
Abstract
This paper explores the predictors of HIV/AIDS awareness and knowledge among older and younger Ghanaian women of reproductive age. Logistic regression was estimated using the 2014 Ghana Demographic and Health Survey data. Results indicate that older Ghanaian women are significantly different from their younger counterparts in terms of the selected socio-economic and demographic characteristics that influence awareness and knowledge of the epidemic. In all, the respondents’ age, region of residence, wealth status, education, marital status and religious affiliation were found to significantly predict knowledge and awareness of HIV/AIDS among women. In addition, pregnancy status and place of residence proved to be significant correlates of HIV/AIDS awareness among Ghanaian women. The study suggests that higher social status is critical in determining whether women of reproductive age are aware of and knowledgeable about the epidemic. Thus, there is the need for policies and interventions to target messages taking into account the varied socio-economic and demographic backgrounds of women in Ghana. Further, health education interventions should be sensitive to the changing technological landscape in order to develop messages that can be delivered via mobile phones, whether as reminders or ringtones, and therefore enhance health knowledge and promote behaviour that brings about desirable health outcomes.
Introduction
The incidence of HIV remains high in Sub-Saharan Africa, with the region recording the highest incidence globally in 2015 (United Nations, 2017). This is a worrying situation in light of the fact that in January 2010, the United Nations Security Council held a meeting devoted to the security impact of HIV/AIDS in Africa, and as a consequence, several national governments adopted a number of high-profile declarations of commitment and multilateral agreements to combat the emerging threat (Vieira, 2011). Significantly, at the global level, the decline in new HIV infections among adults have stalled, with the number of new infections rising in some regions of the world (UNAIDS, 2016).
The situation in Ghana is mixed, with the Ghana Aids Commission (GAC) reporting that the country is ‘experiencing a mature mixed epidemic comprising…a low-level generalised epidemic’ with an incidence of 1.47% among the general population (GAC, 2016). The current situation regarding HIV/AIDS prevalence is a reflection of the continuous efforts by the Government of Ghana to address the pandemic. Presently, the fight against HIV/AIDS is anchored on the National HIV and AIDS Strategic Plan (NSP). The goal of the NSP (2011–2015) was to reduce new infections by 50%, whilst that of the NSP (2016–2020), developed with the Sustainable Development Goals in mind, aims to speed up efforts to end AIDS by 2030. Clearly, this is a huge task in light of changing socio-cultural attitudes towards sex and HIV/AIDS in general.
Central to the attainment of these objectives is increased knowledge and awareness of the disease, and changes in sexual behaviour among the general population, particularly those at greater risk of new infection. Because of the socio-cultural and economic dynamics in Ghana, women are usually at greater risk of new infection than men. The 2014 Status Report of the GAC shows that for persons living with HIV, 59% were females, with the majority being adults. Moreover, new infections were higher among females compared to males in the 15–24 age-group. Further, projected estimates of the prevalance rate of HIV from 2014 to 2020 show that females aged 15–49 years have a higher HIV prevlance compared to males. Similarly, in the case of new infections for the same period, the estimates show that more females are likely to be infected compared to males (GAC, 2016). Indeed, the 2016 HIV Sentinel Report by the National Aids Control Programme shows an increase in prevalence rates among pregnant women.
In spite of the general sense of increased risk for adult women, information available from national datasets suggests a decline over time in HIV/AIDS awareness and knowledge among women of reproductive age in Ghana. For instance, HIV/AIDS awareness declined from 98.37% in 2003 to 97.57% in 2014, approximately a percentage point decline. Similarly, knowledge of HIV/AIDS declined from 55.37% in 2003 to 47.81% in 2008 and finally to 42.77% in 2014 (Ghana Statistical Service (GSS) et al., 2015). Thus, in a little over a decade (2003–2014), comprehensive knowledge of HIV/AIDS declined by a whopping 12.6 percentage points. Thus, with the objective of reducing and ultimately ending new HIV infections, the observed declining trend, especially in the case of knowledge of HIV/AIDS, implies that greater efforts at increasing awareness and knowledge leading to behavioural change amongst women of the reproductive age must be critical.
Evidently, HIV/AIDS is prevalent among women of reproductive age within the population. Thus, invariably, one might want to distinguish the broad category of females into younger and older women, particularly because of differences in their socio-economic characteristics. The purpose of this paper is to investigative the determinants of HIV/AIDS awareness and knowledge among these distinct groups of women. We differentiate women into these distinct groups because we expect that the differences in age will suggest that these categories of women of reproductive age are likely to experience unique sets of factors influencing their vulnerability to HIV infection, and hence the higher prevalence recorded among this group within the population.
There is adequate literature on awareness and knowledge of HIV/AIDS in Sub-Saharan Africa, and Ghana in particular. It is recognised that a range of social factors such as residential conditions, age, education, occupation and health services provision inter alia are important in determining health seeking behaviour and outcomes (Nketiah-Amponsah and Afful-Mensah, 2013; Yaya et al. 2016a, 2016b; Zhao et al. 2010). Nevertheless, individual decisions are crucial in influencing the choices made in relation to the individual’s health status (Grossman, 1972, 1982). Further, as noted by Sutton (2005), health behaviours or health-related behaviours may be critical in affecting an individual’s health, although it is also recognised that health behaviours may be influenced by biological, psychological and social factors.
Awareness and knowledge of HIV/AIDS is crucial in curbing the spread of the disease and its potential devasting impact (Zhao et al., 2010). Sareen et al. (1996) argued that a better level of health awareness can trump the effects of differences in socio-economic status on health outcomes. Indeed, several theoretical approaches have explored the linkages among socio-demographic factors, health awareness and health outcomes (see Edwards et al., 2012; Paasche-Orlow and Wolf, 2007; Al Sayah, 2012). This paper opines that health awareness and knowledge fit neatly within the definition of health literacy (Keating, 2006). In that regard, McCormack’s (2010) framework for individual health literacy offers a good theoretical setting to analyse the determinants of HIV/AIDS awareness. McCormack’s analytical framework demonstrates how health literacy is influenced by individual and external factors. These external factors include, socio-demographic characteristics. Critical in this analytical framework is the link between these socio-demographic characteristics and health literacy, which ultimately influences the health status of the individual.
In a more recent study in Bangladesh, Yaya et al. (2016a, 2016b) reported that slightly more than half of Bangladeshi women had good knowledge of HIV transmission, and that education and gender of the household head were found to be significantly aassociated with HIV knowledge. The importance of education in promoting knowledge or information on HIV/AIDS is corroborated by Zhao et al. (2010) in their study among adolescents in China. In a study among pregnant women attending antenatal care in Nigeria, Abioudun et al. (2007) reported a complete awareness of HIV/AIDS by the respondents except in the area of mother-to-child trainsmission, where only 68% were aware of this medium of transmission. It was further reported that electronic media remained the major source of information for the pregannt women (see also, Keating et al., 2006). Other studies have reported the influence of income, illiteracy, gender and religion in explaining differences in knowledge and awareness of HIV AIDS (Asante, 2013; Fenny et al., 2017; Mosharaf et al., 2014; Pascoe et al., 2015; Piot et al., 2007).
Although there is extant literature on HIV/AIDS knowledge and awareness in Ghana, what remains puzzling is the declining awareness and knowledge of HIV/AIDS against the backdrop of the sustained educational campaigns on HIV/AIDS in Ghana. Although knowledge of the epidemic among women is almost universal (97.56% in 2014), a decline in HIV/AIDS comprehensive knowledge from 55.37% in 2003 to 42.77%, a 12.6 percentage points decline over the period (GSS et al., 2015), is alarming enough to warrant a current investigation into the factors that promote awareness and knowledge and those that retard same to help restrategise campaigns and education on the epidemic. Moreover, this paper focusses on women because 59% of the persons living with HIV in Ghana are women (GAC, 2016), coupled with the fact that they are usually at greater risk of new infection than men. There is also evidence of an increase in the prevalence rate among pregnant women. Using the most recent and nationally representative data, this study examines how socio-economic and demographic factors influence HIV/AIDS awareness and knowledge among women in Ghana. Considering the social and economic impact of HIV/AIDS, the findings from this study have useful implications for the HIV/AIDS prevention campaign in Ghana, and to inform policy formulation that address other public health interventions.
Methods
Data
Data were obtained from the most recent Ghana Demographic and Health Survey (GDHS). This survey is nationally representative. It was conducted in 2014 by the GSS in collaboration with other stakeholders. The 2014 GDHS followed a two-stage sampling design. The first stage involved the random selection of clusters, which consisted of enumeration areas. Altogether, 427 clusters were selected. In the second stage, households were systematically selected. A total of 12,831 households were selected in the 2014 GDHS. The successfully interviewed households, however, numbered up to 11,835 – yielding a 98.5% response rate (GSS et al., 2015).
Our focus in this study is on women, hence we used the responses of women from the 2014 GDHS. In total, 9396 women were successfully interviewed. This yielded a response rate of 97.3%, given that 9656 women were eligible to be interviewed (GSS et al., 2015). The women sampled were in the age range of 15–49 years. We used data on 9392 women to explore the correlates of HIV/AIDS awareness, and data on 7829 women to examine the correlates of HIV/AIDS and knowledge (of the illness). The choice of these number of women was informed by the availability of data on the variables of interest. In addition to collecting data on HIV/AIDS awareness and knowledge, the GDHS collects data on the socio-economic and demographic characteristics of respondents.
Outcome variables
In the 2014 GDHS, the sampled women were asked questions about their awareness and knowledge of HIV/AIDS. On one hand, they were asked whether, or not, they had ever heard of AIDS. The main response was either a ‘yes’ or ‘no’, although in some cases respondents could not ascertain whether or not they knew the answer to the question. Conversely, the analysis of the correlates of knowledge about HIV/AIDS was based on four questions. These are as follows:
Can you get HIV by sharing food with a person who has AIDS?
Can you get HIV from mosquito bites?
To reduce risk of getting HIV, should you always use condoms during sex?
To reduce risk of getting HIV, should you have one sex partner only, who has no other partners?
To arrive at comprehensive knowledge about HIV/AIDS, the women who answered all four questions correctly were scored 1, otherwise 0, where at least one of the four questions was wrongly answered. In both cases (correlates of HIV/AIDS awareness, and correlates of knowledge about HIV/AIDS), the outcome variables are binary. There were cases where respondents failed to answer the questions, resulting in missing values in the dataset. The missing values led to a significant loss in the number of observations used to estimate the correlates of knowledge about HIV/AIDS. Summary statistics and measurements of the outcome variables are presented in Table 1.
Summary statistics of outcome variables used in the estimations.
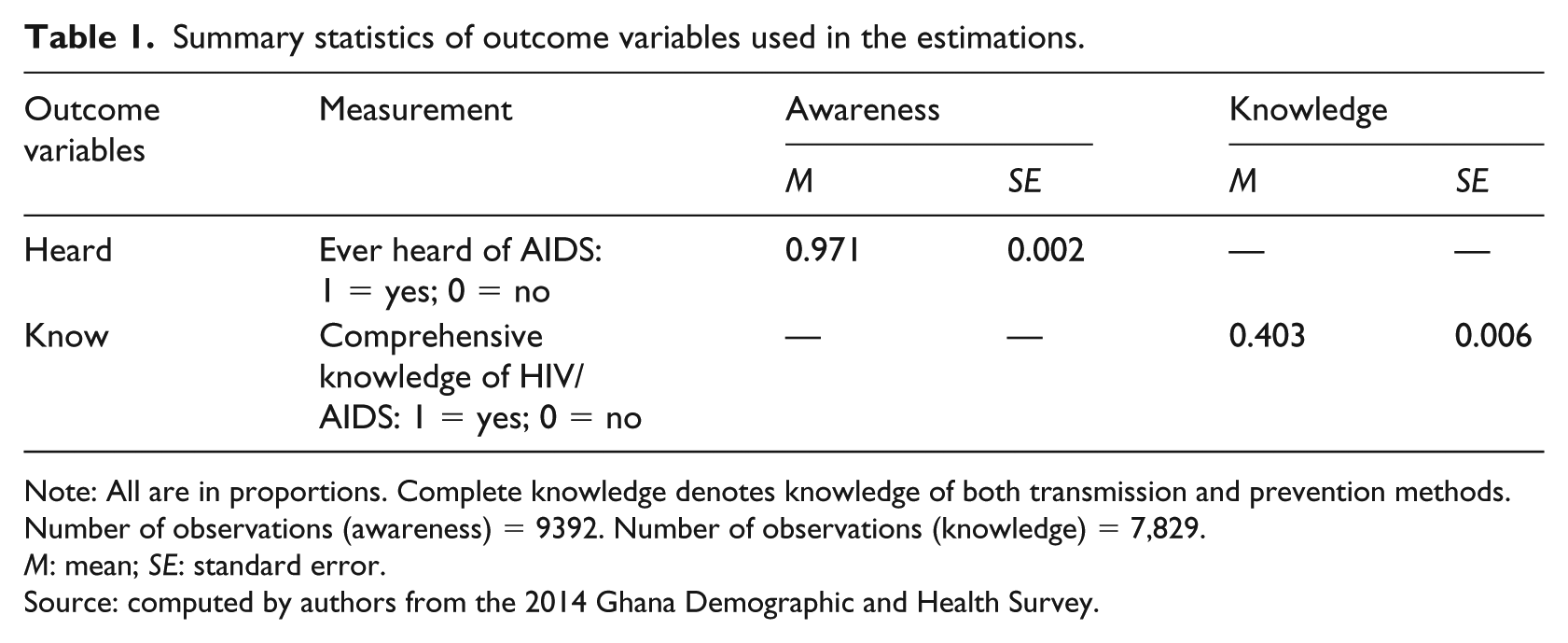
Note: All are in proportions. Complete knowledge denotes knowledge of both transmission and prevention methods. Number of observations (awareness) = 9392. Number of observations (knowledge) = 7,829.
M: mean; SE: standard error.
Source: computed by authors from the 2014 Ghana Demographic and Health Survey.
Based on Table 1, we observe that, although the majority of the sampled women, 97.1%, reported that they had ever heard of HIV/AIDS, only 40.3% of them had comprehensive knowledge of it.
Explanatory variables
The selected socio-economic and demographic variables from the 2014 GDHS include: age; pregnancy status; region and place of residence; wealth, educational and marital statuses; religious affiliation; and choice of contraception method. Table 2 presents a summary of the descriptive statistics and measurements of the explanatory variables used in the study.
Summary statistics of explanatory variables used in the estimations.
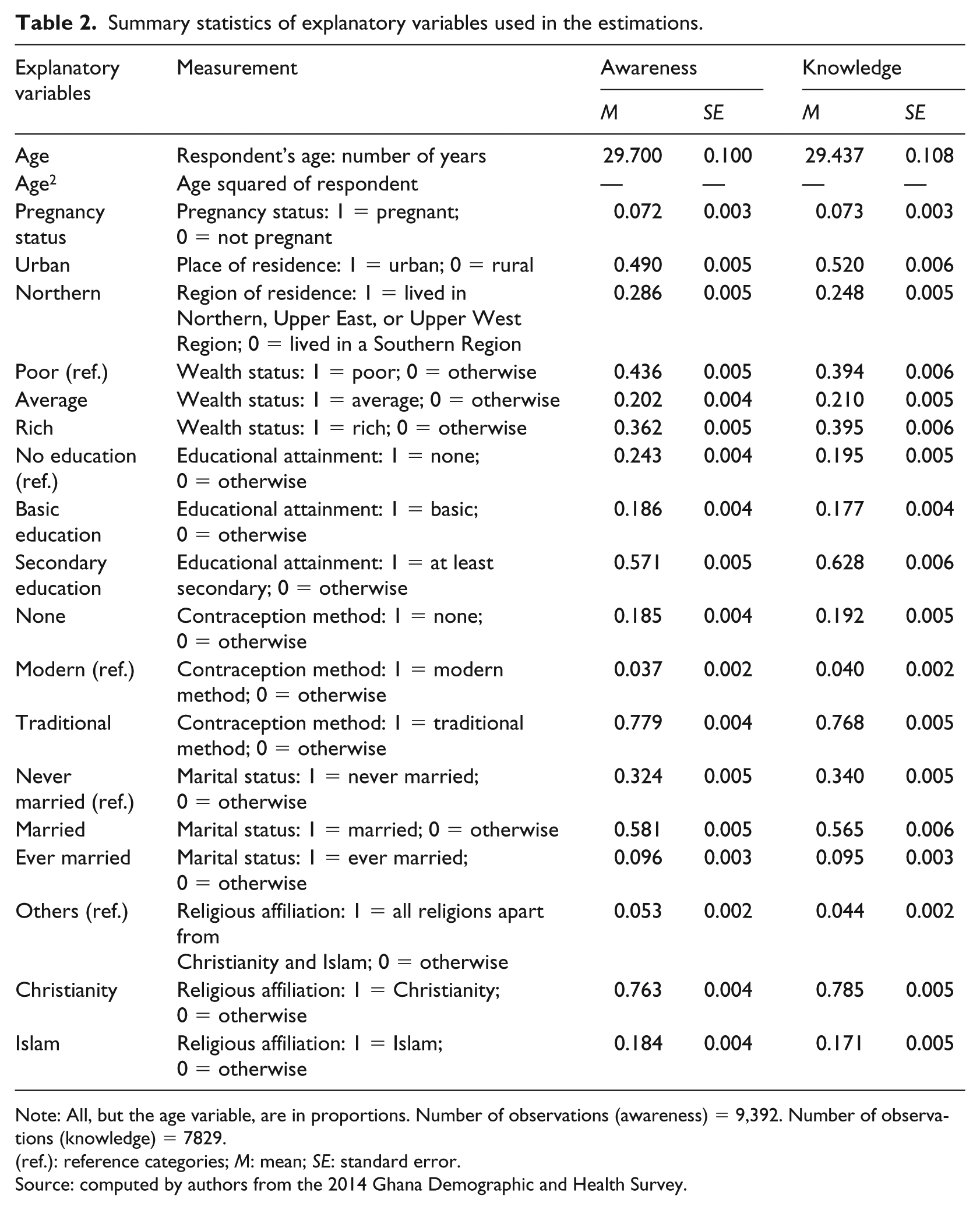
Note: All, but the age variable, are in proportions. Number of observations (awareness) = 9,392. Number of observations (knowledge) = 7829.
(ref.): reference categories; M: mean; SE: standard error.
Source: computed by authors from the 2014 Ghana Demographic and Health Survey.
From Table 2, the average age of the sampled women is roughly 30 years, with a relatively small number, 7.2%, being pregnant at the time of the survey. Further, 51% were resident in rural areas, 71.4% were resident in the southern regions of Ghana, with 43.6% being poor. Additionally, we find that 57.1% had attained at least secondary education, 76.3% were Christian, and 58.1% were married, whilst 77.9% used traditional contraception methods (77.9%).
Statistical analysis
Given that the outcome variables are binary in both cases (correlates of HIV/AIDS awareness, and correlates of knowledge about HIV/AIDS), a binary model is required for our empirical estimations. A logit regression model was therefore used to estimate the socio-economic and demographic factors that predict knowledge and awareness of HIV/AIDS. The empirical estimations were performed using STATA 13.0, taking into account the survey design. With the assumption that

where
Results
Multivariate analysis (logit model)
Logistic regression estimates for the correlates of HIV/AIDS awareness and knowledge among younger and older Ghanaian women of reproductive age are presented in Table 3. Four separate regressions are presented in Table 3; one each, using pooled data, for the correlates of HIV/AIDS and awareness, and HIV/AIDS and knowledge, and one each using data split according to the two categories of women. The statistical significance of the F-statistic of the respective models shows that the models are robust in explaining the determinants of HIV/AIDS awareness and knowledge among these distinct groups of women.
Odds ratios from logistic regression estimation of the correlates of HIV/AIDS awareness and knowledge among Ghanaian women, 2014.
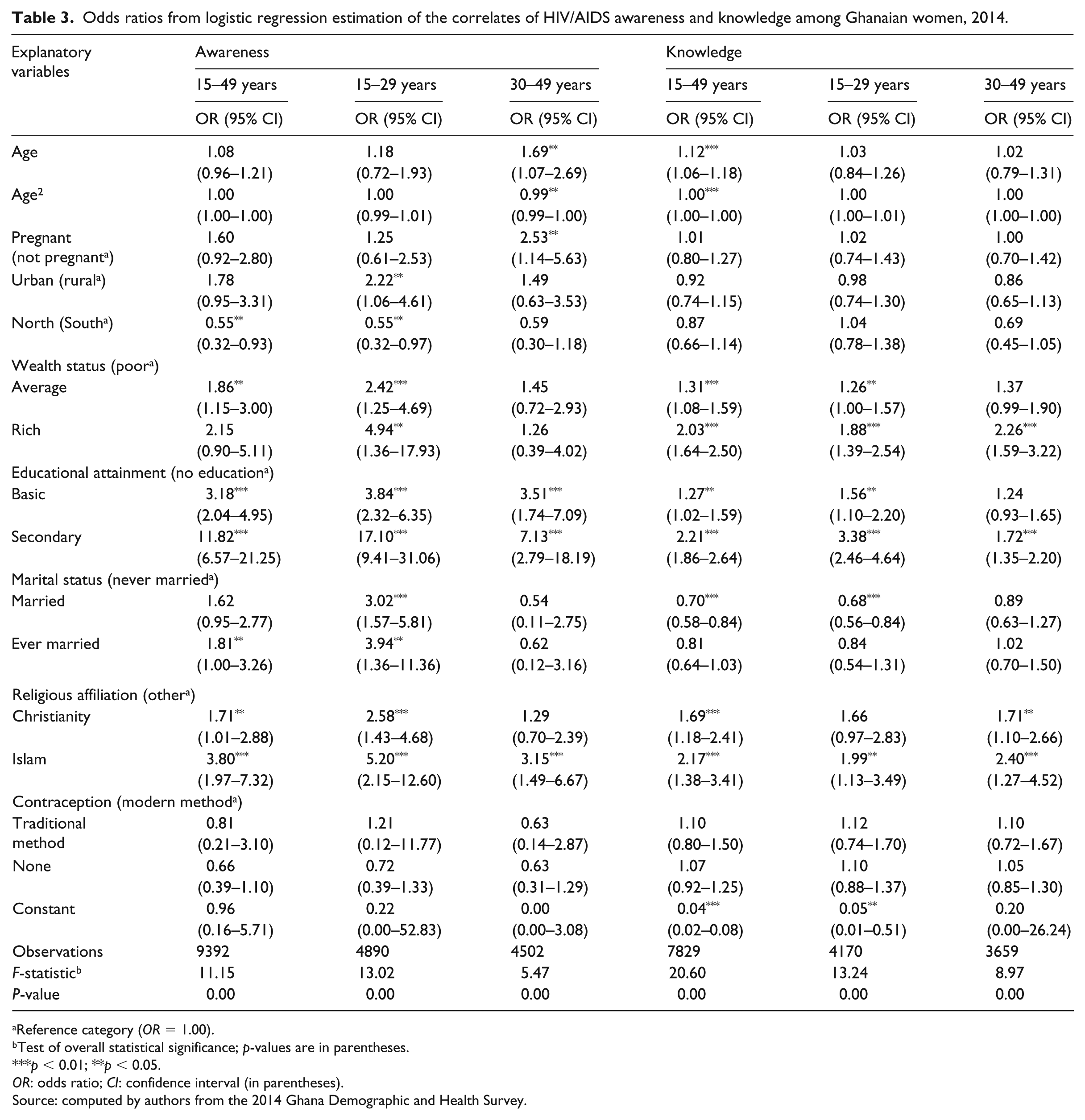
Reference category (OR = 1.00).
Test of overall statistical significance; p-values are in parentheses.
p < 0.01; **p < 0.05.
OR: odds ratio; CI: confidence interval (in parentheses).
Source: computed by authors from the 2014 Ghana Demographic and Health Survey.
With regard to the pooled data on awareness of HIV/AIDS, the results indicate the influence of location, wealth, educational attainment, marital status and religion. These factors are important predicators of awareness, which in turn influence attitudes to HIV/AIDS and ultimately behaviour towards the illness. In the case of knowledge of HIV/AIDS, we find that age, wealth status, educational attainment, marital status and religion are significant in explaining the correlates of HIV/AIDS knowledge. What emerges from these two estimation results is the dominant influence of economic and socio-cultural factors – wealth, education, marriage and religion – in affecting the knowledge and awareness of HIV/AIDS among Ghanaian women of reproductive age.
Separate estimations were performed for younger and older women to observe the probable disparities likely to exist in the correlates of HIV/AIDS awareness and knowledge among the two groups of women. The results from the logit model show that there are differences between the two groups of women, affirming the conclusions from the test of difference in means (see Table 4). Thus, different factors are revealed to affect the awareness and knowledge of HIV/AIDS among younger and older women in Ghana. For instance, age and pregnancy status of older women affect their awareness of HIV/AIDS compared to younger women. On the other hand, wealth status, marital status and being of the Christian faith are important predictors of HIV/AIDS awareness among younger women. Educational attainment and being of the Muslim faith are significant in the case of both groups of women.
Logit regression estimates (coefficients) of determinants of HIV/AIDS awareness and knowledge.
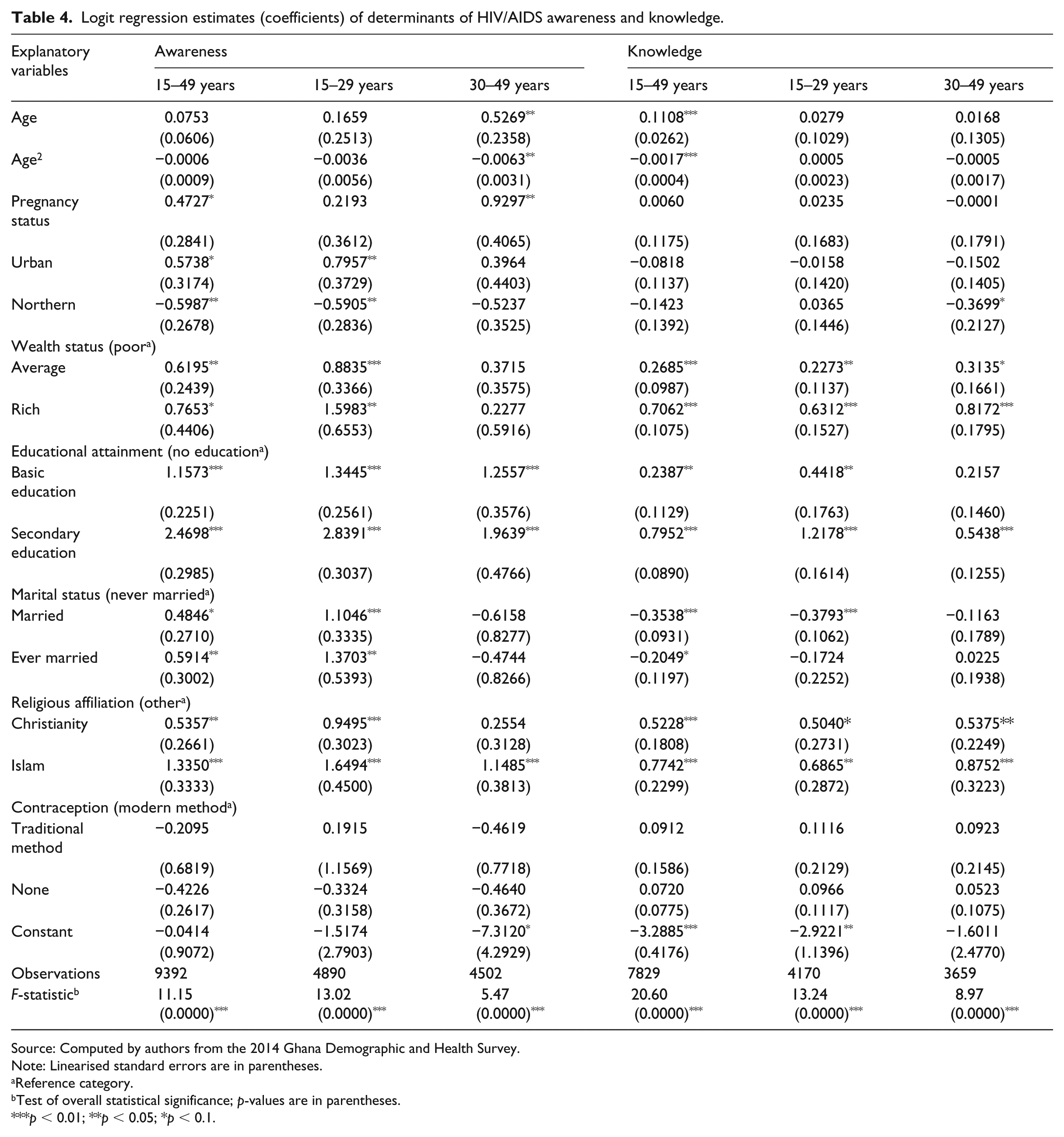
Source: Computed by authors from the 2014 Ghana Demographic and Health Survey.Note: Linearised standard errors are in parentheses.
Reference category.
Test of overall statistical significance; p-values are in parentheses.
p < 0.01; **p < 0.05; *p < 0.1.
On the correlates of HIV/AIDS knowledge, we observe that few differences exist between the two groups of women. Wealth status, religious affiliation and having attained secondary education are significant predictors of HIV/AIDS knowledge for both younger and older women. However, attaining basic education was significant in the case of younger women but not older women.
One important conclusion that emerges from the preceding discussion on HIV/AIDS awareness and knowledge of women of reproductive age is the relevance of education – secondary education – as a critical predicator factor. This is significant for both groups of women. This suggests that for women with lower levels of educational attainment, information packages must be sensitive to the literacy levels of such women. This is a very important observation, because health behaviours can only be influenced by health beliefs, and education is arguably the single most important element in changing health beliefs.
Discussion
The study finds that wealth or income is positively associated with HIV/AIDS awareness and knowledge; wealthier women are more likely to know about and be aware of HIV/AIDS. In addition, we also find education to be an important factor affecting HIV/AIDS awareness and knowledge. Our finding regarding the importance of education is consistent with existing studies, such as Fenny et al. (2017). Importantly, we note that higher education, as measured by secondary school attainment, is a very significant predictor of comprehensive knowledge of HIV /AIDS.
Similarly, compared to women with no formal education, those with formal education are found to have a higher probability of having comprehensive knowledge of HIV/AIDS as well as being aware of the epidemic. The positive and significant association between wealth and comprehensive knowledge is underscored by other studies, including Yaya et al. (2016a, 2016b), Pascoe et al. (2015) and Fenny et al. (2017). In particular, Yaya et al. (2016a, 2016b) reported a similar finding among women in Bangladesh where those with higher education (tertiary) are more likely to have a comprehensive knowledge of HIV/AIDS relative to their counterparts with no education. Indeed, Gillespie et al. (2007) have noted that richer and better educated individuals will have better access to reproductive healthcare and by extension, better information on health-related matters, such as HIV/AIDS. Evidently, wealth and higher education, which clearly suggests a higher socio-economic status, have also been found to be important in affecting the choice of safer sexual behaviour (De Walque et al., 2005; Glynn et al., 2004).
Thus, socio-economic status links knowledge and awareness of HIV/AIDS among Ghanaian women of reproductive age to the issue of affordability. It is worth mentioning that information leading to awareness and knowledge about HIV/AIDS is freely available through media advertisement and other public education campaigns, hence no direct costs are incurred. Nevertheless, to obtain further information beyond that provided through electronic media, other channels of obtaining information involve costs. These costs, mostly opportunity costs, are relatively higher for poorer women. Another dimension to the issue of affordability is that of access to education. In other words, where a woman cannot afford a formal education, she is less likely to know about and be aware of HIV/AIDS. Consequently, policy should therefore be geared towards targeting health education about HIV/AIDS for poor women to achieve improved health behaviours.
Age is another significant determinant of awareness of HIV/AIDS among the women. Older women are more likely to be aware of the HIV/AIDS epidemic than younger women. This finding contrasts with Okeke et al. (2012), who find no significant differences in knowledge of the disease among army personnel in Nigeria. We also find that older women who are pregnant are more aware than younger women. Thus, there appears to be a link between their pregnancy status and awareness. In other words, it appears being an older woman and pregnant increases the awareness of these women to the issues surrounding HIV/AIDS. This is probably because older women take the information at ante-natal clinics in Ghana more seriously, better appreciate the risks associated with the illness, and/or better understand the implications of the illness, compared to younger women. It is worth mentioning that pregnant women are provided a range of information on health and wellbeing at ante-natal clinics, among which includes HIV/AIDS. This is now the practice, for as noted by Kharsany and Karim (2016), in generalised epidemic settings, HIV prevalence is well-established in pregnant women attending antenatal clinics. Further, older women might have seen relatives or members of the community who had experienced HIV/AIDS, which has challenged them to learn more about the epidemic. Thus, experiential knowledge of HIV/AIDS at the household level or work-place could potentially explain the greater likelihood of awareness among older women.
Another striking finding is that younger women who are married are more likely to be aware of, and have comprehensive knowledge of, HIV/AIDS compared to older women. Indeed, awareness of the illness extends to younger women who have previously been married; in fact, they have a higher probability of being aware of HIV/AIDS than older women who had previously been married. This seems to suggest that marriage among younger women is a strong predictor of awareness and knowledge. This may be due to increased risk of infection from their partners, which, as noted by Glick and Sahn (2007), is because of the low share of adults in Africa who have been tested for HIV. This probably indicates that young women (and more broadly couples) who get married now have increased awareness of the disease. Indeed, in the last decade and a half, many churches in Ghana have encouraged pre-testing of HIV as part of the counselling provided to young couples intending to marry. Addo (2005), for instance, in a study on pregnant women in Kumasi, finds that the majority of women who had done an HIV test did so as a pre-requisite for church blessing of their marriage.
We can also infer that younger women would have grown up in the period when increased awareness of the epidemic was high, but as they have matured into marriage life, they realise the increased risk of infection from partners who may not know their status, and/or may be unfaithful. Consequently, as argued by Glick and Sahn (2007), couples in such a situation will take precautions to avoid infection. We then argue that by taking precautions to avoid infection, awareness among young married women is heightened, as evidenced by our finding.
Younger women in urban areas have a higher significant probability of being aware of HIV/AIDS than their counterparts who are resident in rural areas. Whilst it is not surprising that information about the illness is more accessible in urban areas than rural areas, it raises important policy issues, particularly with HIV/AIDS campaigns intended to bring about behavioural changes. This calls for better targeting of health campaigns, such as those aimed at particular groups of women at risk, whilst at the same time ensuring that these health messages reach them in the home and at their work places.
Finally, we find that being a Christian or Muslim woman significantly influences awareness and comprehensive knowledge of HIV/AIDS. This is not a surprising outcome, because the churches and mosques were included in the awareness and health dissemination campaigns in the 1990s and early 2000s. As observed by the Open Society Institute (2010), whilst voluntary HIV testing has been the policy in many African countries, churches have adopted mandatory premarital testing. However, it is only in Ghana that the government successfully worked with local churches to make premarital testing voluntary.
Conclusion
This paper sought to investigate the determinants of HIV/AIDS awareness and knowledge among women of reproductive age in Ghana.
Findings from the study indicate that older Ghanaian women are significantly different from their younger counterparts in terms of socio-economic and demographic variables that influence their awareness and knowledge of the epidemic. The paper reveals that younger women’s wealth status and marital status significantly affects their awareness of HIV/AIDS, whilst age and pregnancy influenced that for older women. In the case of comprehensive knowledge, married younger women had better knowledge compared to married older women. For the pooled sample, we find that location, wealth status, educational attainment, marital status and religious affiliation are important predictors of HIV/AIDS awareness. On the other hand, a woman’s age, wealth status, educational attainment, marital status and religious affiliation were found to significantly affect the comprehensive knowledge of HIV/AIDS. In addition, pregnancy status and place of residence were found to be significant correlates of HIV/AIDS awareness among the women.
This paper highlights the importance of higher social status in mediating awareness and knowledge of the disease. Whilst every woman cannot possibly be ‘rich’, what this implies is the need for policies and interventions to provide targeted messages that take into account the varied socio-economic and demographic backgrounds of women in Ghana. Further, health education interventions should be sensitive to the changing technological landscape in order to develop messages that can be delivered via mobile phones, whether as reminders or ring tones, and therefore enhance health knowledge and promote behaviour that brings about desirable health outcomes. Apart from contributing to the existing studies on the subject, the findings will inform policymaking and thus contribute to eradicating the epidemic. The foundation of public health educational interventions is the connection between health beliefs and health behaviours. Thus, the importance of well-formulated health education campaigns cannot be over-emphasised.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.