
Abstract
The Opioid and Naloxone Education (ONE) Program expanded to correctional facilities in North Dakota to address the impact of opioid misuse among incarcerated individuals. This pilot aimed to evaluate the feasibility and outcomes of implementing comprehensive opioid risk screening, education, and harm reduction interventions in correctional settings. Among 168 individuals who were screened, 65.5% were at risk for opioid-related harm. Unsafe medication storage and disposal were common, and 13% reported diversion behaviors. Nearly 90% accepted naloxone, lockboxes, and disposal tools, demonstrating initial engagement with harm reduction modalities. Seventeen percent have previously received medication for opioid use disorder, and 19% expressed interest in initiating treatment. The findings of this pilot suggest implementing opioid risk screening and harm reduction education within correctional settings is feasible and associated with high engagement. The ONE Program may provide a structured approach to identifying risk and supporting linkage to harm reduction resources.
Introduction
Opioid misuse remains a major public health crisis in the United States, with vulnerable populations, including incarcerated individuals, being disproportionately affected. Data from the Bureau of Justice Statistics estimates that 63% of those incarcerated in local jails meet criteria for substance use disorders (Mital et al., 2020). Nationally, opioid overdose is the leading cause of death among individuals recently released from incarceration, with studies showing a 10-fold increase in overdose risk during the immediate post-release period compared to the general population (Hartung et al., 2023; Merrall et al., 2010). Correctional facilities frequently adopt an abstinence-only approach, and seldomly offer medications for opioid use disorder (MOUD) (Malta et al., 2019). The literature suggests a relationship between the history of incarceration and risk of opioid overdose, likely due to the period of abstinence while in custody followed by the lack of social and financial support faced upon reentry into the community (Mital et al., 2020). Data from the North Dakota Department of Corrections and Rehabilitation (DOCR) indicate incarcerated individuals in North Dakota have high rates of substance use disorder, mental illnesses, and limited access to continuous healthcare, factors known to increase the risk of misuse, diversion, and accidental overdose (Reports and Statistics, n.d).
Despite the well-documented need for harm reduction strategies in correctional facilities, access to opioid risk education, overdose prevention, and MOUD remains limited (Flanagan, 2023; Varsaneux et al., 2025). This gap in care not only exacerbates individual health risks but also contributes to broader public health concerns, including the spread of infectious diseases (The Global State of Harm Reduction in Prisons|Journal of Correctional Health Care, 2025; Varsaneux et al., 2025). Harm reduction strategies are vital to mitigate the risk of opioid misuse immediately after release, decrease opioid-related overdose and mortality, and improve retention in opioid use disorder treatment. Literature suggests implementing harm reduction prevention services within correctional facilities such as expansion of overdose education and naloxone programs, establishment of comprehensive medication assisted treatment programs as standard of care, development of corrections-specific overdose risk assessment tools, and increased collaboration between corrections entities and community-based organizations in attempt to reduce opioid misuse risks (Brinkley-Rubinstein et al., 2017).
The Opioid and Naloxone Education (ONE) Program was originally developed to implement comprehensive opioid risk screening, education, and prevention interventions in a community pharmacy setting across North Dakota (Landing Page, n d). People receiving an opioid prescription are screened for opioid misuse and overdose risk. Based on risk level, individual-centered interventions are provided including naloxone distribution and educational resources (Skoy et al., 2020, 2022; Strand et al., 2020; Strand & Eukel, 2019; Webster & Webster, 2005). With over 33,000 people receiving and opioid prescription screened across North Dakota, the ONE Program has expanded its (Eukel et al., 2025; Eukel et al., 2023). Building on this success, the program expanded in 2023 to implement a pilot program currently operating in four correctional facilities across North Dakota, further extending its reach and impact.
The success of this pilot has prompted efforts to expand the program’s reach beyond the initial four pilot sites. Through the creation and dissemination of infographics and other educational materials, the ONE Program team is engaging correctional, legislative, and healthcare partners to promote awareness and secure buy-in for statewide implementation. This manuscript outlines the development, implementation, and early outcomes of the ONE Program pilot in 4 correctional facilities, while highlighting the collaborative partnerships, interprofessional engagement, and informational outreach that are key to its growth. By focusing on this vulnerable population, the initiative serves as a model for integrating opioid harm reduction into correctional healthcare and advancing public health in North Dakota and beyond.
Methods
Pilot correctional facility sites were identified through ONE Program team contacts and existing relationships with local public health units across the state. A corrections nurse or officer at each correctional facility served as champion of the program’s implementation and communicated with jail administration. Each site’s logistics for performing and documenting screenings and providing education, naloxone, and medication safety kit materials to incarcerated individuals were discussed with the ONE Program team and coordinated amongst local public health unit and jail staff.
Nurses and correctional officers at each of the pilot sites completed a 50-min ONE Program-developed training delivered online asynchronously. This brief training was designed to equip staff with the skills and knowledge necessary to conduct screenings, identify common risk factors for opioid-related harm, and deliver targeted education to individuals based on screening outcomes. A robust website was created to house FAQs, training materials, and resources for staff. Additional information, and Q and A sessions for staff were offered to each site upon request. Feasibility of the pilot would be demonstrated if each of the 4 pilot sites conducted at least 10 screenings.
This pilot used standardized screening tools developed by the ONE Program to assess individuals during routine health assessments (Appendix 1). The risk stratification screening tool incorporating the Opioid Risk Tool (ORT), a validated tool to measure opioid misuse risk, and an assessment of overdose risk based on clinical guidelines (Webster & Webster, 2005). An additional six questions were added to the screening specific for this population including brief questions about typical medication storage practices, medication adherence, history of medication diversion and desire to start or continue MOUD. Nurses or correctional officers evaluated incarcerated individuals using a medication safety questionnaire and corresponding outcomes worksheet as key tools for data collection on resident medication safety practices, opioid risk harm, and interventions offered. Each screening assessed medication storage and disposal, adherence to prescribed regimens, past behaviors related to drug diversion, use of pain medications (opioid and non-opioid), risk for opioid misuse, risk for accidental overdose, and current or prior engagement with MOUD treatment. Risk for opioid misuse is based on the ORT, which provides a numeric risk evaluation. Incarcerated individuals were deemed to be at high risk for opioid misuse score with an ORT >7, consistent with published literature (Webster & Webster, 2005).
Following each screening, the program specified that individuals should receive education tailored to their needs, covering topics such as medication adherence, diversion prevention, proper medication storage and disposal methods, and opioid risk reduction strategies. As a critical part of the program’s harm reduction approach, each person screened is offered a medication safety kit (Figure 1). Kits are offered at the time of screening and education, distributed at the time of release, and include two doses of nasal naloxone, a daily medication organizer, a locking medication bag, Deterra® pouches for safe medication disposal, and educational brochures about opioid use disorder (OUD) and overdose prevention. If the incarcerated individual agrees to accept the kit, it is placed in their personal belongings locker and distributed at the time of release. The approximate cost of each kit is $50 and was supported by grant funds through the North Dakota Department of Health and Human Services with no cost forwarded on to the resident or correctional facility. Discharge kit components
All screenings and intervention outcomes were documented and collected from February 2, 2023 through January 1, 2025 in REDCap, a secure, web-based application designed to support data capture for research studies (Harris et al., 2009). De-identified information from REDCap was collected in one secure Excel spreadsheet containing data from the screenings of 168 incarcerated individuals. Review of data resulted in removal of 0 cases due to incomplete data. The final sample size was 168. Excel was used for descriptive data analysis of the final data set. The evaluation of this program was approved by an IRB. This pilot study was funded through North Dakota State Opioid Response (SOR) funds.
Results
Demographics
Facility, Medication Safety, and Opioid Risk Screening Results (n = 168)
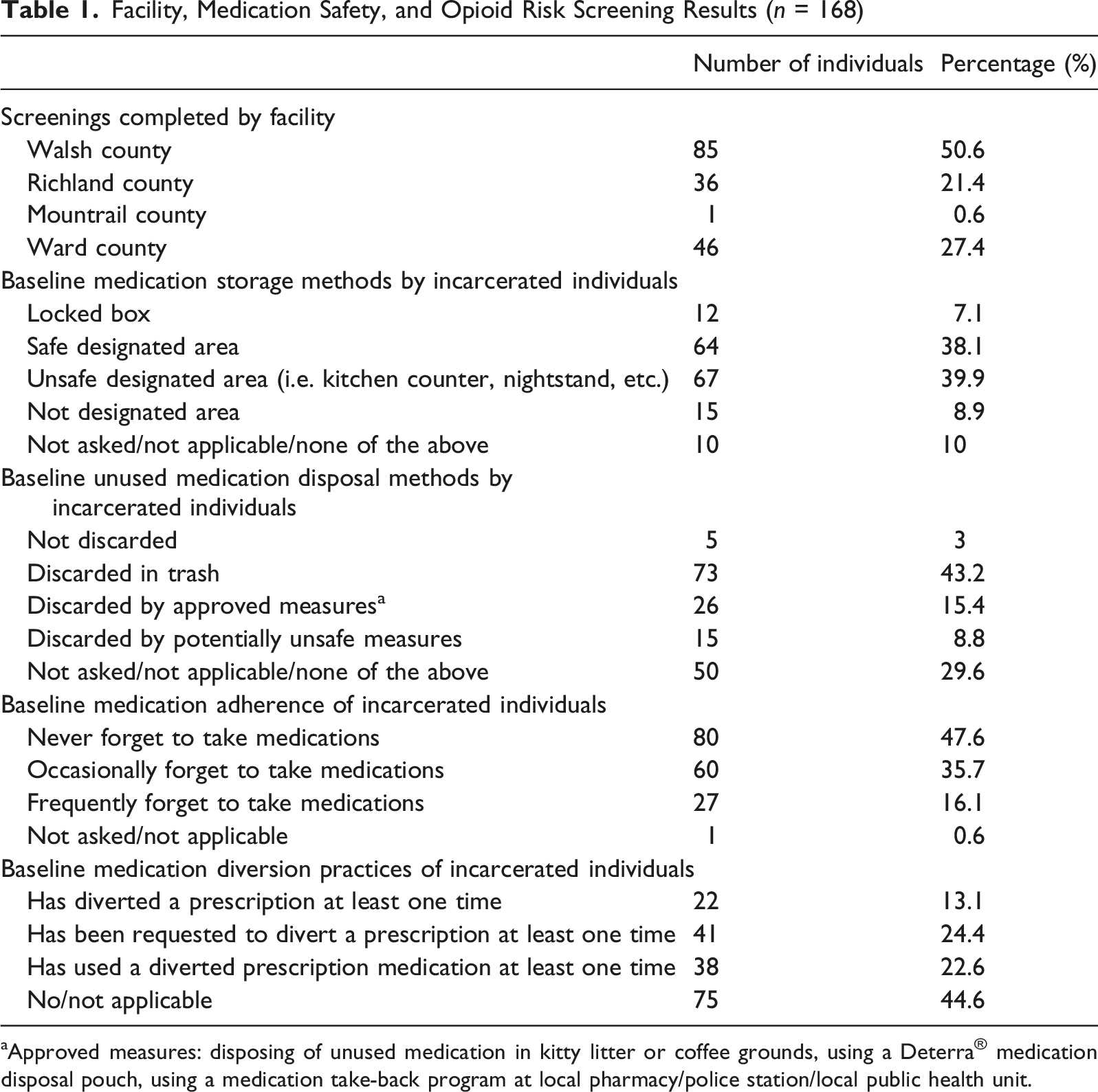
aApproved measures: disposing of unused medication in kitty litter or coffee grounds, using a Deterra® medication disposal pouch, using a medication take-back program at local pharmacy/police station/local public health unit.
Pilot locations across north Dakota
Medication Safety Behaviors
Of the 168 screenings conducted, 58% of this population are storing their medications in an undesignated or unsafe area, such as on the countertop, on a nightstand, or within reach of children or pets. Over 80% are not disposing of their medications safely, which may include flushing down the toilet or throwing in the garbage. More than 50% have forgotten to take their medication (Table 1). A total of 13% have diverted at least one prescription medication, over 20% have been requested to divert a prescription, and over 22% have taken a diverted prescription medication at least once (Table 1).
Opioid Misuse Risk and MOUD
Opioid Overdose, Misuse, and Intervention Results for Incarcerated Individuals (n = 168)

aAs assessed by the ONE Program Opioid Misuse and Overdose Risk Screening Tool (Appendix 1).
Interventions
Education for storage, disposal, adherence, and diversion was provided to almost every resident (93.5%). Medication lock boxes, Deterra® pouches, and naloxone were offered to each resident and accepted by and provided to over 80% of incarcerated individuals at release.
Discussion
This study included 168 incarcerated individuals. This does not represent the entirety of incarcerated individuals during the data collection period at these sites. Participation in the study was voluntary for the incarcerated individuals, and not all agreed to receive the screening and/or have their results shared with the researchers. This study demonstrates a significant need for structured medication safety and opioid misuse prevention efforts within correctional facilities.
The majority of participants who exhibited any risk for developing opioid use disorder were deemed to be at high risk for opioid misuse (65.5%) via the ORT portion of the screening, which is notably higher than the general population. In the general population, of the patients receiving opioid prescriptions who were screened, 3.9% screened at high risk for opioid misuse using the same screening tool (Strand et al., 2022). Data collected from this population regarding incarcerated individuals’ previous use of and preference for availability of MOUD were shared in aggregate to state and local public health entities in order to better inform future directions in correctional health in the state and support the addition of another layer of assistance for those managing opioid dependence.
Despite the identified risks among the incarcerated population, the program saw overwhelming acceptance of education and physical resources by incarcerated individuals. Nearly 90% of participants accepted naloxone, lockboxes, and Deterra® pouches, demonstrating high engagement with preventive strategies. Moreover, over 87% of those already prescribed OUD treatment wished to continue it during incarceration, and nearly 1 in 5 expressed their interest in initiating treatment. A distinctive feature of the program is its commitment to equity. All incarcerated individuals, regardless of their assessed risk level, were offered medication safety kits upon release, requiring only 5 min of time from correctional staff per resident. This universal access ensures that everyone benefits from harm reduction resources, supporting safer reentry into the community. The combination of education, screening, and tangible medication safety tools represents a proactive public health approach that strengthens both individual care and broader community safety. The high rates of unsafe medication practices, diversion, and opioid misuse risk among this population reinforce the need for proactive, system-level interventions.
Feasibility, shown by conducting at least 10 screenings per site, was demonstrated in all but one of the correctional facilities. The facility that conducted just one screening experienced loss of its single correctional nurse shortly after program initiation and that staff position was not replaced. This highlights a prominent limitation of this study in general— correctional health workforce and corrections workforce was an often-presented concern in discussions about program implementation, especially with jail administrators. Emphasis on the short time requirement for resident screening and intervention as well as fitting the screening into already-occurring booking paperwork or health assessment practices was important to the successful implementation at the other 3 sites.
This study included 168 incarcerated individuals. This does not represent the entirety of incarcerated individuals during the data collection period at these sites. Participation in the study was voluntary, and not all agreed to receive the screening and/or have their results shared with the researchers. The researchers have no way of knowing the percent of total incarcerated individuals as this was not collected as a data point due to IRB restrictions. This pilot study was completed in jails only, not prisons, and the findings may not be generalizable to all correctional settings.
Additional limitations of this study included a lack of examination of long-term health or opioid-harm related outcomes among the screened incarcerated individuals. We also did not collect data related to overdoses or future recidivism, nor about stigma or other barriers to successful public health outcomes. These areas deserve exploration in future studies. These findings suggest that correctional settings represent a critical point of intervention to reduce opioid-related harm. By equipping incarcerated individuals with education, tools, and access to OUD treatment, facilities can mitigate future opioid misuse and overdose risk both during incarceration and post-release.
Conclusion
This pilot implementation of the ONE Program within North Dakota identified the value of medication safety within correctional facilities as this population displays higher risks of opioid misuse. The high acceptance rate of medication safety kits and educational materials highlights the importance of readily available resources as incarcerated individuals may not have access to them after being released as well as these individuals being receptive to medication safety interventions. Of equal importance, incarcerated individuals were interested in receiving medication to treat OUD when provided with access and support. These findings support broader implementation of such programs across correctional systems. Future efforts should explore integration of ongoing OUD treatment options and follow-up after release to ensure continuity of care. Longitudinal studies can further evaluate the impact of these interventions on health outcomes and recidivism.
Supplemental Material
Supplemental material - Correctional Facility Opioid Harm Reduction: A Medication Safety and Opioid Risk Screening Program Pilot
Supplemental material for Correctional Facility Opioid Harm Reduction: A Medication Safety and Opioid Risk Screening Program Pilot by Alyssa Hodges, Heidi N. Eukel, Amy Werremeyer in Journal of Drug Issues
Footnotes
Acknowledgements
The authors acknowledge the local public health units and correctional facilities who wilfully and passionately implemented the program. Additionally, the authors acknowledge all members of the ONE Program team for their contributions and support of the program: Elizabeth Skoy, PharmD; Mark Strand, PhD; Jayme Steig, PharmD; Oliver Frenzel, PharmD; Lisa Nagel, PharmD.
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the North Dakota State University Institutional Review Board (#IRB0004741).
Consent to Participate
Participants involved in this research verbally consented to participate in compliance with the project IRB protocol.
Author Contributions
All authors contributed to the study conception, design, material preparation, data collection and analysis, and manuscript writing. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support for project implementation was provided by North Department of Health and Human Services. Financial support was not provided for writing of the report or decision to submit the article for publication. North Dakota Department of Health and Human Services; State Opioid Response Grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Data is not available for downloadable distribution due to IRB limitations.
Data Availability Statement
Data for download is not available due to IRB constraints.
Supplemental Material
Supplemental material is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.