
Abstract
Using the cultural consonance theory and the assumptions embedded in the culture consensus model, the present article addresses the associations between consensually understood and collectively shared cultural models and individual mental health. The study specifically explored the role of internalization. A structured survey was developed to extract the local variant of the American cultural model of a “good, worthy life.” The data collected in New England in fall 2012 (N = 306) contained measures of the individual familiarity with the cultural model, the degree of internalization of its elements, the extent to which each informant’s lifestyle matched the model in their daily life, and measures of positive and negative mental health. The results confirm that the degree of cultural competence and internalization of cultural ideas affect inter-informant variation in both negative and positive mental health, but the relationship is a complex one.
Congruity With Culture and Mental Health Outcomes
The importance of congruity with cultural standards for one’s well-being and self-concept is often cited in psychological research (Cialdini & Goldstein, 2004). Recent cross-cultural studies present evidence of reduced levels of well-being and self-esteem in individuals whose behavior or beliefs deviate from their society’s axiological/normative profile (Kalmijn & Uunk, 2007). The negative consequences of one’s not meeting societal expectations have been documented for a diverse range of personal attributes including morality, religiosity, employment, and personality traits (Fulmer et al., 2010; Gebauer, Sedikides, & Neberich, 2012; Stavrova, Fetchenhauer, & Schlösser, 2013).
An important instance of the interrelationship between matching cultural standards in individual lifestyle and objective health outcomes is represented in the phenomenon referred to as cultural consonance: “the degree to which individuals approximate, in their own beliefs and behaviors, the prototypes for those beliefs and behaviors encoded in shared cultural models” 1 (Dressler, 2005; Dressler & Bindon, 2000). Understood thus, the cultural consonance model develops the specific role of culture (conceived of as a measurable variable) in generating the psychosocial stress affecting the human condition (Dressler, 2005). Its starting point takes an intersubjective view of culture, highlighting its ability to affect what individuals intersubjectively believe to be important in their society. The collective consensus that emerges regarding desirable attributes or normative standards within a group holds even if it is perceived erroneously (Chiu, Gelfand, Yamagishi, Shteynberg, & Wan, 2010; Miller & Prentice, 1994; Prentice & Miller, 1993; Zou et al., 2009), and can generate mutual understanding of whether or not a culturally valued standard is achieved by an individual. The part and parcel of the cultural consonance framework is that culture can act as a chronic stressor and, as such, systematically affect individual health outcomes. The central empirical claim of cultural consonance posits that one’s perceived failure to match a socially desirable standard encoded in a cultural model (i.e., lack of cultural consonance) results in the decrease in individual physical and mental health (greater depression, higher arterial blood pressure, and greater body mass; Dressler, 1991, 2004a, 2004b, 2007a; Dressler, Ribeiro, Balieiro, Oths, & Santos, 2004; Dressler & Santos, 2000). These effects were also found to be independent from stressful life events, which altogether points to cultural consonance as a potential source of chronic stressor producing generalized psychological distress (Dressler, Balieiro, Ribeiro, & Santos, 2007a, 2007b). They were found to be particularly strong for the domains of social distinction and affiliation (Dressler, Balieiro, Ribeiro, & Santos, 2005, 2007a, 2007b). Higher cultural consonance in the cultural domains of lifestyle, national identity, food, and social support was associated with lower psychological distress in several samples from the United States and Brazil (Dressler et al., 2007a). Although there is evidence that the individual deficit in cultural consonance increases likelihood of negative mental health, cultural consonance had an inverse effect on depressive symptoms (measured by using Beck’s Depression Inventory [BDI-I]; Beck, Ward, Mendelson, & Erbaugh, 1961), independent of the occurrence of stressful life events (a risk factor for depression) in a Brazilian sample; the effect was detectable after a 2-year test–retest period (Dressler, Balieiro, Ribeiro, & Santos, 2008). The picture appears to be more complex with respect to explaining the effects of cultural consonance on positive mental health, as it cannot be satisfactorily predicted by cultural consonance alone (Maltseva, 2014b, 2015).
Cultural Models and Internalized Cultural Ideas
Cultural models arrange cultural knowledge of various domains in the individual mind and direct the individual interpretation of events, motivation, and behavior based on the mutually shared understanding of cultural model’s organizing principles. Cultural models are informed by values, social axioms, and similar enculturated normative ideas that form an intersubjectively shared axiological hierarchy within a group. One’s degree of knowledge of the cultural model is the measure of individual cultural competence (Romney, Weller, & Batchelder, 1986). Yet mere familiarity with cultural models or extensive knowledge about them does not necessarily imply complying with them in behavior or warrant them having definite implications for psychological health. A much more important condition for the effective interference of normative culture with one’s motivations, appraisals, and beliefs about self is that of internalization of culture’s normative ideas. Internalizing the elements of a cultural worldview results not only in their acceptance by the internalizer but also in their integration into his or her internal motivational system as personally meaningful (Spiro, 1997). When one internalizes an idea or belief, one cognitively and emotionally absorbs the originally external cultural belief or idea and integrates them into their self. One characteristic feature of internalized ideas is that they are no longer experienced as imposed by the outside world; “embedded, penetrating ideas,” they fit organically into the self-narrative as if they were there from the very beginning (Kral, 1998, p. 223). When a normative idea is internalized, not only can the behavior elicited by the norm be expected to be more frequent compared with the condition when it is followed merely instrumentally (Gintis, 2011), but it also becomes fused with the internally motivated goals (Sheldon et al., 2004). Therefore, individuals successful at pursuing such personally meaningful, internalized standards are not only living up to the socially desirable (external) criteria but are also self-concordant, which is beneficial for mental health (Sheldon, Ryan, Deci, & Kasser, 2004). Failure to achieve self-concordance, on the contrary, can be expected to have the opposite mental health outcomes for individuals internalizing cultural models.
Individuals are capable of internalizing both positive and negative ideas (e.g., internalized stigma; Thoits & Link, 2016). In this manner the internalized ideas regarding what the society would have us believe about our relative cultural value and place in the world come to be firmly held by individuals. When conceptualized this way, internalized normative ideas are more likely to participate in a stress mechanism via self-appraisals with respect to cultural standards and in social comparison, and as such more plausibly have an impact on individual health.
It is important to articulate the distinctions between the concepts of internalization and consonance with culture that inform current research. First of all, consonance implies that one corresponds to the culturally shared standard/profile in terms of knowledge or behavior. It means that the individual knows or does something that is culturally correct. Some degree of correspondence between the individual and shared collective knowledge is typically a result of enculturation and is measurable in terms of individual’s overlap with collectively shared knowledge assessed within the culture consensus model (cf. Romney, 1999; Weller, 2007). This measure captures the degree of cultural competence (Romney, 1999), that is, knowing the “culturally correct answer.” In the present study, it is proposed that internalization is qualitatively different from such correspondence between the individual and collective profiles measured by Romney’s culture consensus model, as well as from cultural consonance measured by Dressler’s cultural consonance model, in several important ways, which should be reflected in the manner it is operationalized and measured.
First, a measure of internalization should reflect the translation of cognitive knowledge about (or understanding of) a cultural idea or standard into emotional response (Spiro, 1997). While congruity/consonance is a cognitive or behavioral domain, internalization supplies an emotional dimension to cultural knowledge. When you internalize, not only do you know about something, but it also informs your motivation to behave (not just gives you knowledge).
Second, directedness toward the self should also be pronounced, as by definition, internalization actualizes some ideas as part of self-concept, making the internalized attribute self-descriptive. As a result of internalization, an individual does not distinguish between the internalized cultural ideas (that used to be external) and his or her internal attributes, preferences, or qualities. Therefore, the individual degree of internalization can be gauged as an extent to which the person is unable to segregate himself or herself from the idea, and thus, the outcome of failing to match the internalized cultural standard means “not being something” rather than “not having/doing something.”
Furthermore, from Spiro’s (1997) seminal work on internalization, we infer that one of the most prominent consequences of internalization of a normative cultural idea or a standard is that once it is integrated with the self, it is difficult to go against it, as such a violation would also mean turning against the self. It implies a state of some psychological conflict, pain, or experience of discomfort if the individual fails to correspond to the internalized standard or idea. It is also particularly apparent with the example of internalizing negative beliefs (such as internalized stigma), which leads individuals to believe that they are actually “tainted” and “damaged goods” because of this attribute (Drapalski et al., 2013). Given that ideas that can be internalized can be either good or bad (stigma, self-stereotypes, etc.), the effect of internalization on individual mental health appears distinct from that of consonance with culture.
That said, cultural consonance framework does not provide an explicit discussion of the mechanism that incorporates the psychological states into the culture–behavior–health relationship. However, the significance of the psychological component in cultural consonance should not be underestimated. First, empirical evidence unequivocally links psychological states and health outcomes, including both physical and mental illness. Although it is not clear if the relationship is direct or mediated (the results from cross-cultural studies are inconclusive), overall, the data suggest that the associations of positive affect with health outcomes is independent from those of negative affect (and depressed mood), and that positive and negative effects have their distinct biological correlates that can benefit or reduce health, correspondingly (Steptoe, Dockray, & Wordle, 2009). Second, there is important evidence regarding the nature of the link between depression, emotional states, and sociocultural normativity. Specifically, in Western and Eastern societies depression affects the individual’s emotional reactivity in both positive and negative contexts by lessening one’s adherence to the cultural norms regarding desirability of emotional displays (Chentsova-Dutton et al., 2007; Chentsova-Dutton, & Tsai, 2010; Chentsova-Dutton, Tsai, & Gotlib, 2010). The present work seeks to shed more light onto the psychological component of cultural consonance and refine our understanding of the interaction of this component with the cultural substrate.
Cultural Consonance and Cultural Models: The Role of Internalization
The goal of the present study is to investigate the relationship between cultural consonance and mental health. The current research question was initially developed in the author’s work in Sweden 2 (2008-2009), where the effects of not matching the standards of normative culture on subjective well-being (SWB) were neutral or slightly negative, that is, not explained by the cultural consonance model that was originally developed on Brazilian data. The author’s research in Sweden lead to investigating possible sociocultural factors other than matching the culturally desirable lifestyle that might intensify or even direct the effects of cultural consonance in individuals (cf. Lu, 2006). Specifically, cultural competence (Romney et al., 1986) and internalization were examined. Internalization was defined as the degree of discomfort an informant would feel if he or she did not live up to the normative standard (Shore, 1996; Shweder, 1991; Spiro, 1997). The results of a series of follow-up studies in New England (fall 2009 to fall 2012, total N = 506) suggested that neither knowledge of cultural models nor their behavioral re-enactment in lifestyle adequately predicted mental health negatively or positively, while the degree of internalization of cultural ideas directly predicted inter-informant variation in SWB (Maltseva, 2015). In these studies, internalization was also shown to be distinct from individual value priorities (operationalized as the degree to which the informant deems the collectively salient item personally important), which, unlike internalization, did not affect SWB (Maltseva, 2015). Finally, lack of cultural competence (poor knowledge of the cultural model) reliably predicted more severe dysfunctional attitudes but not lower SWB in a Swedish sample 3 (Maltseva, 2015).
Given the above findings, the present study specifically stresses the condition of internalization as an important component of cultural consonance. Although there is a logical expectation that internalized ideas are a powerful factor in the relationship among cultural knowledge, behavior, and health, the impact of internalization was not considered in the previous research on cultural consonance (Maltseva, 2014b, 2015). Instead, the causal relationship between one’s lack of consonance with culture and suboptimal health outcomes is conceived of within this framework as alike to the link that exists between the norm and the behavior it elicits. Although fitting to discuss the material aspect of consonance in lifestyle, this approach strips the cultural consonance model of possible psychological insight regarding how individuals perceive and negotiate their relative cultural value with respect to the mainstream societal standards.
A separate methodological problem that the present study seeks to address is that much of the published work on cultural consonance does not distinguish between its cognitive and material aspects while assessing the relationship between the individual’s approximation to cultural standards and his or her mental health, and uses self-reports on individual’s access to the socially desirable material items (possessions such as TV sets, kitchen appliances, accessible foods, etc.) as a measure of an individual’s consonance with normative culture (Dressler, 2007a, 2007b; Reyes-Garcia et al., 2010; cf. Maltseva, 2015). Equally important, although the emic status of the items against which the consonance is measured is ensured by using a free-listing procedure, the ensuing lists of socially desirable items do not compare with the definition of cultural models neither for their complexity nor for their structure. 4 Furthermore, the collective nature of cultural models obtained in the research on cultural consonance is not explicitly demonstrated, to rule out the possibility that the construct in question reflects, in fact, individual preferences averaged within a sample (Fischer, 2009 for review; Maltseva, 2014a, 2015; Van de Vijver, van Hemert, & Poortinga, 2008). Therefore, although the benefits of the methodological approach that reduces cultural models to cultural domains in biocultural research are recognized, its outcomes do not bring the desirable clarity. It tends to leave out many salient cognitive activities humans engage in when feeling unhappy about one’s current situation (such as cognitive reframing, denial, rationalizing, etc.). Overall, it ignores the possibility that the link between low cultural consonance and depression is not a uniformly direct relationship. 5
The present study was designed to address some of the issues that are related to psychosocial factors in cultural consonance, and to put forth several new questions. Based on the collected empirical evidence, cultural consonance may have a more complex mechanism than is currently believed. Namely, there can be a range of psychological processes adding to cultural factors implicated in cultural consonance that requires multidisciplinary contributions to offer a more complete picture.
Based on the theoretical implications discussed in the section on internalization (e.g., adaptive functions, Gintis, 2011; and self-concordance, Ryan & Deci, 2000; Sheldon et al., 2004), and given the reasoning involved in the intersubjective approach to culture (achieving maintenance of consensus and intersubjective reality within a group; Chiu et al., 2010, pp. 484-485; Wan, Torelli, & Chiu, 2010), the following hypotheses were advanced in the study:
In line with the logic of cultural consonance research, it was predicted that:
Higher cultural competence would confer adaptive advantages, including benefits such as higher positive mental health and lower negative mental health. As individual’s greater knowledge about the cultural model (as reflected in higher factor loadings on the first principal component on cultural model measure; Chiu et al., 2010; Wan, Torelli, & Chiu, 2010) can be expected to promote his or her functionality in society, higher correspondence between individual and collective knowledge about the cultural model is likely to entail a better sense of mastery over one’s daily activities, which, in turn, can be expected to positively affect mental health (Chiu et al., 2010). It was, therefore, predicted that:
In view of the empirically based expectations that the effects of internalization and cultural competence might not be independent, an additional exploratory hypothesis was considered. The study evaluated whether internalization and cultural competence would have different effects on mental health either independently or interactively.
Method
Participants
The data collection was conducted at the University of Connecticut, Storrs in fall 2012. The final sample consisted mainly of undergraduates of the University of Connecticut and members of their social networks, N = 306, 54% female, mean age 20 years (SD = 3.18). Individuals in the sample came predominantly from New England (189 from Connecticut, 19 from New York, 16 from Massachusetts, 10 from New Jersey), although there were representatives of 19 different U.S. states, including California (n = 5), Ohio (n = 3), Virginia (n = 3), Colorado (n = 2), Florida (n = 2), Maryland (n = 2), Rhode Island (n = 2), Vermont (n = 2), Arizona (n = 1), Illinois (n = 1), Maine (n = 1), and so on. The sample included individuals from a variety of majors, childhood environments, network sizes, family composition, parents’ education, religiosity, and income. Out of those participants who were employed, 6.6% worked full-time, 3.3% reported a 3/4 workload, 16.9% worked half-time, and 19.3% less than half-time; 41% of all the participants were in a relationship (had a boyfriend or girlfriend) at the moment of surveying. The details of sample composition are offered in Table 1.
Sample Composition: Demographics and Lifestyle Items (N = 306).
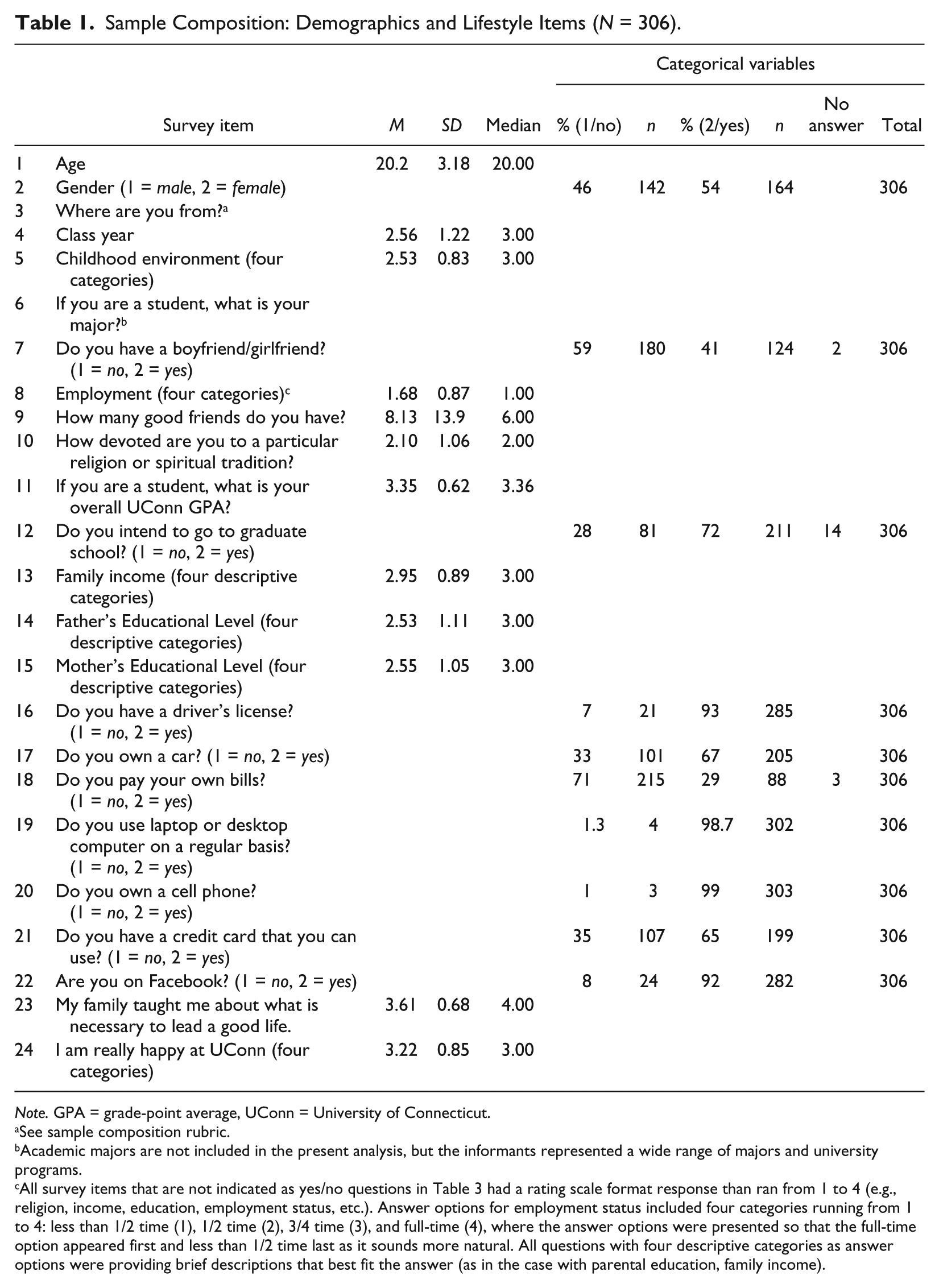
Note. GPA = grade-point average, UConn = University of Connecticut.
See sample composition rubric.
Academic majors are not included in the present analysis, but the informants represented a wide range of majors and university programs.
All survey items that are not indicated as yes/no questions in Table 3 had a rating scale format response than ran from 1 to 4 (e.g., religion, income, education, employment status, etc.). Answer options for employment status included four categories running from 1 to 4: less than 1/2 time (1), 1/2 time (2), 3/4 time (3), and full-time (4), where the answer options were presented so that the full-time option appeared first and less than 1/2 time last as it sounds more natural. All questions with four descriptive categories as answer options were providing brief descriptions that best fit the answer (as in the case with parental education, family income).
Both the initial categories and the resulting survey items focused on the local variant of the cultural model of a good, worthy life within the student population in New England. Given the varieties of cultural models co-existing within a population (cf. Strauss, 2012), and the inter-informant consensus suggesting the shared nature of the extracted cultural model, this sampling strategy did not pose a problem for testing the hypotheses. By sampling from college students, collecting data from a subpopulation with a distinct institutionalized subculture (i.e., the University) was achieved. Elicitation of a universally shared American cultural model was not the goal of the project. As normative culture is expected to be shared, mutually understood, and relatively homogeneous, purposive sampling targeting typical cases is acceptable to produce good empirical generalizations.
Measures
The study collected self-reported cognitive and lifestyle data to extract the cultural model of a good, worthy life, and to evaluate whether the individual’s degree of correspondence to the cultural model (as reflected in lifestyle) predicted individual’s emotional health (measured both in terms of depressive symptoms and as levels of flourishing). The domain of a good, worthy life was chosen for this study because it is a salient positive concept from everyday life. This domain is known to the informants of any age, gender, or profession, and despite some degree of expected variation, there is a low likelihood of distortion due to unavailability of information about it or cultural prohibitions to release it. It is also a domain that was used by the researchers of cultural consonance (Dressler & Bindon, 2000; Reyes-Garcia et al., 2010).
Cultural model items
Data collection involved an initial free-listing (Ross, 2004) to obtain the emic characteristics to begin constructing measures of the cultural model. During the free-listing procedure, the participants (N=19; students of both genders enrolled in Evolution of Social Cognition course at the University of Connecticut, Storrs) were asked to list their responses to six stimuli eliciting the domain features for formulating the elements of the cultural model of a good, worthy life at a later stage: (a) _______ is an important virtue in the United States; (b) In the United States, to be taken seriously, one must have_____. (c) In the United States, to be taken seriously, one must be ____; (d) In the United States, to be taken seriously, one must be able to _____; (e) In the United States, having some of these things eventually makes people happy: _____; (f) Ideally, in the adult life, one should achieve some of the following: ____. An average pool of items elicited by each free-listing stimulus was 130 words. In all, nine to 10 items on each list had a frequency of above 3, combined with their prominent position in recall (as premised by the intersubjective values consensus as discussed in Chiu et al., 2010, pp. 483-484). Culturally salient, positively valenced items included education, freedom, money, honesty, independence, family, friends, job/career, happiness, owning a house/having a good home, having spouse and children, a pet, and a car. An average pool of items elicited by each free-listing stimulus was very similar to the free-listing results reported in Maltseva (2015). In the current sample (UConn), other words such as having enough money/owning expensive items, independence (having a job vs. having one’s parents pay one’s bills), education/career prospects (year, major, grade-point average [GPA], plans to attend graduate school), having friends (both as Facebook-based and actual network sizes), driving a car, and having a romantic partner emerged (see “Lifestyle Items” section).
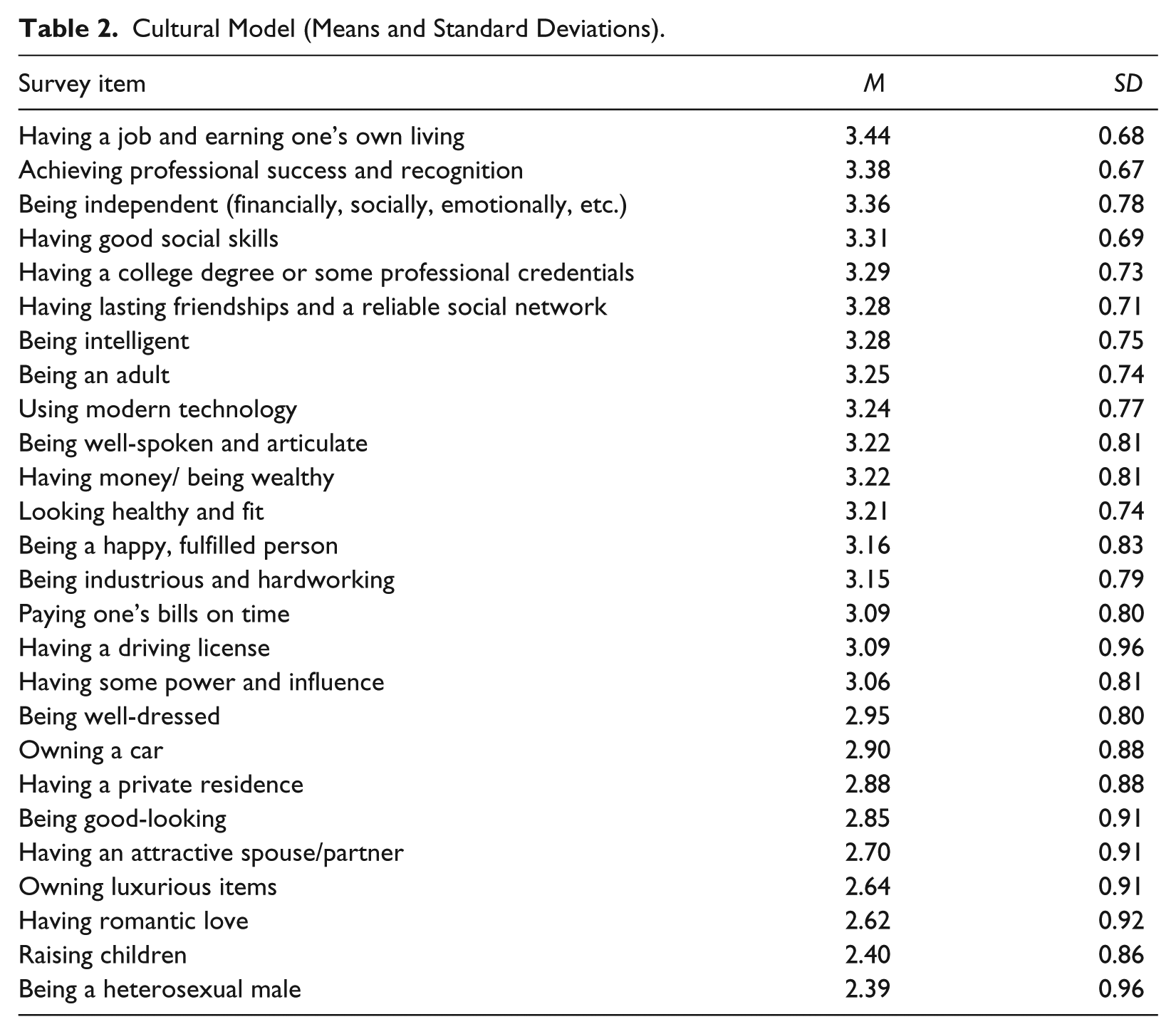
The data from free-listing were analyzed for patterns as described in Jehn and Doucet (1996); the items with the highest frequencies and order of recall were retained. The results were used to generate items for two sections of the survey. First, they furnished the original categories for the cultural model (26 items) that asked an informant to evaluate whether he or she deemed each item to be important to most Americans he or she knew to be viewed seriously by the fellow Americans. The informants were asked to rate the items in this section on the scale from 1 to 4 (1 being absolutely inaccurate and 4 being absolutely accurate). The informants were instructed to select one answer option only. These were measures of individual knowledge about the cultural model and a perceived collective standard of the desirable in American society that individuals consult to assess their situation relative to others. It was also done under the logical assumption that the American university is part of American society, and as such, this is a social institution that prepares students and offers them guidance for efficient functioning in society as part of its working agenda. In fact, intersubjective values consensus is at the heart of cultural identity (Wan et al., 2007; Wan, Torelli, & Chiu, 2010), informing our understanding of institutions’ and other collective entities’ values priorities, and as such, it would provide a meaningful underlying foundation shared by any variant of local cultural models circulating in the United States. Group members typically agree on assumed sharedness of the importance of some attribute within the group (Chiu et al., 2010, p. 483). Accordingly, individuals can be asked to estimate the degree to which an idea is intersubjectively important (i.e., culturally valued) in a group, and this information can be processed to obtain direct quantitative markers of sharedness (e.g., high means and low standard deviations) and to make further estimates of the content of what is shared (Wan et al., 2007; Weller, 2007). Therefore, accessing information regarding standards perceived as shared by other Americans is a reasonable starting step to begin exploring the local modification of the broader cultural model. Several formulations were reworded to be less ambiguous or more neutrally valenced to fit college culture and its discourses, but the core contents of the section dealing with the cultural model was unchanged as in Maltseva (2015).
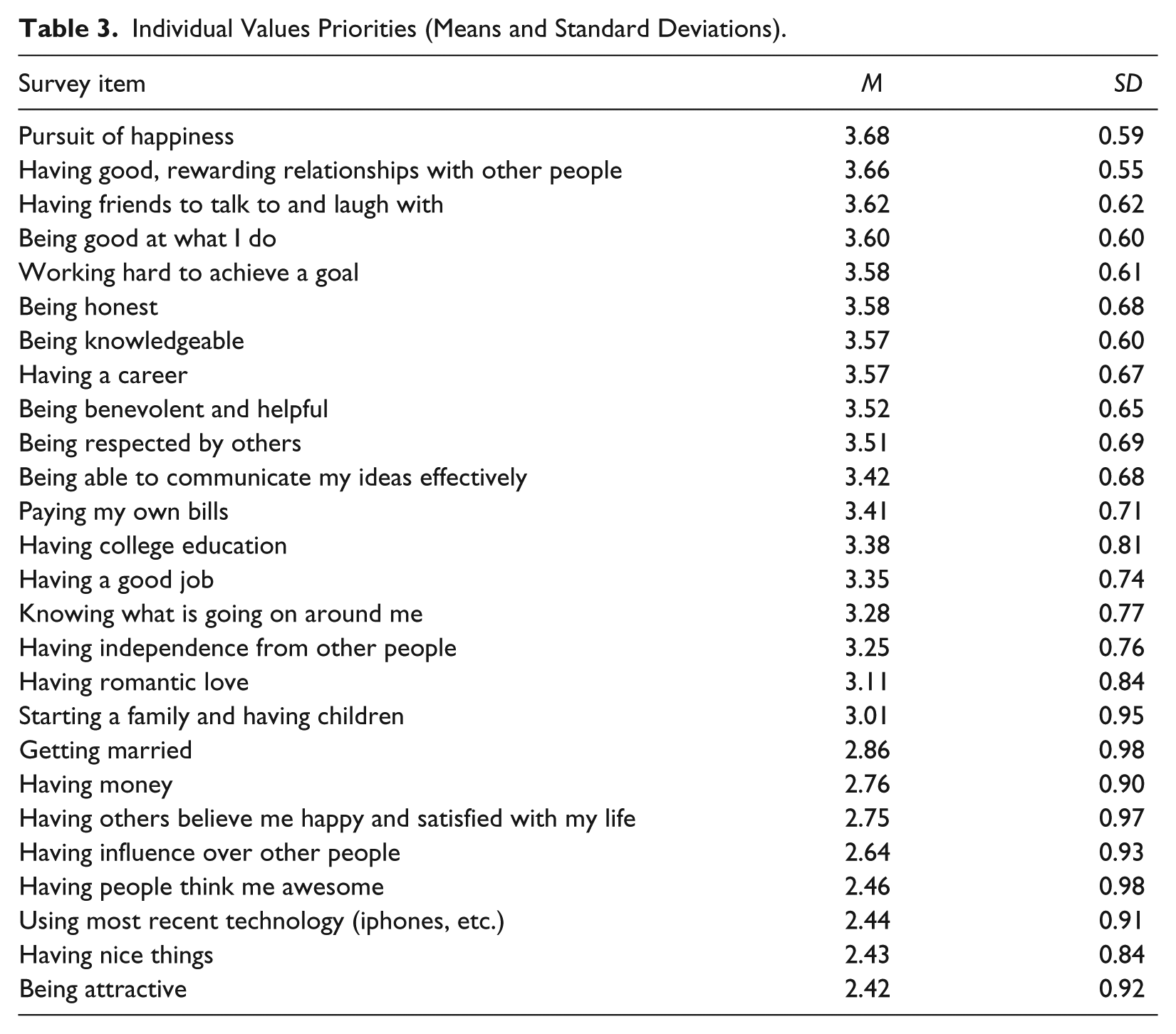
Second, based on these cultural model items and drawing on the author’s previous work on individual values (Maltseva, 2014a), 26 similar items for individual values priorities were formulated; these items probed about essentially the same things but predicated them as important to the informant personally (“In your view, how important is each of these things to be considered leading a good, worthy life?”) and appeared in a different order. The informants were asked to rate the items on the scale from 1 to 4 (1 = not at all important, 2 = somewhat important, 3 = quite important, 4 = very important). The informants were instructed to select one answer option only. These explicit measures of personal values priorities were taken for construct validity purposes as intersubjective perceptions of cultural values characteristics can be dissociated from (and not identical to) aggregated individual-level characteristics (Fischer, 2009; Shteynberg, Gelfand, & Kim, 2009); they did not participate in the main analysis. Individual values measures were included to further demonstrate that (a) internalization and internalized values informing the cultural model is not the same as individual values profile, and (b) the extracted cultural model indeed represents a collective knowledge rather than being an instance of aggregated individual preferences. 6 The lists of both classes of items and descriptive statistics for them are presented in Tables 2 and 3.
Cultural Model (Means and Standard Deviations).
Individual Values Priorities (Means and Standard Deviations).
Internalization item
If an idea is internalized, any infractions against it by definition would cause negative psychological consequences such as experiencing fear, shame, guilt, or loss of self-esteem (cf. Spiro, 1997). One of the ways to assess the inter-personal variation in internalization of the item would be by measuring to what extent the informant’s transgressing this particular prescription/standard would elicit similar negative feelings in each surveyed individual. Therefore, in the questionnaire, internalization was operationalized as the self-reported degree of anticipated emotional discomfort the informant associated with not matching the requisites of the cultural model. As all individuals are able to internalize ideas but vary in the degree to which they are prone to internalize, Likert-type scales from 1 to 4 were used to measure internalization for each individual informant. To ensure that the internalization item measured internalization with reference to the entire cultural model as a coherent, integral entity, the phrasing stressed the entire set of 26 items rather than focus on each of them individually. The following format was used:

While conventional measurement wisdom speaks in favor of using multi-item scales as they can produce an explicit test of reliability, scales are not the only way to go about measuring research constructs and certainly not under any circumstances. Single-item measures can have acceptable psychometric properties and are, therefore, a potentially viable alternative to multi-item scales for construct measurement purposes (e.g., Bergkvist & Rossiter, 2007; Drolet & Morrison, 2001), and their appropriateness for a particular piece of research should be evaluated (Wanous, Reichers, & Hudy, 1997, pp. 250-251). Single-item measures are useful when the construct is unambiguous (Wanous et al., 1997) or when a holistic impression is informative (Youngblut & Casper, 1993), which is the case for internalization (Chiu et al., 2010).
Lifestyle items
Standard demographic information (24 items, including lifestyle items) was collected at the end of the survey (Table 1). The questionnaire items included 11 lifestyle items that were specifically measuring whether the informant engaged in activities or owned items described in the cultural model adjusted for student lifestyle at UConn. For example, the informants were asked whether they owned a cell phone, a car, a laptop, had a credit card they could use, used Internet, paid their own bills, had a Facebook account, and so on. Descriptive statistics for lifestyle items are presented in Table 1.
Mental health scales
The instrument included measures of both positive and negative mental health. The Flourishing Scale (Diener et al., 2010, eight items) and the BDI-I (Beck et al., 1961, 21 items) were used. These scales were chosen due to their previously documented validity and excellent performance in the relevant domain with U.S. students. BDI was chosen as this scale was previously used by W. Dressler. BDI items were scored from 0 to 3 and later computed as an index. Both psychological scales had internal consistency levels comparable with those of other published studies: BDI (α = .90) and Flourishing Scale (α = .86).
Results
Following data cleaning, and reliability and factorial invariance checking for scales, the first step in the analysis was to estimate the degree of inter-informant consensus on the cultural model to demonstrate its collectively shared nature. Consensus analysis is typically used to estimate the degree of sharing of a cultural trait (Romney, 1999). One of the suitable procedures to measure inter-informant consensus on a set of items involves using factor analysis or principal components analysis performed on individuals (q-analysis) and analyzing the factorial structure of the first factor (first principal component in principal components analysis) by computing the average of the factor loadings on the first factor (Weller, 2007). Given that in q-analysis, individual factor loadings represent each informant’s correlation with the latent variable (i.e., the first principal component), and higher averages are created by the prevalence of high positive factor loadings, higher average score is an index of higher inter-informant agreement and, thus, would be indicative of its shared consensual nature of the set of attributes (Weller, 2007, pp. 338-340). Therefore, principal components analysis was performed, and the first principal component was analyzed to estimate the degree of sharing due to culture as discussed in Weller (2007).
The extraction of cultural model was followed by the analysis using linear regression to assess the cultural consonance following procedures used in Dressler’s research on cultural consonance (Reyes-Garcia et al., 2010). Measures of depression and flourishing were regressed on measures of individual’s correspondence to the culturally desirable lifestyle (correspondence to lifestyle index [CLS]; measure of cultural consonance, Reyes-Garcia et al., 2010), knowledge of cultural model, and the degree of internalization. To do this, standardized indices corresponding to lifestyle (CLS), depression, and flourishing were first computed (Reyes-Garcia et al., 2010, pp. 192-194). The measure of individual knowledge of cultural model (measure of cultural competence) participated in the analysis in the form of the individual factor loadings on the first principal component obtained in principal components analysis of individuals (q-analysis) run on standardized data.
Extraction and Description of the Cultural Model
The basic premise of culture consensus theory is that cultural sharing is manifested in the presence of consensus among the enculturated individuals who vary in their knowledge (reflecting their degree of cultural competence). Culture consensus theory builds on these basic analytic approaches. First, estimates of individual knowledge or competency can be estimated from the agreement between people. Then, the culturally correct answers are obtained by weighting the responses of each person by their competency and aggregating responses across people. (Weller, 2007, pp. 340)
Based on that, group beliefs can be estimated from responses to a series of related questions. The simplest way is to aggregate responses and use the average responses . . . (for quantitative responses) to estimate the answers. Agreement between the responses of individuals and the aggregate responses of the group can be used to estimate how well each individual corresponds to the group. (Weller, 2007, p. 339)
Assuming that in the factor analysis of individuals (q-analysis), each individual’s factor loading is a correlation with the extracted latent variable, then “the respondents’ factor loadings correspond to their correspondence with the shared group beliefs” (Weller, 2007, p. 347) and represent “the estimated individual competence values” (Weller, 2007, p. 356). It allows estimating inter-informant consensus and the proportion of cultural sharing.
The estimate of sharing due to culture based on inter-informant consensus was .53, suggesting high degree of sharing due to the cultural model (Weller, 2007, pp. 339-343). 7 Judged by the eigenvalues’ magnitude for the first three principal components (42.3, 22.2, and 14.1), and the number of components with eigenvalues greater than one, one can conclude that the data capture a shared mental model of high cohesiveness (Cattell, 1966; Nunnally, 1978). Means and standard deviations for the cultural model and individual values priority items are presented in Tables 2 and 3. These results show that the extracted beliefs were (a) distinct from individual values preferences (as demonstrated by different top items for cultural model items and individual values preferences), and (b) shared and highly consensual (collective portion has a smaller range of SDs than individual preferences) and indeed represented a cultural model. As most of the participants were college students, the extracted cultural model relies on their prevalent perceptions and represents a vision of life as perceived by a young person in the beginning of their career. Highly consensual ratings of the domain also reflect the high salience of the domain of a good, worthy life for the participants.
Mental Health and Lifestyle Correspondence: Regressions
The next step was testing the prepositions expressed in the exploratory hypotheses. Ordinary least squares regression analysis was performed on individuals who had information about internalization measure (N = 301). Mean scores and intercorrelations of all measures discussed further are shown in Tables 4 and 5.
Means and Standard Deviations for the Main Measures (N = 306).
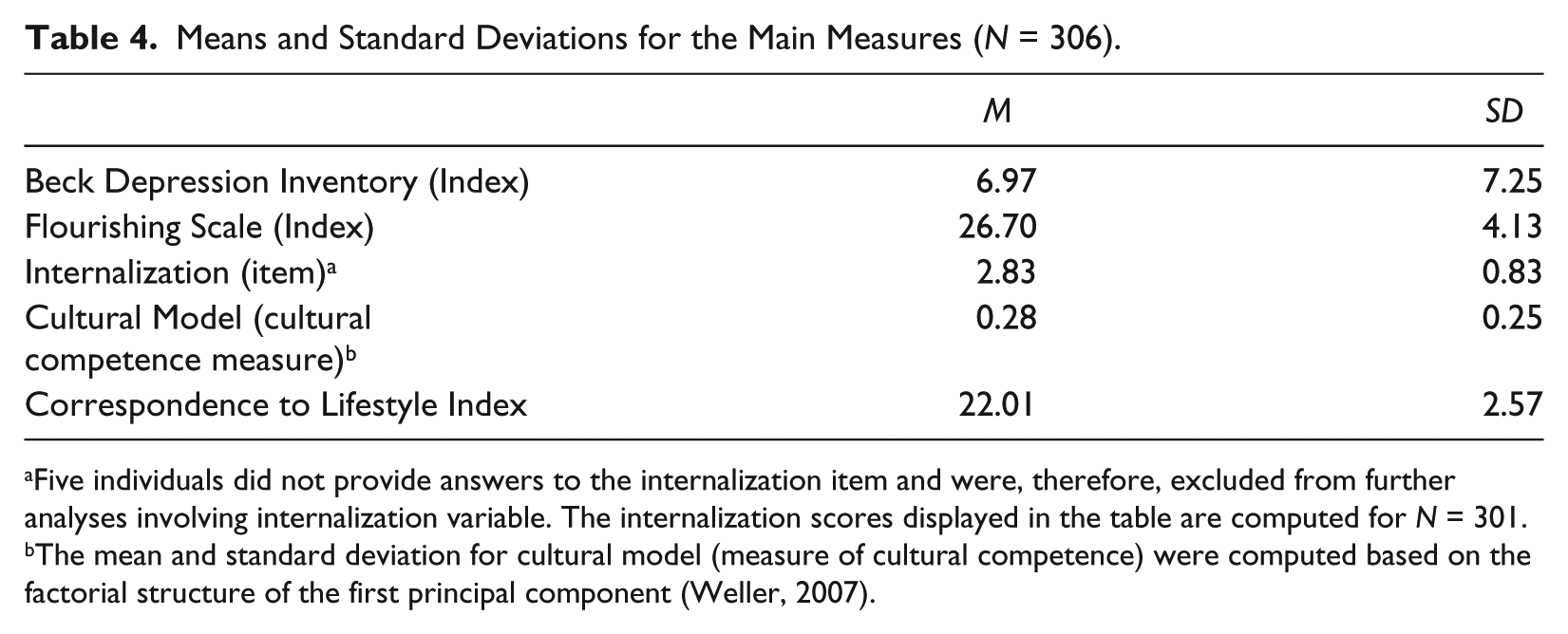
Five individuals did not provide answers to the internalization item and were, therefore, excluded from further analyses involving internalization variable. The internalization scores displayed in the table are computed for N = 301.
The mean and standard deviation for cultural model (measure of cultural competence) were computed based on the factorial structure of the first principal component (Weller, 2007).
Summary of Intercorrelations of the Main Measures.
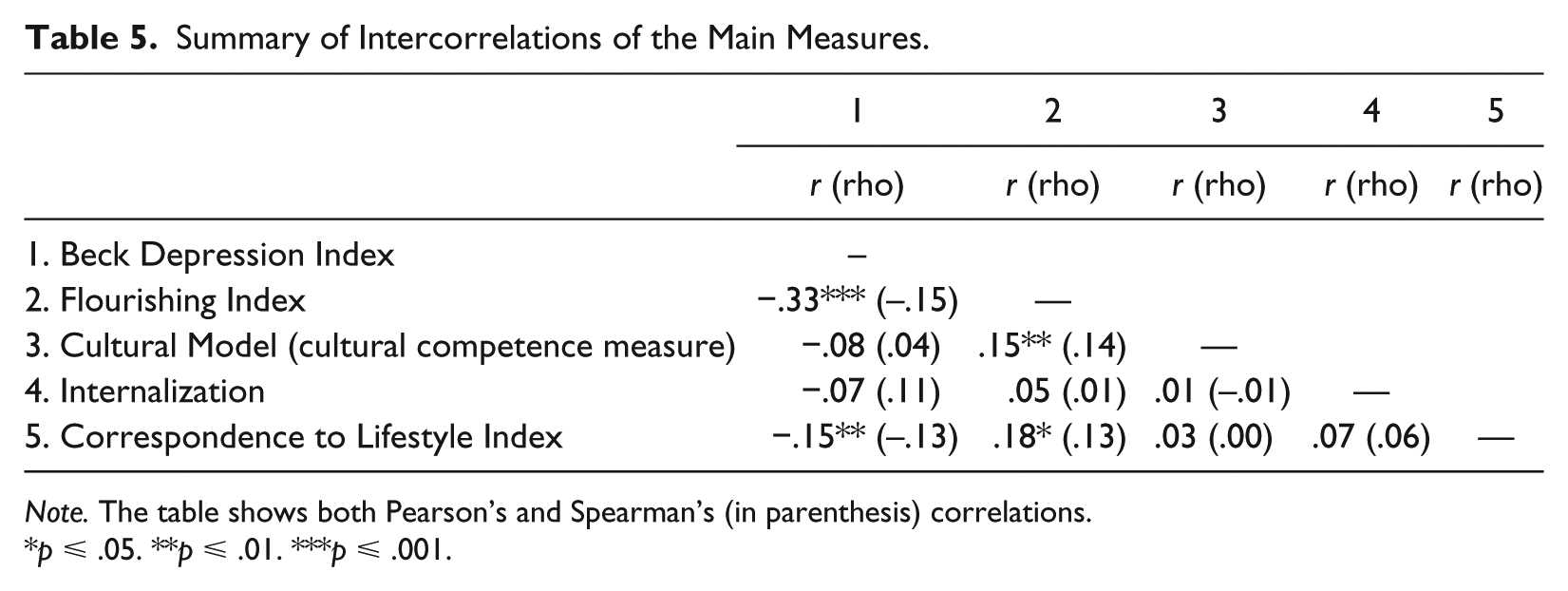
Note. The table shows both Pearson’s and Spearman’s (in parenthesis) correlations.
p ⩽ .05. **p ⩽ .01. ***p ⩽ .001.
When internalization was included in Model 1, this variable was not significant (Table 6, Model 1). The strongest predictor of mental health measures of either type was correspondence with lifestyle (CLS; for example, high congruence with lifestyle was positively related to flourishing and inversely to symptoms of depression measured by BDI-I). This result supports Hypothesis 2 and is consistent with the literature on cultural consonance, thus furnishing further support for their conclusions. Cultural competence (first factor on Cultural Model measure) had a small positive effect on flourishing but not on depression.
Regression (N = 301): Beck Depression Index and Flourishing Index.
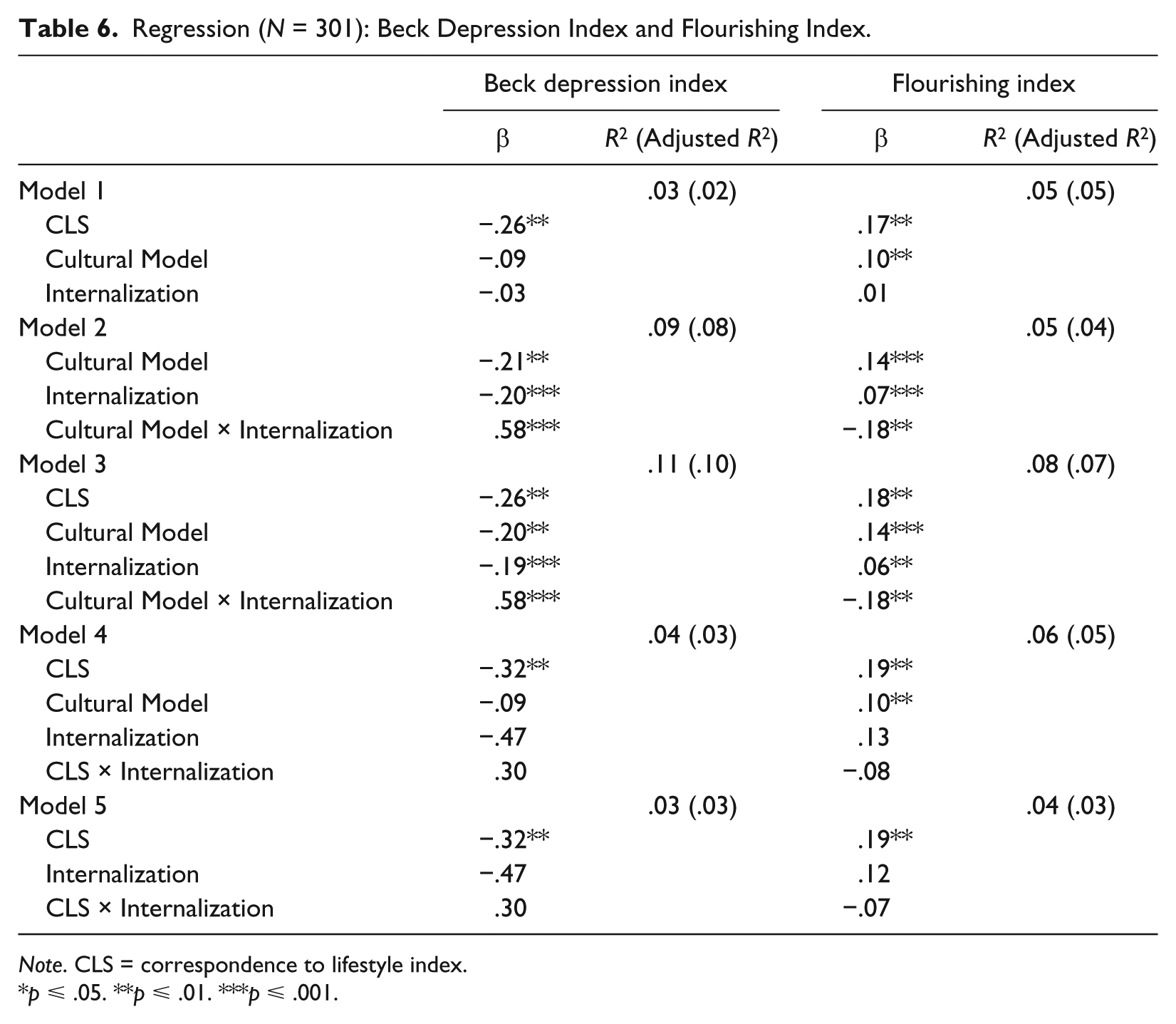
Note. CLS = correspondence to lifestyle index.
p ⩽ .05. **p ⩽ .01. ***p ⩽ .001.
Introduction of the interaction terms into the model has brought some interesting observations into light suggesting refinements to conceptualizations used in Hypothesis 1. When the interaction term Internalization × Cultural Model was introduced into the equation, the situation somewhat changed (Models 2 and 3). While higher correspondence to culturally valued lifestyle remained the most stable predictor of depression, cultural competence became a much stronger predictor of both flourishing and depression symptoms than in the original model, and internalization also gained potency as a predictor (demonstrating positive relationship with flourishing and negative relationship with depression; Models 2 and 3). The significance and magnitude of the lifestyle congruence as a predictor increased less dramatically for both types of mental health measures (Models 3-5). The knowledge of the cultural model (Cultural Model measure, first factor) and internalization contributed to lower scores on depression and higher scores on flourishing when they were considered separately, but taken in their interactions, they had the opposite effect (Models 1-3). In this form, both one’s knowledge of the cultural model and correspondence to culturally desirable lifestyle are linked to higher flourishing and lower depression scores. These results support Hypotheses 2 and 3. Interaction effects of lifestyle correspondence with internalization (Models 4 and 5) enhanced the effect of lifestyle congruence on depression scores on the BDI-I compared with the original model; its effect on flourishing was comparably less pronounced. These results are consistent with earlier studies conducted in Sweden and the United States (Maltseva, 2014b, 2015).
Discussion
General findings point to the link between the individual capacity for internalization, cultural competence, and emotional health, although the relationship is a complex one. Consistent with Dressler’s cultural consonance theory, matching the culturally desirable lifestyle was found to be the strongest predictor of both positive and negative mental health, decreasing depressive symptoms and increasing flourishing. Cultural competence (individual’s familiarity with the cultural model) was shown to be implicated in the process of cultural consonance; it was the second strongest predictor of mental health outcomes. The degree of cultural competence was favorably associated with flourishing but was not associated with the depressive symptoms (unless treated in interaction with the internalization variable). While cultural competence appears to predict either aspect of emotional health to a comparable degree, the results further suggest that lifestyle congruence and degree of internalization weigh much more for depression than for flourishing variables. This result echoes Dressler’s principal finding regarding the association between lifestyle dissonance and depressive symptomatology. It also nuances the observation that while high level of cultural competence makes a relatively meager contribution to individual SWB, it can effectively buffer against negative mental habits (measured by the Dysfunctional Attitudes Scale [DAS]; Floyd, Scogin, & Chaplin, 2004), by comparison (Maltseva, 2015). These results support the major premise of cultural consonance model and extend its reach to include more psychological information in our understanding of cultural consonance. Current findings also suggest that it would be beneficial to distinguish between mental and material aspects of consonance.
Limitations and Future Directions
Cultural ideas, mental habits, and practices operate at multiple levels (Matsumoto & Van de Vijver, 2010). At the collective level, culture exists in the form of observable public representations that are accessible to all members of the cultural community and embodied in social institutions (“culture outside-the-head” as in Morling & Lamoreaux, 2008). The effects of this level of culture on mental health are typically studied by sociologists, social epidemiologists, and economists whose interests involve social aspects of mental health. Such studies employ corresponding distinct methodologies aimed at researching population-level parameters. At the other end of the spectrum is the individual level of culture, which mostly concerns psychologists and psychological anthropologists, who conceptualize culture in the form of internalized individual-level characteristics (Chiu et al., 2010), and it is the interactions of these elements of internal culture with psychological variables that are measured to explain the effects of culture on mental health. Although these levels of analysis are prevalent in cross-cultural psychology research and generate much useful data, both of them, as Chiu et al. (2010) astutely observe, tend to neglect the intermediate level of culture. This level, which Chiu et al. term intersubjective, represents an important aspect of culture that introduces a meaningful nuance to cultural processes, namely, how the members of a cultural group perceive the degree to which a certain cultural trait is consensual/desirable/prevalent (cf. Romney et al., 1986; Weller & Romney, 1988). The present study used this intersubjective approach to bridge the two levels of culture and to address internalization as one of the possible mechanisms by which one’s perceived correspondence to the intersubjectively understood collective preferences affect individual mental health status.
The present study provided the initial data to explore the contribution of internalization and cultural competence to the cultural consonance within a context of the college culture. Collecting data from a representative national sample targeting larger cultural groups would bring in a broader cultural context and, most probably, a more robust and nuanced understanding of the process involved in cultural consonance. Methodologically, one of the key issues for future research is to develop multiple measures of internalization and test their validity.
The study raises several questions that should be explored in greater depth in future research. Is the capacity to internalize cultural ideas beneficial for mental health of individuals and for the cohesion of human groups, from the evolutionary standpoint? Does the degree of the material approximation to the cultural standards affect the emotional well-being in culturally naïve individuals more or less than those with more cultural competence? Furthermore, it would be helpful to explore what other buffering factors exist for low cultural consonance, and how effective they are.
As raising well-being for a greater number of people is one of the goals of science and an objective beyond the scientific world (Veenhoven, 2010), the applied significance of this research has two aspects. The first resides in the attempt to isolate sociocultural factors that negatively affect mental health, increase stress levels, and decrease psychological well-being. Second, it offers important new insights into how human capacity to acquire normative culture and unequal individual abilities to realize cultural models interact to create mental health disparities, and hence contribute to differences in individuals’ well-being. It adds a new dimension to our understanding of biocultural synergies and the mechanism by which systematic cultural stressors are converted into measurable variation in health outcomes across societies or social groups.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.