
Abstract
Prior research on the association of mental health and behavior problems with academic achievement is limited because it does not consider multiple problems simultaneously, take co-occurring problems into account, and control for academic aptitude. We addressed these limitations using data from the National Longitudinal Study of Adolescent Health (N = 6,315). We estimated the associations of depression, attention problems, delinquency, and substance use with two indicators of academic achievement (high school GPA and highest degree received) with controls for academic aptitude. Attention problems, delinquency, and substance use were significantly associated with diminished achievement, but depression was not. Combinations of problems involving substance use were especially consequential. Our results demonstrate that the social consequences of mental health problems are not the inevitable result of diminished functional ability but, rather, reflect negative social responses. These results also encourage a broader perspective on mental health by demonstrating that behavior problems heighten the negative consequences of more traditional forms of distress.
Sociologists maintain a long-standing interest in the social distribution of mental health problems. Literally hundreds of studies have been published on differences in levels of psychological distress or rates of psychiatric disorder based on gender, race-ethnicity, and socioeconomic status (see McLeod 2013 for a review). Although patterns are not always consistent, disadvantaged social statuses are generally associated with high levels of distress and high rates of disorder (Thoits 2010), confirming the strong mark that social organization leaves on our feelings and behaviors.
Despite the dominance of research on the mental health implications of social organization, studies of the social consequences of mental health problems contribute equally to the sociological mission. In contrast to clinicians and epidemiologists, who view social consequences as indicators of disorder severity (e.g., Kessler et al. 2005), sociologists consider social consequences to be evidence of stigma and social exclusion (e.g., Link et al. 1987, 1989). By invoking these concepts, sociologists reject the assumption that the social consequences of mental health problems follow necessarily from functional impairments in favor of the alternative that these consequences reflect fundamentally social processes.
Academic achievement is among the most thoroughly studied social consequences of mental health problems. Most studies come from outside the sociology of mental health, especially from sociology of education, social epidemiology, and developmental psychology (e.g., Campbell and von Stauffenberg 2007). These studies find that youth with mental health problems perform less well in school and attain lower levels of education than other youth. The association holds throughout the early life course—in elementary school (e.g., Alexander, Entwisle, and Dauber 1993; Farmer and Bierman 2002), in middle and high school (Fletcher 2010; McLeod and Kaiser 2004; Needham 2009), and into the postsecondary years (Hunt, Eisenberg, and Kilbourne 2010; Kessler et al. 1995; Miech et al. 1999; Needham 2009). It holds for multiple indicators of mental health problems, including internalizing and externalizing problems in young children (McLeod and Kaiser 2004), psychological distress and depression in preadolescents and adolescents (Needham, Crosnoe, and Muller 2004), and specific disorders such as attention deficit hyperactivity disorder (ADHD) (Galéra et al. 2009). It also holds for behavior problems that are closely associated with mental health, including delinquency and substance use (Lynskey and Hall 2000; Maguin and Loeber 1996; Staff et al. 2008). The consistency of the association across diverse mental health and behavior problems confirms their significance for attainment.
Despite many years of relevant research, empirical evidence for the association of mental health and behavior problems with academic achievement is limited in three key ways. First, few studies consider multiple problems simultaneously (Breslau 2010). Many youth experience more than one problem (Costello et al. 2003), which means that studies of single problems will produce biased estimates. Second, and related, even when they do consider multiple problems, studies have not determined whether some combinations of problems have stronger associations than others. To the extent that they do, estimates from studies that fail to take combinations into account may misrepresent the social consequences of mental health problems. Finally, many studies include only limited controls for academic aptitude, introducing ambiguity into the interpretation of the results. These limitations weaken our understanding of which problems matter most and why.
We address these limitations in our analysis by asking the following:
(1) Which mental health and behavior problems have the strongest associations with future academic achievement among adolescents, independent of academic aptitude?
(2) Which specific combinations of problems are most consequential for achievement?
We answer these questions using data from the National Longitudinal Survey of Adolescent Health, or Add Health, a prospective, longitudinal survey of U.S. adolescents. We rely on a broad definition of mental health and behavior problems and include in our analysis four types of problems that predict academic achievement: depression, attention problems, delinquency, and substance use. These problems cover the two major dimensions of emotional and behavioral problems: internalizing problems—inward-directed forms of distress such as depression and anxiety—and externalizing problems—outward-directed forms of distress such as conduct disorder and impulsive behavior. They also cover a range of “troubled and troubling” behaviors that are of concern to education scholars (Hobbs 1982). Sociologists who study the social distribution of mental health problems have argued for expanding the range of outcomes beyond depression and distress to ensure a comprehensive analysis of the consequences of social inequalities for well-being (Aneshensel, Rutter, and Lachenbruch 1991; Schwartz 2002). We advocate an equally expansive approach to the definition of mental health in analyses of social consequences.
Background
Do Social Consequences Differ Across Problems and Why?
The answers to our questions inform a long-standing debate in research on the social consequences of mental health problems: whether the consequences are attributable to functional impairments or to negative social responses. In mental health research, this debate is associated with labeling theory (e.g., Gove 1982; Scheff 1966). Labeling theory attributes the social consequences of mental health problems to the stigma of mental illness labels and the anticipation and experience of social rejection that follow (Link et al. 1987). Critics of labeling theory minimize the role of stigma and assert that the social consequences of mental health problems are attributable to the functional impairments, or symptoms, associated with the problems (Gove 1982).
Although the two sides of the debate are often presented as irreconcilable, the truth likely lies in between (Gove 2004). For example, in a sample of mental patients, Perry (2011) observed that symptoms of “behavioral and emotional excess” (e.g., delusions and hallucinations) elicited greater social rejection by acquaintances and strangers than symptoms of behavioral and emotional deficit (e.g., flat affect, anhedonia). In other words, even among persons who have been formally labeled, social responses depended on the specific nature of the impairment. In interactions with strangers and acquaintances, symptoms that were more overt and more disruptive to social interactions were associated with stronger negative responses.
The labeling theory debate resonates with research on the role of noncognitive traits in educational and occupational attainment. “Noncognitive trait” are productivity-related habits and traits that influence student success in formal educational settings, including aggressiveness, disruptiveness, emotional stability, self-discipline, effort, and self-esteem (see Farkas 2003 for a review). A central question in this line of research is whether noncognitive traits predict attainment independent of academic aptitude. To the extent that they do, theorists attribute the associations to subtle interactional and institutional processes that differentially value and reward student traits. Teachers prefer students who approach their work with positive attitudes, who are organized, and who are not disruptive in the classroom (Henricsson and Rydell 2004; Mullins et al. 1995; Murray and Murray 2004) and they give heavy weight to work skills and habits when evaluating student performance (Farkas 1996; Rosenbaum 2001). Beyond the classroom, schools reward students whose behaviors contribute to maintaining social order and punish students whose behaviors are disruptive or threatening (American Psychological Association Zero Tolerance Task Force 2008). In short, regardless of students’ abilities to achieve, students’ behaviors importantly determine their eventual attainments.
Although different in the specifics, labeling theory and theories of noncognitive traits share a common interest in the extent to which diminished social achievements result from functional impairments or from negative social responses. At the most basic level, we engage this issue by controlling academic aptitude—the most relevant indicator of impairment—throughout the analysis. Adolescents with high levels of depression, attention problems, and delinquency score lower on standardized achievement tests and tests of verbal and performance IQ than youth with low levels of problems (see Hinshaw 1992 and Roeser, Eccles, and Strobel 1998 for reviews). Finding that the associations of youths’ problems with academic achievement remain significant with controls for academic aptitude would strengthen our claim that the associations reflect more than functional impairments.
Our analysis of differences in the associations across types of mental health and behavior problems engages this issue at a deeper level. Following from Perry’s (2011) finding that different mental illness symptoms elicit different social responses in public settings, we hypothesize that different mental health and behavior problems elicit different responses in school settings. Theories of noncognitive traits imply that behaviors that signal a lack of interest in achievement and/or that are disruptive will elicit more negative responses than anxiety, passivity, and withdrawal. Because the behaviors associated with ADHD, delinquency, and substance use indicate disengagement and are more disruptive, we hypothesize that these problems will be more strongly associated with academic achievement than depression.
The few studies that have considered multiple types of problems simultaneously support this hypothesis. Attention problems, delinquency (or conduct problems), and substance use are more strongly associated with subsequent educational attainment than is depression (Hunt et al. 2010; Johnson et al. 1999; Miech et al. 1999). However, none of these studies included measures of all three types of externalizing problems so we do not know whether certain externalizing problems impede academic success more than others.
Distinguishing attention problems from other externalizing problems is especially important because their interpretation is more ambiguous. Although considered an externalizing problem by clinical and epidemiological researchers, attention problems have direct bearing on learning and could be considered an indicator of aptitude. In a comprehensive analysis of data from six longitudinal studies, Duncan and colleagues (2007) observed that attention skills affected later elementary test scores net of aptitude but that other mental and behavior problems did not. If their finding extends to older ages, it would imply that, contrary to theories of noncognitive traits, non-learning-related traits have little influence on achievement processes.
Do Some Combinations of Problems Matter More Than Others?
Our second research question extends our interest in different types of problems to ask whether there are specific combinations of problems that have especially strong associations with academic achievement. The experience of co-occurring problems is an important source of heterogeneity among youth with mental health and behavior problems. Drawing on data from the Great Smoky Mountains Study, Costello and colleagues (2003) reported that adolescents with ADHD were two to seven times more likely than other adolescents to meet criteria for a depressive disorder. ADHD also increased the risk of conduct disorder—the psychiatric analogue of delinquency—by a factor of three, and substance use disorders increased the risk of mood disorders and conduct disorder by that much or more (Costello et al. 2003; see Lewinsohn, Rohde, and Seeley 1995 for similar results). Evidence for the causal relationships reflected in these patterns is mixed, although it appears that the onset of ADHD and conduct problems precedes the onset of substance use and that depression precedes the onset of substance use, at least in boys (see Kessler 2004 for a review).
Accounting for combinations of problems in studies of academic achievement is important for empirical, practical, and theoretical reasons. Empirically, studies that fail to account for combinations of problems may underestimate associations because youth with the most consequential combinations are pooled with other youth in the estimates. Practically, knowing which combinations of problems are most strongly associated with academic failures informs interventions by identifying subsets of youth with greater need for services. Theoretically, knowing which combinations of problems matter most for academic achievement informs our evaluation of the relative importance of impairment versus social responses.
Clinical research suggests that youth who have more than one problem will face additional challenges in school simply because they are more impaired. For example, depressed youth who experience other mental health or behavior problems have more depressive episodes and use services at a higher rate than depressed youth who do not experience other problems (Rohde, Lewinsohn, and Seeley 1991). Global functioning also declines with increases in the number of problems youth experience (Lewinsohn et al. 1995). Finding that academic achievement declines with the number of problems regardless of which problems they are would suggest that increases in impairment are responsible for the association.
In contrast, theories of noncognitive traits imply that combinations of problems that involve delinquency and substance use will have especially strong associations with academic achievement because these problems are more likely to disrupt classrooms and generate punitive responses. Teachers judge oppositional behaviors as volitional and coercive, whereas they judge the behaviors associated with ADHD as involuntary (Lovejoy 1996). Although most substance use occurs off school grounds, substance use that does occur in school, particularly smoking, may also be interpreted by school personnel as evidence of a defiant attitude (Finn 2006). Finding that combinations of problems involving delinquency and substance use are more strongly associated with academic achievement than combinations of problems involving depression or attention problems would add support to explanations grounded in social responses.
In sum, the current study contributes to theory and research on the social consequences of mental health problems by estimating the associations of multiple problems with academic achievement simultaneously and by considering co-occurrences. The results of our analyses speak to a central debate regarding the relative importance of functional impairment versus social responses in those associations and, more generally, to theories of the role of noncognitive traits in attainment.
Data and Methods
The data for the analysis come from the National Longitudinal Study of Adolescent Health, or Add Health. The Add Health is a longitudinal survey study of the health and well-being of U.S. adolescents that follows youth from the middle and high school years through the transition to early adulthood. A stratified sample of 80 high schools and 52 middle schools was selected into the study in 1994. Seventh through 12th grade youth who attended those schools were invited to participate in an in-school survey (N = 90,118).
Of the youth who participated in the in-school survey, a randomly selected subsample of 20,745 participated in a subsequent Wave I in-home survey; an interview also was conducted with one of their parents. With the exception of the Wave I high school seniors, all respondents to the Wave I in-home survey were invited to participate in a Wave II interview approximately one year later (N = 14,738 completed interviews) and a third wave of data collection in 2001-2002 (N = 15,197). In 2008-2009, a fourth wave of data was collected from the original Wave I respondents (N = 15,701). We included in our analysis 9th through 12th graders from the Wave I in-home survey who were also interviewed at Wave IV and who had valid sampling weights (N = 6,315).
The sociodemographic profile of the sample highlights its representativeness. (See Appendix A in the online supplement [available at http://jhsb.sagepub.com/supplemental] for complete descriptive statistics.) Women comprised just over half the sample (54 percent), and whites were the majority racial-ethnic group (54 percent), with sizable samples of African American and Latino/Latina youth (19 percent and 17 percent, respectively) and of youth with other racial-ethnic identities (10 percent). Roughly 56 percent of youth lived with both biological parents and 25 percent with single parents at Wave I, comparable to national figures (Rawlings and Saluter 1995). Among the parents, 87 percent received a high school degree—also comparable to national figures (U.S. Census Bureau 1994)—and 34 percent received a college degree or higher.
Measures
Academic Achievement
We used two indicators of academic achievement as dependent variables: post–Wave I high school grade point average (GPA) and highest educational degree received. Our measure of post–Wave I high school GPA came from the Adolescent Health and Academic Achievement Study, a supplemental data collection that coded information from high school transcripts. Not all high school transcripts were coded, leaving a smaller sample for analyses of this outcome (N = 4,701). We used post–Wave I GPA rather than cumulative high school GPA because pre–Wave I GPA could be a cause, rather than a consequence, of Wave I mental health and behavior problems. Using post–Wave I GPA eliminates most of the 12th graders from the analysis of this outcome but does not affect our conclusions. 1 Analyses that used a measure of GPA for all of the high school years (and that included all 12th graders) produced comparable results.
Highest educational degree received was based on respondent reports given at the Wave IV interview. We collapsed the original 13-category variable into the following: received no degree (1), received GED or high school equivalency (2), received high school diploma (3), completed technical training (4), completed some college classes (5), received bachelor’s degree (6), or received higher degree (7). Although most people have completed their educations by their late 20s, some respondents may obtain more education in the future.
On average, this is a highly educated sample. The average highest degree received was 4.72, just below “some college.” The high levels of educational attainment are not surprising given that youth were recruited from schools. Nevertheless, some of these youth struggled academically. The average post–Wave I high school GPA was 2.55.
Mental Health and Behavior Problems
Unless otherwise noted, all measures of mental health and behavior problems were based on youth self-reports from the Wave I interview. To facilitate the analysis of combinations of problems, we constructed dichotomous measures for each type of problem. The pattern of main effects was the same for continuous versions of the variables.
Our measure of depression was based on a 19-item revision of the Center for Epidemiologic Studies-Depression Scale (Radloff 1977). 2 The items index physical and psychological symptoms associated with depressive disorders, such as “you didn’t feel like eating, your appetite was poor” and “you felt that you could not shake off the blues, even with help from your family and friends” (coded 0 = never or rarely during the past week to 3 = most of the time or all of the time during the past week). To compute a scale score, all available items were averaged for respondents who answered half of the items or more (α = .87 in this sample). We created a dichotomized measure of depression that represented youth with scores at or above the clinical cutoff (1.15 on the averaged scale; Roberts et al. 1990). Based on this measure, just over 10 percent of youth had high levels of depression, consistent with past epidemiological research (Lewinsohn, Rohde, and Seeley 1998).
Our measure of attention problems was based on retrospective reports of ADHD symptoms from the Wave III data collection. Respondents answered 18 questions about how often they engaged in ADHD-related behaviors when they were between 5 and 12 years of age (e.g., you fidgeted with your hands or feet or squirmed in your seat; 0 = never or rarely, 1 = sometimes, 2 = often, or 3 = very often). As with the measure of depression, we averaged reports across the items whenever the respondent had valid values on half of the items or more (α = .90 in this sample). The items in the scale were based on the SNAP-IV, an instrument designed to assess ADHD in children (Swanson 1992). Similar instruments, when used as retrospective reports, have shown adequate test-retest and internal consistency reliability as well as strong correlations with independent assessments of child behavior (e.g., Wierzbicki 2005). We dichotomized the measure of ADHD at the 80th percentile, which corresponded to a score of 1.11 (between “sometimes” and “often”). Supplemental analyses with a variable dichotomized at the 90th percentile produced substantively similar results (see endnotes). Although our cut point does not adhere to a clinical standard, high but subclinical levels of problems are associated with significant functional and social impairment (Angold et al. 1999).
Following Haynie (2001), we measured delinquency with an additive index based on youths’ self-reports of participation in 14 delinquent activities in the past year, each coded 0 (never) or 1 (one or more times). The items ranged from “painted graffiti” to “shot or stabbed someone.” We dichotomized the index at the 80th percentile to identify youth who were engaged in the very highest levels of delinquency (zero to three vs. four or more). (The endnotes describe results for a 90th percentile measure.)
Our measure of substance use was based on youths’ responses to a comprehensive series of questions about alcohol use (getting “drunk or ‘very, very high’”) in the past 12 months and about cigarette smoking and marijuana and other illicit drug use in the past 30 days. Following Nonnemaker, McNeely, and Blum (2003), for each type of substance, we created dummy variables that distinguished youth who regularly used any of the substances from those who did not. 3 In addition, because some studies have found that cigarette use is more strongly associated with educational attainment than other types of substance use (see Breslau 2010 for a review), we present supplemental results for a disaggregated measure of substance use. The rate of regular substance use in the sample was 23 percent, with 14 percent of youth reporting regular cigarette use, 11 percent regular alcohol use, and 8 percent regular use of other drugs.
Combinations of Problems
Based on the dummy variables for specific mental health and behavior problems, we created a set of mutually exclusive dummy variables to represent specific combinations: for example, depression alone, attention problems alone, depression and attention problems. Although functionally equivalent to constructing multiplicative interactions among the dichotomous indicators, this coding strategy avoids multicollinearity and, when coupled with post-estimation contrasts, facilitates comparisons across all the different possible combinations of problems. The rates of specific combinations of problems were low, but the rates of combined problems overall were high. Roughly 29 percent of youth experienced any of the mental health problems alone, ranging from a low of 4 percent for depression to a high of 10 percent for attention problems. Roughly 20 percent of youth experienced more than one problem, ranging from a low of 0.5 percent for depression-attention problems-delinquency to a high of 4.6 percent for depression and substance use. (See Appendix A online for details.)
Academic Aptitude
We assessed academic aptitude with Wave I standardized vocabulary test scores (range = 14-149, M = 101.39) and a variable based on parents’ reports of whether the youth had a learning disability or received special education services during the 12 months prior to the Wave I parent interview (1 = yes, 0 = no, M = 0.13). 4
Social Background
Mental health problems and low academic achievement are more common among children from lower socioeconomic groups and from single-parent households (Bradley and Corwyn 2002; Pallas 2003). To account for potential spuriousness, we controlled the following Wave I variables in all models: gender, race, whether the youth’s family received public assistance, highest level of parental education, family income, and family structure. We also controlled for grade level and the youth’s age because potential educational attainment is higher for the older students in the sample.
Analytic Strategy
We used regression models tailored to the two dependent variables: ordinary least squares for high school GPA and ordinal logistic for highest degree received. We began with models that included dichotomies for mental health and behavior problems along with controls for academic aptitude and social background, and then we ran models that included the full set of dummy variables for specific combinations of problems.
Although there were few missing values for most of the analysis variables, three variables were missing for more than 10 percent of the sample: family income (23 percent missing), public assistance receipt (13 percent missing), and special education/learning disability (12 percent missing). These variables came from the parents’ interviews and were missing when parents did not participate or did not report the information. To preserve cases for the analysis, we estimated models using the ICE (Imputation by Chained Equations) and MICOMBINE multiple imputation procedures in STATA 11.1 (Royston 2005a, 2005b). 5 Together, these procedures generated 15 data sets—each with a different set of missing data imputations. We estimated the models within each data set and combined the results to yield a single set of parameter estimates. 6
Results
We began by predicting high school GPA and highest degree from the indicators for specific mental health and behavior problems, with controls for social background and academic aptitude. For each outcome, we estimated models that included each mental health or behavior problem alone followed by models that included all problems together. Coefficients for the control variables are omitted for parsimony of presentation.
According to Table 1, attention problems, delinquency, and substance use all were associated with lower high school GPA whether considered alone or simultaneously. In contrast, depression was only significantly associated with high school GPA in models that did not include the other problems. The associations of mental health and behavior problems with high school GPA were strong in terms of statistical significance and modest in magnitude. Based on Model 5 in Table 1, youth with high levels of attention problems had GPAs that were .14 points lower on average than youth who did not, roughly 16 percent of a standard deviation; the difference between youth who did and did not have high levels of delinquency (b = −.15) was of the same magnitude 7 ; the difference based on regular substance use was a little more than twice as large (b = −.34). The final model disaggregates the substance use measure by type of substance: cigarette, alcohol, and other drugs (including marijuana). Cigarette and alcohol use were both significantly associated with lower GPA, but the difference for cigarette use was about three times as large.
Coefficients from Regressions of Academic Achievement on Specific Problems
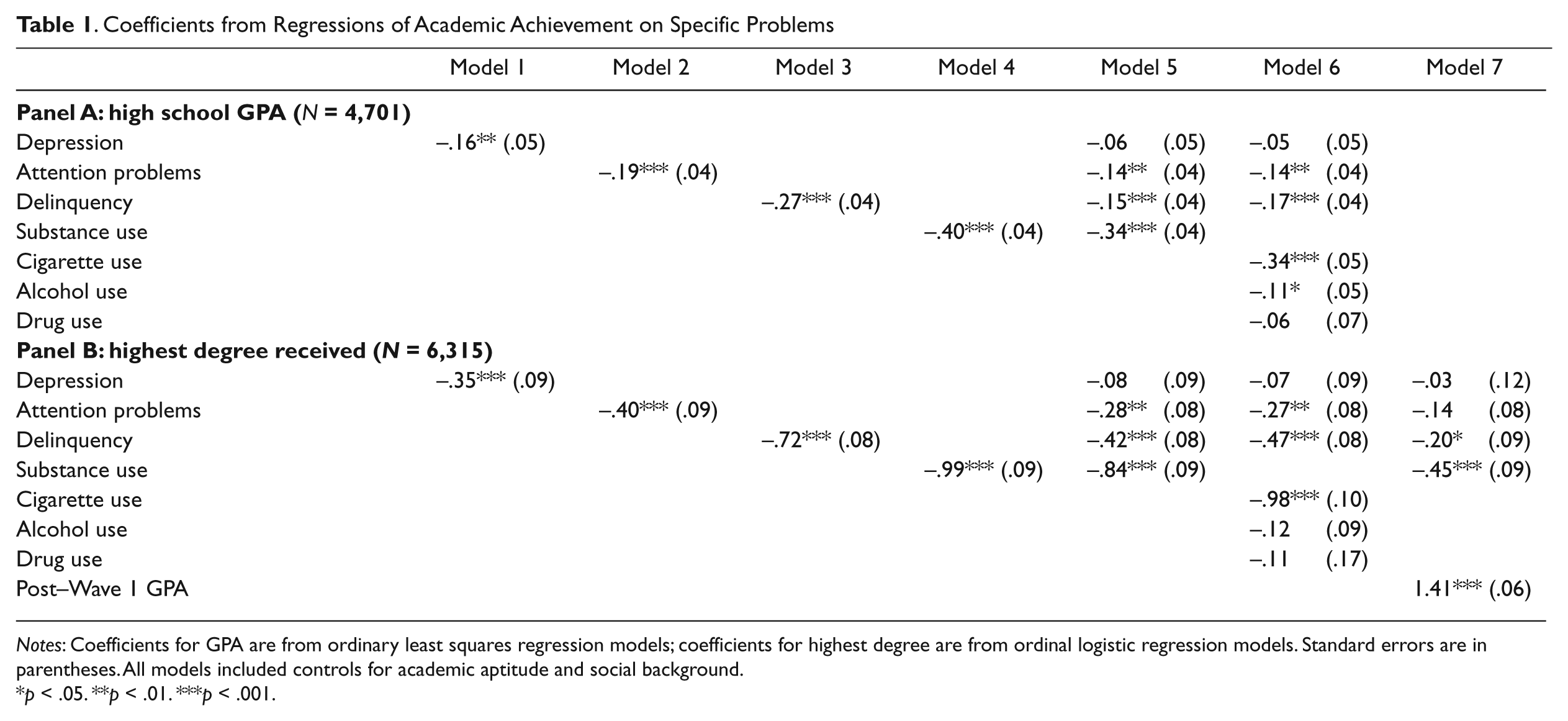
Notes: Coefficients for GPA are from ordinary least squares regression models; coefficients for highest degree are from ordinal logistic regression models. Standard errors are in parentheses. All models included controls for academic aptitude and social background.
p < .05. **p < .01. ***p < .001.
Although the coefficients for the control variables are not included in the table, many were roughly the same size as those for mental health and behavior problems. For example, the coefficient for youth living in a single parent household was −.17, for those receiving public assistance was −.16, and for black versus white race was −.15—about the same size as for attention problems and delinquency. The coefficients for other common predictors of academic achievement, including special education/learning disability status (b = −.22) and having a parent who attained a college education or more (b = .29), were smaller than those for substance use. Thus, although the associations for mental health and behavior problems were modest, they were comparable to those for other major sociodemographic predictors.
The results for highest degree received closely paralleled those for high school GPA. Depression, attention problems, delinquency, and substance use all were associated with receiving a lower degree when considered alone. The association of depression with highest degree became nonsignificant when the other problems were included in the model. Exponentiated coefficients provide estimates of the odds of receiving the next highest degree with a one-unit increase in the independent variable, in this instance, the shift from having a low to a high value on the dichotomous indicators for mental health and behavior problems. For attention problems, having a high versus low level of problems was associated with .76 (e−.28) times the odds (i.e., 24 percent lower odds) of receiving the next highest degree. The comparable odds for delinquency and substance use were .66 (e−.42) and .43 (e−.84), respectively. 8 When we disaggregated the substance use measure by type (Model 6), cigarette use was the only type of substance use that was significantly associated with highest degree. Youth who smoked regularly had .38 times the odds of receiving the next highest degree.
One could argue for including high school GPA as a control in the models for highest degree received because it captures student performance ability. We did not include it in our initial models, because although GPA is a function of student performance, it also is a function of student motivation, teachers’ expectations for student performance, and teachers’ evaluations of student behavior (Farkas 1996; Hamre and Pianta 2001). To the extent that GPA reflects motivations, expectations, and evaluations, controlling for GPA controls for part of the process through which youth problems affect achievement. Nevertheless, to provide the most conservative estimates, we estimated an additional model with GPA added (Model 7 in Panel B of Table 1). The coefficients for delinquency and substance use were reduced by about half but remained significant, and the coefficient for attention problems became marginally significant (p = .093). Thus, even with the most stringent controls for academic aptitude, behavior problems had significant associations with educational attainment. 9
Specific Combinations of Problems
The next set of models takes us to our second research question: the role of combinations of problems in academic achievement. Our initial models may misrepresent the associations of problems with academic achievement if some combinations of problems are more consequential than others.
The left panel of Table 2 presents coefficients for models predicting high school GPA from specific combinations of problems, with controls for academic aptitude and social background. The variables for each specific problem represent youth who experienced that problem alone; the other variables represent youth who experienced specific combinations of problems (e.g., Dp-A = depression and attention problems). We did not estimate models for combinations involving the disaggregated measure of substance use as the sample sizes were prohibitively small.
Coefficients and Predicted Values from Regression of High School GPA on Combinations of Problems
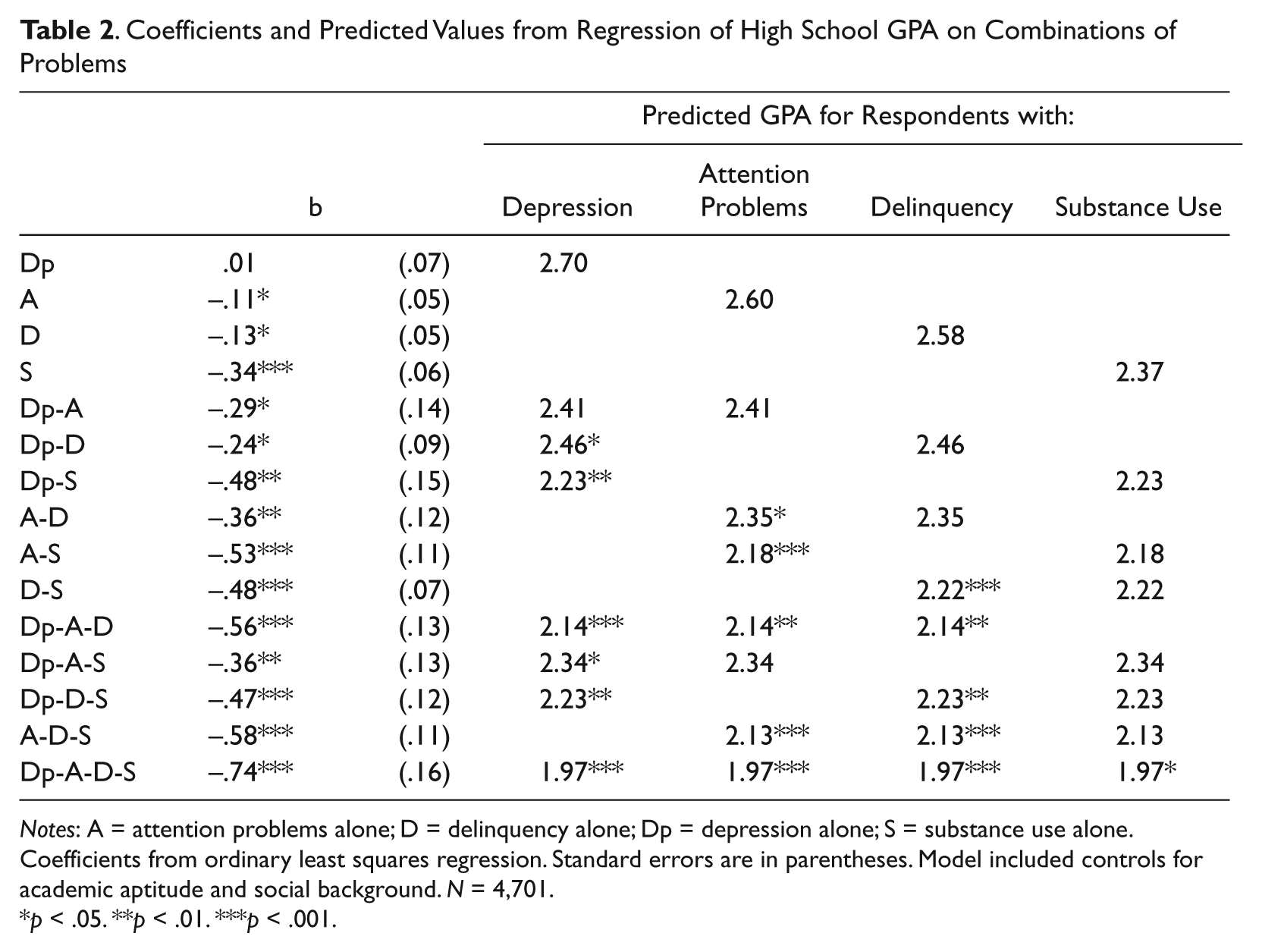
Notes: Dp = depression alone; A = attention problems alone; D = delinquency alone; S = substance use alone. Coefficients from ordinary least squares regression. Standard errors are in parentheses. Model included controls for academic aptitude and social background. N = 4,701.
p < .05. **p < .01. ***p < .001.
With the exception of youth who only experienced depression, youth who experienced every other problem, alone or in combination, had lower average GPAs than youth without any problems. This indicates that depression in and of itself is much less consequential for academic achievement than are behavior problems.
The right panel of Table 2 presents predicted GPAs for youth with specific combinations of problems, along with the significance of post-estimation tests that compared the coefficients for youth with only one problem to those with combinations involving that same problem. For example, the significance level for Dp-D in the first column of the right panel represents the significance of the difference in the coefficients for the Dp-D versus Dp groups. We estimated the significance of the comparisons for all groups but only present the comparisons in “nested” groups, that is, Dp versus Dp-A and Dp versus Dp-A-D but not Dp-A versus D-S.
Our results support three main conclusions. First, according to the coefficients, attention problems, delinquency, and substance use were associated with earning a lower GPA but depression was not. Even in the absence of additional problems, youth who experienced any one of the externalizing problems had diminished achievement. Second, according to the post-estimation comparisons, youth who experienced combinations of problems generally had lower GPAs than youth who experienced only one problem, although the magnitude of the difference varied. Youth with depression who experienced other problems had lower GPAs than youth who experienced depression alone: the predicted GPA for youth with depression was 2.70 whereas that for youth with depression and delinquency was 2.46 and that for youth with depression and substance use was 2.23. Youth with attention problems who also experienced delinquency and substance use had lower GPAs than youth with attention problems alone. Youth with delinquency had lower GPAs when they also experienced substance use but not when they experienced depression or attention problems. In addition, adding depression, attention problems, or delinquency did not significantly diminish the low GPAs associated with substance use. These results confirm that depression did not increase the educational risk associated with other problems and that substance use had the most consistent association with academic achievement.
Third, although not immediately obvious from this table, youth with three or more problems generally did not have significantly lower GPAs than did youth with two problems. Indeed, with one exception, post-estimation comparisons revealed no significant differences in GPA for youth with two versus three problems. (The exception was for youth with depression, attention problems, and delinquency [Dp-A-D] who had significantly lower GPAs than youth with depression and delinquency [Dp-D; p = .03]). Some of the absence of difference can be attributed to small sample sizes but some reflects a true absence of meaningful differentiation. A quick glance at the predicted GPAs across the groups indicates that although there are differences, the differences do not follow an obvious pattern with respect to the number of problems youth experienced. Some predictions in the two-problem combinations were lower than those in the three-problem combinations and vice-versa. The predicted GPA for the group with all four problems was lower than for all others but, based on post-estimation comparisons, was not significantly different on a consistent basis. 10
Comparable results for highest degree received are presented in Appendix B online. We did not include high school GPA as a control in the model based on the reasoning given earlier: GPA may mediate the associations of youth mental health and behavior problems with educational attainment. 11
The three main conclusions from the analysis of high school GPA held for highest degree received, but some of the specific results differed. First, as for GPA, delinquency (b = −0.47, p < .01) and substance use (b = −0.83, p < .001) were associated with receiving a lesser degree and depression was not (b = −0.08, p = .64). However, unlike for GPA, attention problems were not associated with highest degree received either (b = −0.21, p = .10). This suggests that attention problems alone matter less for educational attainment than they do for high school performance. Second, youth who experienced more than one problem generally achieved a lower degree than youth who experienced only one problem. As for GPA, adding depression did not significantly diminish attainment for youth with other problems and adding substance use did. However, unlike for GPA, attention problems were associated with lower educational attainment for youth with depression and substance use, and delinquency was not associated with diminished educational attainment for youth with depression or attention problems. This suggests that co-occurring attention problems heighten the risk of low attainment associated with other problems. Third, having three or more problems was not associated with significantly lower attainment than having two problems.
Discussion
Our analysis addressed two key questions for research on the association of mental health and behavior problems with academic achievement: Which specific problems most strongly predict academic achievement? Are certain combinations of problems more consequential than others? We found that attention problems, delinquency, and substance use were more strongly associated with achievement than was depression and that youth who experienced two or more problems earned lower GPAs and attained lower levels of education than youth who experienced only one problem. More specifically, having an additional externalizing problem—especially substance use—was associated with a significant decline in GPA and attainment. The associations were independent of academic aptitude, lending credence to the general conclusion that mental health and behavior problems are important determinants of status attainment outcomes (Farkas 2003).
Our results confirm previous evidence that regular substance use is associated with diminished academic achievement (e.g., Breslau et al. 2008; Ellickson et al. 1998; Lynskey and Hall 2000; Newcomb et al. 2002). Although many studies that evaluate the association of substance use with academic achievement do not consider multiple substances simultaneously, those that do support our finding that cigarette use is the strongest predictor (Breslau 2010). Why cigarette use is so consequential has not yet been established. One obvious explanation—that the association is spurious due to social background, risk propensity, cognitive impairment, or behavioral disinhibition—has been disconfirmed (Lynskey and Hall 2000; Staff et al. 2008). Another explanation attributes the association to diminished academic motivation, especially as reinforced by deviant peer associations (Breslau 2010). However, in our analysis of highest degree received, we controlled GPA, a reasonable if imperfect proxy for motivation, and observed significant residual effects of cigarette use. We propose an alternative: that cigarette use is more likely to elicit strong negative sanctions from school authorities and that these sanctions diminish attainment. According to the National Center on Addiction and Substance Use (2011), most schools respond to substance use punitively rather than therapeutically (American Psychological Association Zero Tolerance Task Force 2008). Because youth are more likely to smoke cigarettes at school than they are to use alcohol (Finn 2006), the effect of punitive disciplinary policies would be especially pronounced for that substance (McNeely, Nonnemaker, and Blum 2002).
We also observed that delinquency was negatively associated with GPA and educational attainment whether considered alone or in combination with other problems. Research on delinquency and academic success typically assumes that poor academic performance predicts future delinquency (Maguin and Loeber 1996). Because our measure of delinquency was taken prior to the measures of academic achievement, our analysis provides strong evidence for the reverse. Further strengthening our conclusion, the association of delinquency was independent of attention problems—a commonly discussed precursor of both delinquency and poor academic performance (Satterfield, Hoppe, and Schell 1982).
Previous evidence for the association of depression with academic achievement is both more limited and more mixed. Major epidemiological surveys find that early-onset depression is not associated with subsequent educational attainment independent of other mental disorders (e.g., Breslau et al. 2008; Miech et al. 1999). In contrast, studies using the Add Health report a significant effect of adolescent depression on high school completion and college entry (Fletcher 2008; Needham 2009). Our analyses establish that the discrepancy is attributable to our controls for other mental health and behavior problems: We observed a significant effect for depression that became nonsignificant with controls for other problems. For scholars interested in the reciprocal associations between social disadvantage and psychological distress (for which depression is a common indicator), the most important implication of our results is that the causation runs predominantly from disadvantage to distress rather than the reverse. That the same is not true for more disruptive problems highlights the need for a more differentiated framework for the associations of mental health and behavior problems with social attainments.
Such a framework could begin with the debate that motivated our analysis: whether the social consequences of mental health problems are the inevitable result of functional impairments or whether they depend on negative social responses. Three findings support the latter position. First, we observed significant associations independent of academic aptitude (and, for substance use and delinquency, independent of attention problems). Second, problems that disrupt activities, challenge teacher authority, and are likely grounds for punitive action—especially delinquency and substance use—were more strongly associated with academic achievement than depression. Third, although youth who experienced multiple problems achieved less academically than youth who experienced only one problem, academic achievement did not decline consistently with the number of problems. Together, these findings provide strong evidence that impairments associated with behavior problems are not the sole determinants of their negative social consequences. In the case of highest degree received, the learning impairments associated with attention problems do appear to increase the risk of low attainment associated with other problems, but attention problems alone are inconsequential.
Beyond its contributions to this debate, our analysis carries lessons for sociologists of mental health and stratification researchers. For sociologists of mental health, our results suggest the value of incorporating a broad array of emotional and behavioral dysfunctions into our analyses, consistent with the practice of developmental scholars (Achenbach et al. 1981). Sociologists of mental health have tended to maintain a narrow focus on “distress,” often as represented by depression. Some scholars conceptualize substance use as a “masculine” expression of distress analogous to depression (e.g., Aneshensel et al. 1991), but others assert that substance use represents “bad behavior” rather than distress (Mirowsky and Ross 1995). Delinquency and other threatening behaviors have receive comparatively little attention (Schwartz 2002; Umberson, Williams, and Anderson 2002). Our results demonstrate that even if distinct from “distress,” substance use and delinquency are important components of the complex problems youth experience in the real world (Mirowsky and Ross 2002) and that they have profound social consequences.
For stratification researchers, our analysis demonstrates that the thoughts, feelings, and behaviors that characterize mental health and behavior problems are relevant to how adolescents fare in the educational system. Most research on noncognitive traits focuses on conscientious work habits, self-confidence, and the like. Although there is direct evidence for teachers’ differential evaluations of these traits (Farkas 2003), less is known about how teachers evaluate mental health and behavior problems. As the effect sizes for these problems are greater than or equal to those for traditional predictors of academic achievement, they deserve greater attention from stratification researchers.
We acknowledge three features of our analysis that limit our conclusions. First, we did not have access to formal diagnostic measures. Although our dichotomized indicators captured high levels of problems, the associations we observed might be stronger for problems that meet diagnostic criteria for major mental disorders (Breslau 2010). Second, we lacked information on academic achievement in earlier grades. The process we observed may have begun much earlier in youths’ educational careers, driven either by the effects of early mental health problems on later academic achievement or the effects of early academic failures on later mental health problems (Roeser et al. 1998). Consistent with the latter possibility, some research indicates that youth initiate cigarette use as a means of coping with poor achievement (Schulenberg et al. 1994). Third, the causal sequence among the co-occurring problems youth experienced remains uncertain. Co-occurring substance use could represent a coping response for youth with depression or attention problems. If so, models that include substance use would underestimate the effects of other problems because they control for the mediational process that produces their effects. Arguing against this possibility, depression and attention problems were more weakly associated with academic achievement even before the control for substance use was introduced. Nevertheless, knowing more about the origins of co-occurring problems would deepen our understanding of how mental health and behavior problems come to affect achievement.
Despite these limitations, our analysis advances research on the social consequences of mental health problems in three important ways: by highlighting the special relevance of disruptive problems within school settings; by demonstrating that youth with co-occurring problems face more academic challenges than other youth; and by providing evidence that although abilities powerfully shape future attainments, so too do subtle evaluative processes.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant R01 HD050288 from the National Institute of Child Health and Human Development.
Notes
Bios
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.