
Abstract
Neighborhood social capital—resources inherent within community networks—has been identified as a potential facilitator of personal well-being. We test hypotheses concerning how neighborhood social capital moderates the influence of parenting strain on mastery (individuals’ understanding of their ability to control personal life circumstances) for female primary caregivers of children. First, we test how different forms of neighborhood social capital—social support, social leverage (information exchange), informal social control, and neighborhood organization participation—modify the association between parenting strain and mastery. Second, we test whether such moderation depends on one’s access to these forms via neighbor ties. Analyses of Los Angeles Family and Neighborhood Survey data (N = 765) indicate that the negative relationship between parenting strain and mastery worsens as informal social control increases. Social support and informal social control, however, buffer this parenting strain-mastery relationship when caregivers have stronger ties to neighbors. Our findings implicate mechanisms of “negative social capital” and warrant more nuanced considerations of neighborhood social capital’s health-promoting potential.
The concept of social capital has received intense interest within population health—particularly among researchers interested in how neighborhood environments contribute to the health of individuals. Within this “neighborhood effects” research, social capital generally has been conceptualized as resources of community social ties or networks that can be used by residents to promote or maintain health and well-being (e.g., Kawachi 2010). Although this research has helped highlight how community contexts matter for personal well-being, most of these studies have analyzed only direct effects of neighborhood social capital on personal health outcomes. Little attention, however, has been paid to whether neighborhood social capital, as a resource to be drawn from by residents in times of need, may moderate—that is, minimize or exacerbate—one’s capacity to undertake action to maintain or improve health and well-being (for one exception, see Browning and Cagney 2002).
Motivated by this issue, we use a previously developed theoretical model of neighborhood social capital and research on community and family processes to propose and test several hypotheses concerning how different forms of neighborhood social capital—alone and in conjunction with personal access to these forms—may serve as community-located resources for moderating the impact of life stresses encountered by individual residents. We specifically focus on female primary caregivers of children—as prior literature has implicated neighborhood conditions as important for their well-being (e.g., Dominguez and Watkins 2003)—and mastery, the extent to which one considers life chances being in one’s personal control versus fatalistically ruled (Pearlin and Schooler 1978) and a critical personal resource for pursuing and/or maintaining health and well-being. The current study extends prior neighborhood social capital health research that typically (a) analyzes only the direct or main effects of neighborhood structural conditions on individual-level outcomes, (b) focuses on general adult populations rather than specific demographic groups for whom neighborhood context may have particular importance, and (c) overlooks personal capacity for maintaining or enacting changes to health practices (Robert, Cagney, and Weden 2010).
Background
Neighborhood social capital may have the greatest implications for the well-being of those who rely most on their neighborhoods (Carpiano 2008). Thus, women—and primary caregivers of children in particular—provide an excellent opportunity to examine the implications of neighborhood social capital for two related reasons. First, research has identified that women have more neighbor ties than do men (Campbell and Lee 1992, Moore 1990). Second, women are more likely than men to be the primary caregiver for a child (Rosenfield 1999), a demanding and challenging social role for which neighbors may often be used in personal efforts to address daily tasks and achieve optimal health and nonhealth outcomes for herself, her child(ren), and other family members (Crnic and Low 2002, Dominguez and Watkins 2003).
In theorizing how neighborhood social capital may matter for personal health and well-being, we empirically focus on the relationship between parenting strain and mastery. Even though parenting strain has been extensively linked to parental and child well-being (Crnic and Low 2002:256) and mastery has been studied with respect to adults’ general network-based social capital (Moore et al. 2009) and mothers’ neighborhood social contexts (Christie-Mizell and Erickson 2007), little research has investigated the relationship among parenting strain, mastery, and neighborhood social capital. Guiding our examination of neighborhood social capital for female primary caregivers is a conceptual model, detailed in Figure 1, that highlights the key constructs of interest. We use this model to frame the discussion of our theoretical background and formulation of our study hypotheses.

Conceptual Model of Neighborhood Social Capital Processes on Individual Mastery
Mastery
Mastery “concerns the extent to which one regards one’s life-chances being under one’s own control in contrast to being fatalistically ruled” (Pearlin and Schooler 1978:5). Identified as sharing a common conceptual core with personal control (Skaff, Pearlin, and Mullan 1996) and self-efficacy (Gecas 1989), mastery is not a fixed personality characteristic but rather a self-concept shaped by life situations, including stress and social support (Krause 1999; Skaff et al. 1996). With respect to health and well-being, mastery is important to examine for several reasons. First, increased mastery is associated with self-initiated preventive care, optimism concerning the efficacy of early treatment, fewer doctor visits, and better health (Seeman and Seeman 1983) as well as lower depressive symptom scores (e.g., Turner and Noh 1988).
Second, mastery is a key psychological resource that helps individuals cope with stressors, giving them a sense of control over their own life situations and mediating stressors’ negative effects on health and other outcomes (Pearlin and Schooler 1978; Thoits 1995). Conversely, low mastery may be associated with avoiding challenging or difficult situations, such as undertaking changes in health practices (Strecher et al. 1986). Third, mastery also has been considered in relation to social networks. Seeking assistance (whether emotional, informational, or material in nature) from social networks in dealing with life stressors can help replenish or enhance mastery that may have been undermined by stressful circumstances (Krause 1999). In terms of neighborhood networks, people who lack neighborhood social ties report higher levels of powerlessness (Geis and Ross 1998). In sum, mastery constitutes an important construct to examine the interplay between individual psychological resources and neighborhood social structures.
Parenting Strain
Because mastery can be undermined by stressful life situations, we specifically consider the impact of parenting strain on mastery. Increased child-related chronic strains are linked to lower mastery among parents (Cassidy and Davies 2003). Likewise, everyday parenting-related hassles have been identified as contributors to negative parenting behavior and lower parental and child well-being (see Crnic and Low 2002). Furthermore, social support has been found to buffer maternal psychological distress associated with parenting hassles (Crnic and Greenberg 1990). Thus, parenting strain is a crucial determinant of functioning in parenting and nonparenting domains, and neighborhood social networks may factor importantly in moderating this relationship.
Social Capital and Neighborhood Constructs
Our conceptualization of social capital and neighborhood constructs is based on Carpiano (2006), who draws upon Bourdieu’s (1986) social capital theory in formulating a multilevel conceptual model of neighborhood-based social capital and personal health and well-being that delineates social capital from its antecedents and consequences (see Portes 1998) and thus can be used to generate testable hypotheses. As this model has been discussed extensively elsewhere (e.g., Carpiano 2006, 2008; see also Cene et al. 2011; Witten et al. 2009), we briefly review it here. Central to this model are three neighborhood-level constructs (social capital, social cohesion, structural antecedents) and one individual-level construct (neighborhood attachment).
Social capital, according to Bourdieu’s (1986) theory, refers to actual or potential resources inherent in social networks. In conceptualizing neighborhood social capital as neighborhood network-based resources, Carpiano’s (2006) model considers four “forms” of social capital identified in community sociology research as important for individuals in pursuing various outcomes: social support, social leverage, informal social control, and neighborhood organization participation. Social support is a form of social capital that residents can draw upon to cope with daily problems, while social leverage helps residents access information and potentially advance socioeconomically (e.g., via the sharing of job and child care information; Briggs 1998; Dominguez and Watkins 2003). Informal social control concerns residents’ ability to collectively maintain social order and keep the neighborhood safe from criminal or delinquent activity (Sampson 2001). Neighborhood organization participation refers to residents’ formally organized collective activity for addressing neighborhood issues (Altschuler, Somkin, and Adler 2004; Saegert and Winkel 1998). Each form has been theorized to affect health and well-being via numerous material and psychosocial pathways and may be either beneficial or detrimental to health and well-being (Carpiano 2007a). We discuss specific pathways in the Study Hypotheses section.
Social cohesion refers to patterns of social interaction and values (e.g., network formation and mutual trust) that lead to social capital and that serve as intermediaries between structural antecedents and social capital. It may also impact outcomes independently of the resources to which it gives rise (see Cene et al. 2011). Structural antecedents are neighborhood and surrounding-area structural characteristics (e.g., socioeconomic disadvantage, residential stability) that have implications for the extent of network ties and associated values (social cohesion) and resources (social capital) available within the neighborhood itself (Wacquant and Wilson 1989). Because this study centers on social capital and its outcomes, structural antecedents and social cohesion will be treated as neighborhood-level confounders.
Access to Resources: Neighborhood Attachment
Individual residents’ neighborhood attachment refers to the degree to which individuals socialize with neighbors and thus are embedded in neighborhood-based networks. This construct recognizes Bourdieu’s (1986) focus on the importance of a person being connected—or having access—to networks that possess resources. Some neighborhood resources may be limited to specific network members, and as one’s network membership increases, so too does one’s benefits—and risks—received from different forms of social capital (Carpiano 2008; Cene et al. 2011; Witten et al. 2009).
Study Hypotheses
How might neighborhood social capital (as conceptualized in the model detailed above) matter regarding the relationship between parenting stress and mastery? Prior research provides useful insights for specifying several a priori hypotheses, which we review below with respect to the pathways numbered 1 and 2 in Figure 1.
Pathway 1: Neighborhood Resources Moderating the Parenting Stress-Mastery Relationship
In Pathway 1, forms of neighborhood social capital moderate the relationship between parenting stress and mastery. We propose two hypotheses regarding the direction of this relationship.
Neighborhood resource advantage hypothesis
On the basis of extensive research documenting a generally positive association between the extent of social resources available in a community and residents’ personal well-being (e.g., Robert 1999), we first propose a neighborhood resource advantage hypothesis: Increasing levels of neighborhood social capital—a neighborhood network-based resource—can be beneficial for residents in their efforts to manage personal life situations and maintain or increase their personal well-being (e.g., Robert 1999). In terms of moderating the effects of parenting strain on mastery, social support can provide caregivers with expressive and instrumental assistance for handling daily child care and other life tasks, while social leverage can provide useful information regarding parenting and other life domains (e.g., jobs), including local programs and other opportunities (Cattell 2001; Dominguez and Watkins 2003). Informal social control can provide community concern and action for maintaining order and safety (from crime) as well as for monitoring of local children, while neighborhood organization participation offers formally organized efforts for addressing local issues with the social and physical environment (e.g., aesthetics, potential hazards, and service provision) that may benefit quality of life for families (Altschuler et al. 2004; Friedman et al. 2007; Witten et al. 2009). Empirical evidence consistent with this hypothesis would need to demonstrate that the negative association between parenting strain and mastery diminishes as the level of neighborhood social capital increases.
Neighborhood resource disadvantage hypothesis
Neighborhood social capital can also have harmful consequences—for adults in general and female caregivers of children in particular (Carpiano 2007b, 2008). First, the extent of neighborhood social capital may provide less incentive for residents to establish and/or use social capital outside of their neighborhood. Thus, favors obtained via social support and information received via social leverage may be less useful for dealing with problems due to highly concentrated and less diffuse network ties (Cattell 2001; Granovetter 1973; Small 2004). Second, a community may (a) exert excessive informal social control (e.g., a culture of conformity) that constrains individual or group attitudes, opportunities, and actions (Friedman et al. 2007; Portes 1998) and/or, (b) in terms of neighborhood organization participation, engage in collective activities to maintain or alter the local social and physical environment that (regardless of the group’s intention) may undermine some residents’ well-being and quality of life (Altschuler et al. 2004). Collectively, this evidence supports a neighborhood resource disadvantage hypothesis: Increasing levels of neighborhood social capital can be disadvantageous for residents in maintaining or increasing their personal mastery. Empirical evidence corroborating this hypothesis would need to show that the negative relationship between parenting strain and mastery worsens as the level of neighborhood social capital increases.
Pathway 2: Personal Access to Neighborhood Social Capital
As noted by Witten et al.’s (2009:2893) study of parents, neighborhood social capital can provide assistance, but personal access to such resources is not always assured. Pathway 2 thus specifies a three-way interactive relationship whereby the degree to which forms of neighborhood social capital moderate the relationship between parenting stress and mastery is also contingent upon an individual’s level of neighborhood attachment, thereby leading to two contrasting hypotheses.
Personal access, mastery-promoting hypothesis
Health disparities research suggests that people with greater access to beneficial social connections (among other factors) are better situated to avoid harm and maintain health and well-being than are those with less access (Carpiano et al. 2007). A personal access, mastery-promoting hypothesis would thus suggest that greater neighborhood social capital will be more advantageous for residents in maintaining or increasing their personal mastery if they have greater personal access to that social capital. Empirical evidence supporting this hypothesis would need to show that the buffering effect of neighborhood social capital on the parenting strain-mastery relationship is stronger for caregivers with greater neighborhood attachment.
Personal access, mastery-damaging hypothesis
Higher levels of personal access to some forms of neighborhood social capital may also have risks (Carpiano 2008). Research suggests several related ways in which this may occur for each of the four social capital forms. First, residents with high levels of network access may have most of their network located in their neighborhood. Such network density may be less useful for achieving desired outcomes, compared with more diffuse networks through which more abundant or useful resources, such as social support and social leverage, may be available (Cattell 2001; Granovetter 1973; Small 2004). Second, one’s extent of neighborhood attachment may affect the degree to which neighborhood social capital can limit personal choice and behaviors due to constraints of informal social control (Friedman et al. 2007; Portes 1998) and neighborhood organization participation activities (Altschuler 2004). Third, residents in general, but female caregivers in particular, with greater attachment may receive more demands—and, thus, more strains—from their neighborhood community involvement, such as frequent obligations to provide social support and social leverage to neighbors and to participate in collective and neighborhood organization-based activities (Dominguez and Watkins 2003; Portes 1998).
Collectively, this evidence supports a personal access, mastery-damaging hypothesis: Increased neighborhood social capital will be more disadvantageous for residents in coping with the impact of personal life situations on mastery if they have greater personal access to that social capital. Empirical evidence supporting this hypothesis would need to show that the exacerbating effect of neighborhood social capital on the negative parenting strain-mastery relationship is stronger for caregivers with higher levels of neighborhood attachment.
Data and Methods
Data Set and Sample
Our study data are from Wave 1 of the Los Angeles Family and Neighborhood Survey (L.A.FANS), which is an ideal data set for testing our hypotheses. L.A.FANS is representative of all neighborhoods and households in Los Angeles County, California, and oversamples poor neighborhoods and families with children (L.A.FANS 2011). The adult module contains 2,620 individuals sampled within 65 census tracts (85 percent response rate), from which we constructed two samples: one sample for creating neighborhood-level social capital and social cohesion measures for each of the 65 census tracts and another sample for creating respondent-specific measures (e.g., parenting strain and mastery).
The sample used to create our neighborhood-level measures was composed of 2,557 respondents who had complete (nonmissing) data for the neighborhood measures. Of these respondents, more than 95 percent had nonmissing data for all demographic variables needed for computing the neighborhood-level measures (method detailed below and in the Online Supplement). Thus, as missing data for this sample were negligible (≤3.1 percent for any variable), depending on the variable, the mean, median, or mode was imputed.
The sample used for our respondent-specific measures consisted of 765 female primary caregiver (to children) respondents who (a) had complete data on the variables needed for our analyses (91 percent) and (b) lived in their current residence for 12 months or longer—due to the logic that most “neighborhood effects” on well-being, including the effects of social capital tested here, are not immediate and require some length of exposure to a neighborhood environment (see Carpiano 2008). Supplementary analyses using multiple imputation via the ice procedure in Stata 10 (Royston 2005) indicated that missing data were not biasing our findings.
Neighborhood-Level Measures
All neighborhood-level variables were measured at the census tract level, which L.A.FANS used for approximating neighborhood boundaries and sample recruitment. For the four social capital forms and social cohesion, neighborhood-level measures of each construct were computed using L.A.FANS survey items regarding perceived neighborhood environment, for which each of the 2,557 aforementioned respondents answered. Table 1 details the survey items that were used to create the neighborhood-level measures of the four social capital forms (social support, social leverage, informal social control, and neighborhood organization participation) and social cohesion constructs that were discussed in the Background section. The neighborhood organization participation item asks about participation in the past 12 months; hence, the sample used to create this measure was restricted to respondents who lived in their neighborhood for 12 months or more.
Items Used for Neighborhood-Level Social Capital, Social Cohesion, and Individual-Level Neighborhood Attachment Variables
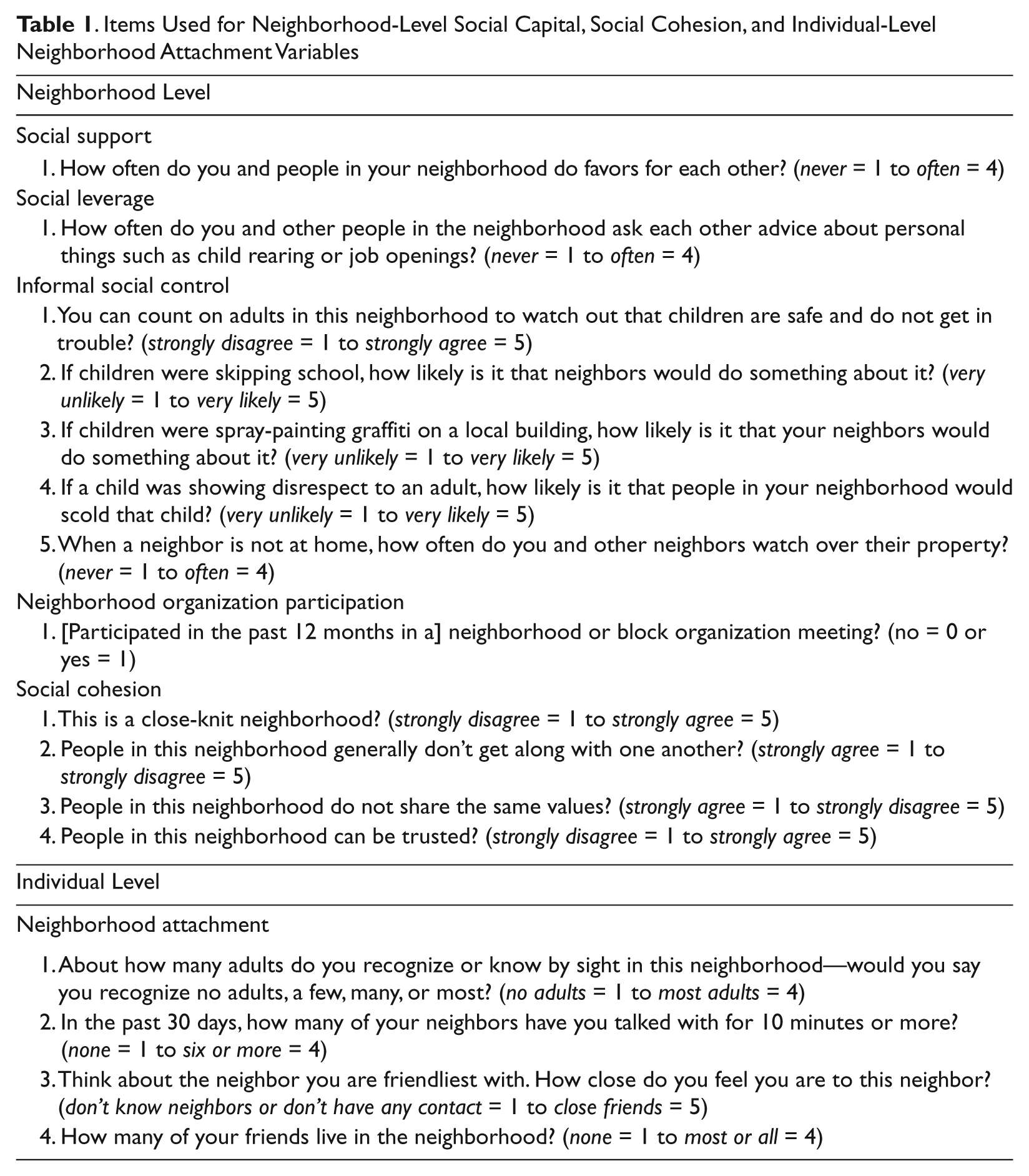
Because L.AFANS’s sample was clustered within 65 census tracts, respondents served as raters of their own neighborhoods; thus, numerous ratings were available for each of the 65 neighborhoods. Instead of simply aggregating these survey-based ratings and computing a neighborhood-specific mean score for each social capital and social cohesion measure, we used empirical Bayes residuals derived from multilevel regression models as neighborhood-level measures of the social capital forms and social cohesion. Each of these empirical Bayes residual-based measures is a neighborhood-specific estimate of social capital forms and social cohesion that (a) is a standardized deviation from the neighborhood-level grand mean score of each measure and (b) is adjusted for sociodemographic and item response characteristics of every respondent “rater” (as such factors could influence responses that a rater provides when asked about his or her neighborhood’s social capital and social cohesion). This method, detailed in the Online Supplement, has been used extensively in prior research (e.g., Browning and Cagney 2002; Carpiano 2007b).
Structural antecedents were assessed with two measures created using U.S. Census 2000 Summary File 3 (U.S. Census Bureau 2011). Socioeconomic disadvantage was computed using five indicators: income inequality, mean family income, percentage foreign-born, percentage female-headed households, and percentage living below the poverty level. Income inequality was measured using the Gini coefficient, which can range from 0 to +1.0, whereby the higher the value, the larger the degree of unequal income distribution. A composite score was created by z-scoring each item (Cronbach’s alpha = .89) and computing the mean of the five items. Residential stability was measured using the percentage of residents who lived in the same tract five years earlier. All neighborhood-level measures were standardized to have a mean = 0 and standard deviation = 1.
Table S1 in the Online Supplement presents correlations for the neighborhood measures. Correlations for some of these measures pose potential implications for multicollinearity in multivariate analyses, which can limit accurate assessment of whether a variable is significantly associated with an outcome (due to widening confidence intervals and inflated p values). We address this issue in the Discussion section.
Individual-Level Measures
All individual-level measures were obtained from the L.A.FANS data. Table 2 reports their univariate statistics. Mastery is the dependent variable, measured as the sum of five items of Pearlin and Schooler’s (1978) Mastery Scale. Respondents were asked the degree to which they agree or disagree with the following statements: “There is really no way I can solve some of the problems I have,” “Sometimes I feel that I’m pushed around in life,” “I have little control over the things that happen to me,” “I often feel helpless in dealing with the problems of life,” and “There is little I can do to change many of the important things in my life.” Each item uses a 4-point response scale ranging from strongly agree = 1 to strongly disagree = 4. All items were coded such that higher scores reflected higher mastery (Cronbach’s alpha = .77).
Descriptive Statistics of Individual-Level Variables (N = 765)
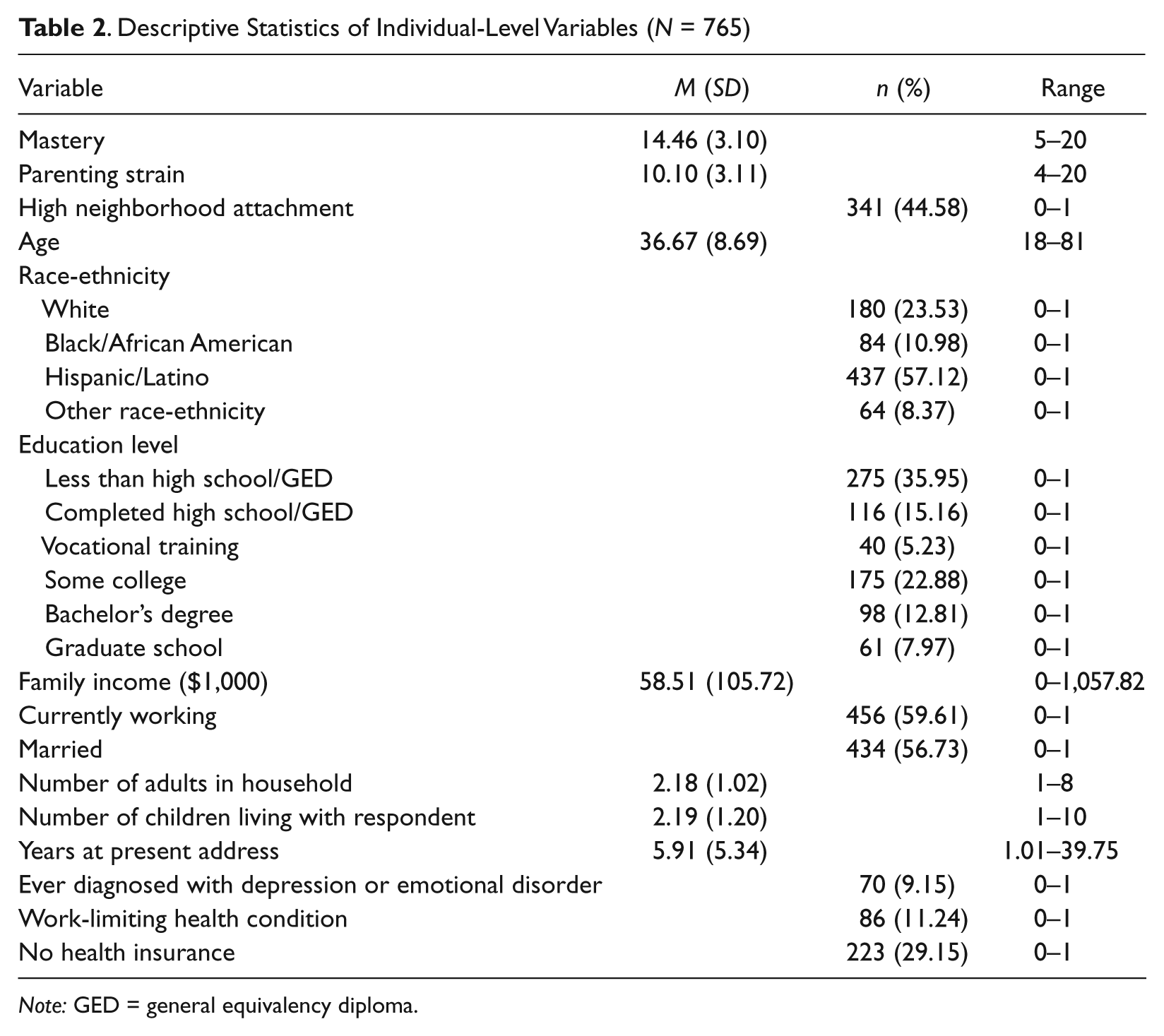
Note: GED = general equivalency diploma.
Parenting strain is measured using a composite scale consisting of the sum of four extensively used items that asked respondents their opinions regarding the following statements: “Being a parent is harder than I thought it would be,” “I feel trapped by my responsibilities as a parent,” “I find that taking care of my child/children is much more work than pleasure,” and “I often feel tired, worn out, or exhausted from raising a family.” Each item used a response scale ranging from completely false = 1 to completely true = 5. The Cronbach’s alpha for these four items was .70, indicating acceptable reliability.
Neighborhood attachment is measured with four items (see Table 1) summated into a single measure (Cronbach’s alpha = .65). On the basis of its prior use and interpretation (Carpiano 2007b, 2008) as well as to facilitate analysis and interpretation of interaction terms, this scale was dichotomized according to the median score of 11 into low (≤11 = 0) and high (>11 = 1) neighborhood attachment.
Sociodemographic confounders included age, race-ethnicity (coded as black/African American, Hispanic/Latino, and other, with white as the referent category), education level (coded from less than high school or GED = 0 to graduate or professional school = 5), annual family income (in USD $1,000 units), currently working (yes = 1, no = 0), marital status (married = 1, other marital status = 0), number of children and adults living in the household, years at present address, and health status. For parsimony, we modeled education as a continuous variable, although similar results were obtained when we modeled it as a series of categorical variables. For income data, we used the L.A.FANS income file, which accounts for incomplete or missing information via various income measures throughout several interview modules and multistep imputation procedures (L.A.FANS 2011). Because health poses potential implications for both mastery and social engagement, we also control for health status using three variables (each coded yes = 1, no = 0): (a) ever being diagnosed with depression or an emotional disorder (assessed via two items asking the respondent whether a doctor ever told her that she had either condition), (b) the presence of a work-limiting health condition (based on a lone item asking whether the respondent has a “physical, psychological, or nervous condition that limits the type of work or the amount of work [she] can do”), and (c) no health insurance.
Analytic Procedures
We tested our hypotheses using two-level hierarchical (random intercept) linear regression models in Stata version 10 (StataCorp, College Station, Texas), whereby all parameters are specified as fixed effects with only the intercept specified to have a (between-neighborhood) random effect. Preliminary analyses (not shown here) indicated that the interactions we modeled did not significantly vary across neighborhoods; hence, all interaction terms are specified as fixed effects with no corresponding random effect term. We report p values ≤.05 as statistically significant.
Results
Table 3, model 1, shows estimates for parenting strain and neighborhood attachment while only individual-level confounders are controlled for. Increased parenting strain is significantly associated with lower mastery. Though not shown, the directions of the slope coefficients for other covariates are consistent with prior studies: Mastery is positively associated with both education and income (p ≤ .01) and negatively associated with age (p ≤ .10). Also, preliminary analyses (not shown) revealed that neighborhood attachment does not mediate the relationship between parenting strain and mastery.
Unstandardized Slope Coefficients for Individual-Level Mastery Regressed on Individual-Level Parenting Strain, Neighborhood Attachment, and Sociodemographic Factors and Neighborhood-Level Social Conditions
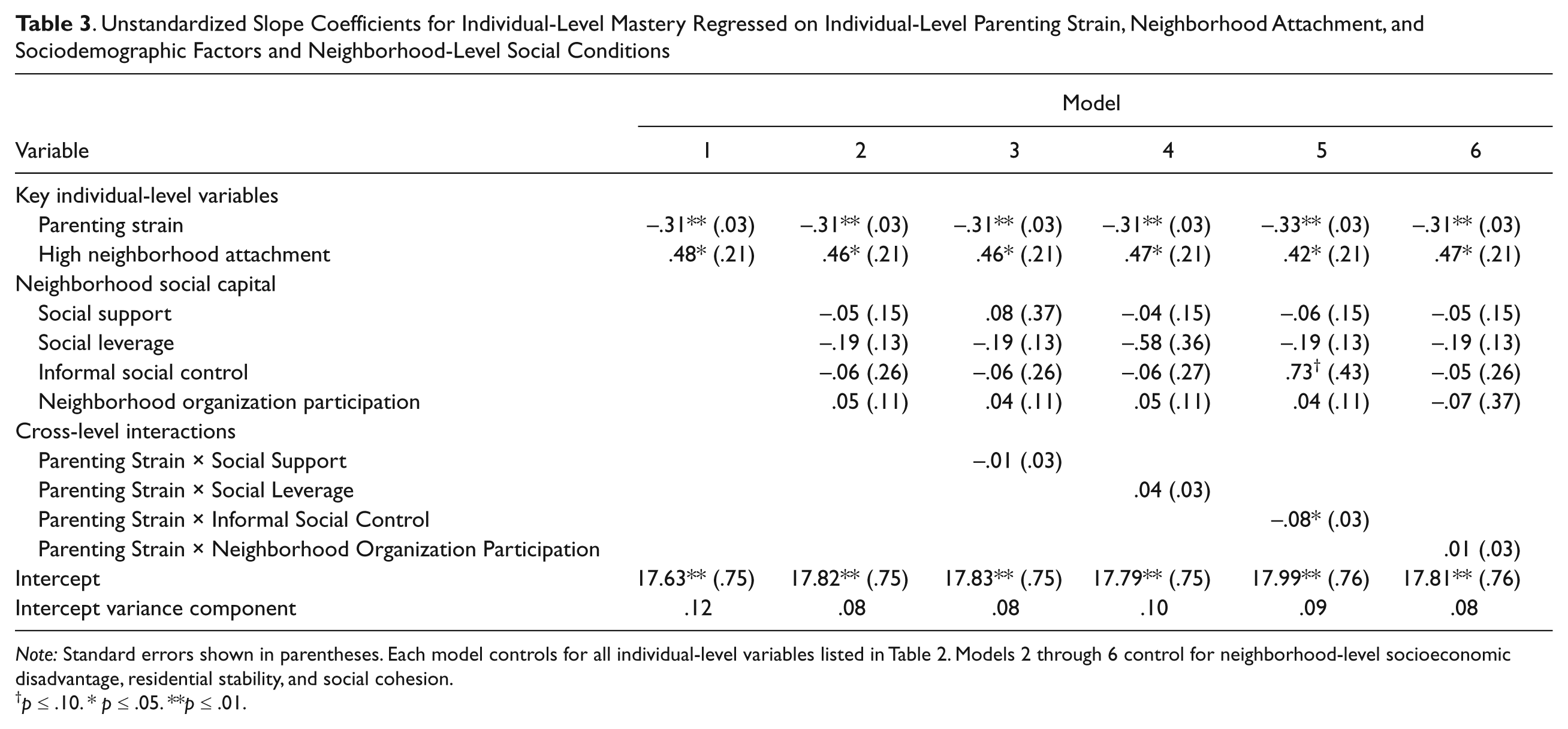
Note: Standard errors shown in parentheses. Each model controls for all individual-level variables listed in Table 2. Models 2 through 6 control for neighborhood-level socioeconomic disadvantage, residential stability, and social cohesion.
p ≤ .10. * p ≤ .05. **p ≤ .01.
Model 2 expands model 1 by incorporating all neighborhood-level variables to test the direct effects of the four neighborhood social capital forms (social support, social leverage, informal social control, and neighborhood organization participation) on mastery. None of the social capital forms has a significant direct effect on mastery. Next, we proceed to presenting the results of models that test our specific study hypotheses.
Testing the Resource Hypotheses: Neighborhood Social Capital Forms as Moderators
Does neighborhood social capital moderate the negative relationship between parenting strain and mastery observed in model 1? To evaluate this question (and test the resource-specific hypotheses), models 3 through 6 include interaction terms for parenting strain and each social capital form. Informal social control is the only social capital form that significantly moderates the association between parenting strain and mastery. Figure 2 graphs this interaction by plotting predicted mastery scores for parenting strain (at the 25th, 50th [median], and 75th percentile values) according to three values of informal social control values (–1 SD, M [0], +1 SD) with all other covariates set to their mean, median, or mode. This graph indicates that the parenting strain-mastery association increases as informal social control increases: The actual and standardized point differences in mastery between the lowest and highest levels of parenting strain at the −1 SD, M, and +1 SD levels of informal social control are, respectively, 1.0 (0.33 SD), 1.3 (0.42 SD), and 1.6 (0.52 SD) points.

Personal Mastery Scores for the 25th, 50th (Median), and 75th Percentile Values of Parenting Strain According to Neighborhood-Level Informal Social Control
Testing Hypotheses Concerning Personal Access to Neighborhood Social Capital
Next, we test our personal access hypotheses: the extent to which the moderating effect of neighborhood social capital (resource) on the parenting strain-mastery relationship is contingent upon an individual’s level of neighborhood attachment (access). We estimated four separate models—each of which specified a three-way interaction between parenting strain, one of the four social capital forms, and neighborhood attachment—as well as (for proper model specification) all three lower-order, two-way interactions between these three variables. Table S2 in the Online Supplement shows the estimates for these models. The coefficients for the three-way interaction terms indicate moderating effects of social support and informal social control contingent upon a caregiver’s level of neighborhood attachment.
Figure 3 graphs these results for (a) social support and (b) informal social control in the same manner as Figure 2 but stratified by low and high neighborhood attachment. Mastery is generally higher among caregivers with higher (versus lower) neighborhood attachment. Also, for each level of social support, the difference between the mastery scores for the lowest and highest levels of parenting strain is smaller for caregivers reporting high versus low neighborhood attachment. For caregivers with low attachment, these differences in mastery between high and low parenting strain range from 1.6 (at the −1 SD level of social support) to 1.4 points (at the +1 SD level of social support)—differences of 0.52 to 0.45 SD units. By contrast, caregivers with high neighborhood attachment have difference scores ranging from 0.40 (at −1 SD social support) to 1.2 points (at +1 SD social support) or, respectively, 0.13 to 0.39 SD units.
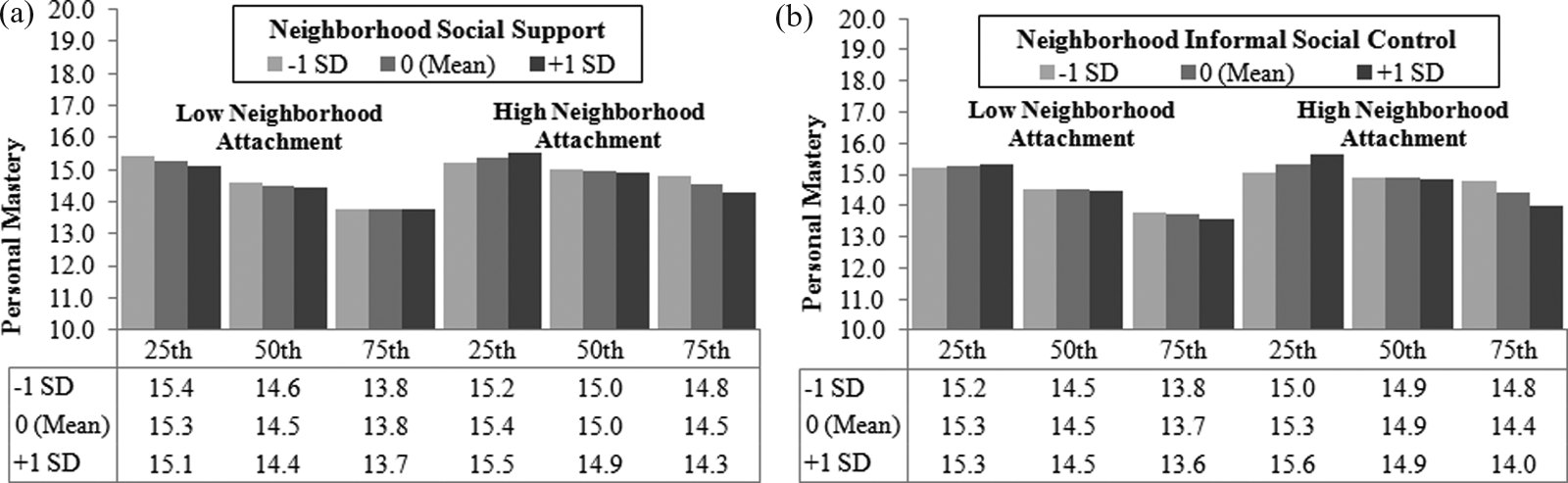
Personal Mastery Scores for the 25th, 50th (Median), and 75th Percentile Values of Parenting Strain According to Levels of Neighborhood Social Capital and Personal Neighborhood Attachment: (a) Neighborhood Social Support and (b) Neighborhood Informal Social Control
For informal social control, a similar pattern of results is found. Mastery scores are generally higher for caregivers with high (versus low) neighborhood attachment. For each level of informal social control, differences in mastery between the highest and lowest parenting strain levels for caregivers with low attachment range from 1.4 (at −1 SD informal social control) to 1.7 (at +1 SD informal social control), or differences of 0.45 to 0.55 SD units, but, for caregivers with high attachment, range from 0.2 to 1.6 (or 0.06 to 0.52 SD unit differences). Thus, greater variation exists in the moderating effect of increased informal social control among caregivers with high (versus low) attachment; however, for each level of informal social control, differences in mastery found across parenting strain levels are either comparably smaller or, in the case of the +1 SD level of informal social control, roughly equivalent to the difference scores observed for caregivers living in neighborhoods with the same levels of informal social control but reporting low neighborhood attachment.
Discussion
We began this study with the aim of understanding how neighborhood social capital may serve as an important social structural resource for moderating the relationship between personal social circumstances and the capacity to pursue health and well-being. In pursuing this aim, we applied an existing conceptual model of neighborhood social capital and related constructs to the empirical test case of parenting strain and its relationship to mastery among female primary caregivers of children. Below, we discuss our findings with respect to our a priori hypotheses based on prior literature.
Evidence for the Resource Hypotheses
Our first set of hypotheses concerned the extent to which neighborhood social capital, as resources, can positively or negatively moderate the association between personal circumstances and well-being. We found support for the neighborhood resource disadvantage hypothesis for informal social control: The general pattern of a negative parenting strain-mastery relationship was exacerbated across increasingly higher levels of neighborhood informal social control. This finding is consistent with classic sociological considerations of how group membership can undermine personal agency and well-being (e.g., Durkheim 1951) as well as contemporary studies documenting specific mechanisms through which social capital can have downsides (e.g., Altschuler et al. 2004). Increased informal social control may be indicative of specific local norms regarding parenting behavior that may present further constraints on how one is able to respond to stressors as they arise. Consequently, these added constraints on one’s options or repertoire may serve to further undermine personal mastery. More neighbors looking out for local children’s well-being may mean increased norms regarding how one should parent a child, which may also spill over into how one handles other areas of one’s life. Alternatively, as parenting strain increases, a high informal social control neighborhood may provide a caregiver with resources that may, in turn, have the unintended consequence of undermining personal mastery due to extensive reliance on others enabled via the availability of such social capital.
Evidence for the Personal Access Hypotheses
Our second set of hypotheses concerned personal access to neighborhood social capital: how the moderating effect of neighborhood social capital may be contingent upon one’s degree of socializing with neighbors. Our findings support the personal access, mastery-promoting hypothesis for two of the four forms of social capital: For caregivers with higher levels of personal neighborhood attachment, increased neighborhood social support and informal social control may be beneficial for moderating the parenting strain-mastery relationship. Consistent with this hypothesis, caregivers who lived in neighborhoods with higher levels of social support and informal social control and who reported high neighborhood attachment had higher mastery scores across nearly all levels of parenting strain compared to caregivers at similar parenting strain and neighborhood social capital levels but who reported low neighborhood attachment. Although more variation in the moderating effects of social support and informal social control was found among caregivers with high (versus low) neighborhood attachment, the general pattern of results indicates that having high neighborhood attachment is beneficial in buffering the negative association between parenting strain and mastery.
These findings are consistent with existing research that suggests that people with greater access to beneficial social connections (among other resources) are better situated to avoid harm and to maintain health and well-being than are those with less access (e.g., Carpiano, Link, and Phelan 2008). Consistent with Bourdieu’s (1986) social capital theory, having high neighborhood attachment indicates a level of embeddedness in neighborhood networks that permits access to and use of network resources. For neighborhood social support, such access is likely important because neighbors may be less inclined to offer social support (i.e., in terms of favor exchange and sharing of other instrumental assistance) to residents they do not know well or with whom they infrequently socialize. For informal social control, high neighborhood attachment may be important for fostering bonds with neighbors that are necessary for local social norms to emerge and be practiced and reinforced—as well as to have regulatory influences upon individual residents’ behaviors. At the very least, socializing with neighbors allows residents to know (a) who lives in the neighborhood and, (b) in the case of parenting and child monitoring, who the local children are—both of which are important from the standpoint of maintaining community safety and order.
Consideration of the Collective Study Findings
Although these findings are consistent with our a priori hypotheses based on prior literature, social support and informal social control are only two of the four neighborhood social capital forms examined in this study. Overall, the nonsignificant findings are also instructive in at least two ways for understanding how different forms of neighborhood social capital may operate for health.
First, some forms of neighborhood social capital may be insufficient for modifying the effects of parenting strain, a specific type of chronic strain, on mastery, a specific outcome. Prior studies indicate that each of the social capital forms examined here affect health via other direct and moderating pathways (e.g., Carpiano 2007a, 2008). Hence, our nonsignificant findings for social leverage and neighborhood organization participation warrant further study of all four social capital forms with respect to other direct, indirect, and moderating pathways with other health outcomes.
Second, some nonsignificant findings may be indicating competing positive and negative effects of social capital—an important issue for both theory and measurement. As explicitly considered in this study, social capital can provide assistance as well as burdens and demands. As such, there is a need in future research to better measure and model these positive and negative features of each social capital form.
Strengths and Limitations
In light of these findings, several limitations must be considered. First, our study focused predominantly on informal neighborhood social ties and was limited in its ability to account for formal organizations (e.g., child care centers, social service and other community-based organizations) that may also provide resources to caregivers as well as foster social capital (Small 2006). These organizations are beyond the study’s scope, but including measures of such organizations in future analyses would be an important next step to further evaluate some of the mechanisms tested in this study. Nevertheless, it could be argued that if such mechanisms are operating within a particular neighborhood, then our measures are accounting for resources that may become available to caregivers as a result of ties formed through such organizations—as well as through informal means.
Second, the cross-sectional data limit our ability to make causal inferences. Reverse causality may be responsible for some of the found associations, as mastery may impact one’s parenting strain. Nevertheless, several pieces of empirical evidence give us greater confidence that our results are not simply attributable to reverse causality. We conducted random-effects analysis of variance for parenting strain and mastery to determine their respective between- and within-neighborhood variances. Mastery had significant between-neighborhood variation, but parenting strain did not. Furthermore, no other independent variable in our models (at the neighborhood and individual levels) significantly predicted parenting strain but did predict mastery in ways that are consistent with prior studies. Also, in terms of face validity, the wording of the parenting strain scale items requires respondents to consider past and current parenting experiences (i.e., the entire time of one’s “parenting experience”). By contrast, the mastery scale items are worded in a manner based on current perspectives. Collectively, these factors give us greater confidence that our model is correctly specified.
Third, limitations exist with the social capital and neighborhood attachment measures. Social support, social leverage, and neighborhood organization participation are represented by one item each. Few health studies, however, have examined these forms together, so even the limited measures available here contribute to the literature. Although more specific data on the type(s) and level(s) of neighborhood organization participation would have been ideal, this measure is still useful when aggregated to the neighborhood level, as neighborhood participation via formal groups provides resources that can be tapped by residents (Altschuler et al. 2004).
Although neighborhood attachment measured the extent of one’s neighborhood social ties, we were limited in assessing what proportion of respondents’ networks exists outside of the neighborhood. Thus, a resident with low neighborhood attachment could have the majority of her network living outside her neighborhood or could simply have few to no friends or family at all. Nevertheless, it can be argued that our findings reflect the presence of extraneighborhood ties. After all, it is difficult to conclude that all caregivers reporting low attachment have few to no family and friends.
Fourth, in terms of our analyses, our sample size as well as potential multicollinearity due to some correlated neighborhood-level variables may have limited our ability to detect some statistically significant associations. Also, although we control for numerous factors that might select one into a particular neighborhood, we cannot rule out the possibility that caregivers select where to reside partly on the basis of the attributes of neighborhoods we are studying, which might bias our findings. Fifth and finally, using census tracts as valid proxies for neighborhoods poses potential limitations. L.A.FANS’s 65 census tracts are within an urban county; hence, the sampled tracts have rather small geographic areas and, thus, are arguably more representative of actual neighborhoods compared to census tracts sampled from a more rural area. Despite these limitations, it is important to recognize that L.A.FANS represents one of the best U.S. data sets for studying issues related to neighborhood social capital.
Conclusion
In testing theoretically driven hypotheses regarding how neighborhood social capital moderates the impact of parenting strain on mastery among female caregivers of children, our study makes several contributions to furthering research. First, our findings contribute to a growing literature documenting “downsides” of social capital for health and well-being (e.g., Carpiano 2008; Moore et al. 2009). Population health research has tended to focus on the positive potential of social capital (Kawachi 2010). Our study suggests the need for more nuanced and critical considerations of social capital in terms of its potential deleterious effects and its potential limits for promoting well-being.
Second, our study rises to Robert et al.’s (2010) call for neighborhood health effects research to move beyond its predominant focus on the direct effects of structural conditions on individual-level health outcomes and also consider the role of personal capacity (agency) for maintaining or enacting changes to health practices within the context of structural conditions. In light of these issues, future health studies of neighborhood social capital need to examine such moderating effects for the influence of not only other personal circumstances and social roles on personal psychosocial resources, health practices, and health outcomes but also specific social capital forms and residents’ access to these forms. Doing so will facilitate improved understanding of how community life contributes to health inequalities.
Footnotes
Acknowledgements
The authors thank the editor and the three anonymous reviewers for their detailed and helpful comments during the review process.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Richard Carpiano coauthored this manuscript while receiving funding from Investigator Awards from the Michael Smith Foundation for Health Research and Canadian Institutes of Health Research. This study uses data from the Los Angeles Family and Neighborhood Survey (L.A.FANS), which is funded by Grant R01 HD35944 from the United States National Institute of Child Health and Human Development to RAND in Santa Monica, California. For further information on L.A.FANS, please visit ![]() .
.
Bios
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.