
Abstract
As nonmarital childbearing becomes a dominant pathway to family formation, understanding its long-term consequences for children’s well-being is increasingly important. Analysis of linked mother-child data from the 1979 National Longitudinal Survey of Youth indicates a negative association of having been born to a never-married mother with adolescent self-assessed health but not with depressive symptoms. We also consider the role of mothers’ subsequent union histories in shaping the adolescent health outcomes of youth born to unmarried mothers. With two exceptions, unmarried mothers’ subsequent unions appear to have little consequence for the health of their offspring during adolescence. Adolescents whose mothers subsequently married and remained with their biological fathers reported better health, yet adolescents whose mothers continuously cohabited with their biological fathers without subsequent marriage reported worse adolescent mental health compared with adolescents whose mothers remained continually unpartnered.
Forty-one percent of all births in the United States now occur to unmarried mothers (Martin et al. 2011), and fewer than half of all unmarried mothers marry within five years of their nonmarital birth (McLanahan 2011). Thus, substantial numbers of children spend their earliest years, a critical period of development, in unmarried-parent households. The rapid growth in nonmarital childbearing has been accompanied by concerns about “family decline” and predictions of negative consequences for U.S. society at large (Brooks 2002), and a growing body of literature documents negative consequences of nonmarital fertility for offspring in early childhood (see McLanahan 2011). Whether there are mental and physical health consequences of nonmarital fertility that endure beyond early childhood is less clear, however, because conclusions about the importance of the two-parent family for young adults have been based primarily on studies of children of divorce (see Amato 2010). That a sizable cohort of children born to unmarried mothers is now reaching young adulthood allows an examination of longer term consequences of nonmarital childbearing for the health and well-being of offspring whose mothers were at the forefront of substantial demographic change in family formation patterns.
Growing rates of nonmarital fertility, accompanied by high rates of poverty in single-parent homes, have fueled debate about the most effective ways to improve the lives of children born to unmarried mothers. Public discourse and policy have focused on promoting marriage among low-income single mothers, building on evidence that children raised by two biological parents fare better on many outcomes than children born to unmarried mothers. But such findings may have limited relevance for children born to unmarried mothers because most unions formed after nonmarital childbearing involve partners who are not the biological fathers (Cancian, Meyer, and Cook 2011; Guzzo and Furstenberg 2007; Osborne and McLanahan 2007). Determining the impact of nonmarital fertility and subsequent union formation for adolescent health and well-being requires a specific focus on children born to unmarried mothers and attention to the subsequent union status of their mothers plus the paternity status of the mother’s partner. Attention to potential health differences for black versus white youth is also important given stark racial disparities in nonmarital childbearing and subsequent union formation (Osborne, Manning, and Smock 2007; Qian, Lichter, and Mellott 2005).
We address these questions using data from the 1979 National Longitudinal Survey of Youth (NLSY79) mother-child files. First, we compare the mental and physical health of adolescents born to never-married cohabiting or unpartnered mothers with that of their counterparts born to married mothers, paying attention to variations between black and white youth and controlling for numerous maternal background characteristics. Second, among adolescents born to never-married mothers, we compare the health of those whose mothers subsequently cohabited or married with that of their counterparts whose mothers remained unpartnered. We distinguish mothers’ union histories by marital vs. cohabitation status, marital stability, and paternity status of the partner and, where possible, consider differences by race.
Background
Nonmarital Fertility and the Health of Offspring in Adolescence
Rising nonmarital childbearing rates in the United States have raised concerns among both policy makers and the general public about implications for the long-term well-being of children. Research on children of divorce shows that spending time in a single-parent home is associated with negative cognitive, psychosocial, and behavioral outcomes across the life course (for reviews, see Amato 2010; Brown 2010). Much less is known about the long-term well-being of children born to unmarried mothers, however, and what empirical knowledge exists skews heavily toward a focus on early childhood outcomes. Also unknown is whether unmarried mothers’ cohabitation status at birth has long-term consequences for children’s health in adolescence, a question of growing importance as approximately 58 percent of nonmarital fertility now occurs within cohabiting unions (Martinez, Daniels, and Chandra 2012).
Research and theory provide strong support for our hypothesis that maternal marital and cohabitation status at the time of a birth are associated with offspring mental and physical health years later during adolescence. Although identifying mechanisms is beyond the scope of this study, it is well established, for example, that nonmarital fertility is often followed by substantial economic strain and exposure to chronic stressors linked to family and residential instability. Children born to never-married mothers are more likely to live in poverty than those born to married parents, even those whose parents later divorce (Huang, Mincey, and Garfinkel 2005), and early economic deprivation is strongly associated with adverse mental and physical health outcomes across the life course (Conley and Bennett 2001; Duncan and Brooks-Gunn 1997). Furthermore, children born to unmarried mothers have smaller networks of social support (Harknett and Hartnett 2011) and are at especially high risk for experiencing potentially stressful conditions, including multiple residential moves (Murphey, Bandy, and Moore 2012) and mothers’ partnership instability (Osborne and McLanahan 2007). Chronic stress exposure, in turn, has cumulative negative effects on health through numerous biological and psychosocial pathways (Pearlin et al. 2005). It is important to note that although any impact of early-life factors on adolescent outcomes likely operates through multiple pathways, it is critical to first document these basic associations and potential heterogeneity by race and other factors. Our analyses, therefore, do not control for potential intervening variables (e.g., mother’s socioeconomic attainment after the child’s birth, later family instability) that may mediate between mothers’ union status or history and adolescent outcomes, because doing so would underestimate the true association of interest (Lieberson 1985).
The Fragile Families and Wellbeing Study has provided mounting evidence of negative cognitive, behavioral, and health outcomes for children born to unmarried women (Bzostek and Beck 2011; Carlson and Corcoran 2001; Waldfogel, Craigie, and Brooks-Gunn 2010). However, because these data currently extend only to nine years of age, relatively little is known about the consequences of being born to an unmarried mother for adolescent health. The few studies that have examined a broader age range have not focused specifically on adolescent mental and physical health. This research indicates, however, that adolescents and young adults born to unmarried mothers have more behavior problems in school (Hofferth, West, and Kaufman 1994), have younger ages at sexual debut (Cavanagh, Crissey, and Raley 2008), are at greater risk for teen and premarital births (Francesconi 2008; Wu 1996), and are more likely to divorce (Teachman 2002) than those raised with both biological parents. However, none of these studies specifically distinguish youth born to cohabiting mothers or specify whether such youth are grouped with those born to married biological parents or with those born to unpartnered mothers.
Finally, prior research on the link between maternal union status at birth and adolescent well-being does not differentiate youth born to never-married mothers from those born to divorced mothers. Between 1995 and 2008, only 14.4 percent of all nonmarital births occurred to divorced women, and this figure is likely even smaller for the nonmarital first births on which we focus (Wu 2008). Given lower rates of marriage among disadvantaged and minority women, nonmarital fertility following divorce is less likely to occur in the same context of disadvantage as it does among the never married and therefore may have substantially different consequences for child health. For this reason, youth born to previously divorced unmarried mothers should be kept analytically distinct from those born to never-married mothers. Unfortunately, we do not have enough postdivorce cases to constitute a separate category, and we therefore exclude them from our analyses. We argue that this is an improvement over prior research that combined youth born to divorced and never-married mothers.
The life course epidemiology framework emphasizes that the cumulative effects of early-life factors on health and well-being often take decades to emerge (Ben-Shlomo and Kuh 2002; Hayward and Gorman 2004) and guides our focus on exploring long-term consequences of nonmarital fertility for offspring health in adolescence. A key tenet of this paradigm is that a short-term perspective whereby health is measured contemporaneously with influential life events can underestimate true long-term effects (Ben-Shlomo and Kuh 2002). Furthermore, from both policy and public health perspectives, it is important to identify events and conditions with enduring health consequences.
Subsequent Maternal Union History and Adolescent Health
An equally important question is whether an unmarried mother’s subsequent marriage might improve health outcomes for her children, as suggested by proponents of marriage promotion initiatives. However, one cannot assume that two-parent homes experienced by children born to two married parents necessarily have the same impact on health and well-being as those experienced by children born to unmarried mothers who later marry. Women who marry after nonmarital births report more conflict, less companionship (Timmer and Orbuch 2001), and less perceived stability (Williams, Sassler, and Nicholson 2008) in their marriages than women who have children within marriages. Women who marry after nonmarital births are also more likely to marry men who already have children or who have low levels of income and education (Lichter, Graefe, and Brown 2003). Consequently, few unmarried mothers appear to receive economic (Edin and Kefalas 2005; Graefe and Lichter 2007) or health (Williams et al. 2011) benefits from marriage. Given the importance of economic and family stability to child well-being (Bzostek and Beck 2011; Heard 2007; Wu 1996), evidence that unmarried mothers face barriers to forming stable, high-quality, and economically beneficial marriages challenges the assumption that unmarried mothers’ later marriages will necessarily promote the health and well-being of their children.
In fact, several recent studies concluded that there is little evidence that maternal marriage benefits children born to unmarried mothers (Acs 2007; Bachman, Coley, and Chase-Lansdale 2009), although none have focused specifically on the mental and physical health of adolescents. Prior research has focused on short-term processes, examining child well-being as a function of mother’s current union status or recent union transitions (Acs 2007; Heard 2007). As Wagmiller et al. (2010) noted, “Failure to consider how the effects of parental marriage change over time is likely to understate the long-term benefits of marriage, especially if the effects of marriage on children are examined . . . immediately after a parent’s transition to marriage” (p. 202). We address this issue and further consider how union type, marital stability and the paternity status of the mother’s partner shape the health of adolescents born to unmarried women.
Union Type, Union Dissolution, and Paternity Status
Marriages that unmarried mothers enter are especially vulnerable to dissolution, partly because of the relative lack of “marriageable men” available (Harknett and McLanahan 2004; Qian et al. 2005). Unions may introduce instability into children’s lives by increasing exposure to alcohol, drugs, violence, and union dissolution (McLanahan 2006), with negative consequences for child well-being. Although some research suggests that family instability is more predictive of children’s outcomes than is family structure, per se (Heard 2007; Wu 1996), other research indicates that much of the instability effect (but not the effect of mother’s union status at birth) is explained by mother’s antecedent characteristics (Fomby and Cherlin 2007). Furthermore, mothers’ cohabiting and marital unions can provide financial and emotional benefits for households (Cavanagh et al. 2008; Fomby and Cherlin 2007), making it important to clarify the relationships between union status at birth, subsequent union change, and offspring well-being. We distinguish mothers whose later marriages dissolve from those whose marriages endure.
Paternity status of the spouse is also relevant. Data from the Fragile Families and Wellbeing Study suggest that only a minority of never-married mothers marry the fathers of their children (Carlson, McLanahan, and England 2004). Furthermore, all fathering statuses are not equivalent in their ramifications for children (Aquilino 1996; Brown 2004; Hofferth 2006; Morrison and Ritualo 2000) or in the perceptions of mothers, whose assessments of fathers’ parenting practices are contingent on both paternity status and union status (Berger et al. 2008). For example, biological fathers are more trusted than nonbiological residential “social fathers,” but social fathers are seen as more cooperative, particularly in marital unions (Berger et al. 2008). Although drawn largely from studies of children of divorce, the benefits of a two-parent home for child well-being appear diminished for children living with stepfathers compared with children living both with biological fathers (Chase-Lansdale 1994; Hofferth 2006) and those whose mothers remain unmarried (Aquilino 1996; Brown 2006; Fomby and Cherlin 2007). We focus on children born to never-married mothers and differentiate those whose mothers subsequently married their biological fathers from those whose mothers formed unions with others. Unmarried mothers’ cohabitation experiences (at birth or later) may also shape offspring mental and physical health. Mounting evidence suggests that the benefits of having a father in the household are limited to marital unions, in part because paternal investment in offspring is weaker in cohabiting unions (Berger et al. 2008; Brown 2004; Hofferth 2006). Cohabitations are also less stable and shorter lived than marital unions, particularly for the less educated and when children are present: over 80 percent of cohabiting unions last fewer than five years (Qian et al. 2005). Thus, for offspring of unmarried mothers, a mother’s cohabitation, even with the child’s father, will likely be associated with fewer favorable outcomes than marriage, but its expected effect compared with mothers remaining unpartnered is less clear.
Race, Family Structure, and Adolescent Health
Black youth are especially likely to be born to unmarried mothers and to spend much or all of their childhood years in unmarried-parent homes. In 2009, nonmarital births accounted for 29 percent and 72.8 percent of all births to white and black women, respectively (Martin et al. 2011). White women are also significantly more likely to marry after the birth of children than are black women. Among women who experienced nonmarital births between 1982 and 2004, 71.4 percent of white women but only 36.3 percent of black women had wed within the next 10 years (Gibson-Davis 2011, Table 2). Black children born to cohabiting parents are also significantly more likely to witness their parents’ union dissolve than are white children (Osborne et al. 2007). It is therefore important to consider variation by race in the consequences of nonmarital childbearing for adolescent health and well-being.
Several studies suggest that family structure and family instability matter more for the well-being of white than black children (Dunifon and Kowaleski-Jones 2002; Fomby and Cherlin 2007; Fomby, Mollborn, and Sennott 2010; Manning and Brown 2006). Scholars speculate that differences in the normative status of nonmarital parenthood and in the familial and community support provided to unmarried parents may be relatively protective for black children (Fomby and Cherlin 2007; Gerstel 2011), and some even suggest that an emphasis on marriage and nuclear family life disregards the very social resources and community ties crucial to the survival strategies of low-income populations (Gerstel 2011). Additional evidence indicates that unmarried African American fathers have more frequent contact and involvement in their children’s lives than their white counterparts (King, Harris, and Heard 2013; Stier and Tienda 1993). Whether these differences are associated with the health of adolescent offspring remains unexplored, however. We consider race differences in the association of adolescent health with mother’s marital status at birth and, when our data allow, with mother’s subsequent union history.
Data and Methods
Data are from the NLSY79, which interviewed a nationally representative sample of 12,686 young men and women aged 14 to 22 in 1979. Respondents have been interviewed annually through 1994 and biennially since. Retention rates remain at over 80 percent of cases eligible to be interviewed, and we use data on this cohort that spans 31 years, through 2010. A strength of the NLSY79 is the availability of linked data on children born to NLSY79 women. Beginning in 1994 and continuing biennially, children aged 15 years and older are interviewed with their own young adult survey. As of 2010, more than 90 percent of first-born children had aged into the young adult sample. When weighted, children of the NLSY79 mothers can be considered representative of children born to U.S. women aged 14 to 21 years on December 31, 1978.
Measures
Dependent variables
Our models predict self-assessed health and depressive symptoms. Self-assessed health is strongly predictive of morbidity and mortality (Idler and Benyamini 1997) and is recognized as a valid and reliable indicator of health status in general populations (Ferraro and Farmer 1999). We construct two measures of self-assessed health from responses to the following question: “In general, would you say your health is excellent, very good, good, fair, or poor?” Fair or poor self-assessed health is a dichotomous measure in which 1 = fair or poor health and 0 = excellent, very good, or good health. We use the full five-category indicator of self-assessed health. Depressive symptoms are assessed using a summed seven-item version of the Center for Epidemiologic Studies Depression Scale (CES-D; range = 0–21). Respondents assess the frequency of seven somatic and emotional symptoms of depression over the past week on a scale ranging from 0 to 3. We use the natural logarithm of the CES-D score to reduce the positive skew in the untransformed variable. The CES-D is highly correlated with other depression scales and is a common indicator of mental health status in community populations.
We measure the dependent variables when young adults are aged 14 or 15 years for about 71 percent of the analytic sample. If data are missing at these ages, we take information from young adults at progressively older ages: 16 (20 percent), 17 (5 percent), and 18 (4 percent) years, controlling for age at measurement. Descriptive statistics for all variables are presented by both mother’s marital status at the child’s birth and race in Table 1.
Descriptive Statistics for Analysis 1 (Table 3) by Mother’s Marital Status at Adolescent’s Birth and Race (total n for all groups = 2,033).
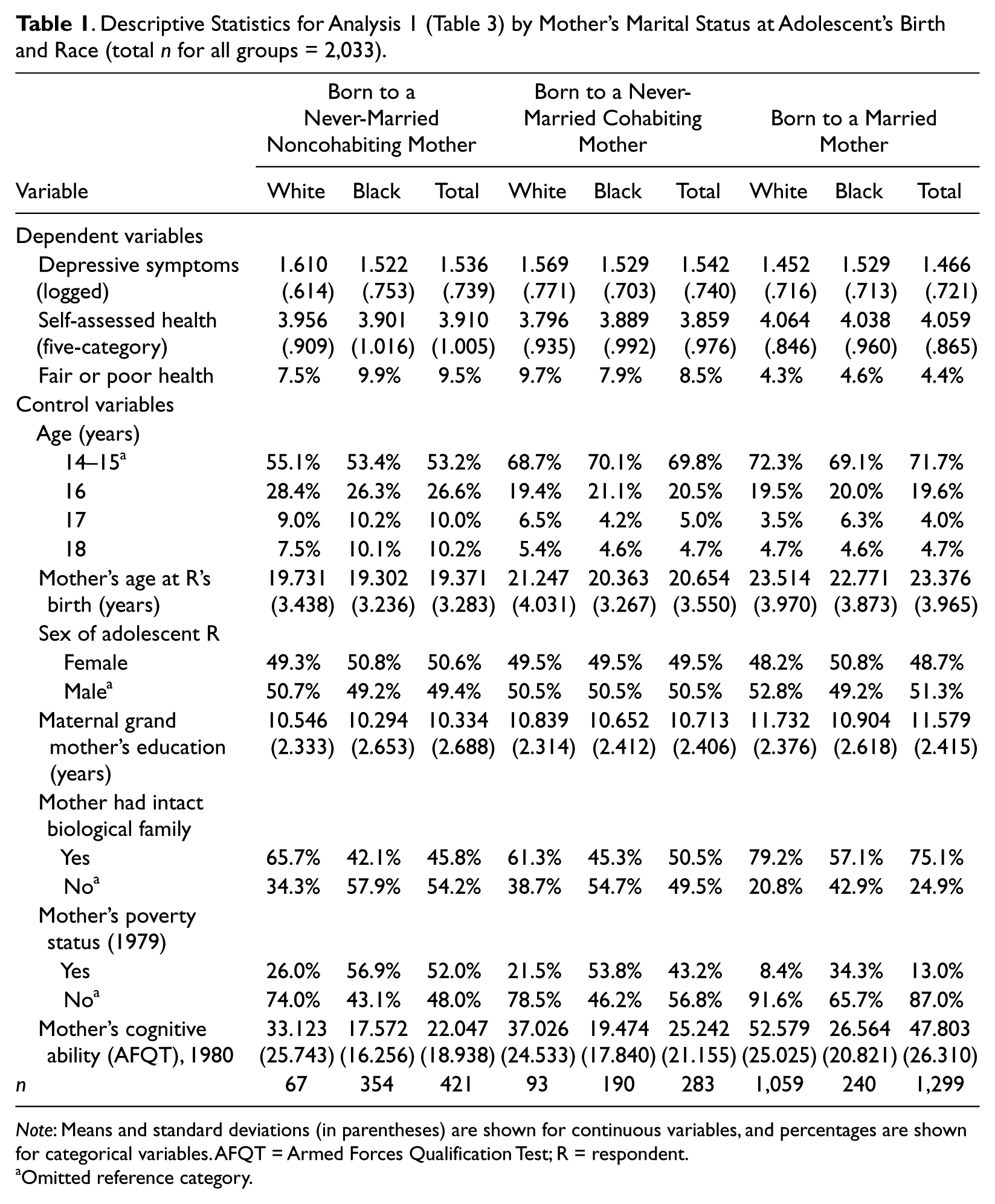
Note: Means and standard deviations (in parentheses) are shown for continuous variables, and percentages are shown for categorical variables. AFQT = Armed Forces Qualification Test; R = respondent.
Omitted reference category.
Mother’s marital status at birth and subsequent union history
The primary independent variable in the first stage of our analysis is mother’s marital status at birth. Dummy variables distinguish those born to (a) never-married noncohabiting mothers (n = 421), (b) never-married cohabiting mothers (n = 283), and (c) married mothers, the reference category (n = 1,299). We exclude 57 youth whose mothers’ cohabitation status at birth was unknown.
The second stage of our analysis is limited to 761 youth born to never-married (cohabiting or noncohabiting) mothers. Seven mutually exclusive dummy variables distinguish mothers’ subsequent union histories, using a hierarchy that first identifies those who eventually entered into marital unions, followed by those who cohabited without marrying. The categories are as follows: (1) entered an enduring 1 marriage with the biological father (n = 150), (2) entered an enduring marriage with someone other than the biological father (n = 136), (3) entered and exited a marriage with the biological father (n = 63), (4) entered and exited a marriage with a new partner (n = 68), (5) never married but cohabited with the biological father (n = 88), and (6) never married but cohabited with a new partner (n = 47). The reference category (7) consists of young adults born to mothers who never married and never cohabited at birth or later (n = 209).
Although all youth in analysis 2 were born to never-married mothers, some mothers were cohabiting at birth. Although sample sizes did not allow us to separately analyze youth born to cohabiting versus unpartnered mothers, we control for mother’s cohabitation status at birth and incorporate it into the union history categories as follows: categories 1 through 4, representing youth born to never-married mothers who subsequently married include those whose mothers who were, at the time of the children’s birth, already cohabiting with the partners they later married. Categories 5 and 6, representing youth whose mothers never married but cohabited, include those whose mothers were cohabiting with those partners (the children’s biological fathers or new partners) when the children were born. We also include in this analysis (in categories 1–5) 57 youth whose mothers’ cohabitation status at birth was unknown and include an “unknown” category in the cohabitation status control variable. Category 7 (the reference category) is limited to youth whose mothers never married and never cohabited at birth or later. Alternative specifications, including those in which youth whose mothers cohabited at birth were included in the reference category, did not alter the pattern of results. The distribution of mother’s union history by race among adolescents born to never-married mothers is presented in Table 2.
Distribution of Mother’s Postbirth Union Histories by Race among Adolescents Born to Never-Married Mothers for Analysis 2 (Table 4).
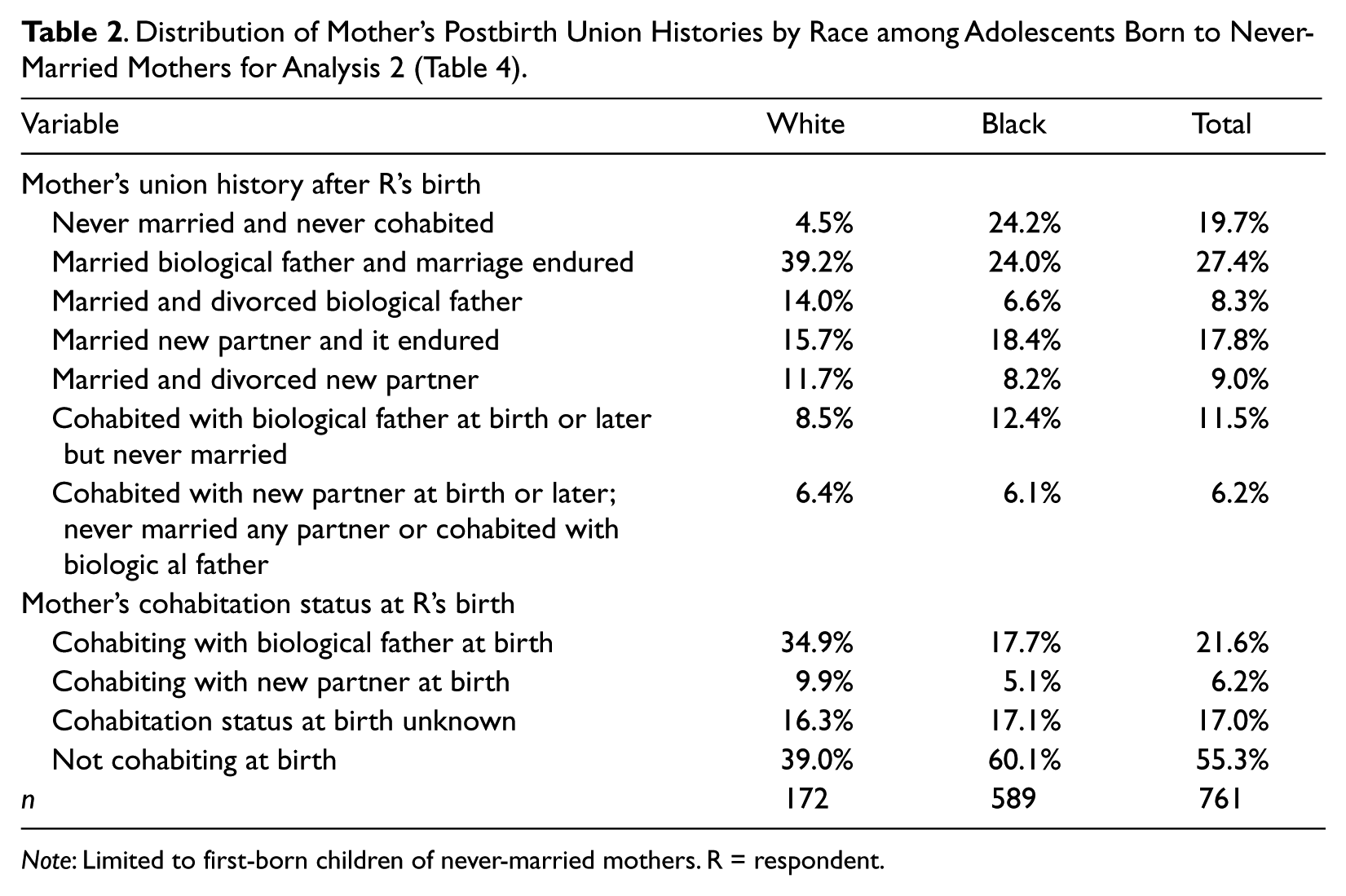
Note: Limited to first-born children of never-married mothers. R = respondent.
Control variables
To minimize the probability that observed associations of mother’s union status with adolescent health are spurious, we control for a range of variables that prior research and theory suggest are predictive of both mother’s union history and later child health. Background variables that occur prior to or contemporaneously with a child’s birth include the following characteristics of the adolescent’s mother: race (1 = non-Hispanic black, 0 = non-Hispanic white), age, cohabitation status (cohabiting, not cohabiting, or unknown) at the child’s birth, cognitive ability (1980 Armed Forces Qualification Test score), family composition at age 14 years (1 = lived with both biological parents), poverty status at baseline (1 = in poverty, on the basis of whether the family income was below the federal poverty income guidelines for the particular family size in 1978), and her mother’s (i.e., the adolescent’s maternal grandmother’s) years of education. Controlling for characteristics of the adolescent or mother measured after the adolescent’s birth would underestimate the gross effect of our primary independent variables because many such characteristics are likely mechanisms through which the consequences of mother’s union status at birth for adolescent health are produced. We control for only two adolescent characteristics, neither of which are influenced by mother’s union status: sex (1 = female, 0 = male) and the age at which the dependent variable is measured (16, 17, 18, or 14 or 15 [reference]).
Analysis Plan
We use ordinary least squares regression to predict logged depressive symptoms, logistic regression models to predict the probability of reporting fair or poor health, and ordered probit models when using the five-category measure of self-assessed health. We imputed missing data using the chained equations program for STATA (Royston 2005), and the cases imputed in each analysis are detailed below.
Analysis 1 (Table 3)
We first examine the long-term consequences of being born to a never-married mother compared with a married mother for adolescent health and well-being. Although the NLSY79 includes data on all children born to female respondents, we limit all analyses to first-born children because many children from higher order births have not yet aged into the young adult sample (i.e., reached age 14 or 15 years by 2010; born by 1996) and those who have were disproportionately born to younger mothers. As of 2010, the NLSY79 had interviewed 2,870 young adults who were the first-born children of NLSY79 mothers and were born between 1977 and 1994. We exclude 612 youth born to Hispanic mothers because there were too few cases in each union history category to analyze separately in Analysis 2. Of the 2,258 offspring eligible for inclusion, 7.3 percent were excluded because of missing data on one of the dependent variables (n = 168) or on mother’s union status at birth (n = 57), leaving a total sample size of 2,033 for the first part of our analysis (Tables 3 and 4). We imputed missing data on the following measures of the adolescent’s mother’s background: cognitive ability (3.6 percent [n = 74]), 1979 poverty status (6.3 percent [n = 128]), and her mother’s educational attainment (5.4 percent [n = 110]).
Adolescent Depressive Symptoms (logged), Level of Self-Assessed Health, and Probability of Fair or Poor Self-Assessed Health Regressed on Mother’s Union Status at Birth (n = 2,033).
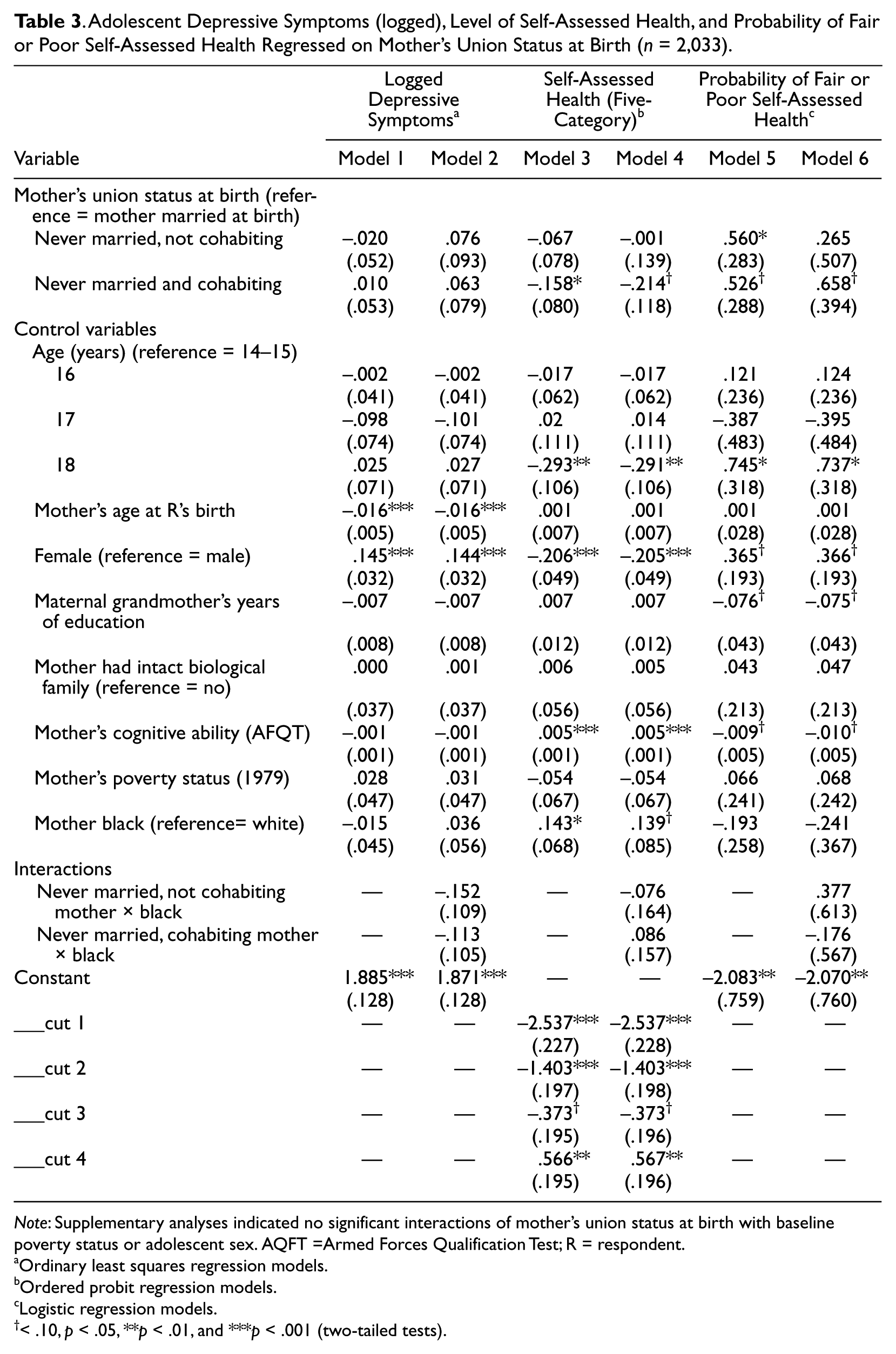
Note: Supplementary analyses indicated no significant interactions of mother’s union status at birth with baseline poverty status or adolescent sex. AQFT =Armed Forces Qualification Test; R = respondent.
Ordinary least squares regression models.
Ordered probit regression models.
Logistic regression models.
< .10, p < .05, **p < .01, and ***p < .001 (two-tailed tests).
Coefficients from Models Estimating the Association of Mother’s Union Transitions with Logged Depressive Symptoms, Probability of Fair or Poor Self-Assessed Health, and Self-Assessed Health (five-category) among Black and White Adolescents Born to Never-Married Mothers.
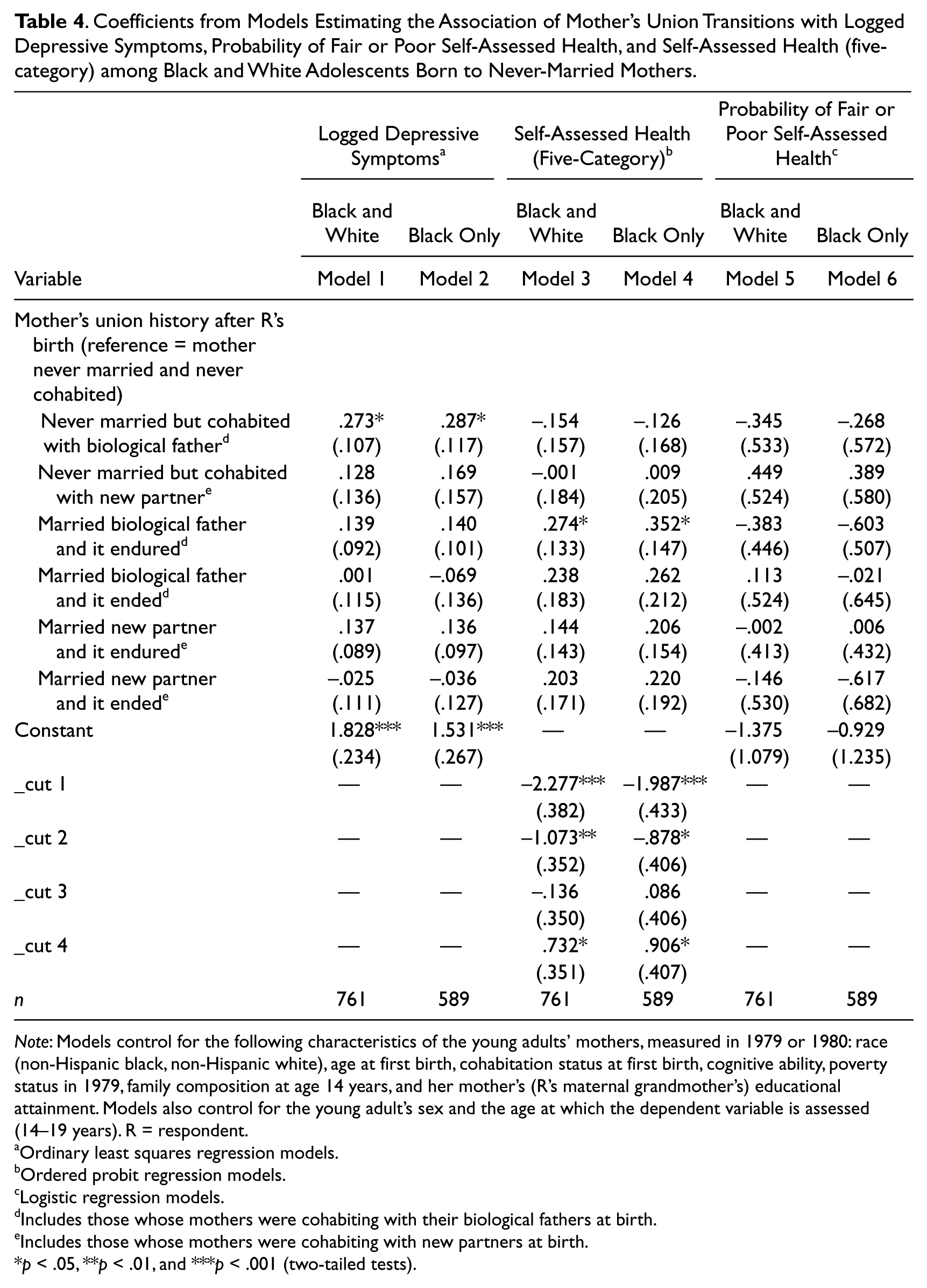
Note: Models control for the following characteristics of the young adults’ mothers, measured in 1979 or 1980: race (non-Hispanic black, non-Hispanic white), age at first birth, cohabitation status at first birth, cognitive ability, poverty status in 1979, family composition at age 14 years, and her mother’s (R’s maternal grandmother’s) educational attainment. Models also control for the young adult’s sex and the age at which the dependent variable is assessed (14–19 years). R = respondent.
Ordinary least squares regression models.
Ordered probit regression models.
Logistic regression models.
Includes those whose mothers were cohabiting with their biological fathers at birth.
Includes those whose mothers were cohabiting with new partners at birth.
p < .05, **p < .01, and ***p < .001 (two-tailed tests).
Analysis 2 (Table 4)
Models estimating the health of adolescents born to never-married mothers as a function of mothers’ subsequent union histories are limited to the 761 (589 black and 172 white) young adults born to never-married black or white mothers. This analysis includes youth who were born to never-married cohabiting mothers, although we control for mother’s cohabitation status at birth. We imputed missing data on the following measures of the adolescent respondent’s mother’s background: cognitive ability (3.4 percent [n = 26]), 1979 poverty status (5.7 percent [n = 43]), and her mother’s (i.e., the youth’s maternal grandmother’s) educational attainment (7.9 percent [n = 60]). As shown in Table 2, small sample sizes in some categories among white unmarried mothers prohibit us from directly comparing children born to black versus white unmarried mothers, so we explore whether the general patterns observed in the total sample differ for black adolescents.
Results
The results in Model 1 in Table 3 indicate that youth born to never-married mothers, regardless of cohabitation status at birth, do not have significantly higher levels of depressive symptoms in adolescence than youth born to married mothers, after controlling for a wide range of maternal background characteristics. Tests of the interaction of mother’s union status with race in Model 2 and other supplementary analyses (available on request) indicate that these patterns do not differ by race, baseline poverty status of the mother, or sex of the adolescent.
Ordered probit models predicting the five-category indicator of self-assessed health (Models 3 and 4) and logistic regression models estimating the probability of reporting fair or poor adolescent self-assessed health (Models 5 and 6) are estimated next. Although the specific pattern of results differs depending on the way the dependent variable is measured, the general pattern of findings indicates that youth born to both cohabiting and noncohabiting unmarried mothers have worse self-assessed health in adolescence than youth born to married mothers. For example, Model 3 indicates that, even when controlling for an extensive array of maternal background characteristics, youth born to never-married cohabiting mothers report lower levels of health in adolescence than those born to married mothers. This same pattern is found in the logistic regression models predicting the dichotomous indicator of fair or poor health (Model 5), although this coefficient reaches only a marginal level of significance. Model 5 also indicates that compared with youth born to married mothers, youth born to noncohabiting never-married mothers are more likely to report low levels of health (fair or poor) in adolescence than are youth born to married mothers. Supplementary analyses using “mother never married and never cohabited” as the reference category indicated no significant differences between youth born to never-married mothers who cohabited at birth and those who were unpartnered at birth in the coefficients predicting either measure of self-assessed health, suggesting that the health of youth born to cohabiting mothers is more similar to that of youth born to unpartnered mothers than to the health of youth born to married mothers. Analyses in Model 4, Model 6, and supplementary analyses (available on request) indicate that none of the associations in Table 3 differ by race, sex, or the baseline poverty status of the mother.
Our second aim is to identify the association of mother’s subsequent union histories with the health of adolescents who were born to unmarried mothers, with attention to marital stability and paternity status of mothers’ partners. In other words, whereas the focus of the analysis in Table 3 was on estimating the consequences of maternal union status at birth, this analysis focuses on maternal union history after the child’s birth among those born to never-married mothers. Because sample sizes prohibited us from differentiating youth by mother’s cohabitation status both before and after the birth, our analysis is limited to black and white adolescents who were born to never-married cohabiting or noncohabiting mothers, and models control for mother’s cohabitations status at birth. Results of ordinary least squares models predicting logged depressive symptoms (Models 1 and 2), ordered probit regression models predicting the ordered five-category measure of self-assessed health (Models 3 and 4), and logistic regression models predicting the probability of reporting fair or poor health (Models 5 and 6) are presented in Table 4. Models control for the same set of background characteristics as shown in Table 3 plus the cohabitation status of the mother at the adolescent’s birth. Odd-numbered models pertain to black and white youth combined and even-numbered models to the black subsample.
The general conclusion from Table 4 is that, with two exceptions, mothers’ subsequent union histories have little consequence for the mental and physical health of black or white adolescents born to unmarried mothers. Those whose mothers remained unpartnered throughout their youth report similar levels of depressive symptoms (Models 1 and 2) and probabilities of reporting fair or poor health (Models 5 and 6) than those whose mothers married their biological fathers or new partners, regardless of whether the marriage endured, and these patterns persist in the black subsample. However, youth born to unmarried mothers who cohabited with their biological fathers reported more depressive symptoms in adolescence than their counterparts whose mothers remained unpartnered and did not enter new cohabiting unions (Model 1; combined black and white sample) and this association persists in the black subsample (Model 2).
The second exception is shown in Model 3, which suggests some benefits of unmarried mothers’ subsequent marriages for their offspring when the five-category indicator of self-assessed health is used. The analysis in Model 4 replicates Model 3 among black adolescents and produces similar results. Black youth born to unmarried mothers who subsequently entered enduring unions with their biological fathers report better self-assessed health than those whose mothers remained unpartnered. Determining whether this association persists for white youth is difficult given the small sample sizes in union history categories, although supplementary analyses (not shown) limited to whites suggests a smaller coefficient. Thus, the apparent benefits of mother’s subsequent enduring marriage to the biological father for adolescent self-assessed health (five-category) in the combined sample may be limited to black youth, although further testing of this hypothesis must await future data with a larger sample of white unmarried mothers. Still, it is important to note that these apparent benefits are limited to youth whose mothers married their biological fathers and remained married to him throughout their childhood and as shown in Models 5 and 6, potential benefits of the mother entering and remaining in a marriage with the biological father do not appear to differentiate youth with the most extreme levels of poor health.
Discussion
High rates of nonmarital fertility in the United States led us to investigate two research questions: Does nonmarital fertility have long-term negative health consequences for offspring in adolescence? Do mothers’ subsequent union experiences, including marriage, improve the health outcomes in adolescence of children born to unmarried mothers? Our first conclusion is that compared with youth born to married mothers, black and white adolescents who were born to unmarried mothers have worse self-assessed health but similar levels of depressive symptoms compared with youth born to married mothers. Although the association with adolescent health of being born to a cohabiting or unpartnered versus a married mother differs depending on how self-assessed health is measured, the general pattern of findings is one of health disadvantage associated with mother’s unmarried status, regardless of whether she was cohabiting. That is, youth born to cohabiting mothers appear to have adolescent health assessments that are more similar to those of youth born to unpartnered mothers than to those of youth born to married mothers. Our findings extend the vast body of research showing that growing up in a single-parent home poses substantial risks to the well-being of children across a range of behavioral, educational, and psychosocial outcomes throughout the life course (see Amato 2010; Cherlin, Chase-Lansdale, and McRae 1998; McLanahan and Sandefur 1994). Our study is the first to demonstrate that this pattern extends into adolescence for children born to unmarried mothers, at least in terms of their self-assessed health.
That we find few race differences in the consequences of having been born to an unmarried mother is somewhat inconsistent with studies that indicate that living in a single-parent home has fewer negative consequences for the well-being of black compared with white children (Dunifon and Kowaleski-Jones 2002). However, our study differs from most past research because we examine differences in adolescent self-assessed health and focus specifically on children born to never-married mothers as opposed to children living in single-parent homes after divorce. Our findings suggest that being born to an unmarried mother, even an unmarried cohabiting mother, may have negative consequences for adolescent health regardless of race.
In contrast to the findings for self-assessed health, we find no evidence of enduring negative consequences of being born to an unmarried mother for adolescent mental health, at least as measured by depressive symptoms, after controlling for a range of maternal background characteristics. These findings may be seen as a caveat to decades of research, based largely on children of divorce (Dunifon 2009; Sweeney, Wang, and Videon 2009), which has found that growing up without both biological parents is associated with a range of negative outcomes throughout the life course (Amato 2010). Our analyses suggest that negative mental health outcomes in adolescence do not extend specifically to children born to unmarried mothers. Still, psychological distress in adolescence may be expressed in multiple ways, including behavioral outcomes such as alcohol and drug use and other forms of risk-taking behavior. Future research should consider whether our findings for depressive symptoms extend to other indicators of psychological well-being, achievement, and externalizing behavior.
Our second central finding is that, on average, mothers’ subsequent unions have few consequences, positive or negative, for any of our measures of the mental or physical health of adolescents born to unmarried mothers. One notable exception is when mothers subsequently marry and remain married to biological fathers, which is associated with better adolescent self-assessed health than when mothers remain unpartnered. Even here, however, the estimated effects are small and do not significantly differentiate youth with the worst (i.e., fair or poor) self-assessed health from others. Adolescents whose mothers marry and divorce their biological fathers, marry new partners, or cohabit without marrying have levels of self-assessed health that are no different from those whose mothers remain unpartnered.
It is telling that any physical health benefits of a mother’s marriage accrue only to adolescents whose mothers marry their biological fathers and remain in the union. It is well known that children in stepfamilies have more negative developmental, educational, and behavioral outcomes than children with two continuously married parents but do not differ on average from children of single parents (Acs 2007; Cavanagh 2008; Deleire and Kalil 2002; Sweeney et al. 2009). Our study indicates that this pattern applies specifically to adolescents born to never-married mothers and suggests that for these youth, the introduction of a stepfather in the home offers no greater benefits to adolescent health than living with a continually unpartnered mother. In addition, consistent with research indicating that mothers’ relationship instability undermines the well-being of children born to unmarried mothers (Osborne and McLanahan 2007), we find that their mothers’ subsequent marriages to their biological fathers only benefit adolescents’ health if the marriages endure.
The observed benefits to children’s self-assessed health associated with their mothers’ marrying their biological fathers, but not new partners, may partially reflect the timing of the marriage. Bzostek, McLanahan, and Carlson (2012) found that only 21.6 percent of unmarried mothers in the Fragile Families and Wellbeing Study entered coresidential relationships (either cohabitation or marriage) with new partners within 5 years of the children’s birth, whereas 37.6 percent were cohabiting with or married to the biological fathers. Although comparable data on the timing of marriage to the child’s biological father are not available, it is likely that such marriages occur sooner after the child’s birth than marriages to new partners. Thus, children in these households (particularly those whose parents remain married) likely spend less time in single-parent homes than children whose mothers marry stepfathers, thereby reducing their exposure to family instability, a primary mechanism through which nonmarital fertility likely undermines child health in the first place (Bzostek and Beck 2011). As Gibson-Davis (2011) surmised, “From the child’s perspective, the timing of marriage may be just as important as the event of marriage” (p. 267). An important avenue for future research is to consider the influence of time spent in a single-parent home and in various other household structures for the well-being of offspring across the life course.
Our third central finding is that, among youth born to unmarried mothers, mother’s cohabitation with the biological father (either at birth or later) is linked to more depressive symptoms in adolescence than living with a continually unpartnered mother. It is likely that children whose mothers cohabited experienced substantial instability throughout their lives including the dissolution of their mothers’ cohabiting unions to their fathers (Lichter, Qian, and Mellott 2006; Manlove et al. 2012; McLanahan 2011) and multiple subsequent cohabiting unions. Because of small group sizes, we were unable to distinguish children whose mothers cohabited with one versus multiple partners or children whose mothers had one versus multiple divorces. Given the rising prevalence of serial cohabitation (Cohen and Manning 2010; Lichter, Turner, and Sassler 2010), particularly among the disadvantaged, future research should focus specifically on its consequences for the long-term well-being of offspring. Still, it is unclear why mother’s cohabitation (without marriage) with the biological father would be associated with more depressive symptoms, whereas mother’s cohabitation with a new partner or marriage followed by divorce is not. It may be that mothers who repartner have higher standards for new partners (Bzostek et al. 2012; Edin and Kefalas 2005), perhaps leading to a lower degree of conflict within the household than within a continuously cohabiting two–biological parent household. The cross-sectional evidence suggests that unmarried mothers’ new partners are often highly involved with their stepchildren and that children reap benefits from this social fathering (Berger et al. 2008).
It is important to note that our focus on examining longer term outcomes for youth in adolescence required us to limit our analysis to youth born no later than 1996. Demographic changes in family formation patterns may affect the extent to which our findings can be reliably generalized to more recent cohorts. For example, cohabiting at the time of the birth was far less prevalent in the 1980s, when the majority of youth in our sample were born (Musick 2002; Raley 2001), particularly among black women, who make up the largest share of nonmarital births in our sample (Raley 1996). As of the first decade of the twenty-first century, however, nearly 60 percent of nonmarital births occur to women in cohabiting unions (Martinez et al. 2012). The more normative status of births in cohabiting unions may mean that being born to an unmarried cohabiting mother has fewer negative long-term consequences for adolescent health than we observe. On the other hand, there is some evidence that cohabitation disruption rates are higher among more recent cohorts (Lichter et al. 2006) who are more likely to end their relationship with the baby’s father than to marry him (Lichter et al. 2006; Manlove et al. 2012; McLanahan 2011). Furthermore, black cohabiting parents have the lowest relative risk for transitioning to marriage (Manlove et al. 2012). In summary, we might see more negative consequences were we to focus on more recent cohorts and specifically on those who experienced multiple cohabiting unions (Williams et al. 2008).
Conclusion
Our results suggest that being born to an unmarried compared with a married mother may have some negative long-term consequences for adolescent self-assessed physical health, but not adolescent depressive symptoms. However, with one exception, mothers’ subsequent marriages or cohabiting unions offer few advantages over stability in an unpartnered state for the health of adolescents born to unmarried mothers. Our findings suggest that although healthy, enduring marriages between biological parents of children born to unmarried mothers may have some limited positive consequences for the self-assessed health of offspring in adolescence, they do not appear to protect such adolescents from the most extreme health problems. Even here, however, selection remains a concern: Although the NLSY79 data allow us to control for a wide range of mothers’ background characteristics, it remains possible that unobserved characteristics that both select unmarried mothers into marriage with biological fathers and shape child health explain these patterns. However, even if healthy and enduring marriages between biological parents after a nonmarital birth have positive causal effects on the health of children born to unmarried mothers, such unions are increasingly rare, and the likelihood of successfully facilitating such unions in the future remains an open question. If, as we conclude here, nonmarital fertility poses some risks to the long-term health of offspring, and mother’s subsequent marriage, even to the biological father, offers only limited benefits, it is vitally important for future studies to identify factors with greater promise to improve the health of the growing numbers of youth born to unmarried mothers.
Footnotes
Acknowledgements
We are grateful for the support of the Institute for Population Research at The Ohio State University and the Netherlands Interdisciplinary Demographic Institute.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant R01HD054866 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Child Health and Human Development or the National Institutes of Health.