of RMG workers.
Introduction
In 2010, Bangladesh ranked second among ready-made garment (RMG) exporters in the world (Bangladesh Garments Manufacturers and Exporters Association, 2016). The contribution of this sector to the national economy is enormous, leading the government to widely promote the industry. However, the reputation of the industry has been undermined by adverse working conditions including low wages, long working hours, tiring work and exposure to workplace violence.
It is in this climate that worker safety, security and health became serious concerns following the collapse of a factory building located in Rana Plaza, Savar (a sub-district of Dhaka), in April 2013 (Yardley, 2013). The lack of even minimum safety standards at the workplace along with the practice of irregular and meagre pay for workers have raised serious concerns. There is a general recognition of the need for revision and improvement of both safety standards and wages. After two industrial disasters (Tazreen Fashion in 2012 and Rana Plaza in 2013), working conditions in the RMG industry seemed to improve. More social compliance practices were introduced under the purview of the Ministry of Labour and Employment, Government of Bangladesh and the International Labour Organisation. However, the implementation of minimum wage law is still dubious (Asadullah and Wahhaj, 2016). Shortcomings are noted in the process of revising the Bangladesh minimum wage on a regular basis. For example, the government did indeed raise the minimum wage of the RMG industry four times in the last 20 years (i.e. in 1994, 2006, 2010 and 2013), but this was not done on a regular basis taking into account market value. Instead, it was only revised in response to massive public protests by the workers (Asadullah and Wahhaj, 2016).
Previous studies have identified various health problems among industrial workers in general, and garment workers in particular (De Silva et al., 2013; Gupta et al., 2015). Karasek and Theorell (1990) argued that poorly educated and low skilled workers are extremely susceptible to poor health. As a result of high physical demands in the manufacturing industry, blue-collar workers experience more health-related problems than white-collar workers (Lahelma et al., 2012). Therefore, it is necessary to identify the factors that are critical to improving the health of garment workers, and remove hindrances to good health. Apart from benefiting the workers, such measures will also have a positive impact on firm productivity.
There is now considerable study done on the physical and occupational health problems faced by garment workers in Bangladesh (Ahmed and Raihan, 2014; Gupta et al., 2015; Islam et al., 2014). Overcrowded work environments, verbal and physical abuse, high noise levels, inadequate ventilation, and the overall physical environment of the workplace seriously affect worker health. While these accounts are rich, they have not taken into account psychosocial working conditions and their effect on worker health. One study did broach psychosocial working conditions, but it only focused on workers in one firm (Steinisch et al., 2013). Furthermore, physical working conditions and health outcomes were not explored in that study.
In addition to examining subjects from a large sample of workers, we use the capability approach (CA) advanced by Sen (1992, 2001), which offers room to analyse the well-being of workers as an outcome variable (Mabsout, 2011). Functioning refers to ‘constitutive of a person’s being’ (Sen, 1992). Health is one of the basic functioning variables. Robeyns (2003) expanded the CA of Sen (2001) by discussing the conversion factors that are essential to achieving this functioning. Therefore, all conversion factors play important roles in either hindering or expanding the capabilities of humans. The relationships between the variables are shown in the conceptual framework (Figure 1). All three conversion factors (environmental, individual, and social) have been included to examine whether or not they influence health outcomes. In other words, the main aim of this study is to examine the effect of the conversion factors as expounded by the CA on the health condition of workers in the RMG industry in Bangladesh.

Conceptual framework.
The findings using the CA provide alternative policy interventions that could be used to improve working conditions of RMG workers in Bangladesh. Improvements in the health of workers will also improve the public image of garment factories in Bangladesh, which largely export to European and North American markets (Ahmed and Ahmed, 2011). The total number of workers employed in the RMG industry in Bangladesh was 4 million in 2015, which makes it one of the largest employers in the country (Bangladesh Garments Manufacturers and Exporters Association, 2016). Clearly, the long-term sustainability of garment industry employment depends heavily on worker health – therefore, research into the relationship between conversion factors and their effects on the health of workers is of paramount importance.
The remaining sections of the paper are organised as follows: the next section discusses the methodology, followed by an analysis of results and discussion; it finishes with the conclusions and identifies areas for future research.
Methodology
There has been increasing interest in the impact of working conditions on worker health, following the expansion in global value chains and the tightening of trade regulations on working conditions at host-sites in major markets (e.g. Barrientos et al., 2011). However, most researchers focused on case studies using qualitative analysis. In contrast, this study is based on a quantitative analysis using a large data set, and makes a significant contribution by complementing previous research.
Conceptual framework
We adapted the capability framework proposed by Robeyns (2005), which in turn was based on the principles of Sen’s (2001) CA. Capabilities can be expanded or constrained depending on conversion factors (Tao, 2010), as they are means by which individuals can convert resources to functions. According to Robeyns (2005), capabilities consist of a combination of functioning, either potential or achieved, and can be categorised into:
individual conversion factors (e.g. intelligence, skills, age, gender and education);
environmental conversion factors (e.g. geographical location, logistics and infrastructure); and
social conversion factors (e.g. social norms and gender relations, roles and identities).
The role of conversion factors is critical in converting the characteristics of goods into individual functions, and they help to translate the conditions into capabilities.
Figure 1 illustrates how conversion factors contribute to shaping the capability set of workers with information on three distinct kinds of indicators:
environment (psychosocial working conditions, physical working conditions and workload),
individual (age, education, and gender), and
social (marital status).
We have chosen proxies to measure conversion factors (environmental, individual and social) and determine the relationship between them and health functioning. ‘Capabilities’ refers to the freedom or opportunity enjoyed by an individual to perform work; that is, by being healthy. Conversely, the conversion factors may restrict capability, and result in poor health functioning. All three conversion factors can either restrict or expand capability. On the one hand, psychosocial and physical working conditions could contribute to illness or poor health of workers, as well as affect the choices or freedom of workers. On the other hand, these environmental conversion factors could contribute to good health. Individual conversion factors (e.g. education, age and gender) and social factors (e.g. married or unmarried) could improve the health of workers. Because the determinants of health functioning are the conversion factors, we attempt to identify the conversion factors that contribute to positive health functioning among low-wage garment workers in Bangladesh. This is illustrated in Figure 1.
Conversion factors and effort-reward model
The Effort-Reward Imbalance Model (ERIM) developed by Siegrist et al. (2004) is based on two components – efforts and rewards. It posits that when efforts (e.g. pressure to finish work on time) are not sufficiently rewarded (e.g. an adequate salary, good promotion prospects, job security and recognition), it may cause distress to workers and eventually weaken their health. Nieuwenhuijsen et al. (2010) considers adverse working conditions as a major determinant of worker health. ERIM emphasises the environmental factors in the workplace – when these factors are favourable, workers are likely to experience reasonable levels of good health; whereas if these factors are unfavourable, worker health could be adversely affected. However, the model did not take into account individual and social factors. To address that shortcoming, this study mainly adapted the capability frameworks of Robeyns (2005) and Sen (2001), and also incorporated some questions from the ERIM questionnaire to formulate a more comprehensive set of proxies on environmental factors that affect workplace settings.
According to Danielsson et al. (2015), the workplace constitutes two factors: psychosocial and physical environment. Both contribute to stress in the workplace. The importance of psychosocial working conditions in enhancing worker health has been well recognised (e.g. Nieuwenhuijsen et al., 2010; Steinisch et al., 2013). In addition, researchers also identified workplace noise (Jahncke et al., 2011) and crowding (De Croon et al., 2005) as environmental factors that can create stress at the workplace; these have been used as measures of the physical working environment (Loscocco and Spitze, 1990). Excessive noise is detrimental to health and could pose a threat to the quality of life of workers, as it causes stress at the workplace (Chauhan and Pande, 2010; Evans and Johnson, 2000). Given the importance of both psychosocial and physical working conditions in the RMG industry of a least developed country (LDC), we included both variables in the conceptual framework as environmental conversion factors. The use of individual conversion factors in this study is similar to previous studies (e.g. Otto and Ziegler, 2006; Robeyns, 2003). Marriage is a social institution, and Robeyns (2005) considered social institutions as a social conversion factor. Therefore, in the proposed conceptual framework, environmental conversion factors comprise psychosocial and physical workplace environments; individual conversion factors are age, gender, and education; and marital status is considered to be the social conversion factor.
Data, sample size and sampling
In light of the lack of data, we opted to collect primary data on garment workers in Bangladesh. The dataset was collected via fieldwork conducted between May and November 2015, using a structured questionnaire as the primary instrument. In order to obtain an appropriate sample size, the following formula was used (Lind et al., 2007):

where n is the minimum size of the sample, π (0.50) is the population proportion, Z is the standard normal value corresponding to the desired level of confidence, and E is the maximum allowable error. Based on the formula for sample size, Z = 1.96 (95% confidence level), π = 0.5 and E = 5%. The above function is appropriate for infinite population size sampling and a minimum sample size of 385. According to Krejcie and Morgan (1970), this figure is an appropriate sample size, so it can be argued that the outcome of the current study should not raise concerns of bias due to the sampling procedure used.
Sampling frame. The study used multistage random sampling to collect data. Garment factories are located in nine districts in Bangladesh (Department of Inspection for Factories and Establishments, 2015). We have divided the whole of Bangladesh into nine clusters, as they are homogeneous in nature. After that, we chose the districts of Dhaka and Narayanganj randomly (i.e. through a lottery method) following the database of the Department of Inspection for Factories and Establishments under the Ministry of Labour and Employment.
According to the Bangladesh Bureau of Statistics (2013a), Dhaka district has 41 Thana 1 and six Upazila. 2 We randomly selected five Thana (namely Mirpur, Gulshan, Mohammadpur, Tejgaon Industrial Area and Tejgaon) and one Upazila (namely Savar) using a lottery method. There are 1961 factories in Dhaka district, and 734 factories in Narayangonj district (Department of Inspection for Factories and Establishments, 2015). Next, using the database of Department of Inspection for Factories and Establishments, we randomly selected seven factories from each of the six administrative units – for a total of 42 factories. Finally, using the factory registers, we selected 420 workers (i.e. 10 workers from each factory). 3 We collected 400 valid responses using face-to-face interview technique.
The same sampling frame and mode were used to decide the sample size for Narayanganj District. According to the Bangladesh Bureau of Statistics (2013b), Narayanganj District has five Upazila and six municipalities. We selected five Upazila (namely Narayanganj Sadar, Bandar, Rupganj, Sonargaon, and Araihazar) and then selected seven factories randomly from each administrative unit, for a total of 35 factories. Using the factory registers, we chose 12 workers from each factory – for a total of 420 workers. We collected 375 valid interviews from these 420 randomly selected respondents. Overall, 775 interviews were completed, out of which the respondents were 560 female and 215 male. 4
Analytical technique
The logit model is a commonly used model when the response variable is a dichotomised binary response. According to Greene (2003), logistic regression is used to predict the probability of an event occurring or not occurring, by fitting data to a logit form. The equation for the logit model is as follows:

where p = Prob (Y = 1) is the probability that an individual reports absenteeism due to poor health, β0 is the intercept parameter, and β1 is the regression coefficients of the ith variable in the model.
The description of the selected variables used for the study is shown in Table 1.
Definition and measurement of the variables.
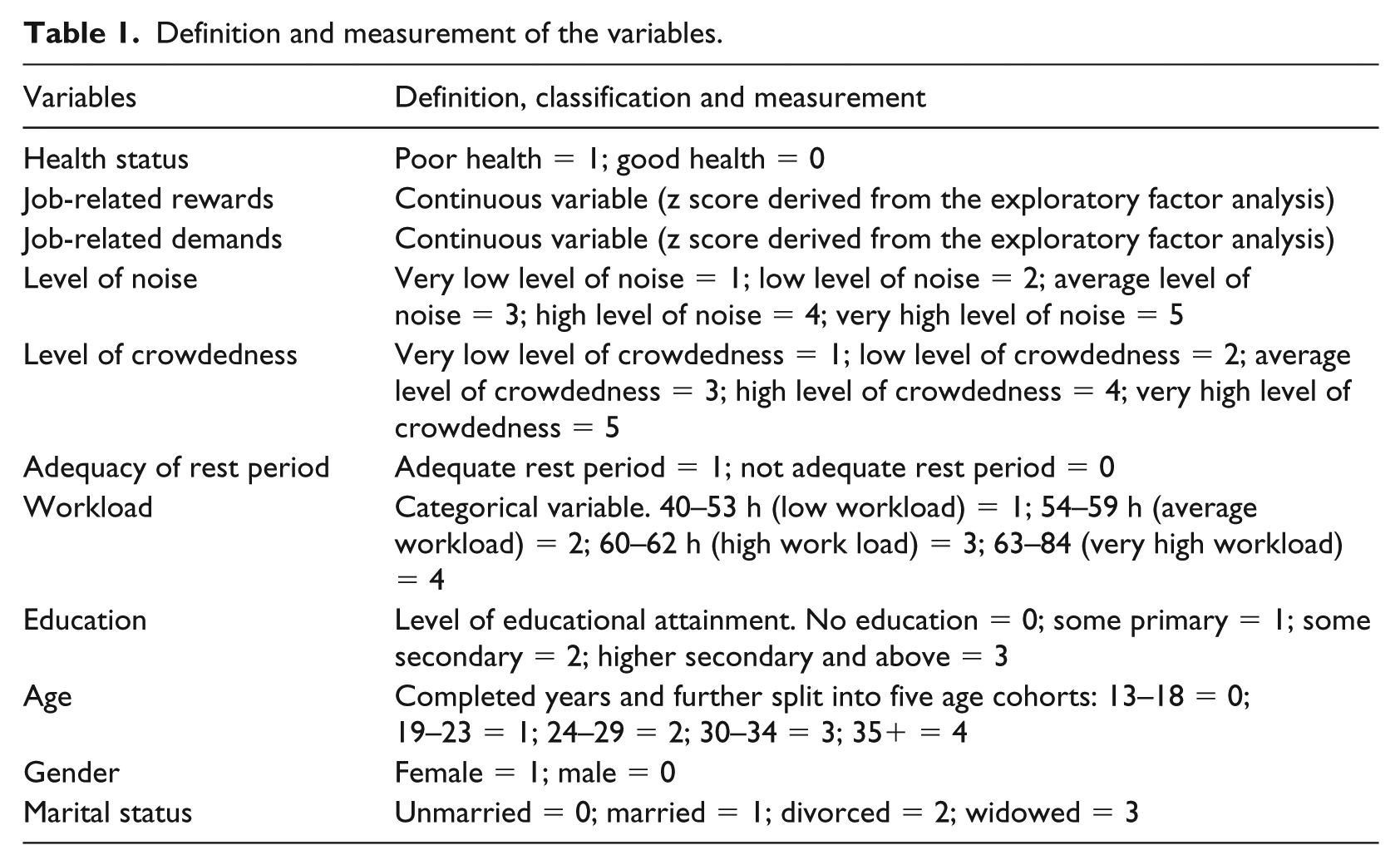
Dependent variable. Sickness absence or absenteeism due to poor health is a global measure of health status and an indicator of social, psychological and physical functioning for working people (Marmot et al., 1995). It is evident that the longer the period of sickness absence, the poorer the health status (Niedhammer et al., 2013). Occurrence of sickness absence happens as a consequence of several work-related factors, and it is one of the proxies for gauging the health status of workers. We asked the respondents whether they had been absent from work due to illness in the previous year.
This measure was dichotomised by grouping response scores into health absenteeism occurrence as a category of poor health, and health absenteeism non-occurrence as a category of good health. Therefore, the dependent variable is scored as follows: Y = 1, if a worker is absent due to poor health; Y > 0 Y = 0, otherwise; Y = 0
Independent variables: Psychosocial working conditions. We used the shortened version of the ERIM questionnaire that had previously been used for analysing the health outcomes of RMG workers (Dragano et al., 2010; Steinisch et al., 2013). In line with the previous studies, we measured efforts based on the perceptions of the workers – including physical demands and time pressure. Reward was measured using five aspects: social support, salary, recognition, promotion prospects and job security. We recorded all affirmative answers as ‘strongly disagree’ to ‘strongly agree’ to maintain the consistency of the respondents’ scores in a five-point Likert scale (1 = ‘strongly disagree’ and 5 = ‘strongly agree’). The full list of items is provided in Appendix A.
Independent variables: Physical working conditions. A five-point Likert Scale was used to measure stressors in the physical working environment – noise and crowdedness. Respondents were asked to rate noise levels and the degree of crowding at their workplace, with categories ranging from 1 for ‘very low noise’ to 5 for ‘very high noise’ and the same range for ‘very low crowding’ to ‘very high crowding’. In addition, workers were also asked whether the rest breaks provided by the factories were adequate or not, thus providing a dichotomous variable where 1 indicated ‘sufficiently adequate’ and 0 indicated ‘not adequate at all’.
Paul-Majumder (1996) found that long working hours in the RMG industry was the factor most adversely affecting the health status of workers. The RMG industry has often been criticised for its long working hours (Yunus and Yamagata, 2012), and studies have identified this as a factor causing psychosocial illness among the RMG workers (Padmini and Venmathi, 2012). Hence, we have included industry-specific working conditions (working hours per week as a proxy to measure workload) in this study.
Independent variables: Individual and social conversion factors. Education, gender and age were used as categorical variables and individual conversion factors, while marital status (which is also a categorical variable) was considered as a social conversion factor.
Independent variables: Exploratory factor analysis. An exploratory factor analysis (EFA) was conducted in order to determine the potential elements of the psychosocial working environment. We used orthogonal rotation (Varimax) which allows for correlation between potential factors. To test the sensitivity of the analysis, we ran additional analyses based on oblique rotation (Promax). Both indicated the correlation of potential factors.
At the beginning, we identified factors based on the eigenvalue exceeding 1. The EFA suggested two factors on the basis of this criteria. We label the first factor as job-related rewards that comprises four items: support, recognition, adequate salary, and promotion prospects. The second factor is labelled as job-related demands and consists of two items: physical demands and time pressures. Importantly, the items that belong to a particular factor have loadings of 0.5 or higher (see Table 2). The factors identified via EFA are very similar to the factors found by Steinisch et al. (2013), but they had instead identified three factors. The loadings of the items of our study do not allow for three factors. Sampling might be the reason for this result, as the above-mentioned study was based on only one garment factory. Cronbach’s alpha was computed for each of the identified factors, with job-related rewards at 0.616 and job-related demands at 0.552.
Exploratory Factor Analysis of the seven items on psychosocial working conditions or work stress (N = 751).
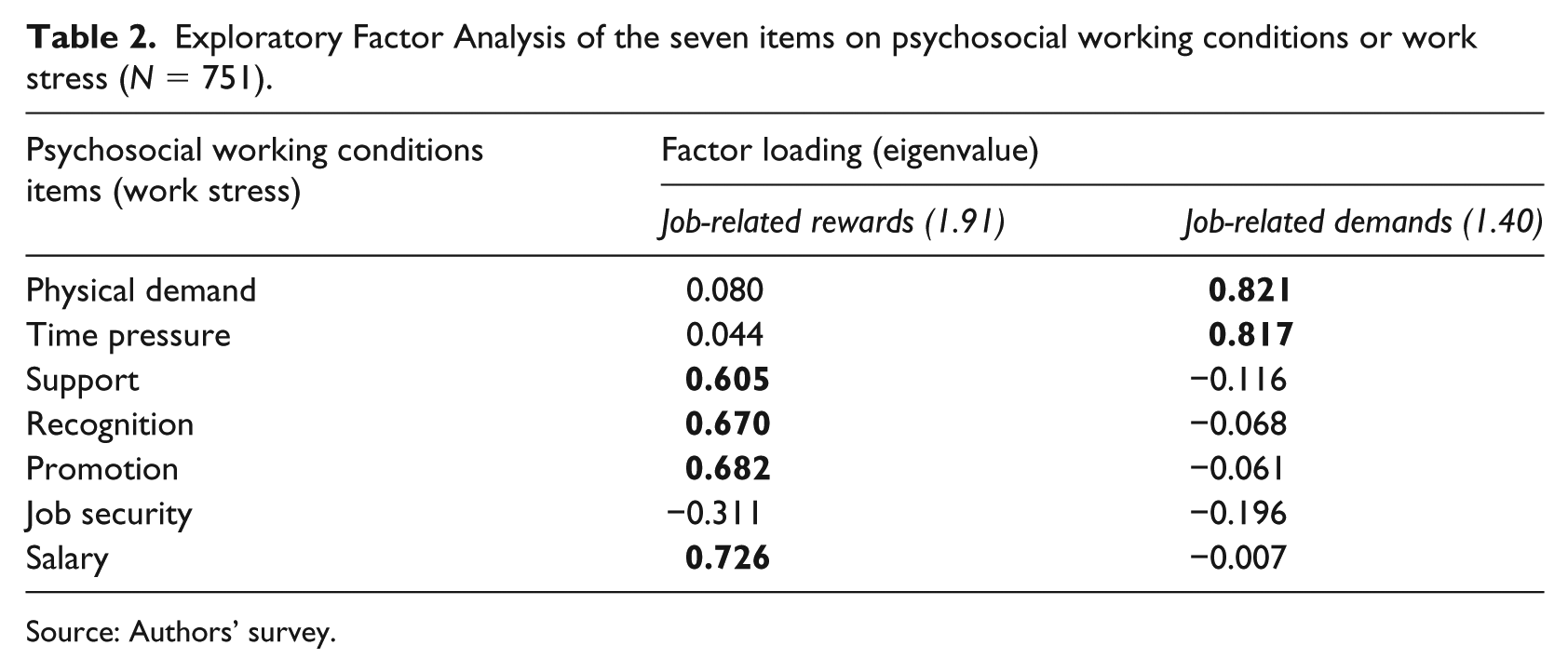
Source: Authors’ survey.
Model specification. According to the capability framework, we estimate the health status equation as follows:

Here, JR and JD denote job-related demands and job-related rewards, respectively, that we derive from the EFA; noise, crowd, and restp represent the level of noise, crowding, and adequacy of rest breaks, respectively; wl denotes working hours per week (proxy to measure workload); and education, age, and ms (marital status) are measured as categorical variables. Gender denotes a binary variable where female is coded as 1 and male is coded as 0.
Results and discussion
The correlation matrix of the independent variables is shown in Appendix B. The variance inflation factor and tolerance statistics also show that there is no multicollinearity problem among independent variables (see Appendix C).
Table 3 presents the percentage distribution of all categorical variables. We were not able to make the percentage distribution of JR and JD with the health conditions, as both are continuous variables. The Chi-squared test is used to test the significant differences among the various categories and subgroups of variables. Table 3 shows that the majority of workers who reported high levels of noise, crowdedness and inadequacy of rest period were in poor health. It is also evident from Table 3 that the majority of workers who reported poor health status (61.66%) have a very high level of workload (working hours per week of 63–84 hours). While exploring the effects of education, we can see that those who have no education reported poor health status more in terms of percentage distribution (69.23%). Only 39.71% of the lowest age category (13–18) reported poor health, in contrast to 68% among the oldest age category. Marital status is found to be an important factor for determining health condition, with a higher percentage of divorced workers reporting poor health compared to other categories. We also found a gender difference among those who reported poor health: 54.11% of female and 33.95% of male workers reported poor health status. A previous study that examined the association between poor health and psychologically adverse working conditions found that 67.9% of female and 56.6% of male workers were in poor health (Paul-Majumder, 2003). This may partly be explained by the impact of some recent developments in the sector, such as changes made to the minimum wage law (which was amended three times) and continuous international pressure on health and safety issues in the RMG industry. These factors appear to have made wages and working conditions more favourable compared to the past.
Percentage distribution of categorical variables and poor health of RMG workers.

Source: Authors’ survey.
Here, 48.52% of the respondents reported that they were absent from work during the previous year due to illness, indicating that poor health is a factor for nearly half of the workers. Based on the diagnostic test of logistic regression (Hosmer-Lemeshow Test with a p value = 0.758), we could say that our model fits the data well.
Table 4 presents the results of a multiple logistic regression analysis against all independent variables, using a dummy dependent variable (1, 0) for the question of whether respondents were absent or not absent from work due to poor health. The first and second columns present estimates of the expressions in equation (1) with coefficient values and odds ratio (OR) values. The logistic regression reveals a negative and statistically significant relationship between job-related rewards and poor health of RMG workers. It suggests that a one-unit increase of job-related rewards decreases the log odds of being in poor health by −0.354 of a unit. This is in contrast with the study conducted among 332 workers of a garment factory based in the capital city of Dhaka (Steinisch et al., 2013). The difference might be the result of different sampling frames. It is worthwhile to mention that high work-related rewards were found to be an important component in other studies that looked at high-income countries (Lau, 2008). The OR of job related rewards was 0.701.
Results of multiple logistic regression.

Robust SEs are in parentheses.
p < 0.10, **p < 0.05, ***p < 0.01.
OR: odds ratio; CI = confidence intervals; RC: reference category; SEs: standard errors.
Source: Authors’ computation.
There is a positive and significant association between high job-related demands and poor health. According to equation (2), a one-unit increase of job-related demands increases the log odds of poor health by 0.200 of a unit. The OR is 1.222, which suggests that those who reported high job-related demands are likely to have poor health status. This finding is consistent with another study of the RMG industry in Bangladesh (Steinisch et al., 2013), where they found a positive association between poor health and high job-related demands.
Regarding noise levels, a very low level is used as the reference category. Noise level was found to be highly significant at average, high, and very high levels, and the relationship with absenteeism due to poor health was positive. This indicates that higher noise levels affected the health conditions of RMG industry workers. Note that coefficients and OR increased when moving from average to high, and from high to very high noise levels (ORaverage noise level = 2.211, ORhigh noise level = 2.541, ORvery high noise level = 5.463). This indicates that higher noise levels are significantly associated with poor health of workers. Therefore, we can conclude that the higher the level of noise, the higher the probability of absenteeism due to poor health. A high level of noise is one of the factors responsible for poor health status of workers. This result is consistent with previous findings on industrial noise being an underlying cause of poor health among workers in American manufacturing companies (Cohen, 1974) and among European blue-collar workers (Melamed and Green, 1991).
Workplace crowding also showed a positive relationship with absenteeism due to poor health. Very low crowding was used as the reference category, and crowding in the workplace was found to be consistently significant – starting from very low all the way to very high levels. It should be noted that when workplace crowding shifted from very low to low levels, from low to average levels, from average to high levels, or from high to very high levels, then both the coefficients of crowding levels from average to very high-level crowding and the adjusted OR increased simultaneously. The OR of crowding at high and very high levels of crowdedness were 4.727 and 5.029, respectively. This finding is consistent with the outcomes of other studies (Lamminpää et al., 2012; Pekkarinen et al., 1979) that noted crowding as a contributing factor detrimental to health.
Adequacy of rest breaks was found significant in model 1 at the 5% level. It suggests that a one-unit increase of adequacy of rest breaks decreases the log odds of being in poor health by 0.554 of a unit. This outcome has been endorsed by Taylor (2005).
Working hours per week was used as a proxy in order to estimate workload, and the results suggested that workload influenced the health conditions of workers. We found a positive and statistically significant relationship between workload and poor health conditions of workers. We used low workload as the reference category. The result suggests that average and high workloads increase the probability of being in poor health when compared against low workload. The OR also indicates that the chance of being in poor health is 2.351 higher for those who have very high workload comparing with those who have low workload, similar to the findings of previous studies (Bannai and Tamakoshi, 2014; Paul-Majumder, 1996).
From the analysis, this study reveals that individual conversion factors such as education, age and gender are associated with health condition. From Table 4, it can be seen that the adjusted OR for no education, primary education, and secondary education stood at 5.855, 4.955, and 3.248, respectively, against the reference category that represents the highest level of educational attainment (higher secondary level and above). The effect is found to be the highest among those with no education, in contrast to those with the highest level of education. In addition, the groups with some primary and secondary levels of educational attainment also reported a higher probability of being in poor health when compared to the group with the highest level of education. This finding is also consistent with the previous literature (Adams et al., 2003; Ross and Wu, 1995). By looking at gender where male is used as the reference category, the results suggest a positive and significant association. It implies that the chances of reporting poor health are 2.227 times higher for a female worker in comparison to a male worker. This is consistent with the previous findings in RMG settings in Bangladesh (Paul-Majumder, 1996). Furthermore, age was found to be an important factor. Those who are in the oldest age category have a 3.061 times higher chance of reporting poor health condition than those who belong to the lowest age category, a finding that is consistent with existing literature (Khan and Flynn, 2015).
Turning to marital status, being unmarried is used as the reference category. Although being married decreases the logarithmic probability of being in poor health, it is found statistically significant at a 10% level. Hence, the effect is not much stronger compared to the effects of other significant variables. This result is also consistent with the findings of previous studies (Khan and Flynn, 2015).
Conclusion
This paper examined the relationship between health status and the conversion factors of environmental, individual, and social conditions of RMG workers in Bangladesh, using a comprehensive framework based on the capability approach of Robeyns (2005), Sen (2001) and the Effort–Reward model of Siegrist et al. (2004). It employed cross-sectional data comprising 560 female workers and 215 male workers in the Dhaka and Narayanganj districts to find out the factors affecting health conditions of RMG workers. The dependent variable was whether the respondents were in good health or poor health. The study considered those who were absent from work due to illness as being in poor health, and identified the factors that were responsible for poor health or that hindered the achievement of good health. Multiple logistic regression was used for data analysis.
The results showed that the following conversion factors constrained the capability and choice of workers in achieving good health functioning: high job-related demands, high noise levels, high crowding in the workplace, increased workload, and low level of educational attainment. However, it also found that high job-related rewards and being married expanded the capability to achieve a level of good health functioning. Furthermore, the study revealed that being a female worker increased the probability of having poor health condition. Poor health was prevalent among the oldest age group of workers, which is also a consequence of ageing.
The empirical evidence supports the role of conversion factors to increase the capability of RMG workers in enhancing health functioning. Hence, environmental, individual and social conversion factors play a significant role in shaping the health status of RMG workers in Bangladesh. By examining how the conversion factors shape the health status of RMG workers, the study firstly confirms that both psychosocial and physical working conditions are crucial to enhance the health status of RMG workers. Secondly – in particular for RMG workers – environmental conversion factors matter more than individual and social conversion factors. This study confirms the fact that women face more difficulty in achieving good health status than men, which also concurs with previous findings (Paul-Majumder, 1996, 2003). Clearly, women are at a disadvantage in achieving capability and health functioning. Previous studies have used either psychosocial working conditions (Steinisch et al., 2013) or physical working conditions. We have instead combined both psychosocial and physical working conditions – something that has been seldom used in the literature in examining the health conditions of manufacturing workers in general, and RMG workers in particular.
A number of policy implications can be drawn from this study:
Employers or owners need to be aware of psychosocial working conditions – by reducing the high physical demands of jobs and time pressure, they can improve the poor health status of RMG workers. Another set of psychosocial working conditions that employers or owners should be aware of includes good promotion prospects, recognition of work, adequacy of salary and support – improving these conditions may facilitate improvements in the health status of workers. Reducing noise levels and workplace crowding are likely to contribute to better conditions and a reduction in absenteeism due to poor health. Reducing working hours is likely to have a positive impact on improving the health status of RMG workers. Firm owners need to take necessary steps to provide proper health services, in particular to women workers.
Although the results of this study are robust, they should be treated with caution since this study relies on a cross-sectional rather than a panel dataset – the latter of which is important to establish causality. There was also no comparison made between the health status of workers in the RMG industry against other manufacturing sectors. Future studies should focus on following a sample of RMG industry workers over time and attempt to compare findings with research on other manufacturing sectors. In addition, the influence of environmental, individual and social conversion factors could also be measured separately both for physical and mental health. Moreover, future studies in RMG settings also can use different measures of health outcome (e.g. biomarkers, self-reported health status) instead of the proxy of absenteeism due to poor health, in order to see whether the results differ or remain the same.
Footnotes
Appendix
Variance inflation factor and tolerance statistics.
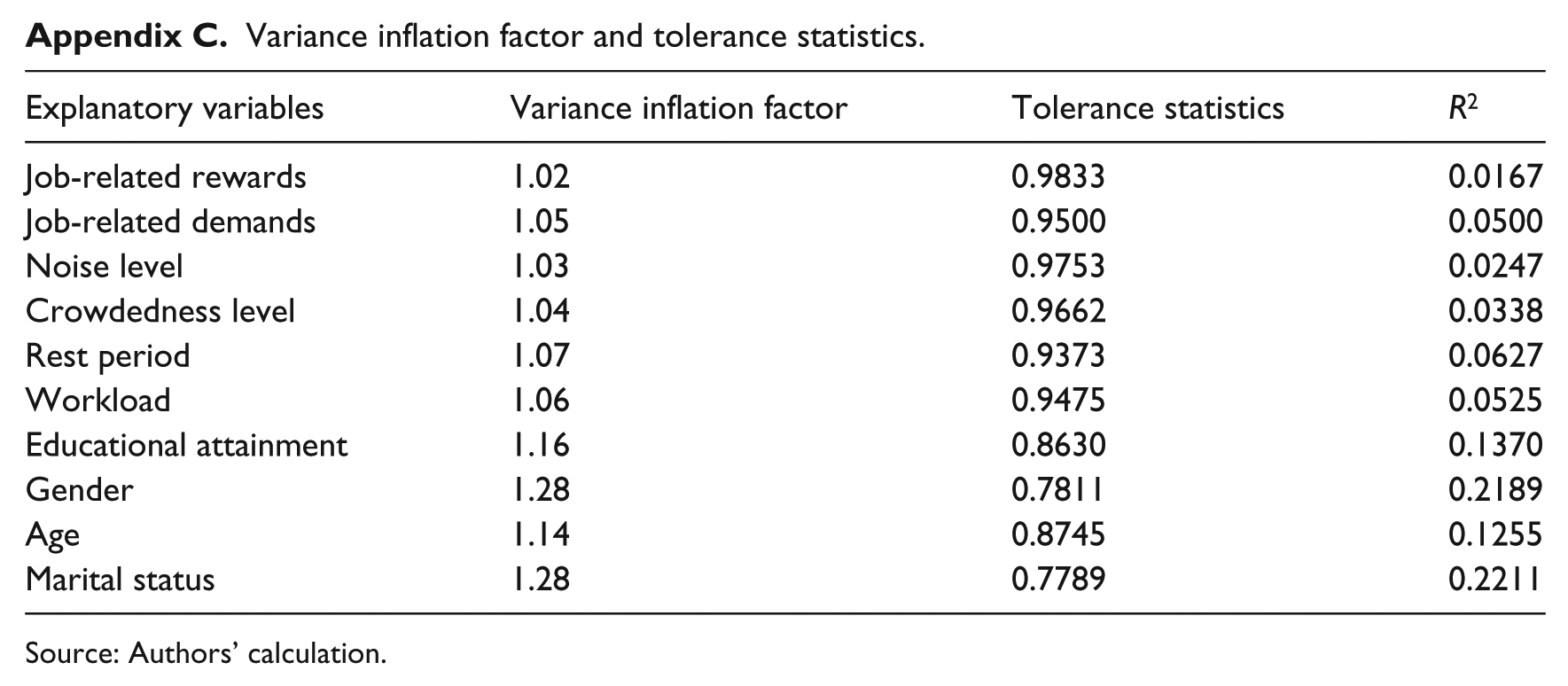
| Explanatory variables | Variance inflation factor | Tolerance statistics | R 2 |
|---|---|---|---|
| Job-related rewards | 1.02 | 0.9833 | 0.0167 |
| Job-related demands | 1.05 | 0.9500 | 0.0500 |
| Noise level | 1.03 | 0.9753 | 0.0247 |
| Crowdedness level | 1.04 | 0.9662 | 0.0338 |
| Rest period | 1.07 | 0.9373 | 0.0627 |
| Workload | 1.06 | 0.9475 | 0.0525 |
| Educational attainment | 1.16 | 0.8630 | 0.1370 |
| Gender | 1.28 | 0.7811 | 0.2189 |
| Age | 1.14 | 0.8745 | 0.1255 |
| Marital status | 1.28 | 0.7789 | 0.2211 |
Source: Authors’ calculation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.