
Abstract
Despite the proliferation of studies documenting the relationship between physical limitation and depressive symptoms in the United States, we currently do not know (1) whether physical impairment is associated with other dimensions of emotional well-being and (2) if these associations differ for men and women as well as married and nonmarried adults. We use panel data from two national samples to examine gender and marital status variations in the impact of physical limitation on four indicators of mental health. We find that physical limitation is associated with increases in depressive symptoms and negative feelings as well as decreases in positive emotions. Although the patterns are complex, we also find gender and marital status differences in these associations. Our results provide additional support for Aneshensel’s (1992; Aneshensel, Rutter, and Lachenbruch 1991) argument about the highly contingent nature of stress reactivity and contribute to theory about both gender and marital status differences in the impact of stress on mental health.
A by-product of the increase in longevity over the 20th century that has received considerable research attention is the rise in the population of physically limited adults in the United States. Given the difficulty they have performing activities of daily living and their dependence on others for social support, it is not surprising that studies find physical limitation to be a significant stressor in the lives of individuals, which puts them at elevated risk for depression (Turner and Noh 1988; Yang 2006). However, while researchers have identified psychosocial factors that both mediate and moderate the relationship between physical limitation and depressive symptoms, two important gaps exist in current knowledge about this growing population of adults.
The first is that we do not know whether physical limitation is associated with other dimensions of mental health, such as alcohol use/dependence or the frequency of negative and positive emotions. The near-exclusive focus on depressive symptoms limits our understanding of the various ways in which physical limitation influences adults’ emotional well-being. The second gap is that we do not know whether the association between physical limitation and mental health differs for men and women as well as married and nonmarried adults. The absence of research on gender and marital status variations in the physical limitation-mental health relationship impedes our understanding of whether these two major adult social statuses moderate the emotional impact of this particular source of chronic stress.
Drawing on Aneshensel’s (1992; Aneshensel, Rutter, and Lachenbruch 1991) theoretical argument about the highly contingent nature of stress reactivity, we investigate gender and marital status variations in the association between physical limitation and four indicators of emotional well-being. We examine several dimensions of mental health in order to obtain a broader perspective of the ways in which physical impairment influences the emotional lives of individuals as well as to capture gender and marital status differences in emotional reactions to this source of stress. This topic is not only timely but important on theoretical grounds; in addition to shedding more light on the highly contingent nature of stress reactivity, our paper contributes to theory about both gender and marital status differences in emotional reactions to life stress—particularly, the stress associated with challenges to one’s physical ability and independence.
Background
Physical Limitation and Mental Health
According to the U.S. Department of Health and Human Services (2009), 14 percent (or one in seven) adults have physical difficulties that substantially limit their ability to perform activities of daily living. Although increases in physical limitation are part of the aging process (Verbrugge and Jette 1994), research shows that they interfere with the ability to perform social roles, limit social interaction, and reduce involvement in the community—effects that are associated with decreased social integration and increased loneliness (Russell 2009; Waite and Hughes 1999). The stigma of physical limitation and dependence on others for help with day-to-day activities and emotional support also threaten self-concepts (Turner and Noh 1988; Yang 2006), an unsurprising finding in light of the value placed on self-reliance in American culture.
Several studies have examined the mental health of physically limited adults. This research focuses on symptoms of depression and finds that physically limited persons report significantly more symptoms than nonlimited persons (Gayman, Turner, and Cui, 2008; Turner and Noh 1988; Yang and George 2005). While scholars debate the causal direction of the physical limitation-depression relationship, there is evidence that the depressing effect of disability is greater than the disabling effect of depression (Kennedy, Kelman, and Thomas, 1990; Ormel et al. 2002).
Based on insights from the stress process perspective (Pearlin 1989), mental health researchers now consider physical limitation to be a major chronic stressor in the lives of adults and have turned their attention to identifying social factors that influence its emotional impact. Studies indicate that psychosocial resources both mediate and moderate the relationship between physical limitation and depression. Low sense of control and self-esteem as well as decreased perceptions of social support—more common among physically impaired people—help explain the association between physical limitation and depressive symptoms; physically limited adults who possess greater resources also report fewer symptoms than physically limited adults who possess fewer resources (Bierman and Statland 2010; Turner and Noh 1988; Yang 2006).
Despite the proliferation of studies identifying psychosocial resources that influence the relationship between physical limitation and depressive symptoms, researchers have not examined whether physical impairment is associated with other dimensions of emotional well-being. The lack of attention to other mental health outcomes is surprising in light of the large body of research documenting an association between exposure to stress and a wide array of emotional problems (Simon 2002; Thoits 1983). Researchers have also not examined whether this association differs for men and women or for married and nonmarried adults. The lack of research on this issue is also surprising since a substantial body of work indicates that gender and marital status are two major adult statuses that moderate the emotional impact of life stress.
The Contingent Nature of Stress Reactivity
It is now 20 years since the publication of Aneshensel’s (1992; Aneshensel, Rutter, and Lachenbruch 1991) seminal theoretical argument about the highly contingent nature of emotional distress and stress reactivity. According to Aneshensel, although stressful life experiences often have deleterious consequences for individuals, the impact of stress on well-being depends on the type of stressor involved, social characteristics of persons, and mental health problem considered. A premise of her argument is that the impact of stress is not limited to any specific mental health problem per se (e.g., depression) and that members of various social groups differ in their dominant modes of expressing distress. Another premise of her argument (and sociological stress theories) is that the larger structural and cultural context in which individuals are embedded renders members of some social groups more vulnerable than others to the adverse emotional consequences of stress.
Aneshensel’s theoretical insights provide a useful framework for assessing gender and marital status differences in the relationship between physical limitation and various dimensions of emotional well-being. Theory and research on gender, marital status, and mental health provide insight into how and why these major adult statuses moderate the emotional impact of this particular source of stress.
Gender Differences in Stress Reactivity
Mental health scholars have long theorized about gender differences in distress and emotional reactions to stress. In sharp contrast to earlier theoretical claims that women’s insufficient psychosocial resources render them more vulnerable than men to the emotional effect of stress in general (Kessler 1979; Pearlin and Schooler 1978), a substantial body of research indicates that some stressors are more distressing for women while others are more distressing for men. Women tend to be more reactive to family-related stress and events that negatively affect others, whereas men tend to be more reactive to employment-related stress and events that negatively affect themselves (Conger et al. 1993; Kessler and McLeod 1984; Simon 1998; Simon and Lively 2010; Turner and Avison 1989). These findings have led scholars to conclude that stressors do not have the same meaning and significance for women and men. To account for gender differences in stress reactivity, Thoits (1995) and Simon (1992) suggest that stressors that threaten people’s valued identities are more distressing than identity-irrelevant stressors.
There is, however, also evidence that the impact of other types of stressors does not differ for men and women when male and female types of mental health problems are considered. While women tend to respond to divorce and widowhood with symptoms of depression, men tend to respond to these same stressors with substance use/abuse (Horwitz, White, and Howell-White 1996; Simon 2002; Umberson et al. 1996; Williams 2003). These findings are consistent with epidemiological studies documenting females’ higher rates of internalizing problems, such as depression, and males’ higher rates of externalizing problems, such as substance use/dependence (Kessler et al. 1994). They have also led to the conclusion that studies focusing exclusively on depressive symptoms overestimate women’s vulnerability to stress and underestimate men’s.
This research suggests that the association between physical limitation and mental health may not differ for men and women when gendered expressions of distress are considered; physical impairment may be associated with symptoms of depression among women and substance problems among men. Insofar as this is the case, the association between physical limitation and the frequency of positive and negative emotions may not differ for women and men. At the same time, this research also points to two contrasting hypotheses regarding gender differences in emotional reactions to the stress associated with physical limitation.
Gender Variation in the Association between Physical Limitation and Mental Health
The first hypothesis is that the association between physical limitation and emotional well-being is greater for men than women. Gender and masculinity scholars have long argued that cultural norms about the importance of self-reliance throughout the 20th century in the United States are greater for males than for females (Connell 2005; Kimmel 2005; Ridgeway 2011). Coming of age in a context that equates masculinity with self-reliance, current cohorts of men’s adult roles are based on the enactment of this ideal. Since physical limitation increases dependence on others for help with daily activities and emotional support, it may be emasculating and subsequently more harmful for men’s self-conception and emotional well-being than for their female counterparts. There is indirect support for this hypothesis; although they did not examine mental health per se, qualitative studies show that chronic illness and physical disability threaten men’s identity as self-reliant (Charmaz 1994; Gershick and Miller 1995; Ostrander 2008).
The second hypothesis is that the association between physical limitation and emotional well-being is greater for women than for men. Gender and feminist scholars argue that providing care to others is a cultural ideal for women in the United States (Cancian and Oliker 2000; Ridgeway 2011). Raised in this context, current cohorts of women’s adult roles are based the enactment of this ideal. Because physical limitation impedes not only one’s capacity to care for self but also the ability to care for others, it may undermine women’s self-conception as caregiver and take a greater toll on their well-being than that of their male peers. Most studies that bear on this issue focus on the mental heath of women caring for a family member (rather than being cared for) and are part of a larger body of research on the costs of “care-work” performed by women (Barusch and Spaid 1989; England and Folbre 1999). However, a recent qualitative study of women with breast cancer provides preliminary support for this hypothesis; Sulik (2007) finds that having to put their own needs for care before the needs of others threatens women’s identity as caregiver.
Marital Status Differences in Stress Reactivity
Mental health scholars have also theorized about marital status differences in distress and vulnerability. Although earlier studies focused on depressive symptoms, a large body of work finds that married men and women report higher levels of well-being than their nonmarried counterparts across several dimensions of mental health, including symptoms of depression, substance use/dependence, and the frequency of positive and negative emotions (Horwitz, White, and Howell-White 1996; Simon 2002; Simon and Nath 2004; Umberson et al. 1996; Williams 2003). Some researchers attribute married persons’ higher level of emotional well-being to their greater resilience to the deleterious effects of stress. Kessler and Essex (1982) argued that married adults have more psychosocial resources, which renders them less vulnerable than nonmarried people to the emotional impact of stress. And drawing on insights from symbolic interaction, Thoits (1986) argued that marriage provides purpose and meaning in life and an important identity, which also buffer the mental health impact of stress. Numerous studies find that married men and women are less vulnerable than their nonmarried counterparts to the emotional impact of undesirable life events (Kessler and Essex 1982; Thoits 1986) and ongoing strains (Pearlin and Johnson 1977; Simon 1998).
However, while this research documents that marriage reduces the negative emotional impact of a variety of acute and chronic stressors, physical limitation may not be less distressing for married than for nonmarried adults. Studies also find that the mental health advantage of marriage is only evident when spousal support is high and spousal strain is low (Umberson et al. 1996; Williams 2003). This finding suggests that the degree to which marriage moderates the physical limitation-mental health association may depend on the quality of the marriage. This literature suggests two contrasting hypotheses regarding marital status differences in vulnerability to the stress associated with physical limitation.
Marital Status Variation in the Association between Physical Limitation and Mental Health
The first hypothesis is that the negative association between physical limitation and emotional well-being is weaker for married than for nonmarried adults. The emotional security of having an intimate partner—who can assist with day-to-day activities and provide emotional support—may increase feelings of social integration and self-worth among married persons with physical limitations relative to their nonmarried counterparts. Extending Kessler and Essex’s (1982) argument, these psychosocial resources may buffer the impact of physical limitation on their mental health. By increasing their sense of purpose and meaning, the spousal identity may also increase married people’s resilience to the emotional impact of this source of stress, as Thoits (1986) suggests. Indirect support for this hypothesis comes from a recent study, which finds that physically limited people who are married are less lonely than their nonmarried peers (Russell 2009). Another recent study (Yorgason, Booth, and Johnson 2008) reports increases in marital happiness among men and women following the onset of their disability. One spouse’s physical limitation may also trigger dyadic coping efforts that reduce the emotional impact of this source of stress (Berg and Upchurch 2007).
The second hypothesis is that the negative association between physical limitation and emotional well-being is greater for married than for nonmarried adults. Married people’s dependence on their spouse for help with activities of daily living and emotional support may increase marital strain—an additional source of stress to which their nonmarried counterparts are not exposed. The loss of competencies may also interfere with their ability to perform marital roles and, in doing so, decrease marital equity and increase feelings of resentment, anger, guilt, and shame. To the extent that these negative marital processes operate, marriage may exacerbate the negative emotional impact of physical limitation. There is indirect support for this hypothesis; Booth and Johnson (1994) found that challenges to marital role performance contribute to lower levels of marital quality among less healthy compared to healthier adults.
In the following section, we examine whether physical limitation is associated with symptoms of depression and alcohol use/dependence as well as the frequency of negative and positive emotions in two national data sets. We also investigate gender and marital status differences in the association between physical limitation and these indicators of mental health.
Data and Methods
Data
The first data set we use is the National Survey of Midlife Development in the United States (MIDUS), a two-wave panel study developed to assess stress, social relationships, and health among adults in midlife (for details, see Brim et al. 2007). A representative sample of 3,032 adults between 25 and 74 years participated in a mailed questionnaire in 1994-1995. Ten years later, 1,748 of these respondents completed a second questionnaire, resulting in a response rate of 57 percent for the panel after adjusting for mortality (Ryff and Davidson 2010). Analyses reported elsewhere (Radler and Ryff 2010) indicate that attrition was higher among male, nonwhite, younger, less educated, and unmarried persons. Our attrition analyses also indicated that people who reported poorer physical health and physical limitations at Wave I were more likely to leave the study by Wave II. This panel may, therefore, overrepresent married and physically healthier adults.
This data set is ideal because physical limitation increases with the aging process and older adults were oversampled at Wave I. MIDUS also includes four indicators of emotional well-being. Since racial and ethnic minorities were not oversampled at Wave I, only 7 percent of the panel is nonwhite; results for MIDUS may, therefore, not represent the experiences of minorities in the United States.
To assess whether our findings replicate in another national sample with different measures of the independent and dependent variables, we conduct parallel analyses on the first two waves of the Americans’ Changing Lives study (ACL; House et al. 1994). Face-to-face interviews were conducted in 1986 with 3,617 people ages 24 and older in the contiguous United States; three years later, 2,867 of these respondents were reinterviewed, resulting in a response rate of 79 percent for the panel. Analyses reported elsewhere (Umberson et al., 1996) indicate that 21 percent of attrition was due to mortality. Our attrition analyses (available) show that males, nonwhites, older persons, less educated persons, and persons who consumed more alcohol at Wave I were more likely to leave the study; in contrast to MIDUS, ACL respondents who reported poorer physical health and physical limitations at Wave I were not more likely to leave the study by Wave II.
Like MIDUS, the ACL survey was developed to assess stress, social relationships, and health among adults and included an oversampling of older persons. Unlike MIDUS, ACL has two measures of mental health, includes an oversampling of African Americans, and has a three-year interval between Waves I and II. The latter difference allows us to investigate the longer- versus shorter-term association between physical limitation and two indicators of mental health that are available in both studies. For comparability across data sets, we restricted the Wave I ACL sample to respondents who were 25 to 74 years old. Supplementary analyses (available) based on the full sample produced identical patterns to those we present.
Measures
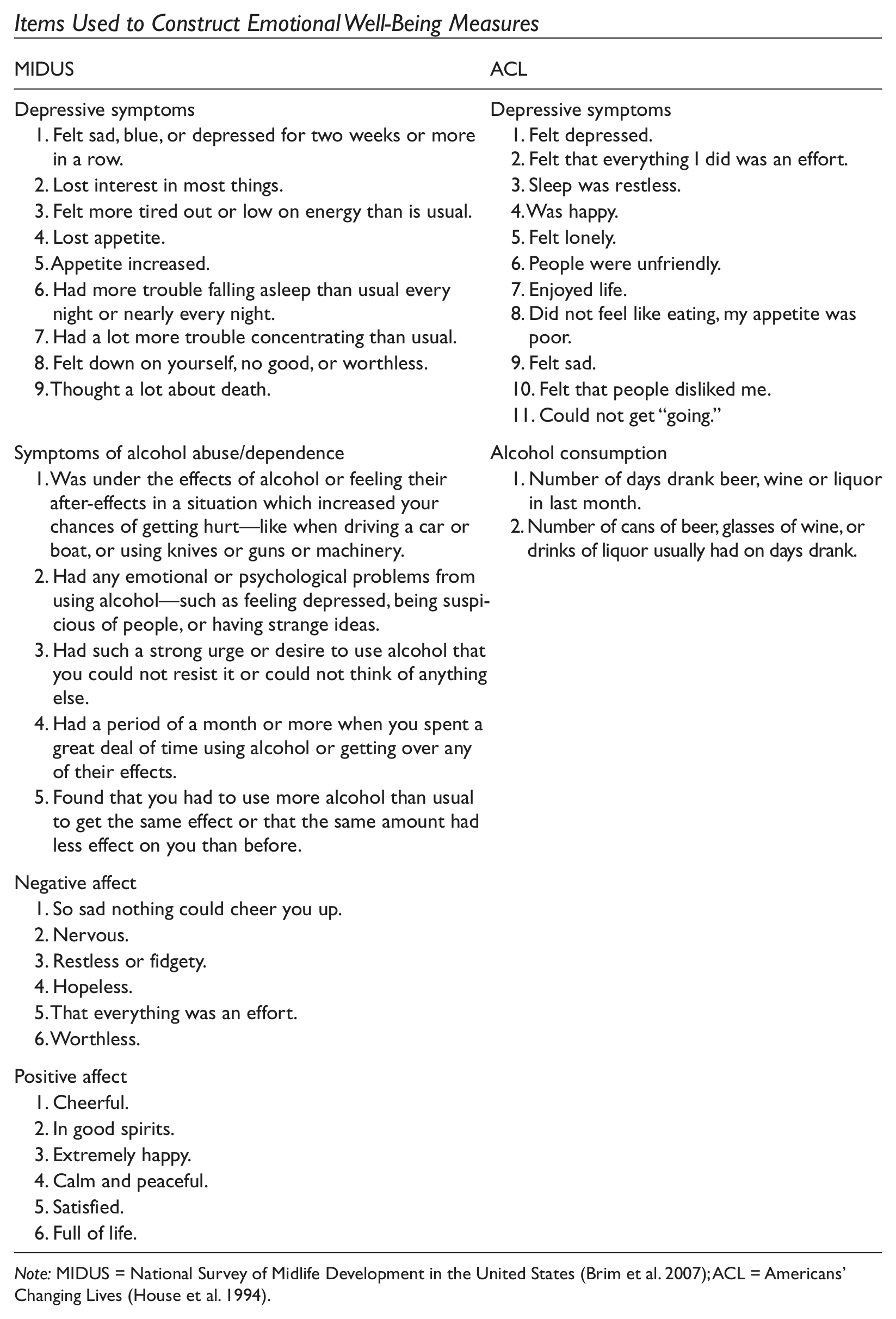
The items included in our measures of emotional well-being are shown in Appendix A. Depressive symptoms in MIDUS are measured with a nine-item count based on the short form of the Composite International Diagnostic Interview (CIDI; Kessler et al. 1998). The CIDI is a valid and reliable measure of depressive symptoms in population surveys based on criteria from the DSM-IV. Respondents who reported a period of sadness for two or more weeks in the past 12 months (yes = 1) were asked whether they experienced eight other symptoms of depression (yes = 1); reliability is .93, and scores range from 0 to 9. Depressive symptoms in ACL are measured with the 11-item version of the Center for Epidemiologic Studies Depression Scale (Radoff 1977), another valid and reliable measure of depressive symptoms in the general population. Respondents were asked how often during the past week (never or hardly = 0, some of the time = 1, most of the time = 2) they experienced each symptom; reliability is .82 with scores ranging from 0 to 21.
Symptoms of alcohol abuse/dependence in MIDUS are measured with a five-item count of problems respondents experienced in the past year as a result of their drinking; reliability is .70, and scores range from 0 to 5. This measure, which comes from the Michigan Alcohol Screening Test (Seltzer 1971), assesses serious problems caused by excessive drinking. Because research finds that adults with disabilities have lower rates of alcohol dependence (Compton et al. 2007; Kessler et al. 1994; Turner, Lloyd, and Taylor 2006), this measure may not capture physically limited persons’ distress. Alcohol consumption in ACL, which is based on the number of days in the past month respondents consumed alcohol multiplied by the number of drinks they had on those days, may better capture physically limited persons’ distress. Because they were skewing our results, we omitted the four respondents who had more than 300 drinks; scores on this measure range from 0 to 300.
Negative Affect is a summary scale based on six questions in MIDUS asking respondents how often in the past 30 days they experienced a variety of negative emotions. Positive Affect in MIDUS is also a six-item summary scale; in this case, respondents were asked how often in the previous month they felt a variety of positive feelings. Items came from valid instruments including Bradburn’s (1969) Affect Balance Scale. Response categories range from none (coded 0) to all (coded 4) of the time; reliability is .85 and .91, respectively, with scores ranging from 0 to 24. Because they are based on the experience of everyday emotions rather than mental health problems per se, these measures may capture more subtle gender and marital status variations in the association between physical limitation and emotional well-being.
To investigate the association between becoming physically limited (as well as explore the association between being physically limited) and change in emotional well-being between Waves I and II, we created three dummy variables for physical limitation status. MIDUS respondents reported how much difficulty they have with four activities, including (1) “bathing or dressing yourself,” (2) “bending, kneeling, or stooping,” (3) “walking one block,” and (4) “lifting or carrying groceries.” We considered MIDUS respondents to be physically limited if they had a “lot of difficulty” performing one or more activities. ACL respondents were asked how much their health or health-related problems limit their daily activities; for comparability across data sets, we considered ACL respondents to be physically limited if they reported “a great deal” or “quite a bit” of difficulty. “Became physically limited” (coded 1) includes persons who did not report difficulty at Wave I but reported difficulty at Wave II. “Physically limited at Waves I and II” (coded 1) contains those who reported difficulty at both waves. “Not physically limited at Waves I and II” (coded 1) includes people who did not report difficulty at both waves. In their extensive analysis of different physical limitation measures, Long and Pavalko (2004) conclude that binary measures, similar to the ones we constructed, are as reliable as if not more reliable than scales. Keep in mind that our measures distinguish between persons who did and did not have difficulty performing daily activities at Wave I and/or Wave II.
To avoid conflation between the influence of becoming physically limited and a marital status change between Waves I and II on mental health, we focus on persons who were either married or not married at both waves in each data set. To this end, we created a dichotomous variable, “married at Waves I and II” (married at both waves = 1, not married at both waves = 0).
All analyses include respondents’ gender (female = 1), race (nonwhite = 1), age (in years), age-squared, education, parental status (parent = 1), employment status (employed = 1), and household income at Wave I. We include age-squared to control for nonlinearity in the association between age and emotional well-being. Education is a categorical variable in MIDUS and an interval variable in ACL. To reduce the number of missing cases on household income, we assigned imputed scores to these respondents derived from regressing income on their gender, race, age, and education as well as marital, employment, and physical limitation status. Because physical health is highly correlated with physical limitations and mental health, our analyses include a single-item measure of self-rated health (poor = 0 to excellent = 4), allowing us to assess the association between becoming (and being) physically limited and mental health independent of the association between physical health problems and emotional well-being.
Analytic Samples
Because one of our main goals is to assess whether marriage moderates emotional well-being during the disablement process, we restricted the analytic samples to respondents who were either married or nonmarried at Waves I and II. In addition to excluding persons who reported a marital status change, we omitted the small number of respondents who were physically limited at Wave I but not at Wave II. 1 Supplementary analyses (available) indicate that persons who reported a marital status change did not differ from the rest of the sample with respect to symptoms of depression and alcohol use/abuse or the frequency of negative and positive emotions at Wave I. However, respondents who were physically limited at Wave I but not at Wave II reported significantly more depressive symptoms and negative feelings than the rest of the sample at Wave I. Although mental health at Wave I did not significantly predict attrition from either sample by Wave II, the exclusion of the latter respondents from the analytic samples may have resulted in an overrepresentation of persons who were emotionally healthier at Wave I. It is, therefore, likely that our results provide conservative estimates of the association between physical limitation and mental health. The MIDUS analytic sample contains 1,239 persons (71 percent of the panel); the ACL analytic sample includes 1,673 people (58 percent of the panel). Since our sample is highly selective and we control for all sociodemographic variables included in the sampling weights, we report the results of ordinary least squares (OLS) regression analyses based on nonweighted data.
Results
Table 1 shows the sociodemographic characteristics of our analytic samples by physical limitation status. Based on our conservative measure, 10 percent (n = 121) of the MIDUS sample became and another 6 percent (n = 70) were physically limited over the study, which when combined is similar to the percentage of physically limited persons in the United States (U.S. Department of Health and Human Services 2009). Respondents who became physically limited are more likely to be older, have less education, have lower household incomes, and are less likely to be employed. Similar to Waite and Hughes’s (1999) study, they are also more likely to be female and less likely to be married. The same sociodemographic differences are evident between persons who were not and who were limited throughout the study, with the exception that there is no significant marital status difference between stably limited and nonlimited respondents. Not surprisingly, persons who became and were physically limited rate their physical health as poorer than persons who were not limited.
Sociodemographic Characteristics of Analytic Samples by Physical Limitation Status.
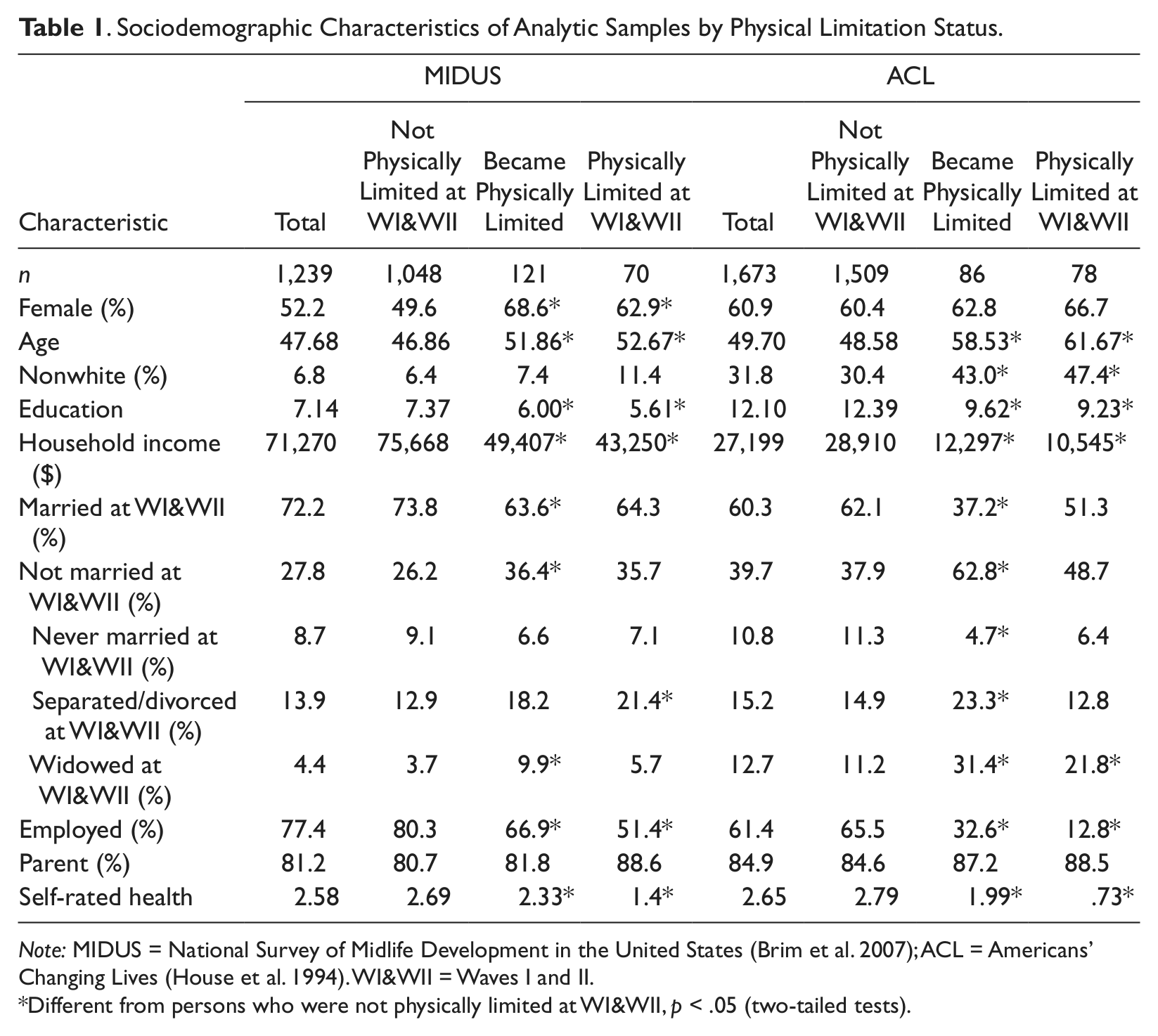
Note: MIDUS = National Survey of Midlife Development in the United States (Brim et al. 2007); ACL = Americans’ Changing Lives (House et al. 1994). WI&WII = Waves I and II.
Different from persons who were not physically limited at WI&WII, p < .05 (two-tailed tests).
Only 5.2 percent (n = 86) of the ACL analytic sample became and another 4.7 percent (n = 78) were physically limited over the study, which when combined is lower than the percentage in the United States; this difference between ACL and MIDUS may be due to the different measures of physical limitation and the shorter interval between Waves I and II of ACL than MIDUS. Nevertheless, the same sociodemographic differences we observe between physically limited and nonlimited individuals in MIDUS are evident in ACL, with the exception that women are not more likely than men to be (or have become) physically limited in ACL. ACL respondents who became and were limited are, however, more likely to be nonwhite. 2
The Association between Becoming (and Being) Physically Limited and Emotional Well-Being
Using OLS models, we next regress each measure of emotional well-being at Wave II on three sets of variables. Table 2 presents results for MIDUS; Table 3 summarizes results for ACL. To assess whether becoming (and being) limited is associated with different dimensions of mental health, each Model 1 in Tables 1 and 2 includes two dummy variables for physical limitation status as well as gender and marital status; the stably nonlimited and stably nonmarried are the reference groups. To determine whether the association between becoming (and being) physically limited and mental health is greater for women or men, we add interaction terms for gender and limitation status in each Model 2 of Tables 1 and 2. Each Model 3 in both tables includes interaction terms for marital and limitation status, allowing us to ascertain whether the association between becoming (and being) limited differs for married and nonmarried adults. Because these analyses focus on change in mental health between Waves I and II, all models include respondents’ level of emotional well-being at Wave I. Although not shown, the models also include sociodemographic characteristics and self-rated health at Wave I.
Unstandardized Coefficients from Regressions of Emotional Well-Being on Physical Limitation Status, Gender, and Marital Status (MIDUS).
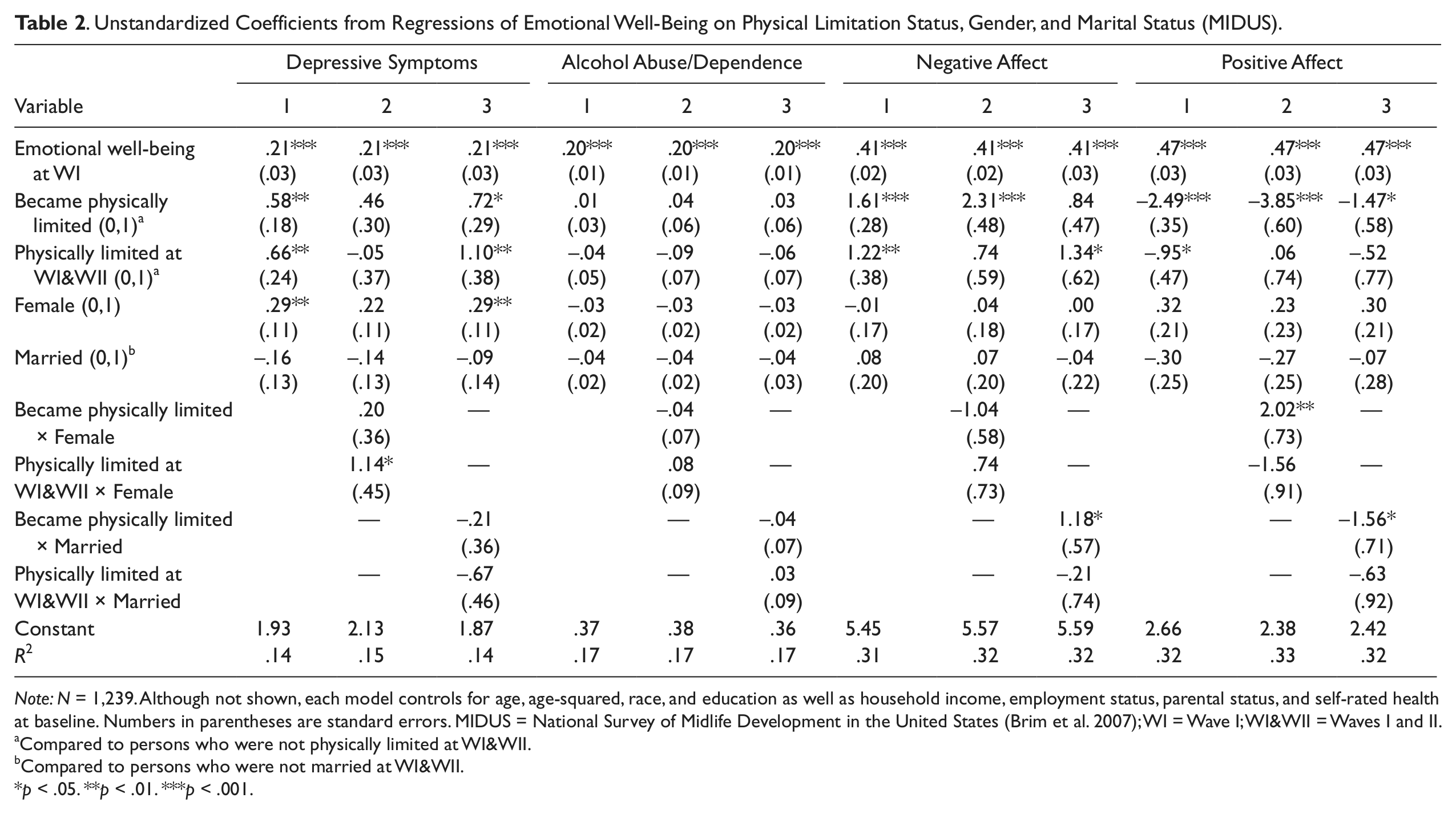
Note: N = 1,239. Although not shown, each model controls for age, age-squared, race, and education as well as household income, employment status, parental status, and self-rated health at baseline. Numbers in parentheses are standard errors. MIDUS = National Survey of Midlife Development in the United States (Brim et al. 2007); WI = Wave I; WI&WII = Waves I and II.
Compared to persons who were not physically limited at WI&WII.
Compared to persons who were not married at WI&WII.
p < .05. **p < .01. ***p < .001.
Unstandardized Coefficients from Regressions of Emotional Well-Being on Physical Limitation Status, Gender, and Marital Status (ACL).
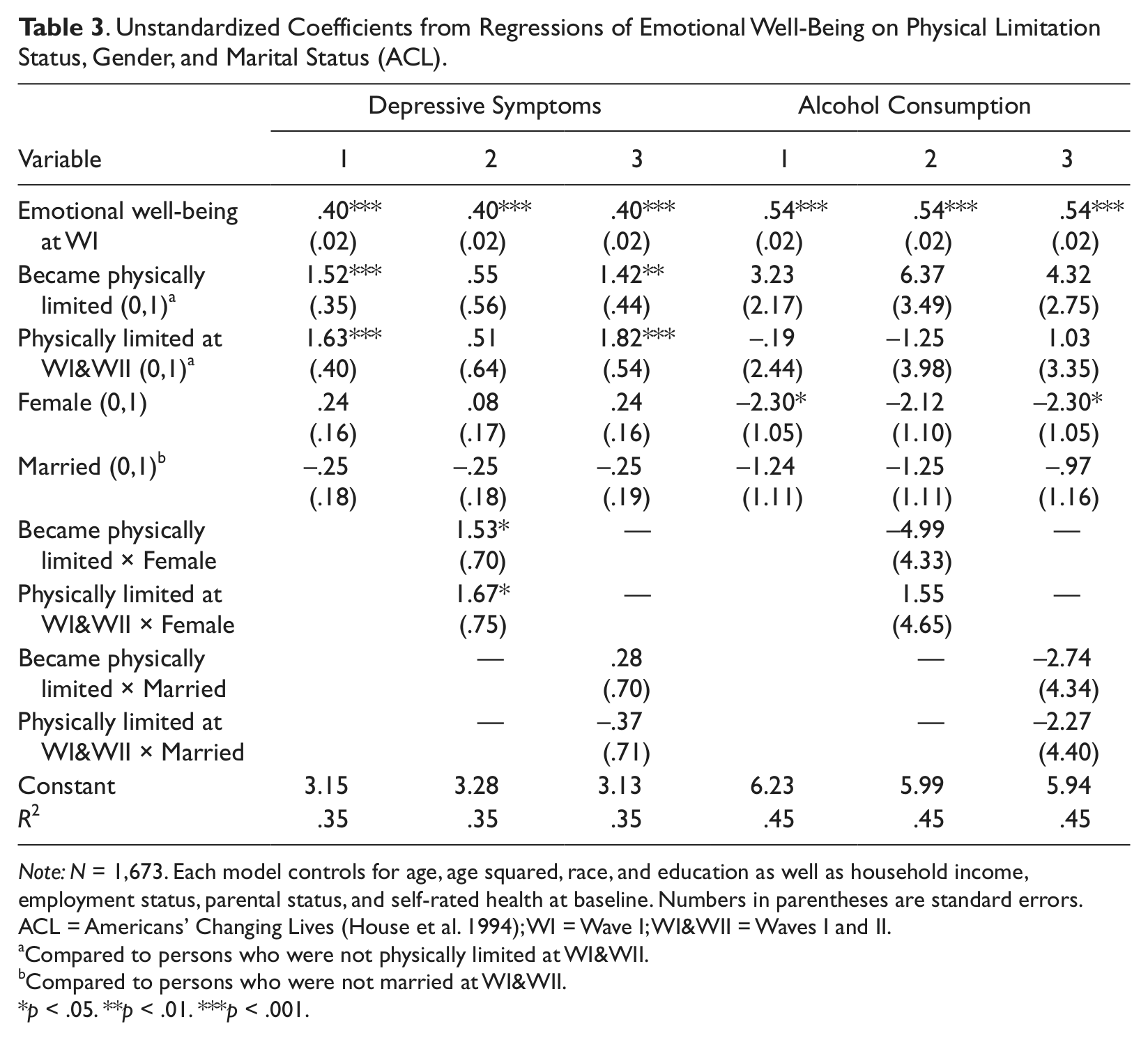
Note: N = 1,673. Each model controls for age, age squared, race, and education as well as household income, employment status, parental status, and self-rated health at baseline. Numbers in parentheses are standard errors. ACL = Americans’ Changing Lives (House et al. 1994); WI = Wave I; WI&WII = Waves I and II.
Compared to persons who were not physically limited at WI&WII.
Compared to persons who were not married at WI&WII.
p < .05. **p < .01. ***p < .001.
Similar to other longitudinal studies, each Model 1 of Table 2 shows that symptoms of depression and alcohol abuse/dependence as well as the frequency of negative and positive emotions at Wave I predict these indicators of mental health at Wave II. Consistent with studies we discussed earlier, physical limitation is associated with significantly lower levels of emotional well-being. Compared to persons who were not physically limited, individuals who became limited experienced an increase in depressive symptoms and negative feelings as well as a decrease in positive emotions. Stably limited persons also experienced an increase in these indicators of emotional well-being, which suggests that physical limitation continues to erode these dimensions of mental health over time—in this case, over a 10-year period. Becoming (and being) physically limited is not, however, associated with increased alcohol abuse/dependence.
There appears to be a significant gender difference in the association between physical limitation status and two dimensions of emotional well-being (Model 2); the decrease in positive emotions among persons who became limited is significantly greater for men than for women. In contrast, the increase in depressive symptoms among persons who were physically limited at both waves is significantly greater for women than men. Together, these subtle yet significant patterns indicate that gender differences in vulnerability to becoming (and being) physically limited depend on the particular dimension of mental health considered.
Additionally, the increase in negative and decrease in positive emotions among persons who became limited is significantly greater for married than for nonmarried adults (Model 3). These findings suggest that married adults are more vulnerable to the impact of becoming physically limited with respect to the experience of everyday emotions—which are more subtle indicators of emotional well-being than symptoms of depression and alcohol abuse/dependence.
Turning to our analyses of the ACL panel in Table 3, we find that depressive symptoms and alcohol consumption at Wave I significantly predict these indicators of distress at Wave II (Model 1). Consistent with our results for MIDUS, physical limitation is associated with significantly lower levels of emotional well-being. ACL respondents who became and were physically limited experienced an increase in depressive symptoms; once again, the latter finding suggests that physical limitation continues to erode this dimension of mental health over time—in this case, over a three-year period. We also find that neither becoming (nor being) physically limited is associated with increased alcohol consumption. Together with our results for MIDUS, these results suggest that physical limitation does not influence this particular dimension of mental health, a finding that is consistent with recent epidemiological studies on physically limited adults (Kessler et al. 2005; Turner et al. 2006).
Also similar to our results for MIDUS, there is a significant gender difference in the association between physical limitation and depressive symptoms in ACL; in this case, the increase in depression among persons who became and were physically limited is greater for women than men (Model 2). The consistency of our results from MIDUS and ACL for depressive symptoms strongly suggests that women are more vulnerable than men to the depressing impact of this source of chronic stress.
Paralleling our results for depressive symptoms and alcohol abuse/dependence in MIDUS, there is no significant marital status difference in the association between either becoming or being physically limited and both depressive symptoms and alcohol consumption in ACL (Model 3). These findings suggest that marital status neither buffers nor exacerbates the impact of physical impairment on these particular dimensions of emotional well-being.
As a final step in our investigation, we conducted supplementary analyses that contain three-way interactions in order to ascertain whether gender differences in the physical limitation-mental health association depends on marital status as well as whether marital status differences in the physical limitation-mental health association depends on the gender of the person. To this end, we interacted each limitation status with gender and marital status. While there are no significant three-way interactions in ACL, these analyses (available) reveal two significant three-way interactions in MIDUS. First, although physical limitation is not significantly associated with substance abuse/dependence, we find that among MIDUS respondents who became limited, nonmarried men experienced a greater increase in this indicator of distress than married men and nonmarried women (p < .01). Second, the decrease in positive emotions among persons who became limited in MIDUS (which is significantly greater for married than nonmarried adults) is greater for married men than for nonmarried men and married women (p < .05).
Due to the small number of cases for each physical limitation, gender, and marital status combination, these results should be interpreted with a great deal of caution. They do, however, suggest that marriage exacerbates the impact of becoming limited on positive feelings while buffering the impact of becoming limited on substance abuse/dependence among men. In other words, men’s greater vulnerability to the stress associated with physical limitations depends not only on the outcome considered but also on their marital status. We do not know whether the inconsistent findings for alcohol abuse/dependence in MIDUS and alcohol consumption in ACL reflect the different time interval between Waves I and II or the different measures of this dimension of emotional distress. However, the lack of a significant three-way interaction for depressive symptoms in MIDUS and ACL suggests that marital status does not play a role in women’s greater vulnerability to the impact of physical limitation on depressive symptoms.
Discussion
A consequence of the increase in longevity that has received considerable scholarly attention is the rise in the number of physically limited adults in the United States. Given the practical, social, and identity challenges associated with diminished physical capacity, it is not surprising that studies find physical limitation to be a major chronic stressor in the lives of adults, which is associated with increased feelings of depression. It is, however, surprising that scholars have not examined the degree to which this source of stress is associated with other dimensions of emotional well-being as well as gender and marital status differences in these associations. In this paper, we addressed these two important gaps in knowledge about this growing population with panel data from two national samples of adults.
Our analyses indicate that becoming physically limited is associated with an increase in depressive symptoms (in MIDUS and ACL) as well as an increase in negative and decrease in positive emotions (in MIDUS). The findings also indicate that being physically limited is associated with an increase in depressive symptoms (in both data sets) as well as an increase in negative and decrease in positive emotions (in MIDUS). Our results for negative and positive affect go beyond previous studies that focused on depressive symptoms and increase knowledge about the associations between physical limitation and other dimensions of emotional well-being. It is noteworthy that persons who were physically limited at Waves I and II reported an increase in depressive symptoms in MIDUS and ACL, even though the former study had a 10-year interval between waves. These findings provide new insight into the long-term emotional consequences of physical limitation, a previously unexplored topic that we think warrants further research.
Physical limitation is not, however, associated with either alcohol abuse/dependence or consumption, a finding that is consistent with epidemiological studies (Kessler et al. 1994; Turner, Lloyd, and Taylor 2006). There are two possible explanations for this pattern. The first is that physically impaired persons tend to be older, and alcohol use and abuse are less common among older people, perhaps because alcohol can make age-related cognitive and physical health problems worse and interact with medication (Goodwin et al. 1987; Stone et al. 2010). The second explanation is that because their physical functioning is already compromised, physically limited adults avoid behaviors that would further challenge their physical abilities.
Interactional analyses revealed complex patterns regarding gender differences in the association between physical limitation and mental health. Recall that the increase in depressive symptoms among persons who were limited at Waves I and II (in MIDUS and ACL) and who became limited (in ACL) is greater for women. In contrast, the decrease in positive feelings among individuals who became limited between Waves I and II (in MIDUS) is greater for men.
Overall, these results provide no support for our two contrasting hypotheses about gender differences in vulnerability to the emotional impact of physical limitation. Indeed, it appears that physical impairment is distressing for men and women, which is evident for different mental health problems; an exclusive focus on depressive symptoms would not have captured men’s vulnerability to this source of stress. These results add to the accumulating body of work documenting that the impact of certain types of stress does not differ for men and women when multiple expressions of emotional upset are considered. Although our data did not allow us to assess this possibility, physical limitations may be distressing for both women and men because they threaten gender-specific sources of self-conception, such as a self-reliant identity among men and caregiver identity among women. Qualitative studies are well suited for capturing how physical limitation affects men’s and women’s gendered identities and emotional well-being.
Interactional analyses also revealed marital status differences in the association between physical limitation and mental health; the increase in negative and decrease in positive emotions experienced by individuals who became limited (in MIDUS) is greater for married than for nonmarried adults. These results clearly indicate that married men and women are more vulnerable than nonmarried people to the emotional impact of physical limitation, at least with respect to these indicators of mental health. The social processes underlying these results are, however, less clear. We initially suggested that married people’s dependence on their spouse for instrumental and emotional support as well as their inability to adequately perform marital roles may be a source of chronic marital strain, which undermines the buffering effect of marriage. To determine whether a decline in marital quality plays a role in their greater vulnerability to physical limitation, we conducted supplementary analyses of married respondents in both data sets. Interestingly, these analyses (available) showed no significant change in either perceived marital strain or support among married persons who became limited between Waves I and II of MIDUS and ACL. Qualitative comparisons of physically limited adults who are married and nonmarried may be better able to capture subtle social processes underlying marital status differences in the impact of this source of stress on the experience of everyday negative and positive emotions.
Exploratory analyses including three-way interactions further revealed that marital status differences in the associations between physical limitation and mental health in MIDUS depend on the measure of distress and gender of the person. These findings suggest that while marriage exacerbates the negative impact of becoming limited on positive feelings, it buffers the impact of becoming limited on alcohol abuse/dependence among men. The latter finding may reflect wives’ “control” over this aspect of their husband’s behavior, as prior studies indicate (Umberson 1987). At the same time, the lack of a three-way interaction for depressive symptoms in both data sets suggests that marital status does not influence women’s greater vulnerability to the depressing effect of this source of stress. The small number of cases involved in these analyses makes us cautious about reading too much into these results. These suggestive patterns do, however, provide fertile ground for future investigations of gender differences in the influence of marriage on different dimensions of physically limited adults’ mental health.
Given our results, what are we to conclude with respect to gender and marital status variations in the association between physical limitation and mental health? When viewed as a whole, it appears that gender and marital status differences in the impact of physical limitation are nuanced, complex, and depend on the measure of well-being. Our results, therefore, provide additional support for Aneshensel’s (1992) theoretical argument that the impact of stress on emotional well-being is contingent on the social characteristics of persons and mental health problem considered. Our results also contribute to theory about the significance of both gender and marital status for understanding the emotional well-being of adults in the United States, particularly as they confront challenges to their physical capacities.
Data limitations prevented us from assessing whether the patterns identified are generalizable to different racial and ethnic groups in the United States. Group differences in cultural norms about the importance of self-reliance for men and caregiving for women—as well as differences in the emotional significance of marriage—may produce different results than those we obtained. An obvious next step for research is to investigate racial and ethnic variations in the association between physical limitation among married and nonmarried women and men. Because they may respond to stress in general, and this source of stress in particular, with different emotional problems, it is imperative to continue examining multiple dimensions of mental health.
Other sample characteristics and measurement limitations may also have influenced our results. However, because both samples may overrepresent emotionally healthier people, it is likely that our results provide conservative estimates of the association between physical limitation and mental health. It is also likely that our basic measures of physical limitation status conceal considerable heterogeneity in the cause, severity, and meaning of physical impairment for individuals—another topic for future research. Despite these limitations, our study begins to fill two gaps in knowledge about the association between physical limitation and mental health. Physical limitation is associated with dimensions of mental health other than depressive symptoms, and there are both gender and marital status differences in these associations.
Footnotes
Appendix A
Items Used to Construct Emotional Well-Being Measures
| MIDUS | ACL |
|---|---|
| Depressive symptoms Felt sad, blue, or depressed for two weeks or more in a row. Lost interest in most things. Felt more tired out or low on energy than is usual. Lost appetite. Appetite increased. Had more trouble falling asleep than usual every night or nearly every night. Enjoyed life. Did not feel like eating, my appetite was poor. Thought a lot about death. |
Depressive symptoms Felt depressed. Felt that everything I did was an effort. Sleep was restless. Was happy. Felt lonely. People were unfriendly. Had a lot more trouble concentrating than usual. Felt down on yourself, no good, or worthless. Felt sad. Felt that people disliked me. Could not get “going.” |
| Symptoms of alcohol abuse/dependence Was under the effects of alcohol or feeling their after-effects in a situation which increased your chances of getting hurt—like when driving a car or boat, or using knives or guns or machinery. Had any emotional or psychological problems from using alcohol—such as feeling depressed, being suspicious of people, or having strange ideas. Had such a strong urge or desire to use alcohol that you could not resist it or could not think of anything else. Had a period of a month or more when you spent a great deal of time using alcohol or getting over any of their effects. Found that you had to use more alcohol than usual to get the same effect or that the same amount had less effect on you than before. |
Alcohol consumption Number of days drank beer, wine or liquor in last month. Number of cans of beer, glasses of wine, or drinks of liquor usually had on days drank. |
| Negative affect So sad nothing could cheer you up. Nervous. Restless or fidgety. Hopeless. That everything was an effort. Worthless. |
|
| Positive affect Cheerful. In good spirits. Extremely happy. Calm and peaceful. Satisfied. Full of life. |
Note: MIDUS = National Survey of Midlife Development in the United States (Brim et al. 2007); ACL = Americans’ Changing Lives (House et al. 1994).
Acknowledgements
We thank the John D. and Catherine T. MacArthur Research Network for the National Survey of Midlife Development in the United States and the National Institute of Aging for the American’s Changing Lives Survey. We are grateful to Brian Powell for his helpful suggestions on earlier drafts. The authors made an equal contribution to this paper.