
Abstract
Health education is seen as highly difficult and challenging, due to the high level of stress observed in students. The precise assessment of perceived stress becomes important for understanding the students’ profile as well as their nutritional habits during the university period. The aim of the analysis described in this article is to assess the associations between mental health, self-reported symptoms/health complaints, and nutritional habits in health students. Our findings suggest using it in other contexts such as public universities and other university courses to assess students’ mental health status and food intake
Introduction
Stress is a growing epidemic of mental health disorders around the world. This covers several populations of different age groups. It can interfere in work relationships/productivity, family relationships, and so on, as it presents itself as physical, behavioral, and psychiatric manifestations (Vidal et al., 2018). Stress is defined as “a complex physiological state that embodies a range of integrative physiological and behavioral processes that occur when there is a real or perceived threat to homeostasis” (Tilbrook, 2007). Upon entering college or university in search of fulfillment and personal satisfaction, academics go through a transition from adolescence to adulthood in the search for a professional future (Abdollahi et al., 2018; Ansari et al., 2014; Vidal et al., 2018), which can be a stressful event for many young people (Vidal et al., 2018). The impact of stress on learning is particularly significant in the context of professional education because it can disturb the capacity to absorb information (Jacob & Einstein, 2016; Walsh et al., 2010). In this way, health students and physiotherapy students may experience high levels of stress (Deasy et al., 2014; Jacob & Einstein, 2016; Walsh et al., 2010).
Health education is seen as highly difficult and challenging, due to the high level of stress observed in students. Factors such as academic pressure, workload, and reduced sleep time are considered the main causes of stress in students (Abdollahi et al., 2018; Stock et al., 2003; Vidal et al., 2018; Walsh et al., 2010). University students generally report a wide range of symptoms and health complaints that can be broadly characterized into (a) psychological health complaints, (b) circulatory and breathing symptoms, (c) gastrointestinal symptoms, and (d) pains and aches (Ansari et al., 2014). The psychological health complaints are related to headache, nervousness, depression, sleep disturbance, and dizziness (Ansari et al., 2014; Stock et al., 2003); the circulatory and breathing symptoms are related to rapid heartbeats/circulatory problem (Ansari et al., 2014); the gastrointestinal symptoms are related to diarrhea and constipation (Ansari et al., 2014; Stock et al., 2003); and pains and aches are related to neck ache/backache (Ansari et al., 2014; Stock et al., 2003).
Stress in physiotherapy students can contribute to reduce academic results, in addition to resulting in psychosomatic suffering, physical problems, and behavioral problems (Abdollahi et al., 2018; Deasy et al., 2014; Hodselmans et al., 2018; Memon et al., 2016; Walsh et al., 2010). This can lead to a failure in coping with stress on the part of the student and, as a consequence, this student may interrupt or not continue his studies or even have unhealthy attitudes such as smoking, drinking, behaving aggressively, or damaging property from the institution (Memon et al., 2016), as well as changes in nutritional standards (Ansari et al., 2014; Errisuriz et al., 2016; Vidal et al., 2018).
The health promotion behavior is directed toward ideal well-being, personal fulfillment, and productive life. Health students must be challenged to take responsibility for their personal health and well-being. During the period of college/university, there are significant changes in lifestyle, mainly related to diet, where students start to develop eating behaviors considered unhealthy, such as skipping meals, consuming large amounts of carbonated drinks, fast food, and high-fat foods, while consuming few fruits and vegetables (Errisuriz et al., 2016; Vidal et al., 2018). Thus, unhealthy health practices and behaviors during youth continue into adulthood, compromising health status (Errisuriz et al., 2016; Nualnetr & Thanawat, 2012). Individuals on the effects of stress change their food choice, consuming the foods they would normally avoid and who ate those foods to feel better (Mikolajczyk et al., 2009; Vidal et al., 2018). This pattern of disordered eating behavior is also observed in students with stress. High stress has been associated with a greater preference for sweet foods (e.g., sweets, ice cream), varied dishes (e.g., pizza, fast food), increased consumption of snack foods, and decreased consumption of foods such as fruits, vegetables, meat, and fish (Errisuriz et al., 2016; Mikolajczyk et al., 2009; Vidal et al., 2018).
Mental health disorders are important from the point of view of health promotion/disease prevention because of their links to risky behaviors and physical illnesses in higher education students (Deasy et al., 2014). In the literature, few studies have documented the relationship between self-reported health complaints/symptoms and the stress perceived by students during college graduation (Abdollahi et al., 2018; Ansari et al., 2014). Thus, there is a need to understand the relationship between nutritional habits and mental health (Ansari et al., 2014; Mikolajczyk et al., 2009). University students have several positive aspects associated with students, which make them very suitable for comparative investigations, in addition to being easily accessible and homogeneous in this population. Another reason for studying university students is the need to understand the state of health and morbidity to develop effective health education and health promotion policies, programs, and practices that target this group (Stock et al., 2003; Walsh et al., 2010). Among health promotion initiatives by World Health Organization, detailed knowledge of students’ health and its determinants is required (Stock et al., 2003).
Aim of the Study
The aims of the study were to (a) assess the association between predictors of perceived stress, 21 symptoms/health complaints, and perceived stress in students; (b) investigate the gender differences in predictors of perceived stress, 21 symptoms/health complaints, and perceived stress in students; and (c) assess the association between predictors of perceived stress and nutritional habits in students.
Method
Procedure and Participants
A total of 218 undergraduate students from three Brazilian physical therapy colleges participated in this study. Participants were provided with a verbal explanation of the investigation, including the aims and objectives, and were informed that they had the right to withdraw from the study at any point before the final data analysis was conducted. The study was conducted in accordance with the guidelines of the Declaration of Helsinki.
Measurement Instruments
Student health and well-being questionnaire
Stress symptoms measures: Perceived stress was measured with Cohen’s Perceived Stress Scale (PSS-10 items), which assesses the extent to which a respondent considers life situations to be stressful. The questions measure how unpredictable, uncontrollable, and overloaded respondents find their lives, using a 5-point Likert-type scale response format (0 = never; 4 = very often). Scores for individual participants were obtained by summing their responses to all 10 items. Employing the PSS scale in a population probability sample in the United States, Cohen and Williamson (1988) reported an internal reliability (Cronbach’s alpha) of .78. The scale’s predictive and discriminant validities were also established in studies that linked the measured concept of stress to health outcomes. In our sample, Cronbach’s alpha of the PSS was .87.
Health problems, strains, and psychosomatic symptoms (21 items): Participants rated 21 symptoms measuring a raft of health complaints as adopted from Stock et al. (2003, 2008). Sample items included stomach trouble/heartburn, back pain, rapid heartbeats/circulatory problem/dizziness, headaches, sleep disorder/insomnia, concentration difficulties, neck and shoulder pain, and depressive mood. Respondents rated the question: “How often have you had these complaints during the past 12 months?” (4-point response scale, 1 = never; 4 = very often). In the current study, Cronbach’s alpha of the whole scale (21 items) was .89.
Assessment of dietary intake (11 indicator variables): This measured their consumption of sweets, cakes/cookies, snacks and fast/canned food, fresh fruits, raw and cooked vegetables and salads, meat and fish, milk products, and cereals. The instrument was created to include food groups that are important when studying dietary habits, in line with other research studies. The introductory question, “How often do you eat the following foods?” asked participants about the frequency of their usual consumption of each food group separately (rated on a 5-point scale: several times a day, daily, several times a week, 1–4 times a month, and never). Both the face and content validity of the instrument were ascertained by grounding the questionnaire on literature review. In our sample, Cronbach’s alpha was .48.
Sociodemographic variables
Age (one item): “What is your age?” Participants reported their age in years.
Income sufficiency (subjective economic position) (one item): Participants rated how sufficient or insufficient they considered the amount of money they have at their disposal is (4-point scale: always sufficient, mostly sufficient, mostly insufficient, always insufficient), later collapsed into two groups (always/mostly sufficient, always/mostly insufficient).
Exercise practice: more than 150 min by week or less than 150 min by week.
Health and well-being variables
Lifestyle characteristics
Frequency of alcohol consumption (one item): “Over the past 3 months how often have you drunk alcohol, for example, beer?” (none, once a week or less, once a week, a few times each week, every day, a few times each day).
Health variables
Health awareness (one item): Students were asked about their general awareness (surveillance) of their health “To what extent do you keep an eye on your health?” (4-point response: 1 = not at all, and 4 = very much).
Quality of life
Quality of life (one item): “If you consider the quality of your life: How did things go for you in the last 4 weeks?” based on the quality of life measurement charts with 5 response categories (poor, fair, good, excellent). The variable was further re-coded into three new categories: poor/fair, good, and very good/excellent quality of life.
Visit a doctor: Students were asked how often they had visited a doctor in the past 6 months (yes or no).
Statistical Analysis
Descriptive statistics were used to present background and demographic data for each undergraduate year. Values given in the descriptive results are proportions, means, and SDs. The Kolmogorov–Smirnov test was carried out to assess data distribution, and all variables analyzed were normally distributed (p > .05). Differences between variables were examined using one-way analysis of variance. Associations between variables were examined using Pearson’s correlation at a univariate level and linear regression at a multivariate level. Internal consistency was assessed for all measures using Cronbach’s alpha and reported in the Method section. All statistical analyses were based on an alpha level of .05, unless otherwise stated, and were conducted using Statistical Package for the Social Sciences Version 22 (SPSS Inc., Chicago, IL, USA).
Results
The sample comprised 218 questionnaires (43 male and 175 female students). In sociodemographic variables, females were of a similar age with male counterparts. Financially, slightly more than half of the sample felt that their income was mostly or always insufficient. About 36% of the sample did not binge alcohol in the month preceding the health survey. Most women (60.6%) practice less than 150 min of physical activity per week. The health and well-being variables showed a significant differences in general health, where male were more likely to report excellent health compared with female. This was paralleled by slightly more females who reported that they kept a constant eye on their health. Most students reported seeing a doctor at least twice in the past 6 months (Table 1).
Demographic and Other Selected Characteristics of the Study Sample.
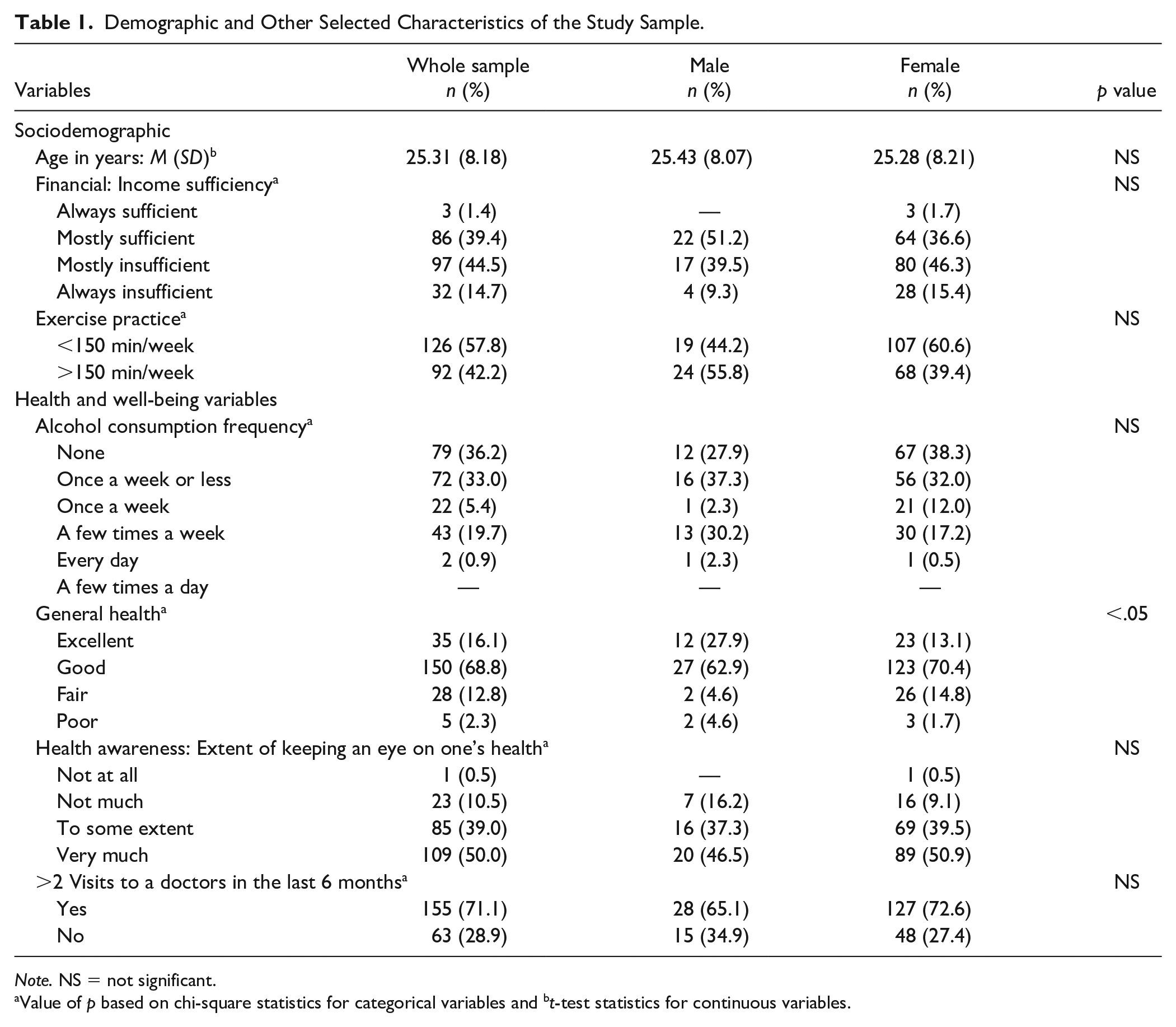
Note. NS = not significant.
Value of p based on chi-square statistics for categorical variables and bt-test statistics for continuous variables.
The association between symptoms/health complaints and symptoms of stress perception showed a positive and statistically significant relationship between the variables of the psychological, circulatory/breathing, gastrointestinal, and pains/aches group both in the total sample and by gender. However, men showed no association between stress symptoms and symptoms/health complaints for nightmares, weight gain/weight loss, diarrhea, and back pain. The comparison between symptoms/health complaints showed no difference between genders (Table 2). The association between food consumption and symptoms of perceived stress showed a statistically significant negative relationship (r = −.165, p < .05) with meat consumption among women. The comparison between food consumption showed no difference between genders (Table 3).
Associations Between Symptoms/Health Complaints During Last 12 Months and Perceived Stress in Students.

p < .05. **p < .01.
Associations Between Food Consumption and Perceived Stress Symptoms (Each Food Group Adjusted Separate Models for Males and Females and for Both Mental Health Indicators).

p < .05.
A multiple linear regression analysis was performed to determine the relationship between symptoms/health complaints of stress and perception of stress by gender and in the sample as a whole. The analysis showed that the symptoms/health complaints of stress predicted a relationship with perceived stress, something statistically significant for males, F(21,22) = 4.54, p < .001, female, F(21,152) = 12.26, p < .001, and whole, F(21,196) = 15.32, p < .001 (Table 4).
Coefficients of Symptoms/Health Complaints Reported in Last 12 Months.

p < .05 β = standardized coefficient.
Multiple linear regression analysis was performed to determine the relationship between stress predictors and perception of stress by gender and in the sample as a whole. The analysis showed that the predictors of stress predicted a relationship with perceived stress, something statistically significant for males, F(4,39) = 8.04, p < .001, female, F(4,169) = 32.96, p < .001, and whole, F(4,213) = 42.05, p < .001 (Table 5).
Coefficients of Predictors of Perceived Stress Among University Students.

p < .05 β = standardized coefficient.
A multiple linear regression analysis was performed to determine the relationship between predictors of stress and eating habits by gender and in the sample as a whole. The analysis showed that the predictors of stress predicted a relationship with eating habits for Psychological, F(11.32) = 1.27, p > .05, female, F(11,162) = 2.07, p < .05, and whole, F(11,206) = 2.16, p < .05, Circulatory/Breathing, F(11,32) = 0.82, p > .05, female, F(11,162) = 1.52, p > .05, and whole, F(11,206) = 1.41, p > .05, Gastrointestinal, F(11,32) = 0.89, p > .05, female, F(11,162) = 2.64, p < .01, and whole, F(11,206) = 2.41, p < .01, and Pain/Aches males, F(11,32) = 1.10, p > .05, female, F(11,162) = 0.73, p > .05, and whole, F(11,206) = 0.59, p > .05 (table 6).
Associations between predictors of stress and interaction on past week food consumption.
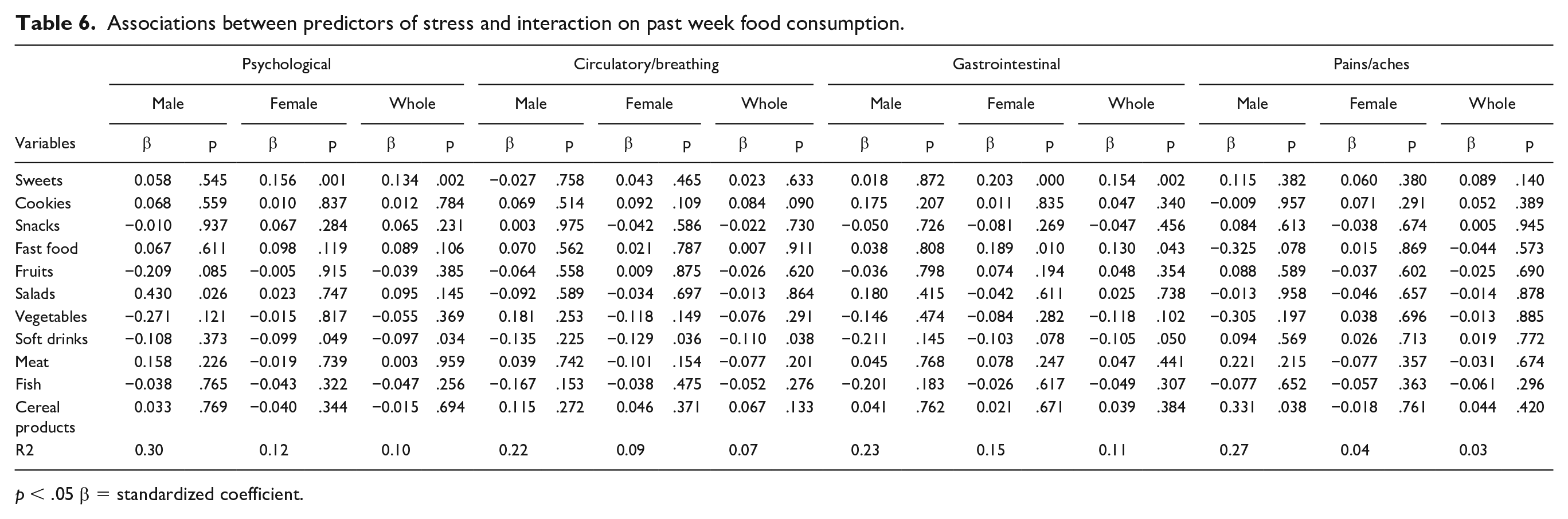
p < .05 β = standardized coefficient.
Overall Discussion
Our result showed that the participants had relatively high levels of perceived stress (M = 19.78, SD = 7.07) compared with previously established norms with a general population sample aged 18 to 29 years (M = 14.2, SD = 6.2) (Cohen et al., 1983; Cohen & Williamson, 1988). Other authors have found values close to ours: 19.7 (Denovan et al., 2017), 17.9 (Shaw et al., 2017), 16.19 (Remor, 2006), and 15.19 (Andreou et al., 2011). A study evaluating physiotherapy students also found a value similar to ours: 19.5 (Jacob & Einstein, 2016). The disparity between the results makes it difficult to generalize a normative score of perceived stress due to several confusing variables. Thus, it may be more appropriate to compare our findings with a student population. Our study found a higher value of perceived stress in women compared with men, however without significant difference. This study supports the use of total PSS-10 scores with Brazilian university students and suggests the scale is not significantly affected by gender bias (Denovan et al., 2017) but differs from another study (Shaw et al., 2017).
As for the first objective of the study, we assessed the association between predictors of perceived stress, 21 symptoms/health complaints, and perceived stress in students. This study explored and compared the frequency of health symptoms/complaints by perceived stress level and showed a relationship with the psychological, circulatory/breathing, and pains/aches predictors. Our result is similar to another study that evaluated stress predictors in students from United Kingdom and Egyptian (Ansari et al., 2014). However, our result did not show a relationship with gastrointestinal problems and perceived stress. Our findings disagree of study with students from Korea, where nursing students with higher perceived stress were significantly more likely to experience gastrointestinal symptoms (Lee et al., 2011). We observed that most students did not practice physical activity regularly, despite having a good health awareness. Sedentary European students with low health awareness and a high level of stress showed an association with psychological, gastrointestinal, and neck ache/backache (Stock et al., 2003), going against our result.
The second objective investigated the gender differences in predictors of perceived stress, 21 symptoms/health complaints, and perceived stress in students. Our study showed that men presented psychological and pains/aches complaints. Women presented complaints with psychological, circulatory/breathing, and pains/aches. This result goes against other studies that found a greater propensity in female students with psychosomatic and gastrointestinal complaints or pain in the neck/back pain (Piko, 2000; Stock et al., 2003; Wardle & Steptoe, 1991). Regarding gender differences in terms of health complaints, we found a greater number of subjective health complaints among women than in men. This finding is supported by previous research that consistently reports higher levels of perceived health complaints among women (Brun Sundblad et al., 2007; Stock et al., 2003, 2008; Von Bothmer & Fridlund, 2005). In our study, women had a higher frequency of nervousness/anxiety, depressed mood, problems with sleep/insomnia, trembling hands, difficulty in speaking, rapid heartbeats, circulatory problems, dizziness, and breathing difficulties. Men, on the other hand, had a higher frequency for back pain. These findings are in line with other studies involving university students from Europe, U.S. and Canada where they exhibited different prevalence of complaints (Ansari et al., 2014; Dyrbye et al., 2006; Stock et al., 2008).
As regards third objective, we assessed the association between predictors of perceived stress and nutritional habits in students. The results of the present study suggest that predictors of stress are significantly associated with certain food choices among university students. Thus, a greater stress predictor associated with a higher consumption of unhealthy foods and a lower consumption of healthy foods and unhealthy drinks was observed in this study. The psychological symptoms showed an association with candy, salad, and soda. Other studies have found an association between the consumption of sweets/fast food and fruits/vegetables and perceived stress (Mikolajczyk et al., 2009), and increased consumption of sweets, chocolate, cake, and cookies was associated with higher levels of perceived stress (Kandiah et al., 2006). Consumption of unhealthy foods and depressive symptoms and perceived stress was observed among students from Poland, Bulgaria, and Germany, especially among students (Mikolajczyk et al., 2009). Our results showed that women consumed more sweets, fast foods, salads, and soft drinks and men consumed more salads and cereal products. In a longitudinal study, carried out only among women, high levels of perceived stress were associated with less physical activity during leisure, increased consumption of fast food, and increased time spent watching television (Mouchacca et al., 2013). Unhealthy food practices and habits could impose health risks later in life. The perceived stress was significantly associated with past week coffee, soda, fast food, energy drinks, salty snack food, and frozen meal consumption (Errisuriz et al., 2016). High levels of perceived stress were associated with low dietary perception and low physical activity (Mouchacca et al., 2013; Vidal et al., 2018). Most of the foods and beverages consumed by the stressed students in this study were energy-dense and nutritionally poor foods. Such choice, for these items, may be related to the ease of substituting healthy meals, for quick sources of energy during a moment of stress experienced by the student (Errisuriz et al., 2016). Convenience was considered the most important reason for choosing certain foods in Canadian college students (Marquis, 2005). There was no association between stress and conscious consumption of healthy foods among students.
Strengths and Limitations
This study demonstrates a relationship between high levels of perceived stress, predictors of stress, and eating habits using a sample of undergraduate physiotherapy students. However, this study has several limitations. First, due to the transversal nature, only the association and not the causality can be determined. In addition, the sample included in the study may not be representative of the total population of physiotherapy students in our country. Our findings were estimated with three samples of students from three private physiotherapy colleges and, therefore, the results may not be extrapolated to public institutions. Second, the variation in student recruitment methods and research timing may have introduced a selection bias, although the direction of the bias is difficult to predict. Third, we did not ask whether students ate at the university canteen/refectory or at their parental home. In both these cases, students may have less control over what they eat, especially at meal times.
Despite these limitations, several important conclusions can be drawn from the results of this study. The variations observed in the health-related lifestyle and in the prevalent complaints show the need for a differential approach to health promotion and disease prevention focusing on young adults. The study has important strengths in terms of improving our knowledge; no previous study seems to have investigated in detail and compared the relationships between perceived stress and a wide range of self-reported health complaints and eating habits in samples from students from different colleges in Brazil. Colleges and universities could develop campaigns to promote healthy food and beverages during the school year, which can have a positive impact on food choices. More research is needed to understand which strategies most effectively reduce stress and poor food choices.
Conclusion
This study showed an association between mental health indicators (perceived stress and health symptoms and complaints) and food intake in physical therapy students. Female students had greater complaints compared to male students. Our findings suggest using it in other contexts such as public universities and other university courses to assess students’ mental health status and food intake.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.