
Abstract
This qualitative, phenomenological study explored four incarcerated adult females’ experiences that contributed to their human immunodeficiency viruses (HIV) status and acts of murder. The participants were purposely selected based on their HIV status and their crime, murder. Data were collected through one-on-one interviews and available secondary reports on the topic. The goal of this research was to answer two questions: (1) What contributed to the female participants’ HIV-positive status? and (2) How did the females’ HIV-positive status shape their crime of murder? A thematic analysis was used to analyse and identify the factors linked to the participants’ HIV status and their crime. The findings suggest irregular testing of HIV/acquired immunodeficiency syndrome (AIDS), promiscuous behaviour, partner infidelity and ignorance of partners’ HIV status as contributory factors to the females’ HIV-positive status. Specific childhood-related and adulthood-related factors explain the murder of the participants’ partners/spouses.
Keywords
Introduction
Human immunodeficiency viruses/acquired immunodeficiency syndrome (HIV/AIDS) is of global importance and is particularly of significance in Sub-Saharan Africa that experiences a copious amount of HIV/AIDS numbers (Ochillo et al., 2017). One offending population affected, but often forgotten, is females incarcerated for murder, who are HIV positive. The incarcerated females’ experiences, the victimisation they endured and their pathways to HIV/AIDS and murder are not always well understood (Anumba et al., 2012; Webster, 2021; Wise, 2017).
A South African research, conducted by Valabdass et al. (2021) on perpetrators of intimate partner homicides (IPHs), cites a history of violent behaviour, murders occurring in private homes, knives and firearms used as weapons, infidelity, jealousy, separation, personality and psychotic disorders and substance abuse as prominent factors in IPH. Valabdass et al. (2021) found that being a female perpetrator of IPH, displaying limited education, unemployment prior to the offence, a history of medical and psychiatric illness and no history of violence, rendered the incarcerated females not fit to stand trial and to be not criminally responsible. In addition, Peltzer (2013) examined the prevalence of intimate partner violence (IPV) in new HIV-positive mothers. He found that many of the females obtained an education of Grade 11 and lower, suffered from depression and sexually transmitted infections, while almost half of the participants indicated that their partners/spouses are also HIV positive (Peltzer, 2013). The females indicated emotional, physical and sexual abuse by their partners and in them (the females) having two or more sexual partners.
Females are generally associated with nurturing, caring and loving traits (Ishoy and Blackwell, 2018). When females commit murder, this rarity is often frowned upon, and people question the perpetrators’ femininity, rationality and sanity, warranting media attention (Ishoy and Blackwell, 2018; Pelvin, 2019). The reasons for questioning females’ ability to commit murder are grounded in the facts that females have a higher sense of morality (the ability to distinguish between right and wrong and good and bad behaviour) and they normally exhibit higher levels of self-control than their male counterparts (Ishoy and Blackwell, 2018). Furthermore, females commit fewer violent offences and they are less violently inclined than males (Ishoy and Blackwell, 2018; Pelvin, 2019).
According to Webster (2021), many women murder men who abused them. This author mentions that in England, 71 females out of a sample of 92 incarcerated females were abused at the hands of their deceased victims. Many females that are imprisoned display histories of childhood abuse (i.e. physical, sexual, emotional abuse and neglect), and often this abuse by intimate partners and/or spouses continues into adulthood (i.e. intimate partner abuse and financial dependence abuse) (Eriksson et al., 2018; Hedderman et al., 2011). Female inmates who are HIV positive display backgrounds that are characterised by financial difficulties, inadequate familial and institutional support and inequality (i.e. employment and opportunities) (Eriksson et al., 2018). Also, incarcerated females’ cognitive functioning (i.e. low self-esteem and poor coping skills) and mental health challenges (that stem from trauma) can be ascribed to their intimate personal relationships with men (Peltzer, 2013).
Regarding the theoretical application, the Situational Action Theory (SAT) developed by Wikström (2004) encompasses an array of theories to explain female offenders’ experiences of their HIV-positive status and their involvement in murder. First, the SAT immersed criminological theories such as the following (Ishoy and Blackwell, 2018):
Rational Choice Theory (Cornish and Clarke, 1986) is based on the idea that all the female offenders are rational beings that selected to commit murder.
General Theory of Crime (Gottfredson and Hirschi, 1990) surmises that due to a lack of self-control, the female offenders committed murder.
Routine Activity Theory (Cohen and Felson, 1979) stipulates that due to the abuse and after being infected with HIV/AIDS, the females were motivated to murder their ‘targets’, that is, their partners/spouses who abused them and infected them with HIV/AIDS, in the absence of ‘guardians’ (i.e. family members and support to mediate the tension and address coping mechanisms with their HIV status).
Lifestyle Theory (Hindelang, Gottfreson and Garofalo, 1978) proposes that due to a promiscuous lifestyle, ignorance to one’s partner’s HIV status, irregular HIV/AIDS testing and infidelity (and multiple sexual partners), some of the female offenders’ lifestyles rendered them prone to being infected with HIV/AIDS.
The SAT identifies that not all females (i.e. female offenders that committed murder) will weigh the costs (i.e. the loss of the breadwinner, father of children, husband, punishment and subsequent imprisonment) and benefits (i.e. revenge, a sense of power and control, empowerment and diminishing of abuse) when deciding to commit murder (Ishoy and Blackwell, 2018). The core principles of the SAT include the interaction effects between a person’s self-control and morality (to distinguish between right and wrong and good and bad behaviour) (Ishoy and Blackwell, 2018).
Furthermore, situational (for instance, divorce of parents influences children’s behaviour), environmental (noise, interior spaces and access to nature) and social disorder factors (rejection, bullying behaviour and humiliation may cause social anxiety) played integral roles in the females’ lives that committed murder. Situational or external factors that contributed to both the females’ HIV-positive status and their engagement in murder include dysfunctional family lives, exposure to childhood (by family members and own) and adulthood (IPV) violence, childhood abuse, absent and abusive parents, abandonment, rejection, poor intimate bonds, limited education, financial stress, isolation and an inadequate support structure. Vis-à-vis environmental factors (social isolation and a lack of support), some of the females resided in areas where neighbours did not get involved in domestic disputes and violence in areas became conducive to disorder. In turn, social disorder resulted in the female offenders accepting IPV as a ‘normal’ and as a private matter, and in their partners abusing substances (Ishoy and Blackwell, 2018).
A qualitative, phenomenological case study analysis was followed to analyse adult females’ lived experiences that may have contributed to their HIV status and their distinct pathways to murder. The aim of the research was to explore female offenders’ experiences, their narratives and paths to HIV/AIDS and murder. The research was directed by two questions: (1) What contributed to the female offenders’ HIV-positive status? and (2) How did the female offenders’ HIV-positive status shaped their involvement in murder?
Methodology
The sample for this study included four adult incarcerated females. Two participants were purposively selected for their HIV status and their crime of murder. These females represent the ‘interviewed participants’. One-on-one semi-structured interviews were conducted with these females, and a semi-structured interview schedule guided the researcher during the interviews. Five interviews were conducted with the participants incarcerated at a Female Correctional Centre in Gauteng province (South Africa), and each interview lasted approximately 90 minutes. The interviewees voluntarily participated in the research, orally consented to their participation (at the time of research, either oral or written consent was required by the institutions) and the researcher treated them with the utmost respect and dignity according to protocols used by Mason (2010). The other two participants were selected from the secondary data documents in the form of criminological pre-sentence evaluation reports that is in the public domain. These females were also included in the research based on their crime (murder) and their HIV status. To identify pertinent themes associated with the females’ HIV-positive status and their involvement in murder, Braun and Clarke’s (2006) six stages of thematic analysis were applied in terms of: (1) familiarising oneself with the data, (2) generating initial codes, (3) searching for themes, (4) reviewing the themes, (5) defining and naming the themes and (6) producing the report (Nowell et al., 2017). The identity of the females cannot be traced in any way as anonymity was ensured (Mason, 2010). Ethical approval was obtained for the interviewed participants and for the secondary document analysis.
The narratives consisting of the four female offenders’ lived experiences, realities and struggles related to their HIV status and their involvement in murder are outlined. Case studies A and C (interview data) comprise one-on-one interviews conducted with the females housed at a Female Correctional Centre in Gauteng province (South Africa), while case studies B and D (document analysis) are representative of dated criminological pre-sentence evaluation reports. The verbatim quotations of the ‘document analysis participants’ were extracted from both the pre-sentence evaluation reports and from questionnaires that participants completed while in prison and busy with appeal of their sentences. These questionnaires were in their files. The interviewees’ own narratives are derived from the interviews. The verbatim quotations are used to illustrate the females’ own reality, feelings and lived experiences.
Discussion
Case study A (interview data)
Biographic and personal background
Ms. A is a 26-year-old African Xhosa-speaking single lady [never married] with two children from different fathers. Ms. A’s children are residing with their paternal grandparents. Ms. A completed Grade 7 schooling. Her mother is a domestic worker and she [mother] was not married to Ms A’s biological father. Ms. A never met her father, and her mother remarried 2 years after her father left them. Her stepfather is a construction worker and has always enjoyed stable employment, and according to Ms. A, gets a good salary. Ms. A is one of four siblings – her three step-siblings are from her mother and stepfather’s marriage.
Childhood circumstances
Ms. A mentioned that her mother and stepfather argued a lot, “they drank beer, smoked marijuana and they fight, yoh . . . hitting each other. I always tried to hide the littles ones” [her step-siblings]. She furthermore revealed that her stepfather used to hit her with his belt [as punishment] on a regular basis, and that her mother did not really love her because (w)e fought a lot. Once when I was 14, she [mother] chased me away from home, it was at night, I was walking alone in the street, I had nowhere to go . . . and these three boys saw me walking around, I was so scared, they said I can join them, stay with them and they will help me and look after me. So, we smoked white pipe [known as ‘slow boat’ – a mixture Marijuana mixed with Mandrax] and they raped me. I saw it [the rape] happening to myself, from outside my body and I could not do anything. It felt like I was dead, but I was alive. I never told anyone until later when I was maybe 18 years or so. I only told one friend that I trust . . . she visits me in prison and . . . I told my last boyfriend that I killed.
Regarding childhood familial abuse, Ms. A disclosed that Yah you know, my mother did not care about me, she left my stepfather to hit me when I did not do the housework or cooking the way they liked it . . . she would not even protect me from him. I could not sit on a chair for 2–3 days after that. She did not even give me a cup of tea for me, nothing. I ended hating them both so much. My stepfather, twice . . . he threw the food that I cooked into the dustbin and took me to the bathroom to hit me for it.
Ms. A divulged that due to her appalling home circumstances, approximately at the age of 14 years, she stole some of her parents’ marijuana and alcohol ‘to cope with everything’. During this time, she also ran away from home, dropped out of school and lived with older men who provided for me . . . food, clothes, beer and drugs. I just wanted to party and forget everything. I felt bad about leaving the children [her siblings], but they did not have it as bad as I did.
When asked how many intimate relationships she enjoyed prior to her current incarceration, Ms. A reported, ‘Oh, many, maybe nine or so I think. She further declared that all of her partners physically abused her, but, at least they all looked after me, they gave me money, food and everything. I did not have to work’. When asked how she coped with the abuse, Ms. A retorted that I used drugs . . . and drinking beer every day to feel better . . . I was looking for love with them [her partners], only now do I realise I looked at the wrong places and with the wrong people.
Ms. A’s children were given to their paternal grandparents after they were born, and Ms. A never looked after her own children. According to her, she ‘visited them mostly over weekends . . . Saturdays and Sundays’.
Crime analysis
Ms. A is a second offender. Her criminal record indicates that she was arrested and convicted for theft (×2) and assault (×1) with the intent to do grievous bodily harm (GBH) – crimes for which she received an 18-month imprisonment sentence. For her current sentence, Ms. A is serving a 7-year sentence for murder, and she unveiled the circumstances as follows: It was my last boyfriend, so, . . . he raped me . . . told me I am a whore . . . and that is why I was raped by those boys [when she was 14-years old] . . . and that I’m a cheap and filthy whore. He hit me so hard that I fell on the floor . . . kicked me in my face and everything. The blood was coming from my face. I just stayed on the floor until he stopped. He left for the couch . . . I got up, took a knife and I stabbed and stabbed him. I think I exploded. I didn’t know how many times I stabbed him. The police told me I stabbed him nine [9] times in his chest, stomach and close to his heart.
HIV/AIDS status
Ms. A was very open about her HIV/AIDS status and in testing positive. She states that she voluntarily underwent a pregnancy test after she entered the correctional institution for her current sentence. When she was called in, thinking the feedback was on her pregnancy test, she found out that she is HIV positive. Ms. A posited that she experienced severe and ‘confusing feelings’ of shock, disbelief, anxiety, anger, shame and guilt and felt depressed. In this sense, Ms. A affirmed that I really thought it was a mistake, that it is another female’s result. I questioned it, my stomach turned the whole time . . . my brain . . . I could not eat, think or sleep. I just cried and cried. I worried about my children and my future. I stayed with myself for weeks.
When asked how she might have contracted HIV/AIDS, Ms. A reflected that I don’t know, I lived with many guys. I am ashamed of it now, but then [prior to her current imprisonment] I did not care, I never thought of HIV/AIDS. I heard other people talk about it, but I never bothered. I really do not know. Here I am now. I tried to think of all of them, and I identified two of the guys that I think could have given it to me, but I am not sure.
When probed on why she thinks these two men might have infected her, she replied that ‘Because I found out that they were seeing other women, it was not just me they were with. That’s why I left them’. Ms. A stressed that her mother traced and contacted her ex-partners to disclose Ms. A’s HIV/AIDS status to them for them to get tested, for ‘I have to be responsible, I am not the only one infected here’. The offender has received no feedback from her ex-partners. She stated that her mother paid for her children’s HIV tests and that they are negative.
Ms. A stated that she receives antiretroviral HIV medicine and she portrayed that the correctional nurses ‘are very good and supportive’. As with other HIV-positive offenders, Ms. A is on a special diet. She noted that at the beginning (and some symptoms are ongoing), the medicine gave her a skin rash, made her nauseous and she struggled to sleep, and at times, she has no appetite. She unveiled that she has lost weight, but that she is trying to stay healthy. Ms. A declared that the correctional psychiatrist is monitoring her for anxiety, depression and sleeping problems for which she is receiving medication.
Concerning Ms. A’s current support structure, three people regularly visit her at the correctional centre. They include her one friend to whom she disclosed that she was gang raped when she was 14 years old, and her one step-sister visits ‘when there is money and extras for travelling’. Since Ms. A’s current imprisonment term, she has reconnected with her mother, who in a period of 5 years (of being in prison) came to visit her approximately 15–20 times. Her mother also sends her money with her friend and step-sister when they come to visit Ms. A. On their reconnection, Ms. A expressed that I never thought I would see or speak to my mother again. We cried when we saw one another the first time. She said she is sorry for me and for not looking out for me. My heart is happy now. It is never too late to love your mother, even me for my own children when I come out of prison.
When asked about contact with her children, Ms. A pointed out that she speaks to her children on the telephone. Her mother consulted with the children’s grandparents and gave them money to use the phone for data so that she could speak to her children. Finally, when asked how she copes with her HIV-positive status, Ms. A stated that I was scared of what others would think of me, ashamed of my past, but now I just pray and pray. I found God and He helps me. This is not the end, with my medicine I can have a long life.
Case study B (document analysis)
Biographic and personal background
Ms. B is a 38-year-old African Swati female. She is a divorced mother of two children (who grew up and still resides with her mother). Ms. B completed Grade 12 and obtained several diplomas in Project Management and Public Relations. Due to an emotional and physical abusive marriage, Ms. B moved to another province and found a well-paid job at a prominent events managing company. She professed that I went overseas to America, England, Germany, Hong Kong and even to China for courses, conferences and events. I also lived in New York for 6 months –we had a big job there and I was the assistant manager of the project.
Ms. B has a younger brother who owns his own construction company.
Childhood circumstances
Ms. B grew up with her mother and grandmother. Her mother is a fabric worker, and her father, a retail shop manager. She did not see her father much as ‘he only came home about once every 2 months or so’. She reported no adverse childhood circumstances and mentioned that her mother and grandmother are very religious and that they (mother, grandmother and Ms. B) went to church every Sunday while she was staying with them.
Crime analysis
Ms. B is a first-time offender and she received a 12-year sentence for murder. She retorted that I met my partner of 3 years at one of our events. He was well known and well-off. I never really liked his type . . . a ‘know-it-all’ and ‘have-it-all’ type. He was too good to be true. He wore nice clothes, fancy shoes, took me out to nice restaurants, bought me beautiful clothes, he just spoiled me so much. He always spoke so nice and softly to me . . . it felt as if I was on a pedestal, and he never lifted a hand to me. I worked very long hours and I saw him about once or twice during the week and over weekends . . . when I did not travel.
Ms. B related that her last trip for work was to Brussels and is preliminary to the murder: He [her partner] was very excited when he heard I was going to Brussels, he was going on and on about it . . . telling me what a nice country it is. He helped me pack my suitcase the afternoon before my flight, something he never did before. I thought he loves me so much and that maybe we will get engaged when I get back from the trip. I was supposed to stay 10 days in Brussels, but my job finished earlier, and I came home a few days earlier . . . not informing, I wanted to surprise him. I even bought him two very expensive shirts and cologne. So, when I got back, I found him with this girl in my place and I just lost it, I grabbed my gun and shot him.
Ms. B stated that she only found out after her arrest that her partner had been seeing the woman for over a year and that they have a baby girl together.
HIV/AIDS status
While out on bail, Ms. B became very ill, she fainted several times and she was constantly nauseous. The doctor thought she might be pregnant; however, the blood test results showed that she is not pregnant, but HIV positive. Once sentenced, Ms. B enjoyed the support and counselling from the correctional nurse and psychologist. Ms. B takes her antiretroviral medication and is on a special diet. She orated that she experienced severe side-effects, such as ‘being tired all the time, I still struggle to sleep, I’m down . . . my skin itches a lot and I vomited a lot in the beginning’. Ms. B revealed that when she found out about her HIV status, I was thinking about ending my life, drinking poison . . . I tested negative when I took out life insurance 2 years into our relationship, my result was negative. I am so ashamed, I thought a lot of what all my friends would think of me.
Due to her suicidal ideation, Ms. B is monitored on a regular basis and she has revealed her status to her mother who ‘was very shocked, but she, my father and my grandmother support me a lot’. Ms. B reported that I am still depressed and angry, because I messed up my life, it was going so well, I had a good job, then my arrest, now the AIDS. I feel I am punished for being a fool to have fallen for him and his lies. I did not think it through, I am really sorry I shot him, I snapped. I took his life and I had no right to do so . . . if I could turn back time, I would have just walked out and pick-up the pieces again. It is all like a bad dream.
When asked how she thinks she contracted HIV/AIDS, Ms. B announced, ‘It was him, I am not his first victim, she (the other girlfriend) also tested positive, someone I worked with told me’. The participant further exclaimed that ‘I am not the only one that is HIV positive that he slept with – does it make sense to you? That is how I was infected and who knows how many other girls before me?’
Vis-à-vis Ms. B’s support structure, her brother, mother, grandmother, father and three of her ex-colleagues/friends support her.
Case study C (interview data)
Biographic and personal background
Ms. C is a 32-year-old Xhosa-speaking inmate who completed Grade 10. Prior to her imprisonment, she did piece jobs (domestic work) for two households to assist her mother with money. Ms. C’s parents were divorced when she was 3 years old. The participant is the mother of two children. Her mother is a street vendor who sells fruit and vegetables, while her grandmother looks after the children. The participant reported that her mother financially supports her two unemployed older brothers and her grandmother. Since her incarceration, her mother is also supporting her two children. Ms. C has no contact with her father, and she does not know anything about him.
Childhood circumstances
At the age of 6 years, Ms. C was raped by her uncle (her mother’s brother). She recalled, he raped me in his car, I came into the house, bleeding and crying, but my mother and grandmother did nothing. They said nothing. My uncle helped my mother every month with money for the house, for food and for other stuff at home . . . maybe that is why they did nothing about it.
The participant claimed that there was always enough food and clothes at home, but the problem was my mother, she was never there for us, she worked all the time. My brothers were just drinking and taking drugs and fighting a lot . . . they used my mother’s money to buy alcohol, and if she did not want to give them money, they would swear at her.
Ms. C lived with the father of her children for four and half years, but after ‘every day of him swearing and shouting at me, hitting me and forcing me to have sex with him, I left him and went back to my mother’s house’. Despite her childhood sexual abuse and neglect, Ms. C managed to abstain from alcohol, drugs and truancy.
Crime analysis
Ms. C is a first-time offender incarcerated for murder, and she is serving a 15-year sentence. She asserted that she would meet up with her ex [father of her children] at the end of each month to get money for the children. During this encounter, she would have to sleep with him: after we had sex, he would accuse me of sleeping with other men, and beat me . . . every time I would leave there with blood, feeling like a whore . . . a worm . . . crawling back to him every month for money for the children.
The murder occurred after Ms. C found out about her HIV status and confronted the father of her children. She says that I knew it was my ex . . . he was the only man I ever slept with, and I knew he was seeing other girls, but I had to get the money every month. I was so furious . . . I went to see him about my HIV status and he said I was the slut, we had a fight, he hit me again . . . I grabbed a knife that was on the counter and I stabbed him 14 times. I did not ask for this, it just happened . . . he gave it to me, I wanted to hurt him – for all the beatings and abuse he gave me . . . and for giving me a death sentence.
HIV/AIDS status
Ms C. fell ill and had to go to the local hospital where she underwent blood tests to establish the type of bacterial infection the doctors thought she had. Once the blood tests returned, it confirmed that Ms. C is HIV positive. As outlined above, Ms. C is certain that her ex-partner (the deceased) gave her AIDS. Once imprisoned, Ms. C reported her HIV status to the medical staff at prison. She confirmed that she receives support from the psychologist, the social worker and from a HIV/AIDS support group in prison. Ms. C refused the special diet and for the last 2 months, she has not taken her medicine because ‘even that food is not nice, and the medicine – I do not know if it really helps me, I feel better without taking it, I sleep better’.
Regarding Ms. C’s support structure, she stated that her mother and grandmother take turns to come and visit her and her children accompany them to prison. While incarcerated, Ms. C got involved in a same-sex relationship in prison and posited that: ‘I thought I knew what love was with my ex . . . it was all a fake, but now for the first time I really feel loved, accepted, appreciated and I have wonderful support’.
Case study D (document analysis)
Biographic and personal background
Ms. D is a representative of the Zulu ethnic group, is 31 years old and is an only child. She is the mother of two boys, of which the youngest is deceased. The participant is divorced, she obtained a Grade 12 Certificate and successfully completed training for a career in the military. Ms. D’s parents are divorced, and she was raised by her maternal grandmother and a great-uncle (the grandmother’s brother). The participant’s mother was working in a factory away from home, and she saw her mother only periodically (approximately five times a year). Regarding her father, she reported that she ‘maybe saw him once or twice a year when I was growing up. I know him, I know he is alive, but I do not know much about him’.
Childhood circumstances
Ms. D described her upbringing as ‘I was like a child in my grandmother’s house, she was my mother and my uncle was my father. I grew up in the village’. According to the participant, she experienced no childhood trauma or abuse and she mentioned that ‘I did not really miss my mother because my grandmother was my mother until Grade 12, when she passed away, I had to go to my mother’. Ms. D’s mother remarried, and she got on well with her stepfather. During her school years, Ms. D struggled at school, in this regard she noted, I had challenges at school, I struggled to concentrate and focus, I thought I was stupid and I was scared that the other kids would laugh at me . . . I once failed mid-year in Grade 4, but I passed it the end of the year. I think I am a slow learner – before I grasp something . . . it takes me a long time.
There is no history of parental criminality or substance abuse and the offender explained that she grew up in a very strict religious family.
Crime analysis
Ms. D is a first-time offender and she is incarcerated for murder and attempted murder for which she received a 15-year imprisonment sentence. She was married to ‘a school friend from the village and he is also in the military’. She described her marriage as in the beginning we were fine, he loved me, and he was involved with me . . . he came home, we cooked together, went to church on Sundays and many weekends we went to visit his family. Then just before my second-born came, he started drinking with his friends, fighting with me . . . hitting me, swearing . . . telling me that I am a bad wife and mother. I struggled with money as I was on maternity leave and he would not help with the boys’ expenses, so I cried every night.
During this period, Ms. D also found out about numerous affairs that her husband enjoyed ‘with younger girls, one of them my friend’s daughter’. After another episode of abuse, the participant decided to end her and their two boys’ lives – who at the time of the murder and attempted murder, were aged 4 years and 7 months old. Regarding the crimes, Ms. D narrated that ‘I made a mixture of powder from my (prescribed) antidepressants, sleeping pills and pain pills and I mixed it with the baby and the other one’s milk’. Both Ms. D and her 4-year-old son survived this ordeal, while the baby succumbed to the overdose of pill-mixture.
HIV/AIDS status
Once in prison, Ms. D volunteered for a HIV/AIDS test, and she tested positive. Upon receiving the news, she revealed that I was so shocked . . . very depressed, I wanted to end my life again, I just could not believe it. We regularly tested in the military for HIV and I was negative, also just after the birth of the little one I was HIV negative . . . my husband told me then that he was also negative, he lied. I became so sick of worries when I heard the news . . . I sent a message to him through a friend about me having AIDS and he [ex-husband] replied that he is not responsible for it, he is negative, and he said I must never contact him again. Where else would I have got it? My son [the one that survived the overdose and attempted murder] is negative, my mom had him tested.
Regarding the murder of her baby, Ms. D expressed feelings of severe sadness and heartache and asserted that ‘I miss my baby so much, there is not a day that I do not think about him . . . I should have died that day, not him’. Ms. D further paraphrased that she needs to live for her (other) son, who according to her, still needs her.
In consideration of the murder of her baby and attempted murder of her son, Midson (2019) states that adults who murder their children are also vulnerable by circumstance or by state of mind. Said persons might suffer from mental distress and often display a history of psychological problems, abuse, substance abuse, abuse of over-the-counter painkillers and being controlled by meaningful others. These factors have an impact on the adult’s ability to think rationally (Midson, 2019). In this regard, Ms. D’s vulnerability was the result of internal factors (stress, depression, feelings of abandonment and rejection and suicidal ideation) and external factors (financial stress and the infidelity of her husband). These factors impeded on her ability to think rationally. Midson (2019) argues that it is assumed that the victims are the vulnerable ones and the offender not, and this is not always the case.
Concerning her HIV status, Ms. D posited that the correctional clinic sister talked to her about AIDS and what to expect from the antiretroviral medicine, ‘but, sometimes I still wonder . . . maybe hope they mixed up the results’. Furthermore, Ms. D keeps to herself in prison, and she has no close friend. She stated that she does not share her feelings or HIV status with anyone and postulated that she ‘is not ready to attend the HIV programme’.
About her support structure, Ms. D’s husband abandoned her, he filed for a divorce during her trial and she has lost contact with him since her imprisonment. Their son resides with her mother, and apparently her ex-husband has never contacted the child again. The participant’s mother, stepfather and son regularly visit her at prison.
Results
Since the 1980s, there has been accumulating interest in female offenders’ pathways in crime and imprisonment (Richter et al., 2010). By utilising pathways, acknowledgement is given to the participants’ lived experiences, their ‘own voice’ and perspectives related to their life histories and entry into criminality (Richter et al., 2010). For example, Hedderman et al. (2011) itemises a female offender’s lived experiences, commencing with adverse childhood experiences and escalating with a history of substance abuse, unemployment, limited education, lack of skills and post-traumatic stress disorder (PTSD). This intensified to mental health problems, diagnoses of personality disorder, split borderline personality, stress disorder, anxiety, depression and self-harm behaviour.
Table 1 outlines the participants of this study’s biographic details.
Biographic details of HIV-positive females that committed murder.
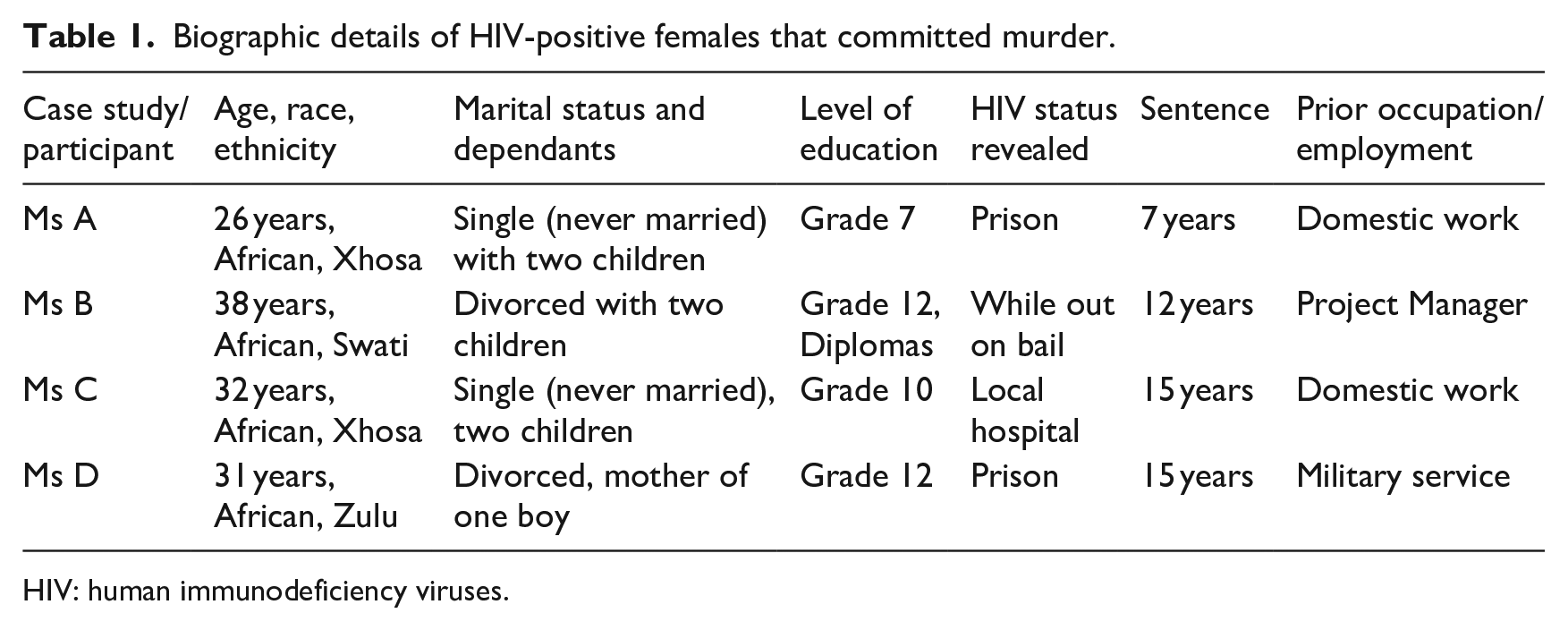
HIV: human immunodeficiency viruses.
As depicted in Table 1, all four participants are African and representative of the Xhosa (case studies A and C), Swati (case study B) and Zulu (case study D) ethnic groups. The youngest participant (Ms. A) was 26 years, and the oldest participant (Ms. B) was 38 years old. Two of the participants (Ms. A and Ms. C) were single and two of the participants (Mses. B and D) were divorced. All four participants had children. Ms. A exhibited the lowest education qualification (Grade 7), Ms. C obtained a Grade 10 education, while Mses. B and D obtained Grade 12 and further training/qualifications. Only one participant (Ms. A) was unemployed at the time of her crime, and this participant is also the only person with a criminal record of theft (×2) and assault GBH (×1) for which she served an 18-month imprisonment sentence.
The contributing (underlying) issues linked to female participants’ pathways to crime and prison are outlined below.
Incarcerated females and their children
All of the participants had more than one child. Ms. D was the only participant who entered the prison with only one child as her other child (baby) is deceased. Research conducted by Nuytiens (2015) illustrates that many female offenders have troubled relationships with their children and/or poor parent–child bonds. Three of the participants (Mses. A, B and C) were living apart from their children (Nuytiens, 2015). Ms. A’s children grew up with their grandparents, with her contacting them on ‘Saturdays or Sundays’. Ms. B’s children grew up and resided with their grandmother. Ms. C’s children were subjected to family violence and abuse prior to her incarceration. Only Ms. D’s child resided with her until prior to her imprisonment.
Table 2 below depicts the factors that are linked to the female participants’ experiences to their HIV/AIDS status and their involvement in crime.
Lived experiences related to HIV/AIDS and murder.
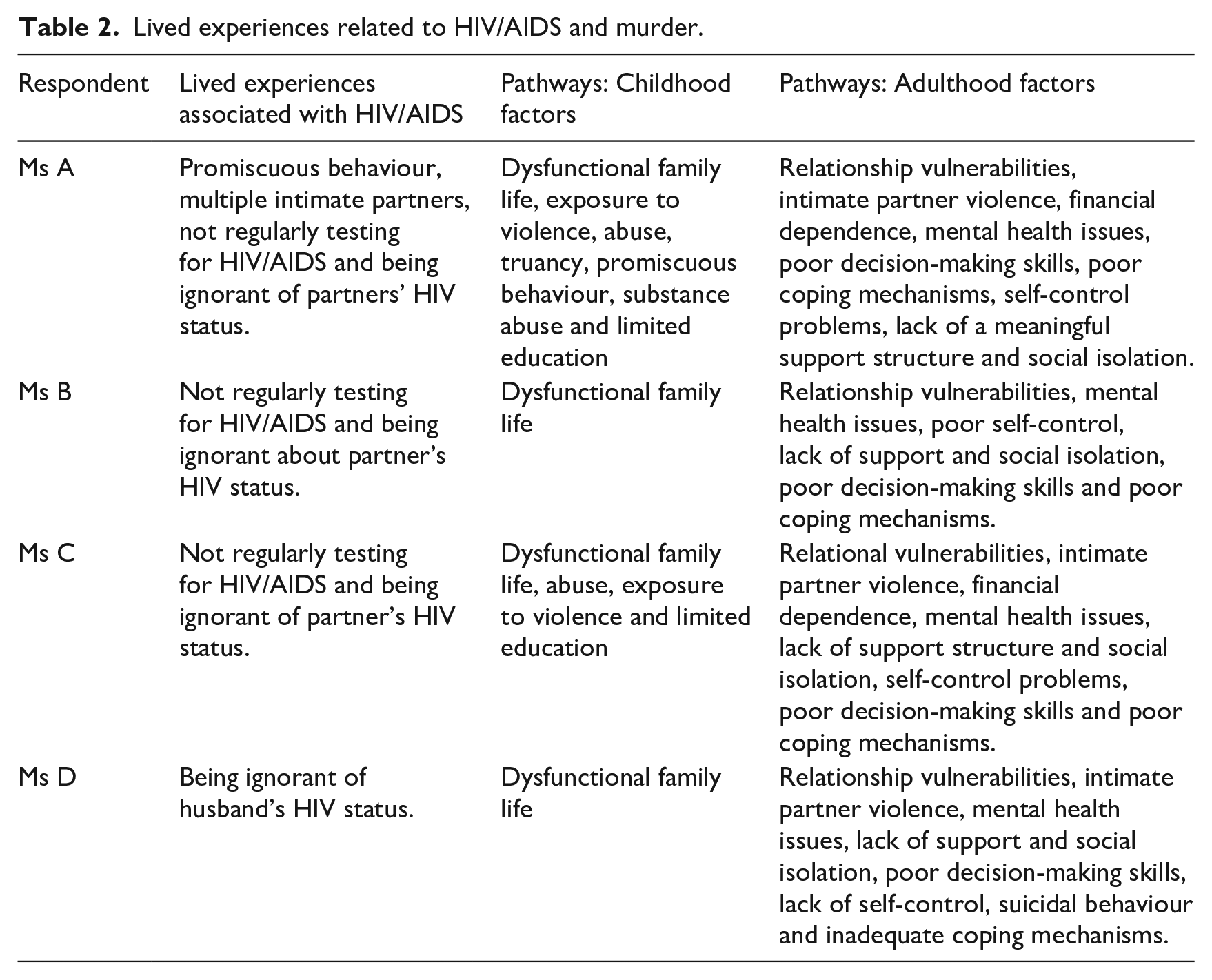
Table 2 represents the female participants’ lived experiences associated with HIV/AIDS and the factors that contributed to their pathways to murder. These factors are outlined below.
Factors linked to female participants’ experiences and HIV/AIDS status
Promiscuous behaviour and infidelity of intimate partners
Only one participant (Ms. A) engaged in promiscuous behaviour that contributed to her HIV status. Ms. A revealed that from the age of 14 years to prior to her imprisonment, she was involved in several sexual relationships. Research (Carney et al., 2019; Ochillo et al., 2017) proves that promiscuity and sex with multiple partners are a risk for HIV/AIDS. On the opposite side, Mses. B and D attributed their HIV-positive status to, respectively, their deceased partner’s (of Ms. B) and husband’s (of Ms. D) unfaithfulness.
Regular testing for HIV/AIDS
Three of the female offenders (Mses. A, B and C) failed to undergo regular HIV/AIDS tests during their intimate relationships. Richter et al. (2010) posit that the stigma attached to HIV/AIDS creates barriers and fear and is one of the reasons why people do not go for regular HIV/AIDS testing. The basis of adequate treatment and prevention of HIV/AIDS is testing for HIV (Wilson et al., 2008). Mses. A and C were tested for HIV/AIDS in prison, while Ms. B went for testing 2 years prior to her crime. Ms. D is the only participant who, due to her work requirements, tested for HIV/AIDS on a regular basis.
Ignorance of intimate partner’s HIV status
All of the participants were ignorant of their partner’s/partners’ HIV status. Ms. A stated that she ‘heard’ of AIDS but thought it will not happen to her. Ms. B was aware of AIDS but was oblivious of her partner’s status and his unfaithfulness. Ms. C also showed no concern about HIV/AIDS prior to her own testing. Only Ms. D was aware of AIDS, and she presumed her husband was too (as he was also tested on a regular basis). Research (HIV i-Base, 2016; Valabdass et al., 2021) suggests that it is important to always know your partner’s HIV status, and that it is better to assume they are positive in order not to put yourself at risk as prevention and regular testing are key to effective treatment and prevention of HIV/AIDS (Valabdass et al., 2021; Wilson et al., 2008).
Factors that contributed to the females’ involvement in murder
According to Nuytiens (2015) and Peltzer (2013), victimisation is a central theme in women’s pathways literature, and childhood and adulthood victimisation are important predictors for involvement in crime. Investigation (Nuytiens, 2015) on gendered pathways to crime has proved that female offenders display individual (childhood abuse, mental stress and depression), relational (interpersonal violence, financial dependence and infidelity) and societal (poverty and low-income jobs) vulnerabilities in their life histories. For this study, the factors that contributed to the female offenders’ involvement in murder are divided into two sections: (1) childhood-related factors to murder and (2) adulthood-related factors and murder.
Childhood-related factors to murder
Adverse childhood factors that predisposed the sample of female offenders include a dysfunctional family life, child abuse, exposure to family violence, truancy, substance abuse, promiscuous behaviour and limited education. These factors are outlined below.
Dysfunctional family life
All of the participants grew up with an absent father (Peltzer, 2013). Two participants (Mses. B and D) enjoyed periodic contact with their fathers, and two participants (Mses. A and C) never saw or met their fathers. Two participants (Mses. C and D) hardly saw their mothers as they were working away from home, and Ms. A lost contact with her mother after she ran away from home when she was 14 years old. Research (Bui, 2018; Degiorgio, 2015; Dennis, 2012; Friedstad, 2012; Lennings et al., 2014; McIvor et al., 2009; Palmer et al., 2014; Walker et al., 2016) is clear that there is a strong correlation between involvement in crime and growing up in a dysfunctional family. Parents’ disconnection is the result of non-empathic relationships with children that are hindered by physical absence (due to work or death) or emotional absence (unavailability) (Nuytiens, 2015). Further research (Callaghan et al., 2018; Lynch et al., 2012) lists family problems as a contributory problem to females’ vulnerability and their pathways to crime.
Exposure to family violence
Only two of the participants (Mses. A and C) reported growing up with family violence. In this regard, Ms. A was subjected to parental domestic violence and physical abuse, whereas Ms. C was exposed to her brothers’ regular fighting. According to Callaghan et al. (2018), Hedderman et al. (2011) and King (2017), many incarcerated women have been exposed to domestic and/or physical violence during their childhoods or have been abused by a family member. Research (Anumba et al., 2012; Callaghan et al., 2018; Hedderman et al., 2011) cites that females who have been subjected to childhood abuse and victimisation are more likely to experience mental health problems, social relationship problems and possible involvement in crime.
Childhood abuse
This section involves physical, emotional and sexual abuse and neglect. Both Mses. A and C were victims of sexual abuse (rape) during their childhoods. Ms. A was gang raped at the age of 14 years, was physically abused by her stepfather and emotionally neglected by her mother. Ms. C was raped by her uncle at the age of 6 years and also emotionally neglected by her mother. Females, and specifically HIV-positive women, display a history of childhood and adulthood sexual abuse (Luyt and Du Preez, 2015; Peltzer, 2013; Valabdass et al., 2021; Walker et al., 2016). Research (Luyt and Du Preez, 2015) on incarcerated women demonstrates that females who were abused as children display psychological problems such as cognitive effects (i.e. self-blame), mood disturbances (anxiety and depression), identity problems, problems pertaining to other people (i.e. distrust) and PTSD into adulthood. Other research (Anumba et al., 2012; Callaghan et al., 2018; Hammerton et al., 2019; Hedderman et al., 2011; Lynch et al., 2012; Valabdass et al., 2021) indicates high rates of child abuse and mental health problems with female offenders.
Truancy
Only one respondent (Ms. A) displayed antisocial and truant behaviour during childhood. Due to Ms. A’s dire home circumstances, she ran away from home, and she used and abused substances from the age of 14 years. According to Nuytiens (2015), victimisation in the family plays a big role in girls running away from home, living on the streets, using substances and getting involved in crime. Carney et al. (2019) concur that it is often a reality that females trade sex as a form of financial survival.
Promiscuous behaviour
Ms. A displayed a history of promiscuous behaviour that commenced at the age of 14 years, and she had multiple sexual partners. Research (Bui, 2018; CARE, 2004; Hopkins, 2016; Morash et al., 2017; Valabdass et al., 2021; Wise, 2017) argues that due to women’s disadvantaged social and economic backgrounds, women frequently engage in risky sexual behaviours for survival purposes. Carney et al. (2019) and Nuytiens (2015) warn about promiscuous behaviour and possible engagement in criminality.
Substance abuse
Only one participant (Ms. A) exhibits a history of substance abuse that commenced when she was 14 years old. Many incarcerated females display histories of substance abuse that are often linked with childhood victimisation, abuse, promiscuous behaviour and mental health problems during adulthood (Anumba et al., 2012; Carney et al., 2019; Hedderman et al., 2011). In like manner, research (Callaghan et al., 2018; Lynch et al., 2012; Pelvin, 2019) illustrates the complex connection between substance abuse, interpersonal violence and mental health problems with incarcerated females.
Limited education
Two participants (Mses. A and C) have limited education. Ms. A completed Grade 7 and Ms. C completed Grade 10. Research (Bui, 2018; Lennings et al., 2014; Peltzer, 2013; Swisher and Dennison, 2016) confirms that poor academic achievement is often the onset of, and escalation into, delinquency and involvement in crime in later years. In addition, research (Callaghan et al., 2018; Kemp et al., 2017; Rocque et al., 2017) demonstrates that school dropout (as with Mses. A and C) and low school achievement are directly linked to a negative life outcome and possible future offending behaviour. Other literature (Nuytiens, 2015) maintains that incomplete schooling has important implications for women’s positions in the job market. It predicts future financial difficulties and amplifies their fragile position in society. In South Africa, limited school education is a widespread problem and these researchers mention that between 50% and 60% of adolescents do not complete high school education (Carney et al., 2019).
Adulthood-related factors and murder
Female offenders often display past trauma, domestic violence/interpersonal violence, substance abuse, mental health symptomatology, economic marginalisation, post-traumatic stress disorder and psychiatric problems (i.e. anxiety, distress, depression, exposure to trauma, neurosis, phobias, self-mutilation and suicide ideation and behaviour) (Chen et al., 2014; Eriksson et al., 2018). These factors are discussed below.
Relationship vulnerabilities
All of the participants experienced relationship vulnerabilities with their intimate partners. Mses. A, B, C and D’s intimate relationships are characterised by infidelity, and these participants (Mses. A, B, C and D) reported abuse in their relationships. Research (Callaghan et al., 2018; Nuytiens, 2015; Pelvin, 2019) found that female offenders who experienced troubled intimate relationships with meaningful others, such as parents, are often further victimised and abused (emotionally, sexually and physically) by their intimate partners. In turn, intimate relational vulnerability enhances feelings of insecurity and worthlessness and may lead to substance abuse and post-traumatic stress symptoms (Callaghan et al., 2018; Pelvin, 2019). This chain of events might ignite crimes such as murder (Callaghan et al., 2018; Morash et al., 2017; Nuytiens, 2015). Furthermore, relationships form a sound foundation for psychological health and disconnection, and isolation from significant others may become a breeding ground for psychological distress. Thus, unhealthy and vulnerable relationships may lead to murder (Anumba et al., 2012; Pelvin, 2019).
IPV
All four participants were exposed to domestic violence in their intimate relationships. Ms. B divorced her ex-husband due to domestic violence. Mses. A, C and D’s last encounters of domestic violence were precursors to the murders. Ms. C reported being raped by her boyfriend. Gender-based violence has increased significantly in South Africa and nears a ‘national emergency’ (Brandt, 2019; Merten, 2019; Pelvin, 2019; Valabdass et al., 2021). Research (Friedstad, 2012; Pelvin, 2019; Sun et al., 2016) proves a strong relationship between female offenders and a history of IPV. Female offenders express high rates of interpersonal violence that are associated with mental health problems and substance use problems (Callaghan et al., 2018; Lynch et al., 2012; Pelvin, 2019). Other researchers (Bloom et al., 2004; Green et al., 2005) found that between 77% and 98% of female offenders’ narrated lived experiences are linked with interpersonal/partner violence. Many of these females developed ensuing major depressive disorders, PTSD and substance abuse problems. Violence perpetrated against women shape gender norms, it dehumanises and objectifies women as objects to be abused (Parry and Segalo, 2017; Pelvin, 2019).
Substance abuse
Only one participant (Ms. A) exhibits a history of abuse (from childhood to incarceration). The relationship between substance abuse and HIV/AIDS has been well established in research (Hopkins, 2016; Lichtenstein and Barber, 2016; Wise, 2017). Drugs provide a feeling of relaxation and an escape from reality and abuse (Nuytiens, 2015). Substance abuse is a major problem for female offenders (Morash et al., 2017) and alcohol and drug addictions mirror women’s brittle position in society (Nuytiens, 2015). Related to this, Smith (2017) indicates that drug abuse prior to arrest is linked to childhood abuse and is a leading pathway to many females’ criminal involvement.
Financial dependence
Two of the participants (Mses. A and Ms C) were financially dependent on their deceased partners. Ms. A was reliant on the money for the children. Ms. C was financially dependent on her partner, and she was forced to partake in sexual encounters with him, even though they were not living together anymore, to secure money for her children. Thus, the abusive nature of their relationship was positioned at a financial level (Nuytiens, 2015). Women who are economically disadvantaged are often oppressed, abused, controlled and exploited by men in exchange for sexual favours (Bernard et al., 2021). Evidently, many incarcerated females’ lived experiences are characterised by financial difficulties prior to their imprisonment (Nuytiens, 2015).
Mental health issues
This segment covers psychological-related factors, such as humiliation, feelings of helplessness and hopelessness, desperation, anger, revenge, shame, guilt, distress, depression, stigmatisation and PTSD. All of the female offenders reported psychological and mental health distress related to the discovery of their HIV status. Three participants (Mses. A, C and D) indicated the same with regard to the IPV that they endured. With regard to the latter, the following mental health issues were experienced: anger and humiliation (Mses. A, C and D). Ms A took revenge as the deceased gave her a ‘death sentence’ because he infected her with AIDS. Ms. D experienced feelings of helplessness and hopelessness, and she was desperate to make an immediate and favourable change to her dire circumstances.
Regarding the discovery of their HIV status, all of the participants experienced feelings of anger, disbelief, shock and distress. In addition, anxiety (Ms. A), shame (Mses. A and B), guilt (Ms. A), feeling depressed (Mses. B and D), stress (Mses. A and D), disengagement (Ms. A), eating problems (Ms. A), sleeping problems (Mses. A and B), humiliation (Mses. A, B, C and D), being afraid of stigma (Ms. B) and suicidal ideation and behaviour (Mses. B and D) were experienced. Finally, two of the participants (Mses. B and D) felt humiliated by their partners’ infidelity.
Female inmates reported higher rates of trauma and mental health problems than their counterparts (Eriksson et al., 2018; King, 2017) and they displayed problems such as depression, PTSD and suicide ideation (Callaghan et al., 2018; Lynch et al., 2012). Trestman et al. (2007) questioned 200 incarcerated women and found that 56% of the females experienced psychological disorders. Green et al. (2005) interviewed 100 female offenders and report that a fourth of the females experienced major depressive disorder, almost one in five of the females suffered from PTSD and one-third of the females had a psychiatric diagnosis. Morash et al. (2017) note that anger, depression and PTSD fuel female offenders’ violent behaviour. In turn, Ramlagan et al. (2019) postulate that HIV-related stigma plays a big role in the emotional function of a person infected with HIV/AIDS. Females with a history of victimisation and childhood abuse are more likely to experience mental health issues and to become involved in criminality (Anumba et al., 2012).
Lack of support and social isolation
All of the participants lacked meaningful support and were socially isolated prior to their crimes. For Ms. A, a lack of familial support pushed her into a promiscuous lifestyle, ‘looking for a better life’. Ms. D’s isolation and feelings of rejection contributed to her suicidal behaviour and the murder of her baby and attempted murder of her son. Persons who lack a positive support structure are more prone to criminality (McIvor et al., 2009; Peltzer, 2013; Pelvin, 2019). Social isolation is an important factor in decision-making, and the absence of social support is a critical factor in criminality (Nuytiens, 2015). Many female offenders lacked adequate social support and lived isolated lives prior to their incarceration (Nuytiens, 2015). Thus, disconnection and isolation are main triggers for psychological distress and female crime, and relationships that nurture psychological health assist with coping with adversity (Anumba et al., 2012).
Poor coping mechanisms
Dismal family circumstances for Mses. A and C, and abusive intimate personal relationships for Mses. A, C and D resulted in the offenders displaying poor coping mechanisms that are linked to their poor decision-making abilities and subsequent commission of murders (Dennis, 2012; Friedstad, 2012; Morash et al., 2017; Ochillo et al., 2017; Palmer et al., 2014). In addition, Ms. A used substances to cope with her lack of upbringing and her abusive relationships. A lack of life skills (i.e. coping mechanisms) is detrimental for female offenders and their effective rehabilitation. Psychological assistance is needed in order for them to learn coping strategies so that they can deal with their problems (Green et al., 2005; Hedderman et al., 2011; Lynch et al., 2012).
Poor decision-making skills
All the participants displayed poor decision-making skills prior to committing the murders that contributed to their criminal involvement. Mses. A and C made poor decisions pertaining to their lifestyles, truancy (running away behaviour), substance abuse, promiscuous behaviour (Ms. A) and an ongoing sexual relationship with an ex-partner for money. Research (Dennis, 2012; Hedderman et al., 2011; Morash et al., 2017; Wooditch et al., 2014; Zavala et al., 2019) proves a definite link between the inability to make sound decisions and crime, and it indicates the need for the acquirement of decision-making and problem-solving skills. Solomon et al. (2012) relate that there is a definite link between abuse, trauma, mental health issues, emotional difficulties, poor decision-making and crime.
Self-control
All of the participants lacked self-control to desist from murder of their intimate partners, including a lack of self-control to desist from murdering a child and attempted murder with regard to the second child (as is the case with Ms. D). In this regard, research (Lynch et al., 2012; Sun et al., 2016; Tully et al., 2015) supports the notion that a lack of self-control is a robust predictor for offending behaviour, and Zavala et al. (2019) reiterate a connection between self-control, victimisation and IPV.
Suicidal behaviour
Ms. D tried to commit suicide, and, in the process, she killed her baby, while she and her son survived. Women who experience family problems exhibit more internally directed problems such as depression, suicidal behaviour and self-mutilation – both during childhood and in adulthood (Nuytiens, 2015). Aborisade and Fayemi (2016) maintain that female offenders have higher rates of suicide and self-harm behaviour when incarcerated than men and the outside community. These researchers further claim that female offenders with a history of mental health problems and challenging intimate relationships adapt poorly to the prison environment, and this may lead to suicidal ideation and suicide behaviour (Aborisade and Fayemi, 2016).
Female breadwinners
Two participants (Mses. A and C) were employed in low-income jobs (domestic work) and were responsible for their children’s living expenses. The other two (Mses. B and D) participants were also the breadwinners for their children. Although Ms. D was married, she stated that her husband did not financially contribute to the children, and this created a lot of financial stress for her in providing for the children, and it furthermore contributed to the murder and attempted murder. Many South African women are the sole breadwinners in their homes, providing the main financial support for their children and families (Parry and Segalo, 2017), and there is an over representation of women in informal work with poor pay as a result of limited education and a lack of formal training (Parry and Segalo, 2017). The majority of South African women are working in a labour market with the poorest salaries, such as domestic work (Parry and Segalo, 2017). Also, being a breadwinner creates financial stress, and poor employment opportunities may result in involvement in crime (Degiorgio, 2015; Sun et al., 2016; Wooditch et al., 2014).
HIV-positive status and coping with HIV/AIDS
Two participants (Mses. A and D) found out about their HIV status while incarcerated, and two participants (Mses. B and C) knew their HIV status before entering the prison. All of the participants were appalled when they found out about their HIV status. People who are HIV positive are initially shocked about their HIV status and once the news is out in the open, their families are ever so often compelled to judgement, discrimination and hostility that are related to the stigmatisation of HIV/AIDS (Makoae et al., 2008). HIV/AIDS arouses public fear and denunciation of those infected, which create stigma and avoidance of the HIV-positive persons. This, in turn, influences HIV-positive persons’ quality of life, in seeking counselling or treatment, creating anxiety, distress, depression, social withdrawal, poor adjustment, unwillingness to reveal their HIV status and an inability to cope with their infection (Makoae et al., 2008).
The nexus between HIV/AIDS and females that committed murder
The following two questions are directly linked to, and illustrate the nexus between, HIV-positive females and their involvement in murder: (1) What contributed to the female participants’ HIV-positive status? and (2) How did the female participants’ HIV-positive status shape their involvement in murder?
In illustrating the nexus between HIV-positive females’ experiences and their involvement in murder, the findings produced the following three main themes:
Promiscuous behaviour and infidelity of intimate partners. Only one participant was involved in promiscuous behaviour (from the age of 14 years to prior to her imprisonment), and she enjoyed sexual relationships with multiple intimate partners that might have contributed to her HIV status. However, two participants attributed their partners’ infidelity to their HIV status.
Regular testing of HIV/AIDS. Three participants failed to go for regular testing for HIV/AIDS and were ignorant about their HIV status.
Ignorance of intimate partner’s status. All four of the participants were oblivious about their intimate partners’ HIV status, and they presumed that they (their partners) were sexually responsible and HIV-negative. Only one participant knew about her husband’s infidelity, but she assumed he was HIV-negative.
In establishing how the females’ HIV-positive status shaped their involvement in murder, specific childhood-related and adulthood-related factors were identified.
Seven childhood-related factors that may have laid the foundation for evolving personal insecurities/vulnerabilities, unresolved inner-conflicts, emotional instability and cognitive and skills deficits were identified, and these factors include the following:
Dysfunctional family life. All of the participants grew up with absent fathers. Two of the females enjoyed sporadically contact with their mothers, and one participant lost contact with her mother during her childhood.
Exposure to family violence. Two of the females grew up with violence within the family. One female was exposed to parental domestic violence and the other female was subjected to sibling violence.
Childhood abuse. Two of the participants indicated that they were raped during their childhood, and one of these females experienced physical abuse and emotional neglect at home.
Truancy. Only one female displayed antisocial and truant behaviour during childhood that encompassed run away behaviour and experimenting with alcohol and drugs.
Promiscuous behaviour. One female was involved in promiscuous behaviour during her childhood years that expanded into adulthood.
Substance abuse. One participant used drugs (alcohol, Mandrax and marijuana) at the age of 14 years.
Limited education. Two of the females obtained low scholastic education – one of them completed Grade 7 and the other one completed Grade 10.
Ten adulthood-related factors linked to the females’ involvement in murder were identified and these factors include the following:
Relational vulnerability. All of the females experienced relationship vulnerabilities, either in the form of abusive relationships or infidelity from their partners.
IPV. Again, all of the participants reported physical abuse, and one of them was also raped by her partner.
Substance abuse. Only one female exhibited a history of substance abuse.
Financial dependence. Two of the participants were financially dependent on their partners.
Mental health issues. All of the females reported symptoms related to psychological and mental health issues, such as anger, depression, eating and sleeping problems, shock, disbelief, shame, guilt, disengagement, stigmatisation, suicidal ideation and suicidal behaviour.
Lack of support and social isolation. All of the participants lacked meaningful support and were socially isolated prior to them committing the murders.
Coping mechanisms. All four of the participants exhibited a lack of coping mechanisms in handling their dire personal circumstances prior to committing the murders. One of the females used alcohol and drugs to cope with her abusive partners.
Decision-making skills. With all of the participants, their poor decision-making skills contributed to them committing the murders.
Self-control. All of the females showed poor self-control to desist from murdering their partners, a child and attempted murder of another child.
Suicidal behaviour. One female displayed a history of suicidal behaviour and ideation – once with the killing of her baby and attempted murder of her second child, and the second time when she was in prison.
In sum, the findings illustrate the nexus between the females’ lifestyle experiences (promiscuity and infidelity of partners), ignorance of their partners’ HIV status, not going for regular HIV/AIDS tests and their own HIV status. This in turn, is interlinked with the females’ childhood and adulthood victimisation experiences that determined their pathways to murder.
Implications and limitations of research
Notwithstanding the fact that this research is of a qualitative nature, the females’ revelations illustrate the richness of the data, and it provided the participants with ‘a voice’ regarding their experiences and narratives related to their HIV status and the murders they committed. The findings highlight this marginalised offender population’s hardship that the females endured that ultimately contributed to the murder of their partners/spouses, baby and attempted murder of a second child. Visibly, due to the small sample size, the research findings cannot be generalised to the greater population of HIV-positive female offenders who committed murder. Further and more elaborate research is needed to highlight and validate the factors that contributed to HIV-positive female offenders whose crimes of murder are linked to their HIV status.
Conclusion
Females who commit murder is a complex crime phenomenon. HIV-positive females whose crimes of murder are linked to their HIV status are more multi-layered than simple exposition of victim–offender relationships. The goal of this research was to explore selected females’ experiences that contributed to their HIV status and the intricate factors associated with the murder of their partners/spouses, a baby and the attempted murder of another child. Two participants discovered in prison that they were HIV positive, and two females knew about their HIV status before they entered the prison. Factors such as promiscuousness, not going for regular HIV/AIDS testing and ignorance of intimate partners’ HIV status contributed to the participants’ HIV status. Underlying adverse childhood factors that contributed to the females’ paths to murder included exposure to dysfunctional families, violence, truant behaviour, substance abuse and limited education. Adulthood factors that shaped the female offenders’ pathways to murder included relationship vulnerabilities, substance abuse, mental health issues, lack of support and social isolation. Other factors that played a role are poor coping mechanisms and decision-making skills, a lack of self-control and suicidal behaviour.
Footnotes
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.