
Abstract
According to Bird and Rieker’s sociology of constrained choices, decisions and priorities concerning health are shaped by the contexts—including policy, community, and work/family—in which they are formulated. While each level received attention in the original and subsequent research, we contend their constrained choices theory provides a powerful multilevel framework for modeling health outcomes. We apply this framework to tobacco clean air restrictions, combining a comprehensive database of tobacco policies with the National Longitudinal Survey of Youth 1997 from ages 19 to 31. Using multilevel panel models, we find that clean air policies lower the odds of past 30 day smoking and dependence while controlling for other policy-, city-, and individual-level constraints. We also find unique between- and within-person effects, as well as gender effects, for the constraint levied by smoking bans. We argue for the theory’s broad applicability beyond commonly cited findings regarding gender and biological influences.
Keywords
In their influential 2008 book, Bird and Rieker introduced a sociology of constrained choices. According to this theoretical paradigm, decisions and priorities concerning health are influenced by the contexts in which they are formulated; such contexts differentially introduce various constraints on decision making and ultimately, health behaviors. Bird and Rieker (2008) consider three levels of contextual constraints: policy, community, and work/family. Each level of constraints affects individual choices and biological processes. Choices and biological processes reciprocally affect one another, which in turn affect health outcomes. While the original and subsequent research makes the case for each level, respectively, we contend that their model also provides a powerful multilevel framework that, when combined with analogous statistical methods, allows scholars to consider a broad range of constraints simultaneously.
We use the case of tobacco clean air restrictions, known colloquially as smoking bans, to analytically demonstrate the applicability of a multilevel approach to constraints. We test the ability of policy—at both the state and local levels—to affect individual-level health behaviors while also considering community, work, and family constraints. To achieve this aim, we combine a comprehensive database of tobacco ordinances within the United States with the geocoded National Longitudinal Survey of Youth 1997 (NLSY97) and census data. We begin by describing Bird and Rieker’s (2008) constrained choices framework while elucidating how a multilevel approach applies. We then consider the case of clean air restrictions and why they cohere with the concept of constrained choices, building on Bird and Rieker’s (2008) suggestion that scholars should consider the effects of specific policy constraints. Our results show support for the effects of clean air policies on young people’s smoking, including within- and between-person effects and particular effects by gender. In addition to this important empirical contribution, we use these findings to demonstrate the utility of simultaneously considering constraints at multiple analytic levels.
Background
Sociology of Constrained Choices as Multilevel
Bird and Rieker (2008) ask a relatively straightforward question: What influences how individuals prioritize health? They argue that individuals experience numerous contextual constraints that affect such prioritization; consequently, individuals do not usually make decisions solely based on the best interest of short- or long-term personal health. Rather, competing priorities and constraints imposed by inhabited social contexts can cumulatively limit options or opportunities, shaping how individuals or families “choose” healthy behaviors. While some constraints impact relatively overt choices between health and another prioritization such as family, others restrict agency in the decision; for example, community-level constraints may inhibit exercise, limit child care options, or impede knowledge on how to make healthier choices. Conversely, constraints can also facilitate healthy choices by restricting practices that lead to unhealthy outcomes (e.g., toxic dumping) or prohibiting specific unhealthy behaviors (e.g., driving intoxicated). Importantly, changes in constraints also occur over time, such that a longitudinal approach best captures this dynamic as it unfolds over the life course of a given cohort (Frohlick and Abel 2014).
We present Bird and Rieker’s (2008:64) model in Figure 1 as it applies to the case of tobacco use. Despite not yet explicitly applied as such, this representation and language throughout their book suggest a multilevel model. Individual-level outcomes result from a nested structure whereby work/family constraints are nested in community-level constraints, which are subsumed within policy-level constraints. These layers of context interact to differentially shape how individuals make decisions. We describe the importance of each level in turn.
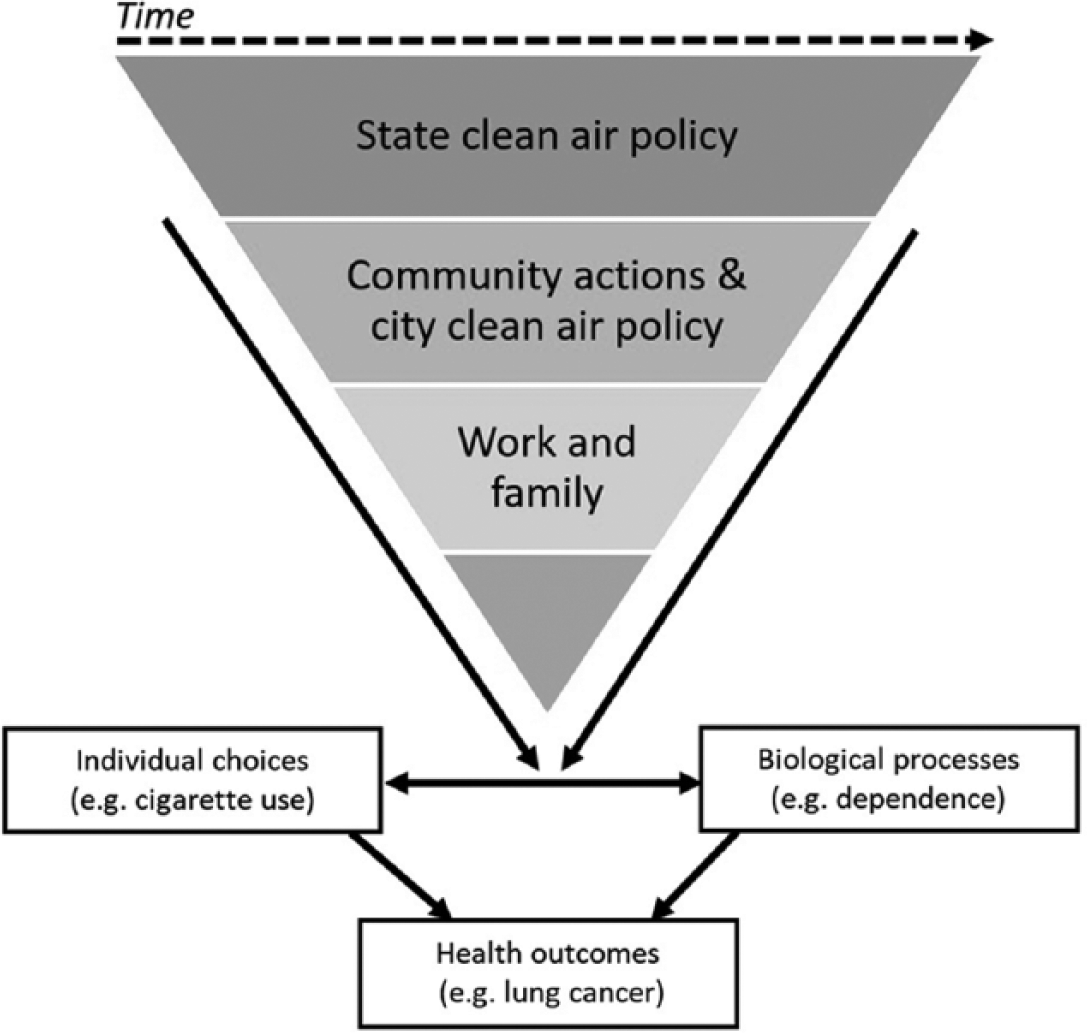
Bird and Rieker’s (2008) Conceptualization of a Sociology of Constrained Choices Applied to Clean Air Restrictions and Tobacco Use.
At the top, Bird and Rieker (2008) emphasize the importance of policy in constraining and facilitating health choices. In this area, the constrained choices framework has incredible value but has been underutilized. Bird and Rieker (2008) broadly consider policy by focusing on cross-national “regime” differences rather than specific policy-behavior matches but note this as an important next step. Although only discussing cross-national differences, they are careful to note that multiple levels of government each control some dimensions of policymaking, such that policy itself should be approached from a multilevel perspective. Accordingly, one goal of their theory is to “identify state and local policy levers and the ways in which decisions at different governmental levels can affect individual choices, behavior, and health outcomes” (Bird and Rieker 2008:124). In sum, multiple levels of policy provide contexts that shape decision making, and ultimately health behaviors.
At the community level, the model emphasizes the physical environment and available resources that may operate as constraints on health behaviors, although these effects are not universal (Meijer et al. 2012). Such factors include physical decay, signs of disorder, and social aspects such as cohesion and trust (for a review, see Sampson, Morenoff, and Gannon-Rowley 2002; also, Altschuler, Somkin, and Adler 2004; Browning and Cagney 2002; Browning et al. 2013; Dupéré, Leventhal, and Vitaro 2012; Ross and Mirowsky 2009). In terms of resources, those who live in communities marked by socioeconomic disadvantage are at greater risk for health problems (for a review, see Robert 1999; also, Carpiano 2006; Leclere, Rogers, and Peters 1998; Wen, Browning, and Cagney 2003). Often, the community acts as a constraint by directly affecting health outcomes (e.g., pollution, Astell-Burt et al. 2013) or restricting the ability to prioritize health (e.g., spatial limitations on physical activity, Ewing et al. 2014). In other cases, community-level effects manifest as sources of increased stress, which in turn affect health outcomes, including substance use (Taylor and Repetti 1997). As stated previously, policy can act within communities as a constraint in a similar manner.
At the individual level, the constrained choices framework emphasizes restrictions and stressors related to work and family that influence how people prioritize health. Research has demonstrated a health benefit for married individuals, though no physical health benefits for parents (see Ross, Mirowsky, and Goldsteen 1990). Recent research, however, has questioned the extent to which the marriage effect is due to other factors, such as self-selection, martial dissolution, marriage quality, and age (Umberson et al. 2006). Childfree individuals report lower levels of depression than those with children (Evenson and Simon 2005); this effect is likely due to increased social and economic burdens for parents (Bird 1997). Work can have both positive and negative effects on health. Work can be both intrinsically and extrinsically rewarding in a manner that promotes health, including among young people (Mortimer, Harley, and Staff 2002), or impairs health if it includes irregular or overnight shifts or long hours (Knutsson 2003). Thus, like community-level contexts, work and family may influence health in both direct and indirect ways in shaping decision making. Beyond work/family, socioeconomic factors impact health outcomes. The unequal distribution of resources shapes the uneven distribution of health outcomes, thus emphasizing predictors related to socioeconomic status (Link and Phelan 1995). Socioeconomic status (SES) can operate as a constraint in that lack of access to resources and information may prohibit prioritization of health-promoting behaviors.
The effects of each level of the theoretical model cumulatively and interactively influence health choices, biological processes, and health outcomes (Bird and Rieker 2008). According to Figure 1, constraints directly influence individual-level health choices and related biological processes. For the latter, stress responses are a key example for Bird and Rieker (2008), given noted differences by gender. Choices and biology also reciprocally affect one another; these each then affect health outcomes.
Bird and Rieker (2008) argue for the importance of each level respectively on analytic outcomes, describing past studies and original analyses that almost exclusively consider a single level. While there is little doubt that they would argue that all levels matter simultaneously and interactively, few empirical studies have tested this framework, and those that do have compartmentalized by level (e.g., Fan et al. 2015; Flood and Moen 2015; Gorman, Read, and Krueger 2010). In fact, most citations use their book only to support theoretical acknowledgements that gender matters, that biology interacts with social factors, or to broadly argue that constraints affect health (e.g., Cullati, Courvoisier, and Burton-Jeangros 2014; Hankivsky 2012; Hill and Needham 2013; Masters, Link, and Phelan 2015; Needham and Hill 2010; Payne 2014; Read and Gorman 2010; Shreffler et al. 2015; Umberson et al. 2014) rather than to empirically test the applicability of the framework, particularly in a multilevel fashion.
To fully understand these contextual processes, we argue that each level deserves consideration in assessments of constraints on health outcomes, which is made possible by current statistical capabilities in multilevel modeling. While we would not argue against the importance of gender in health research and the renewed focus on gender brought about by Bird and Rieker’s (2008) work, there is little reason to limit the focus to gender when considering policy contexts as a constraint—although we do examine gender differences in our outcomes. By primarily focusing on unique levels and gender or biology, however, we believe the constrained choices framework has been underutilized. The emphasis on morbidity and mortality has also led health choices among young people to be relatively underexamined from the perspective of such constraints. As such, we aim to expand the applicability of Bird and Rieker’s (2008) theorization with an examination of tobacco clean air restrictions over time among young people.
Clean Air Restrictions as a Constraint
As noted previously, Bird and Rieker (2008) assert that research on policies as constraints should focus on specific policies across analytic levels. Further, substance use is a central example of an outcome used to argue for their theory, particularly given differences by gender. Since Bird and Rieker (2008:65) indicate that “antismoking policies aimed at improving public health intentionally constrain individual choices related to smoking behavior,” such policies provide an interesting case to consider these issues further. Returning to Figure 1, we elucidate how the constrained choices framework applies to tobacco use.
Research on antismoking policies supports Bird and Rieker’s assertion that such ordinances may constrain individual smoking choices and improve public health. Although once considered glamorous (Brandt 1998), the denormalization of tobacco use in Western nations led to declines in both smoking and its public acceptability by marshalling stigma in an effort to serve the broader public health (Bayer and Stuber 2006). Clean air policies, such as those within bars and nightclubs, have been described as intensifying the process of denormalization of smoking among young people (Kelly 2009). Given the rapid change in attitudes toward smoking and clean air restrictions, this constraint on the spaces in which smoking can occur provides a useful test of a specific policy constraint within a multilevel framework that concurrently accounts for contextual constraints at other levels in the theoretical model.
Despite theorizing on denormalization and the rapid change in the enactment of smoking bans, surprisingly little empirical research examines the effect of these policies on individual-level tobacco use over time. After a spate of early research on workplace bans and employee smoking (see Fichtenberg and Glantz 2002), other studies have inferred ban effects through cohort effects (Boardman, Blacklock, and Pampel 2010), relied on cross-sectional or aggregate data (Chahine, Subramanian, and Levy 2011; Levy, Romano, and Mumford 2005; McMullen et al. 2005; Vuolo 2012), considered only one level of policy implementation (Chahine et al. 2011; Nagelhout et al. 2011; Vuolo 2012), or used data within a single locality (Biener et al. 2010; Klein et al. 2009; Seigel et al. 2004). By examining the impact of comprehensive smoking bans at the state and local levels over time among a nationally representative sample of young people while controlling additional relevant tobacco policies, our study overcomes these past limitations and incorporates suggested emphases on multiple local policies over time (Friend, Limmerman-Kreda, and Grube 2011).
Importantly among these limitations, we address Bird and Rieker’s (2008) underexplored emphasis on the need to consider policy at multiple levels of implementation by considering smoking bans across governmental levels. Thus, we construe smoking bans as not only operating at a national or state policy level but as a community-level characteristic. In the United States, the diffusion of clean air regulations began at the local level and spread vertically up to the state, an unusual example of “bottom-up federalism” (Shipan and Volden 2006). In multilevel analyses, finding weak effects for state-level contextual variables, Chahine and colleagues (2011:757) suggested this may be because “contextual covariates play a larger role more locally, for example at the level of towns or neighborhoods. This may especially be the case for indoor smoking restrictions, which are highly variable within states.” They further suggest that future research should consider contextual variables at the local level to “fully characterize social determinants of smoking variability across populations and places” (p. 758). Thus, it is fitting in this case to consider policy itself as a multilevel phenomenon.
Bird and Rieker (2008) also highlight a subtle difference between policies that target attitudes versus those that target behaviors. Policies that target attitudes may perpetuate or increase health disparities because higher status individuals can more easily use resources to align behavior with prescribed attitudes. By contrast, policies that restrict behavior, including smoking bans, are “protective health measures that do not rely on individual motivations or social capital . . . [and] can be an effective and efficient way to bypass social inequalities and also protect and improve public health” (Bird and Rieker 2008:205). Others suggest that the denormalization of smoking produces stigma that causes more harm than good among socioeconomically disadvantaged smokers (Bell et al. 2010), which is particularly concerning since smoking is more prevalent and contributes to decreased life expectancy among lower SES individuals (Ho and Fenelon 2015; Killoran, Owen, and Bauld 2006). Subsequently, in the specific case of tobacco use, the work on denormalization posits that we might expect larger policy effects among the advantaged. Within the constrained choices framework, we would expect fewer differences by such fundamental causes (Link and Phelan 1995). Such discrepancies emphasize the importance of considering the interactive effect of constraints with durable sources of disadvantage. Notably, the central argument of Bird and Rieker’s (2008) theory is that gender is not a fundamental cause, and thus differences in outcomes by gender and policy are to be expected (Dedobbeleer et al. 2004), again emphasizing the interactive nature of the theory.
One advantage to approaching the effect of clean air policies from a multilevel constrained choices perspective is the ability to simultaneously consider multiple constraints that young adults face in the decision to smoke tobacco. For instance, other community characteristics, aside from policy, may provide important constraints. For example, lower neighborhood SES is associated with lower rates of adolescent smoking (Ennett et al. 1997). Yet, the more rapid recent decrease in smoking prevalence among those with higher income (Killoran et al. 2006) may lead to aggregate patterns whereby higher SES areas are associated with lower smoking rates.
At the individual level, numerous studies support the inclusion of additional constraints, including Bird and Rieker’s (2008) focus on work and family. Marital status, parenthood, and living arrangements in adolescence and young adulthood each influence smoking patterns (Bachman et al. 1997; Brown and Rinelli 2010; Fleming, White, and Catalano 2010). Adolescents who work are more likely to smoke than those who do not, with work intensity increasing smoking among white youth specifically (Johnson 2004). Potentially related to stressors associated with work and family, mental health is a significant predictor of smoking (Swan et al. 2004). Although not discussed at length, Bird and Rieker (2008) recognize the importance of peers for creating constraints, particularly for young people. Peers’ ability to constrain substance use (see Warr 2002) is a cornerstone in studies of deviance. Additionally, academic achievement predicts smoking, with high school grade point average inversely related to later cigarette use (Schulenberg et al. 1994).
Several measures of socioeconomic status (SES) are associated with cigarette use. Parental SES inversely affects adolescent smoking (Friestad et al. 2003; Soteriades and DiFranza 2003), although successfully navigating adult roles may mediate this relationship (Pampel, Mollborn, and Lawrence 2014). There is also a well-established gradient between educational attainment and tobacco use (Bachman et al. 1997; Margolis 2013; Schulenberg et al. 1994). Finally, gender and race are both associated with tobacco use. While historically men smoked at greater rates, steep declines in smoking in recent years have resulted in gender convergence (Pampel 2001). White adolescents are more likely to initiate tobacco use (Johnson and Hoffmann 2000); however, some evidence indicates that cessation occurs at greater rates among whites, resulting in racial convergence in smoking over the life course (Pampel 2008).
In the case of tobacco, we can straightforwardly insert relevant outcomes into the constrained choices framework. We consider the use of any cigarettes to constitute an individual choice, while dependence on the addictive properties of tobacco and resultant smoking behaviors are considered an applicable biological process. The double-headed arrow between these two concepts thus still applies: Dependence will influence an individual’s choice to continue smoking. Finally, the detrimental health effects of such choices and processes are well known; tobacco use is the leading cause of preventable illness and death in the United States (U.S. Department of Health and Human Services 2010). Despite these well-established links between smoking and outcomes such as lung cancer, given our focus on a sample of young people for whom morbidity and mortality has yet to manifest, we do not assess this component of the model. Rather, we concentrate on behaviors related to individual choice and biological processes.
Data and Methods
Individual-level Data: NLSY97
The individual-level data came from the National Longitudinal Survey of Youth 1997 (NLSY97). The NLSY97 has a large, nationally representative, geocoded sample (N = 8,984) designed to track the transition of youth into adulthood. Adolescents ages 12 to 16 were randomly sampled in 1997 and surveyed annually. The retention rate was nearly 83% in 2011. The restricted-access, geocoded NLSY97 identified the respondents’ core-based statistical area (CBSA; i.e., metropolitan or micropolitan area), county, and state. We analyzed a subset of respondents whose city of residence could be identified by combining CBSA and county information with a variable assessing whether the respondent lived in a principal city within the metro area. 1 Thus, we restricted our analyses to those living in the largest principal city of a CBSA, given the importance of the local level within a multilevel policy context. 2 We also restricted analyses to waves 2004 and later (ages 19–31) as this was the first year in which CBSA data are available. 3 This subset amounts to 19,668 observations among 4,341 individuals within 487 cities. 4
Dependent Variables
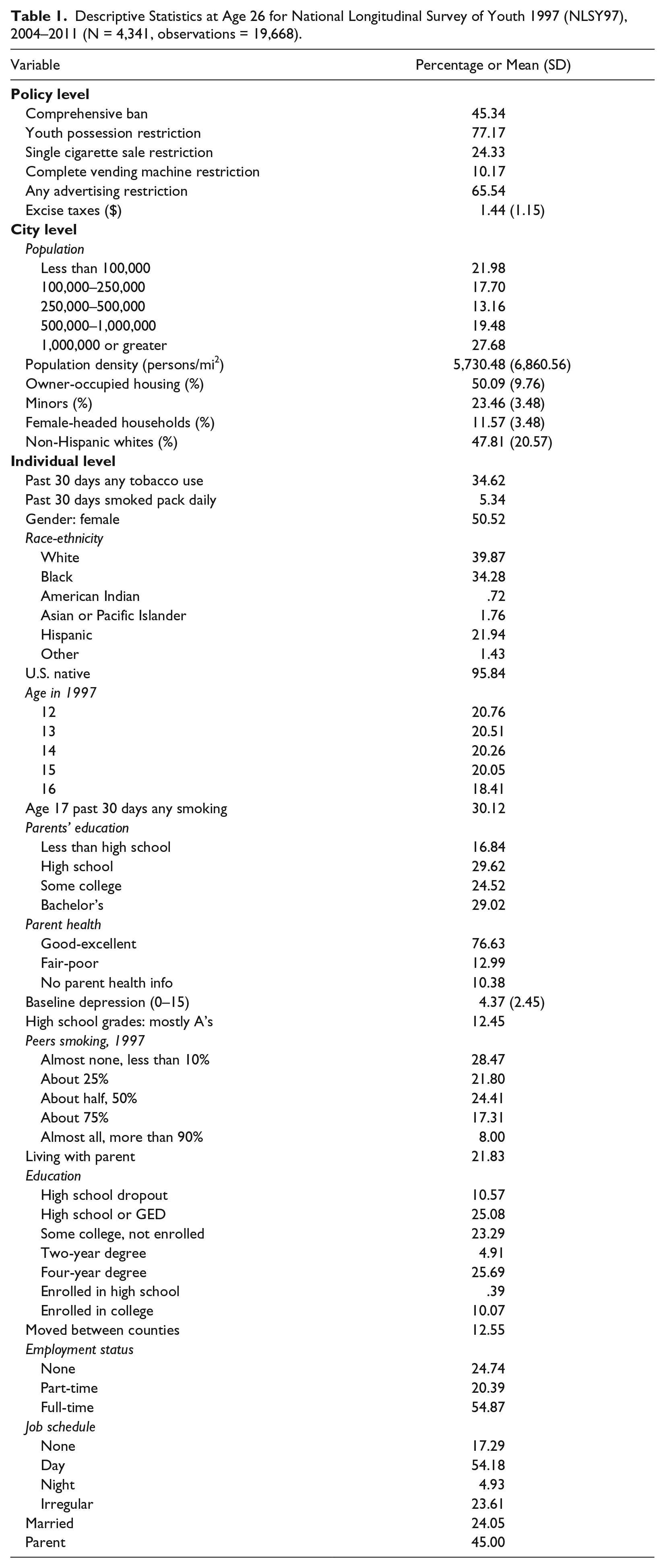
Each year, respondents who indicated they ever smoked an entire cigarette were asked the number of days they smoked during the 30 days prior to the interview and the number of cigarettes they smoked each day on those 30 days. We created two outcome variables: one indicating any past 30 day cigarette use and a second proxy variable for dependency for those who reported smoking at least a pack per day. Table 1 shows the percentage of respondents who indicated yes for each variable at age 26 as well as descriptive statistics for all variables. We report descriptive statistics at age 26 to best represent all respondents given the rapid change in many of these variables from ages 19 to 31. For these dependent variables, 34.6% reported smoking during the past 30 days, while 5.3% reported smoking at least a pack daily.
Descriptive Statistics at Age 26 for National Longitudinal Survey of Youth 1997 (NLSY97), 2004–2011 (N = 4,341, observations = 19,668).
Independent Variables
Motivated by the constrained choices framework and the empirical literature on tobacco use, we included several individual-level variables in the models. In a longitudinal data set, researchers must choose between year and age as the time metric based on theoretical considerations (Yang 2010). Given that age is central to patterns of substance use among young adults, we chose age as our metric. Age in 1997 is also included to control for cohort effects.
Constraints related to family, work, and peers represent the first set of predictors. Regarding family, we included indicator variables for whether the respondent lived with a parent, was married, and had children. We also accounted for recent moves via a dummy variable for a past year move across at least one county. For work constraints, we included categorical variables for job status and job schedule. To assess peer-related constraints, we included the percentage of peers who smoked in 1997, the only year it was measured. For academic performance, we included a dummy variable for receiving “mostly A’s.” 5
Given the pathways at the bottom of Figure 1, we considered health factors that may influence both use and dependence. First, the data set included a five-item scale for depression, of which we use the 2004 baseline measure (alpha = .77). 6 Given that youth who initiate smoking as adolescents have higher odds of smoking, especially heavy smoking, as adults (Wills et al. 2004), we controlled for respondents’ past 30 day smoking status from their age 17 survey. Finally, though we note the lack of parental smoking information is a limitation, we included parents’ self-reported health as a proxy for intergenerational health influences.
We included several measures for socioeconomic status. We measured SES of household of origin by respondent-reported parents’ education level. The respondent’s SES was assessed by a time-varying measure that combined school enrollment status and degree attainment. 7 Finally, we included controls for race-ethnicity, U.S. nativity, and gender.
Policy-level Data: Americans for Nonsmokers’ Rights Foundation
Policy-level data come from the Americans for Nonsmokers’ Rights Foundation (ANRF) tobacco policy database. ANRF collected a complete national repository of tobacco-related ordinances and regulations across the country by date enacted. The main predictor variable is whether or not the respondent lived in a locale with a comprehensive smoking ban, defined as policies mandating that workplaces, bars, and restaurants are 100% smoke-free. From the ANRF repository, we created a location-year data set at the state, county, and city level for each data year. Since higher geographic level policies are not independent of city policy (i.e., a state policy automatically means a city ban, and therefore, the variables must match), we recoded cities within counties or states with bans to reflect this status. Thus, all policy information is statistically at the city level. 8 We used Federal Information Process Standard (FIPS) codes to link the geocoded NLSY97 to ANRF data at the city level, allowing us to determine the tobacco policy context within which respondents were located. Figure 2 shows the percentage of respondents living under a comprehensive ban by year. In 2004, 14.9% of respondents lived in a location with a comprehensive ban. By 2011, that number increased to 58.7%, a rapid proliferation. We used the same procedure to include additional policies as controls that incorporate all the main domains of tobacco control (Friend et al. 2011), including youth possession restrictions, sales restrictions (single cigarette and complete vending machine prohibitions), any advertising restriction, and excise taxes per pack.

Percentage of Respondents Living in a City with a Comprehensive Smoking Ban by Year (N = 4,341, observations = 19,668).
City-level Data: U.S. Census
Several city-level measures from census data are included to account for constraints at that level. To include both population size and density, we created a categorical measure of population, while density is considered continuous (logged due to skewness). We included the percentage of female-headed households, a useful proxy for other economic measures such as poverty and income (LeClere et al. 1998). 9 To measure ties to the community, we used the percentage of owner-occupied housing. Finally, we included the percentage of non-Hispanic whites and percentage of minors to account for community racial and age composition, respectively.
Methods
Given the various levels of analysis and a binary outcome, we used multilevel logistic regression models, also known as mixed effects models, to estimate the effects of constraints on young adult smoking. In our analysis, observations were nested within individuals, which were nested within cities. Individuals can move across cities, such that the data are more akin to a cross-classified multilevel model where observations are cross-classified by both individual and city. Among our analytic sample, only 18% were located among more than one city. 10 Thus, the cross-classification of individual and city represents a very sparse, large matrix. In such cases, the loss in precision of the estimation of the variance components from using the typical multilevel structure is slight relative to the great computational advantage (Goldstein 1999). 11
Our three-level model thus includes random intercepts for both the individual level (Level 2) and the city level (Level 3). These models adjust for the person- and city-level averages through a variance parameter defining a normal distribution for each of those averages. At the lowest level denoting time (Level 1), the predictors represented time-varying measures. At the individual level, we had the time-invariant characteristics of the respondent. Since policy and city characteristics time-vary, they were actually Level 1 variables. These changing characteristics provide an advantage in that they can be decomposed into between- and within-person effects by taking an individual-level average and time-varying centered version of clean air policy. Since we did not include static city characteristics, the random intercept is the only term at Level 3. Despite being statistically at Level 1, the city-level variables still conceptually represented the “city” and “policy” levels of the constrained choices theory, and we categorized them as such for presentation. That is, despite whether a variable is time-varying or time-invariant, we present the results in our tables according to each variable’s place within our theoretical framework rather than the statistical model. Appendices A and B in the online supplemental material (available at http://jhsb.sagepub.com/supplemental) explicitly clarify the relationship between the theoretical and statistical models.
We tested several specifications for age. For any recent cigarette use, the best-fitting model was the quadratic term. According to likelihood ratio tests, the quadratic model had improved fit over a linear specification (χ2 = 7.61, p < .01). Further polynomials and dummies for age offered no improved model fit. We show the predicted values by age in Figure 3, demonstrating steadily high values through age 23, before declining across the late 20s. For daily pack smoking, there was no significant age effect regardless of specification. In other words, there is essentially no change in the probability of dependence beginning at age 19. Nonetheless, we included the squared term for consistency.
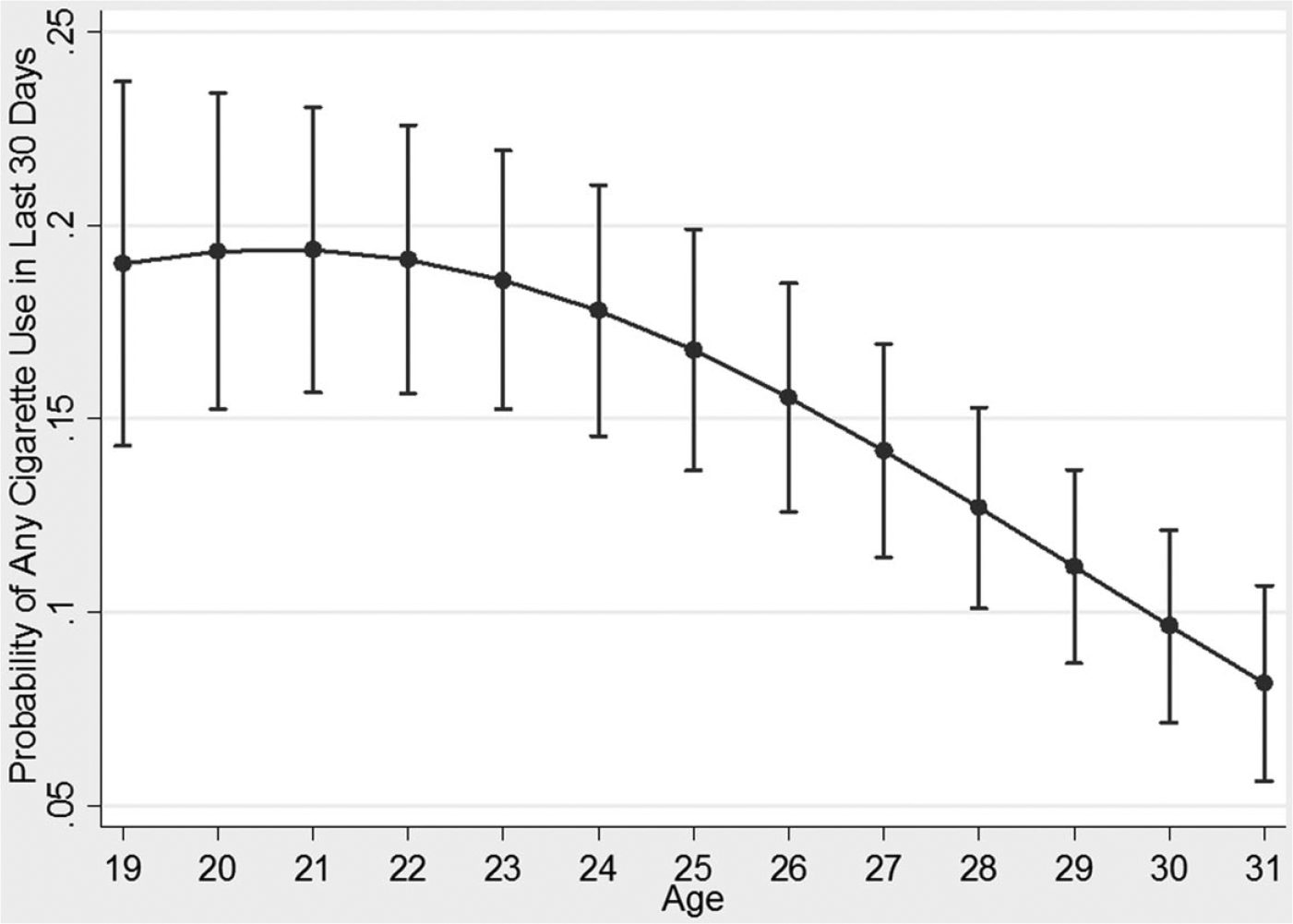
Predicted Probability of Any Cigarette Use in the Last 30 Days by Age (N = 4,341, observations = 19,668).
Results
Main Effects of Policy
Prior to including predictors of tobacco use, we ran the unconditional model. We found that for any recent tobacco use, 6.4% of the variation is at the city level, 83.8% is at the person level, and 9.8% is within individuals over time. For daily pack smoking, most of the variance is at the individual level (96.0%).
Table 2 shows the mixed effects logistic regression models for the outcomes of (1) any recent tobacco use and (2) smoked at least a pack daily. Models 1 and 3 include only the effect of comprehensive smoking bans on these outcomes. Without considering other constraints, respondents living in a city with a comprehensive ban were 41.1% less likely to report any recent tobacco use (p < .001) and 39.6% less likely to report smoking a pack daily (p < .01). When individual, city, and additional policy variables are included in Models 2 and 4, the effect of a comprehensive ban is attenuated but still significant, such that respondents in those locations are 23.7% less likely to report any tobacco use (p < .01) and 32.2% less likely to report daily pack smoking (p < .05). Thus, even considering numerous other constraints and policies, clean air restrictions still constrain individual-level smoking.
Multilevel Logistic Regression of Smoking Outcomes in National Longitudinal Survey of Youth 1997 (N = 4,341, observations = 19,668).

p < .05, **p < .01, ***p < .001 (two-tailed).
Effects of Community- and Individual-level Constraints
With our full slate of predictors, 34.9% of the individual-level and 85.6% of the city-level variation in any recent smoking is explained by the model. For daily pack smoking, 80.4% of the individual-level variation is explained (there is little city-level variance to explain). We find largely consistent results for the effects of the community- and individual-level constraints among our outcomes.
The first set of individual-level constraints pertains to family, work, and peers. Consistent with prior research, married respondents were less likely to have both recently smoked (odds ratio [OR] = .512, p < .001) or smoked a pack daily (OR = .610, p < .05). Among work predictors, only part-time job status was significant and only for any recent smoking, with part-time workers 28.9% more likely than nonworkers to have recently smoked (p < .05). Peer use in 1997 played an important role; those with half their peers smoking were 54.2% more likely (p < .05), those with 75% were 78.1% more likely (p < .01), and those with almost all peers smoking were over twice as likely (p < .01) to report any tobacco use than those with almost no smoking peers. The latter group was also 2.5 times as likely to smoke a pack daily (p < .05). For academic performance, earning mostly A’s in high school decreased the odds of any tobacco use by 43.1% (p < .05) and daily pack smoking by 77.5% (p < .01).
The second set of predictors pertain to the health of the respondent and his or her parents. For every one-unit increase in baseline depression, the odds of any tobacco use increased by 24.9% (p < .001) and by 9.0% for a pack daily (p < .05). Age 17 smoking status was strongly predictive of both outcomes (p < .001). 12 Compared to those who had parents in good/excellent health in 1997, respondents whose parents were in fair/poor health were 56.1% more likely to smoke (p < .05) and twice as likely to smoke a pack daily (p < .05).
There is a clear gradient in the effect of the socioeconomic measure for education. For any recent smoking, compared to those with a four-year college degree, significantly higher odds were found for those currently enrolled in high school (representing those who took longer than typical to complete secondary education given our starting age of 19; OR = 15.44), high school dropouts (OR = 9.93), earned a high school diploma or GED (OR = 5.66), with some college but not enrolled (OR = 4.46), currently enrolled (OR = 2.34), and with a two-year college degree (OR = 2.11). We find the same trend for daily pack smoking.
In addition to the age effects shown in Figure 3, several demographic factors had significant effects. Women were 40.5% less likely to have smoked recently (p < .001) and 57.6% less likely to report daily pack smoking (p < .001); we subsequently return to the gender effect. Blacks (any: −47.9%, p < .01; daily pack: −81.2%, p < .001) and Hispanics (−57.6%, p < .001; −90.0%, p < .001) had lower odds on both outcomes.
Among city-level predictors, one population category (100,000–250,000) had a significant effect, with those living in such cities 43.3% less likely to report any tobacco use (p < .05). For every one-unit increase in percentage of female-headed households, respondents were 15.1% more likely to report daily pack smoking (p < .01). Additionally, a one-unit increase in percentage of non-Hispanic whites increased the likelihood of daily pack smoking by 2.3% (p < .05).
Finally, the policy-level results show nonsignificant findings for other policies, with one exception. A complete vending machine restriction is associated with 54.9% lower odds of any smoking (p < .01), thus also possibly constraining smoking decisions.
Between- and Within-Person Policy Effects
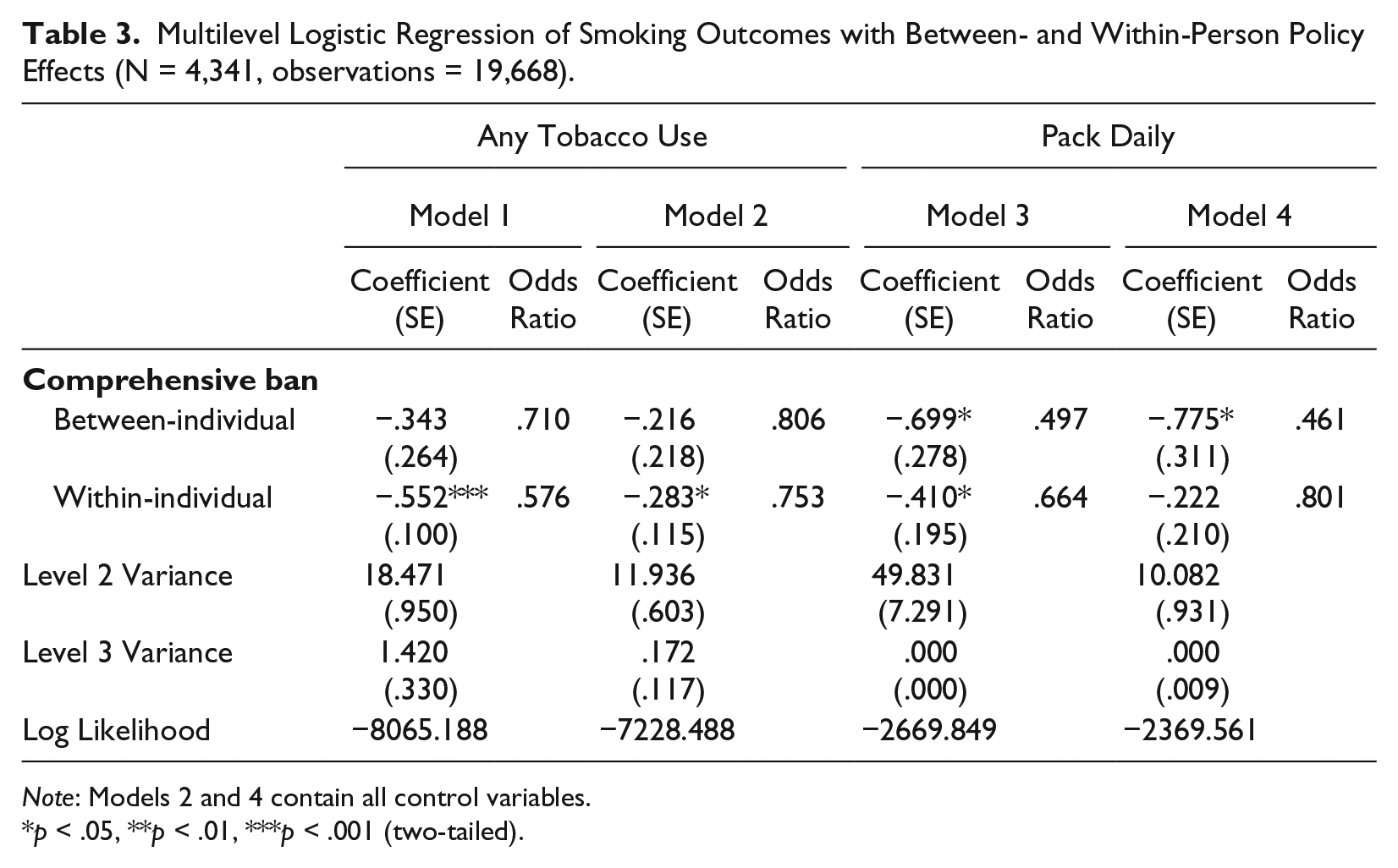
As mentioned previously, an advantage of longitudinal multilevel policy measures is the ability to decompose clean air restrictions into between- and within-person effects, given that the changing nature of the policy implies that the variable resides statistically at the lowest of the three levels in the hierarchical structure. Thus, Table 3 shows our models with this decomposition. The between effect represents the effect of differences in an individual’s average exposure to clean air policies over time and is thus an individual-level effect (Level 2 in the statistical model). The within effects represent an individual’s deviation from their average at each time point such that the effect is at the observation level (Level 1). Given that the decomposition does not affect the controls, we do not repeat them in the table.
Multilevel Logistic Regression of Smoking Outcomes with Between- and Within-Person Policy Effects (N = 4,341, observations = 19,668).
Note: Models 2 and 4 contain all control variables.
p < .05, **p < .01, ***p < .001 (two-tailed).
For any tobacco use in the last 30 days, higher average exposure to a clean air policy does not distinguish which individuals smoke at all over the observation period (the between effects), but changes in clear air policy do distinguish on which observations a given individual smokes (the within effects). For a given individual, the presence of a clean air policy results in 42.4% lower odds of any recent smoking relative to years when they were not subject to a clean air policy (p < .001). This effect remains significant when controls are added in Model 2, though now representing a 24.7% reduction in smoking for a given individual in the presence of a smoking ban.
Turning to our indicator of dependence, in Model 3 without controls, both the between- and within-person effects significantly predict daily pack smoking. When controls are included in Model 4, only the between-individual effect remains significant. Thus, higher average exposure to clean air policies across the observation period distinguishes which individuals are more likely to smoke a pack daily but does not affect whether a given individual is likely to alter their tobacco dependence. Here, a one-unit increase represents the difference between an individual who never resided in a city with a clean air policy and one who always resided in a city with such a policy. The individual with complete exposure to the policy is 53.9% less likely to smoke a pack daily on average across the observations (p < .05). For two individuals separated by .5 on the between-person effect (e.g., an individual never residing in a city with a clean air policy and one residing half the time or a person residing one-quarter of the time and one residing three-quarters of the time), the individual with higher exposure is 32.1% less likely to smoke a pack daily ([e(−.775 ×.5) − 1] × 100%).
These results make intuitive sense. For the lower threshold of any smoking, clean air policies constrain a given individual from smoking in the years in which they reside in a city with such a restriction. Once one’s smoking level reaches dependence, such a constraint does not affect a given individual. It does, however, constrain which individuals in which cities proceeded to dependent smoking.
Interactions with Policy
Finally, we examined interactions with clean air restrictions. The purpose of such interactions was to test Bird and Rieker’s (2008:205) null hypothesis that policies that constrain specific behavior might “bypass social inequalities” relative to the alternative hypotheses proposed by critics of denormalization indicating expected differences. We examined interactions by race and parental education but found no significant effects. Given Bird and Rieker’s (2008) contention that gender is not a fundamental cause, however, the potential for differences by gender remain. As shown in Table 4, clean air policy’s effect on any recent smoking significantly differed by gender, and this effect remained significant after the inclusion of the other constraints (p < .01). In Model 2, the main effect of the comprehensive ban represents the effect for males only, with 38.9% lower odds of smoking for males in the presence of a clean air policy (p < .01). The sum of the main effect and interaction represents the policy effect for females, which is essentially zero (−.492 + .456 = −.036). These effects are highlighted graphically by examining predicted probabilities, shown in Figure 4. For males, the predicted probability of any recent smoking is .19 in absence of a clean air policy and .13 in the presence of a ban. The latter value is close to the predicted value for females, which is .11 regardless of the presence of a ban. The interaction was not significant, however, in predicting daily pack smoking, such that the clean air policy constraint operated similarly for both genders when considering dependence. 13
Multilevel Logistic Regression of Smoking Outcomes with Gender by Policy Interaction (N = 4,341, observations = 19,668).
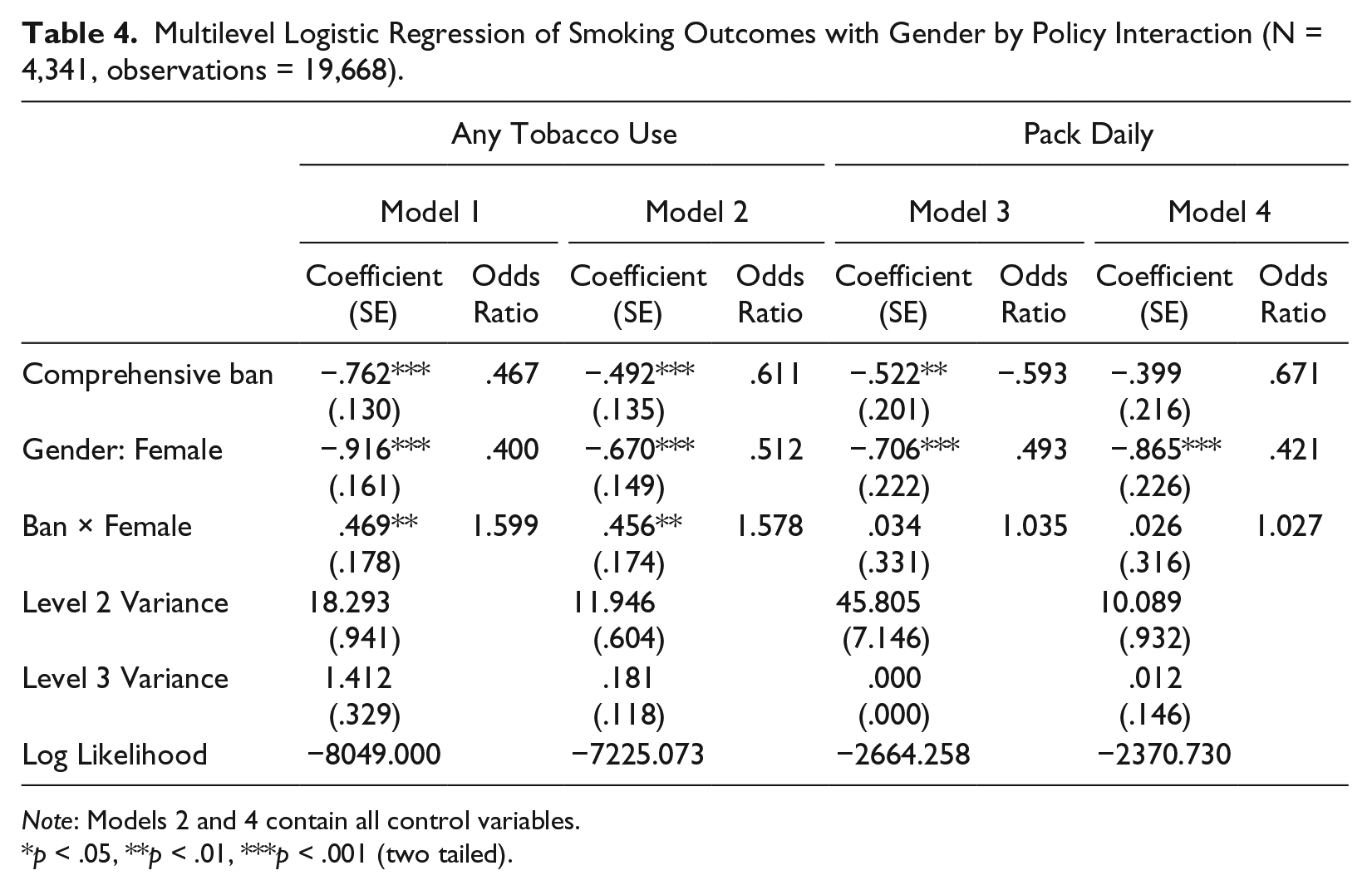
Note: Models 2 and 4 contain all control variables.
p < .05, **p < .01, ***p < .001 (two tailed).
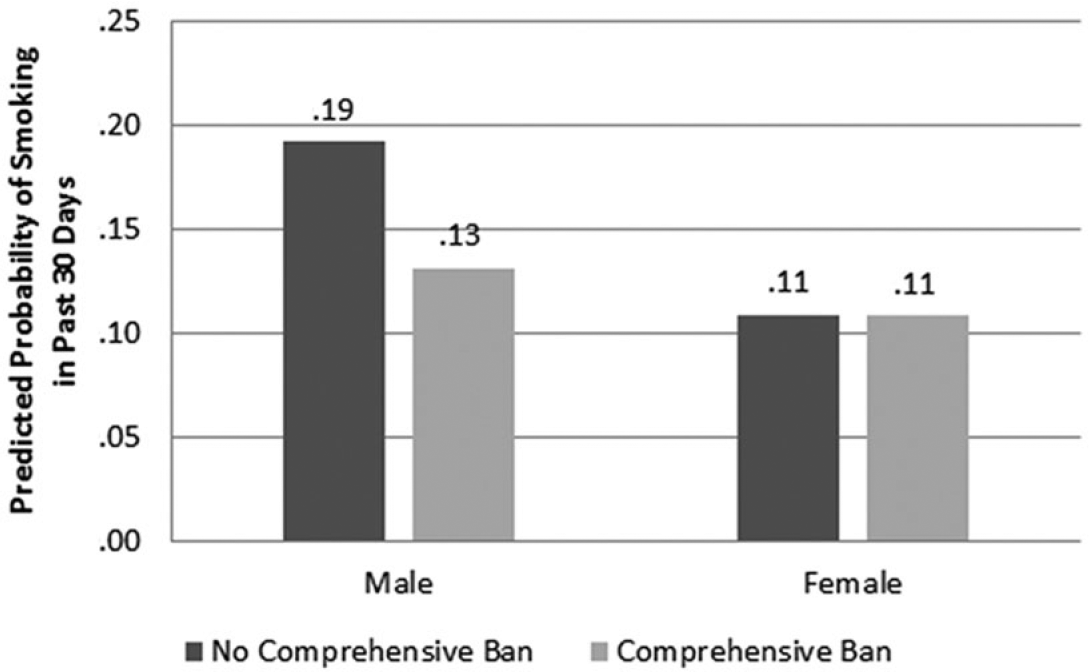
Predicted Probability of Smoking in the Past 30 Days by Comprehensive Clean Air Policy and Gender (N = 4,341, observations = 19,668).
Discussion
In this article, we sought to expand Bird and Rieker’s (2008) sociology of constrained choices in several ways through an examination of comprehensive tobacco clean air policy. First, whereas past research considered each level singly, we emphasized their theoretical model as multilevel, matching the theory with appropriate statistical methods to simultaneously consider constraints across levels. Second, we took seriously their call to examine specific policy-behavior matches, as opposed to characterizations of geographic areas’ broader health contexts. Accordingly, we took advantage of longitudinal data at both policy and individual levels over a period in which policy changed dramatically, allowing us to consider policy constraints as both a between- and within-person phenomenon. Third, we included policy at the local level, emphasizing the importance of cities in promoting clean air policy given that past studies demonstrate that policy changes followed a bottom-up pattern that began with local municipalities and spread to counties and states (Shipan and Volden 2006). Fourth, while prior work on constrained choices has focused on adult and later life health outcomes, we shifted the focus to young people, a more salient period in which to consider substance use. Finally, we tested their proposition that policies that equally restrict behavior regardless of resources might “bypass” social inequalities, which reiterated the importance of gender when considering constraints. In terms of our empirical contributions, our study overcomes limitations (Friend et al. 2011) of past examinations of clean air policy that were cross-sectional or based on cohort effects, examined a single locality or policy, or neglected the local level. We believe we can make stronger claims through the use of repeated observations, nationally representative data, and multilevel policy information that includes both the state level and often overlooked city level.
Importantly, we demonstrate the utility of the multilevel nature of Bird and Rieker’s (2008) constrained choices framework. While the theory describes layers of constraints and multilevel statistical analyses of health outcomes are increasingly common, researchers have yet to explicate a multilevel theoretical and statistical approach to constraints that simultaneously considers these levels. Here, we believe the theory of constrained choices has been underutilized and has considerable explanatory potential. By simultaneously considering the levels of policy, community, and work/family constraints, we can better isolate the effects of each level as well as their interactive and mediating effects, particularly with a longitudinal approach.
For our analysis, the policy level was the central focus in order to further the theory’s applicability by examining a policy specifically designed to constrain a particular behavior. In short, we found that even while including other constraints and tobacco policies, there remains a significant effect of clean air restrictions on young people’s smoking behaviors, both in terms of health choices measured by any smoking in the past 30 days and dependence measured by smoking a pack daily. While proximal levels of constraint may resonate more vividly when an individual is confronted with health decisions, our analysis demonstrates that policy is associated with health choices and outcomes beyond these other critical constraints. We also found that this policy constraint operated differently when considering use and dependence, supporting the theory’s distinction between health choices and biological processes. For any recent smoking, the policy constrains the same individuals such that a given person’s odds of smoking are lower in observations in which they resided in a location with a comprehensive clean air policy. For our indicator of dependence, a change in policy is not associated with a given individual’s likelihood of smoking a pack daily. Rather, such policies constrain which individuals ever reach this level of dependence.
The policy implications for public health are straightforward. Temporally, given the relatively short period we examined, smoking bans have a rather rapid impact on any smoking for a given individual, indicating that they influence cessation among some tobacco users over time. Studies of the denormalization of smoking indeed support this relatively quick change in attitudes and behavior resulting from bans, especially among casual smokers (Kelly 2009). On the other hand, while smoking bans did not affect a dependent young adult’s probability of reducing their level from a pack daily, such bans do distinguish between individuals smoking at that level. Importantly for mortality and morbidity, if policies continue to affect the probability of smoking a pack daily across individuals, fewer young people will reach this level of dependence as policies continue to spread. Thus, while dependent smokers are unlikely to cease smoking when facing these policies, we would expect fewer individuals to eventually become dependent as these policies proliferate. Though not our central focus, we also found that vending machine restrictions may constrain any recent smoking but not dependence.
We also highlighted the importance of examining policies at the local level where appropriate. In the case of smoking bans in the United States, city bans typically preceded state bans (Shipan and Volden 2006), and many states still do not have comprehensive clean air policies while cities within those states do. Thus, considering only a higher geographic level such as the state would neglect these two possibilities, essentially treating some individuals incorrectly as if they lived in a locale without a ban. Here, we considered policy itself as multilevel by accounting for the presence of both state and local policy. As Bird and Rieker (2008) suggested, multiple policy levels, including an emphasis on the local, are important and should be evaluated in future research on health outcomes.
Though not tested in their original work, Bird and Rieker (2008) suggested that policies that affect individuals regardless of socioeconomic status might bypass inequality, using smoking bans as a specific example. We tested this possibility through interactions with gender, race, and parental socioeconomics. The latter two were not significant, suggesting that perhaps smoking bans do bypass inequality and affect young people similarly regardless of race and parental socioeconomic status. In some ways, this finding runs counter to critics of denormalization who state that policies may be less effective for those from disadvantaged backgrounds; our data suggest that these policies are wide reaching and similarly impact the advantaged and young people who occupy more marginal social positions. We are careful, however, to interpret these nonsignificant results with caution and encourage future research in this area. With a significant effect for males and virtually no effect for females, the findings for gender support Bird and Rieker’s (2008) central thesis that constraints operate differently for men and women. While we cannot distinguish the exact mechanism, such as biological differences in the propensity for addiction or perhaps that young men frequent establishments with bans more often, the finding is nonetheless supportive of the central tenets of constrained choices theory stating that gender is not and does not operate the same as fundamental causes related to socioeconomic status.
We are careful to note limitations within our study. First, we only included young adults whose city we could identify, restricting our analysis to respondents who resided in central cities of CBSAs. We are careful to limit our generalizability to such young people. Second, our community-level variables were measured at the city level. This choice was strategic given that this is the lowest geographic level at which clean air policies are enacted. We recognize, however, that for some of the constraints related to community socioeconomics and disorder, a lower level akin to the neighborhood might be necessary and could be driving some of the null results. Third, in the theoretical model, we considered a measure indicative of dependence as tapping into the biological process at the bottom of the figure. We note that this is a narrow definition of biological processes as they relate to tobacco use and dependence. We recommend further research that incorporates actual individual-level biological indicators. Lastly, we did not examine the component of the model related to mortality and morbidity. The health repercussions of tobacco smoke are well established (U.S. Department of Health and Human Services 2010), and we chose to focus on the period of the life course where substance use is highest, thus concentrating on young adults as opposed to later life health outcomes.
Despite these limitations, this article demonstrates that the levels of constraints in Bird and Rieker’s (2008) model can be recast as a multilevel model that simultaneously incorporates several contextual levels. Further, examining policy-behavior matches, particularly at the local level, provides a fruitful avenue for continued research using the sociology of constrained choices, as demonstrated by the significant effect of smoking bans. We argue that the constrained choices framework is more widely applicable than the heretofore narrow utilization of the theory to argue that gender, biology, or some broad concept of constraints are important for health outcomes. Rather, the constrained choices framework offers a powerful theoretical paradigm to synthesize several disparate analytic levels within health research, and we encourage its future application in such a manner.
Footnotes
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.